
Abstract
Background. Current knowledge about spatial neglect and its impact on rehabilitation mostly originates from stroke studies. Objective. To examine the impact of spatial neglect on rehabilitation outcome in individuals with traumatic brain injury (TBI). Methods. The retrospective study included 156 consecutive patients with TBI (73 women; median age = 69.5 years; interquartile range = 50-81 years) at an inpatient rehabilitation facility (IRF). We examined whether the presence of spatial neglect affected the Functional Independence Measure (FIM) scores, length of stay, or discharge disposition. Based on the available medical records, we also explored whether spatial neglect was associated with tactile sensation or muscle strength asymmetry in the extremities and whether specific brain injuries or lesions predicted spatial neglect. Results. In all, 30.1% (47 of 156) of the sample had spatial neglect. Sex, age, severity of TBI, or time postinjury did not differ between patients with and without spatial neglect. In comparison to patients without spatial neglect, patients with the disorder stayed in IRF 5 days longer, had lower FIM scores at discharge, improved slower in both Cognitive and Motor FIM scores, and might have less likelihood of return home. In addition, left-sided neglect was associated with asymmetric strength in the lower extremities, specifically left weaker than the right. Finally, brain injury–induced mass effect predicted left-sided neglect. Conclusions. Spatial neglect is common following TBI, impedes rehabilitation progress in both motor and cognitive domains, and prolongs length of stay. Future research is needed for linking specific traumatic injuries and lesioned networks to spatial neglect and related impairment.
Introduction
Spatial neglect, a disorder of spatial attention, affects perception, memory, action planning, and motor control of, in, or toward the side of space contralateral to the primary injury in the cerebral hemisphere.1,2 For example, a person with this disorder after right brain damage neglects the left side of space. The earliest documentations of spatial neglect, such as Riddoch’s 1935 3 and Brain’s 1941 4 reports, described cases with various acquired brain injuries, including brain tumors, stroke, and traumatic brain injury (TBI). Since then, much has been learned about the mechanisms of various symptoms manifested by individuals with spatial neglect, and the investigation of the disorder has provided many theoretical insights into the understanding of spatial cognition.2,5-7 On the other hand, the effects of spatial neglect are established mainly from studies on stroke survivors. 8 Spatial neglect prolongs stroke survivors’ hospitalization,9,10 impedes stroke rehabilitation outcomes,11-13 and increases stroke patients’ risks of fall14,15 and unsafe navigation while walking 16 or using a wheelchair. 17 It is relatively unknown how spatial neglect affects rehabilitation success in other populations such as those with TBI. In this study, we focus on TBI for the fact that 275 000 Americans are hospitalized because of TBI, and 90 000 experience a long-term disability annually.18,19 Spatial neglect may contribute to the difficulties that individuals with TBI face on a daily basis and, thus, slow down their progress in rehabilitation.
Most studies on spatial neglect following TBI are case reports. One exception is the report by McKenna et al 20 published in 2006. Recruited from a brain injury rehabilitation center with inpatient and outpatient services, 45.2% of their study participants (n = 31) demonstrated spatial neglect. 20 The authors found that in comparison to those without the disorder, TBI patients with spatial neglect had poorer motor function measured with the motor score of the Functional Independence Measure (FIM) or Motor FIM score, but their Cognitive FIM score was not inferior. 20 Thus, like the influence of spatial neglect in stroke patients,15,21,22 the finding by McKenna et al 20 suggests that spatial neglect primarily worsens motor dysfunction in TBI patients. This is quite interesting because the most observable manifestation of spatial neglect reported in the literature to date is in the domain of perception, especially the visual modality, but it can also be observed in auditory, 23 proprioceptive, 24 and tactile modalities. 25 Spatial neglect may be manifested as asymmetric motor weakness or movement abnormality in the neglected side of space (ie, motor or motor-intentional neglect).7,26-29 In the present study, we conducted a retrospective data analysis with a consecutive sample of individuals with TBI in the setting of an inpatient rehabilitation facility (IRF). In addition to examining Motor and Cognitive FIM scores, we investigated whether spatial neglect is associated with an asymmetry in extremities as measured in tactile sensation and muscle strength.
Spatial neglect may decrease the likelihood of stroke survivors’ returning home at IRF discharge.15,22,30 Here, we collected discharge disposition of patients with TBI and examined whether spatial neglect was associated with fewer discharges to home from the IRF in the TBI population. We also explored the lesion-symptom association based on the available injury history and radiology records that were transcribed from acute care records into the inpatient rehabilitation records.
Methods
Patient Selection
The study was approved by the institutional review board of the Kessler Foundation. We reviewed 360 consecutive admission records (February 2012 to April 2013) with a diagnosis of TBI admitted to the Kessler Institute for Rehabilitation; 1 record was immediately discarded because of a missing history and physical examination. For patients who had multiple admissions, we used the last admission for we considered this rehabilitation stay to be the one where patients were able to consistently participate in the prescribed rehabilitation program. Patients were included if they met the following criteria: (1) time postinjury at admission <100 days for including acute to subacute patients, (2) no history of stroke or co-occurrence of TBI and stroke for eliminating stroke-induced neglect symptoms, (3) no disorders of consciousness (DOC) for ensuring the minimal reliability of behavioral testing, and (4) available results from the Catherine Bergego Scale or Star Cancellation Test indicating the presence or absence of spatial neglect. We performed 2 comparative analyses to examine selection bias based on criteria 3 and 4 (see Tables A.1 and A.2 in the appendix).
The final sample included 156 patients (73 women; median age = 69.5 years; interquartile range [IQR] = 50-81; median days postinjury at IRF admission = 9 days; IQR = 5-17). In the included sample, 32 had valid (ie, patient not intubated or sedated) Glasgow Coma Scale scores available (median = 14; IQR = 10-15). The most common cause of TBI in the current sample was falls (n = 105), and other causes were motor vehicle accidents (including cars, bikes, and motorcycles; n = 16), pedestrians struck by a car (n = 12), assaults (n = 5), and others (n = 18). Among the 156 patients, 21 had skull fractures, 15 had facial bone fractures, and 9 had both. For those who had a decompression procedure, 32 patients had craniotomy, 7 had burr holes, and 6 had ventricular drains or shunts.
Group Assignment Based on the Presence of Spatial Neglect
We used the Star Cancellation Test and the Catherine Bergego Scale to identify and categorize patients into the SN+ (ie, presence of spatial neglect) or SN− groups. This choice of instruments, especially the Star Cancellation Test, was based on information availability. Other paper-and-pencil tasks (eg, line bisection, figure copying, text reading) and the double-simultaneous-stimulus detection task have various sensitivities to different symptoms of spatial neglect.31,32 However, a comprehensive battery of neglect tests was not part of the standard care performed in the IRF and, thus, not routinely administered or clearly documented in the current sample of patients. If a given patient was indicated as having abnormality in lateralized omission in the Star Cancellation Test or having spatial neglect in the Catherine Bergego Scale, then the patient was categorized into the SN+ group; otherwise, the patients was assigned to the SN− group.
The Star Cancellation Test, a subtest of the Behavioral Inattention Test, is printed on paper (21.6 × 27.9 cm2) with a random array of 56 smaller stars (8 mm), 52 larger stars (14 mm), 13 letters, and 19 short (3-4 letters) words. The longer edge of the paper is placed parallel to the patient’s chest. The examiner demonstrates the task by marking out 2 smaller stars positioned midline of the page and instructs the patient to mark out (ie, cancel out) all the smaller stars. 33 The cutoff score is 51, suggesting that patients with 3 omissions have spatial neglect. 33 In the present study, we used the biased omission cutoff to determine the presence or absence of spatial neglect in terms of spontaneous spatial exploration. If the left-sided omissions were greater than the right-sided omissions by 3 or more counts, the patient was classified as having left-side neglect, and vice versa.
The Catherine Bergego Scale includes 10 items evaluating incomplete or ineffective behaviors in the neglected side of space during activities of grooming and shaving, putting on sleeves or slippers, eating food on the plate, and cleaning the mouth after eating as well as during observations of spontaneous gaze orientation, knowledge of the left or right part of the body, auditory attention, collisions with people or objects on a path, finding the way when traveling to familiar locations, and finding personal belongings. 34 Each item is scored 0, 1, 2, or 3 indicating no, mild, moderate, or severe symptoms, respectively, of spatial neglect. The final score is the sum of item scores divided by the number of scored items and multiplied by 10. A final score greater than 0 indicates the presence of spatial neglect. 34
Outcome Measures
We used several variables as outcome measures, including extremity asymmetry in tactile sensation and motor strength, length of stay, rehabilitation success (ie, FIM scores at discharge, FIM improvement, FIM improvement rate), number of readmissions, number of acute transfers during or at the end of IRF care, and discharge disposition. Below, we described measures of asymmetry in the extremities and the indices of rehabilitation success.
Asymmetry in Extremities
Attending physicians assess all IRF patients for tactile sensation and muscle strength of upper and lower extremities. After an examination with light touch (by physicians’ hands) from the shoulder to fingers, or from the hip to toes, a given extremity was determined to have intact, diminished, or absent tactile sensation. In this study, if both upper extremities were in the same category, then they were considered symmetric in tactile sensation; if not, they were coded as asymmetric, and the relative difference between the 2 extremities was recorded (eg, left < right). The same coding was applied to the lower extremities.
We also used attending physicians’ evaluation records to determine the patients’ muscle strength. Primarily based on the modified grading Medical Research Council scale, 35 a given muscle group was scored 1, 2, 3, −4, 4, +4, or 5. The higher score meant closer to normal or unimpaired strength. To determine if a given patient had left-versus-right asymmetry in muscle strength of the upper or lower extremities, we categorized each extremity as normal, moderate, or mild to no strength if the most frequently assigned score for that extremity was =5, ≥3, or < 3, respectively, on the scale. Using the assigned strength category, we compared the left and right upper extremities, and the left and right lower extremities. Thus, a patient was determined to have symmetric strength, asymmetric strength with left weaker than right, or asymmetric strength with right weaker than left in the upper or lower extremities.
Rehabilitation Success
We used the FIM to examine the success of inpatient rehabilitation. The FIM consists of 18 items assessing level of independence in 2 domains.36,37 The motor domain includes eating, grooming, bathing, dressing of upper and lower body, toileting, bladder and bowel management, transfers (bed/chair/wheelchair, toilet, tub/shower), and mobility (walk/wheelchair, stairs). The cognitive domain includes comprehension, expression, social interaction, problem solving, and memory. Each item is scored from 1 (maximal assistance) to 7 (complete independence). The measure can be recorded as the Motor FIM score (range = 13-91), the Cognitive FIM score (range = 5-35), and the Total FIM score (range = 18-126). We calculated FIM improvement by subtracting scores at admission from scores at discharge, and defined the FIM improvement rate as FIM improvement per day during the IRF stay.
Brain Injury and Lesion Location
Imaging occurred in the acute care hospital and was reported in the IRF medical record if available. For the exploratory analysis of lesion-symptom association, we collected information on the following variables: cortical parenchymal injury, noncortical parenchymal injury, epidural hematoma, subdural hematoma, subarachnoid hematoma, and intraventricular hemorrhage. Each variable was coded 0 = no record of injury; 1 = left hemisphere; 2 = right hemisphere; 3 = both hemispheres, and 4 = unspecified hemisphere. We also included 2 additional variables: mass effect and diffuse axonal injury.
Analysis
Because all the variables and outcome measures were not consistent with a normal distribution, all the descriptive statistics and the group comparisons were performed using nonparametric statistical methods. All the analyses were performed with STATA/SE 12.1.
Results
Left-Sided Versus Right-Sided Neglect
Of the 156 patients, 84 were assessed using both the Star Cancellation Test and Catherine Bergego Scale, and the rest of the patients were examined with one of the assessments. In all, 132 patients were assessed with the Star Cancellation Test, and 24 of them showed spatial neglect. Specifically, there were 16 patients with left- and 8 with right-sided neglect. Because the performance on this test might be confounded by visual deficits or upper-extremity impairment, we conducted a preliminary analysis and found no evidence that visual field cut or upper-extremity weakness accounted for left- or right-sided neglect.
In all, 108 patients were assessed with the Catherine Bergego Scale, and 30 of them had positive scores indicating spatial neglect. However, in the records we reviewed, no score was noted for left- or right-sided neglect.
Is Spatial Neglect Associated With an Asymmetry in Extremities?
For this series of analyses, we included patients who were assessed with the Star Cancellation Test for its result containing the specific information of lateralization in omission bias, which served as the index of the left- or right-sided neglect. In addition, we excluded patients who had positive scores on the Catherine Bergego Scale but showed no lateralized asymmetry on the Star Cancellation Test.
Tactile Sensation
Among the patients, 14 were not assessed for tactile sensation of the upper extremities. One was not fully assessed because of pain in the upper extremities; 101 had normal sensation in both the left and right upper extremities. For the remaining 2 patients, it was found that the left upper extremity was less sensitive than the right, but they did not show spatial neglect on the Star Cancellation Test.
Similarly, there was no record of tactile sensation of the lower extremities in 14 patients; 1 patient was not fully assessed because of pain in the lower extremities; 1patient had diminished sensation because of diabetes; and 101 had normal sensations in both the left and right lower extremities. For the remaining patient, the left was weaker than the right lower extremity, but this patient did not show abnormal lateralized omission errors on the Star Cancellation Test. Thus, no evidence suggested that left- or right-sided neglect was associated with extremity asymmetry in tactile sensation.
Muscle Strength
The upper extremities of 15 patients were not assessed (or reliably assessed), and 16 patients’ lower extremities were not assessed. Thus, they were not included in this analysis. It was found that 86 patients had symmetrical strength in their upper extremities (49 normal and 37 moderate strength in both left and right) and 85 patients had symmetrical strength in their lower extremities (45 normal, 38 moderate, and 2 mild to no strength in both left and right).
To examine whether left-sided neglect was associated with asymmetric strength in upper or lower extremities, we performed a logistic regression analysis with 2 categorical variables for the upper and lower extremities. Each variable had the same categories: 0 = symmetry strength; 1 = left weaker than right; 2 = right weaker than left. The model accounted for 29% of variance (pseudo R2; P < .001) and revealed only one significant factor—left lower extremities were weaker than the right: odds ratio (OR) = 64.3; standard error (SE) = 84.07; 95% confidence interval (CI) = [4.97, 833.03]; P = .001. ORs of the other factors were above 1.0, but P values were >.500. The same analysis was performed to examine right-sided neglect. However, right weaker than left in both upper and lower extremities were omitted from the model, for they perfectly predicted absence of right-sided neglect. The final model was not significant (pseudo R2 = .07; P = .221), and no factor reached significance (all P > .992). Thus, the results indicated that left-sided neglect was associated with asymmetric strength in the lower extremities, with the left being weaker than the right specifically.
Does Spatial Neglect Impede Rehabilitation Outcome?
In the current sample of 156 TBI patients, 47 (30.1%) had spatial neglect. Among the 84 patients who were assessed with both tests, 31 (36.9%) showed signs of spatial neglect on either (n = 24) or both (n = 7) tests. We used the total sample (n = 156) to perform the group comparisons (SN+ vs SN−) summarized in Table 1. The 2 groups did not differ in sex ratio, age, severity of TBI, time postinjury at IRF admission, total FIM scores at admission, number of readmissions, number of transfers to acute care, or discharge disposition. However, the percentage difference in home discharge—SN+ versus SN− of 68.1% versus 82.6%—was a meaningful effect size (P = .057). The SN+ group had inferior Cognitive FIM scores compared with the SN− group at admission, as confirmed by the 2-tailed U test (P = .004), and the SN+ group stayed in the IRF 5 days longer than the SN− group (P = .007). Even with a longer inpatient rehabilitation stay, the SN+ group had lower Cognitive and Total FIM scores at IRF discharge than the SN− group and lower improvement rates in Motor, Cognitive, and Total FIM scores (Table 1). Thus, spatial neglect hindered the success of inpatient rehabilitation.
Comparison Between Patients With and Without Spatial Neglect (SN+ vs SN−). a
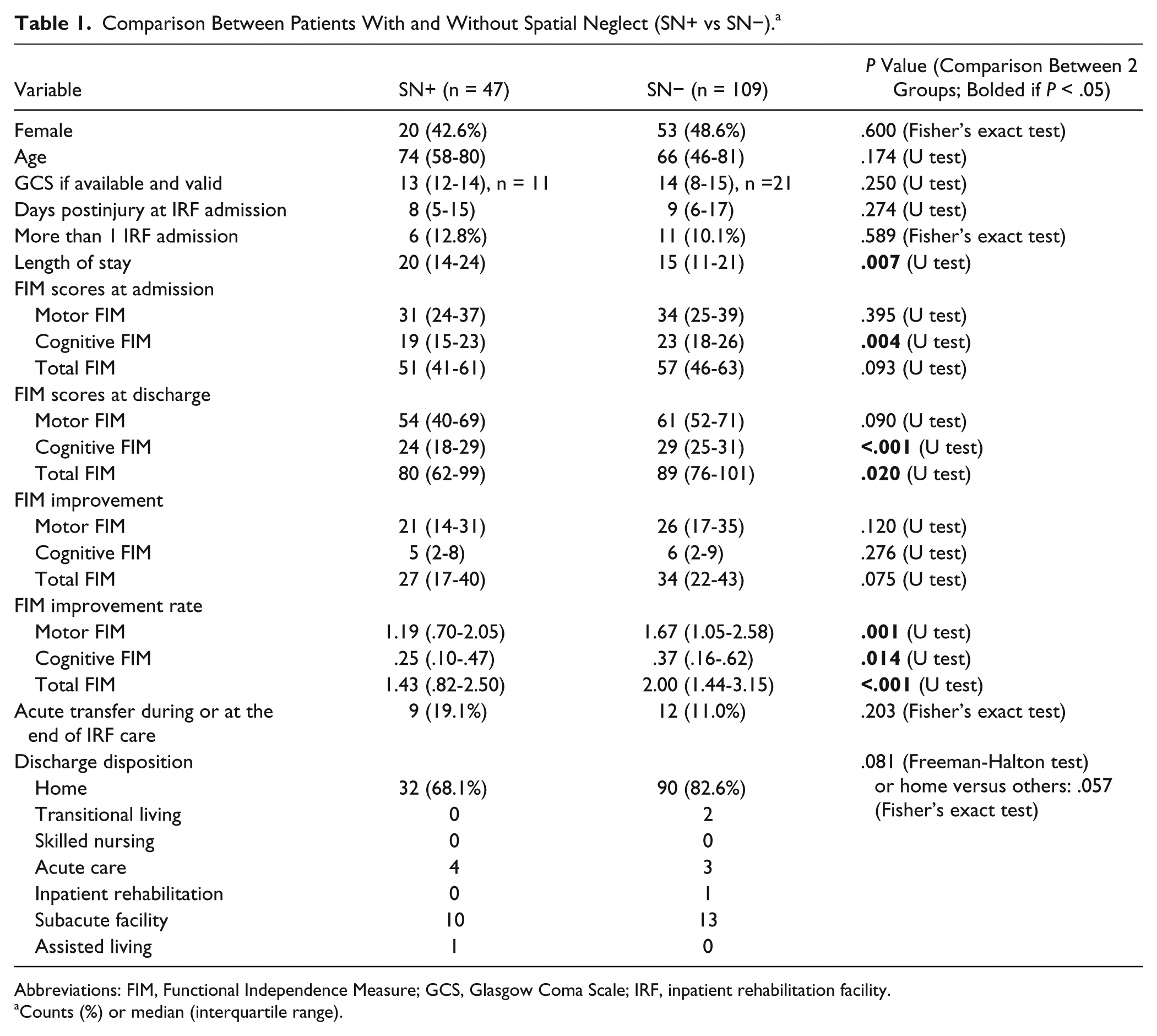
Abbreviations: FIM, Functional Independence Measure; GCS, Glasgow Coma Scale; IRF, inpatient rehabilitation facility.
Counts (%) or median (interquartile range).
Is Spatial Neglect Associated With a Specific Type of Brain Injury?
In this exploratory analysis, we again only included the patients who were assessed with the Star Cancellation Test, for its result indicates the side of neglect, and excluded those who had positive scores on the Catherine Bergego Scale but showed no asymmetric performance on the Star Cancellation Test. Exploring the variables associated with left-sided omission bias, a logistic regression analysis with the 8 categorical variables revealed only 1 significant factor—mass effect: OR = 64.98; SE = 89.64; 95% CI = [4.35, 970.54]; P = .002. Another multivariable logistic regression investigating right-sided omission bias did not result in any significant effect (P ranging from .115 to .908). Thus, we did not find evidence for a unilateral brain injury inducing contralesional neglect, but the presence of a mass effect was associated with left-sided neglect.
Discussion
The present findings have great implications for clinicians and researchers because they may encourage more clinical attention and scientific exploration in spatial neglect after TBI. Consistent with findings reported by McKenna et al, 20 the present study showed that spatial neglect predicted poorer functional independence at discharge from an inpatient rehabilitation center. The association between left-sided neglect and the relatively weaker left lower extremity could have reflected motor-intentional neglect7,26-29 and contributed to the undesirable rehabilitation outcomes; this requires further investigation. In addition, we found that neglect patients stayed longer in IRF by a median of 5 days. This suggests that increasing the days of intensive rehabilitation may not be enough to help neglect patients reach a satisfactory level of functional independence before discharge from an IRF.
That spatial neglect hinders the progress of rehabilitation is supported by the results demonstrating that patients with spatial neglect had lower FIM improvement rates in both motor and cognitive domains than those without spatial neglect. Items comprising the Motor FIM subscale involve cognitive functions such as perception, memory, and action planning that can be impaired by spatial neglect.23-25,38-41 The current findings provide another piece of evidence supporting the need for therapeutic approaches to improve spatial awareness in motor and cognitive tasks in individuals with TBI. 20 For example, if a patient’s self-perceived body midline is deviated from the normal range, he/she may have a harder time participating in a therapy session than other patients who are able to sit up straight (with or without assistance) or attend to their contralesional limbs. To date, research on spatial neglect has been primarily conducted in the stroke population, and a few advances have been applied to stroke rehabilitation.42,43 The characteristics and symptoms of spatial neglect in TBI might differ from those after stroke because of the difference in etiology. To optimize rehabilitation outcomes in the 30% to 45% of patients with TBI affected by spatial neglect, 20 it is crucial that specific and systematic spatial rehabilitation techniques for the TBI population are developed.
Well-established from stroke studies, spatial neglect renders abnormal bias toward the hemispace ipsilateral to the brain lesion, and hence, the patient neglects the contralesional hemi-space. After a stroke, damage to the brain is usually focal or unilateral; however, damage to the brain after a TBI is often multifocal or diffuse. Previous studies suggest that individuals with TBI are at a high risk of left-sided spatial neglect or attentional imbalance biased toward the right hemispace regardless of the profile of their brain lesions.20,44,45 Those studies are consistent with the accumulating evidence suggesting that it is the damaged neural network rather than a specific brain area that is critical for the occurrence of spatial neglect.46-49 However, perhaps because of incomplete information, the present study only revealed 1 significant predictor—that is, injury-induced mass effect in the brain, associated with left-sided neglect. Sophisticated lesion classification and imaging analysis will be necessary to further understand the underlying mechanism of spatial neglect following TBI.
Study Limitations and Suggestions
Our findings may only be applicable to individuals with TBI receiving IRF care and cannot be applied to those admitted with the classification of having a disorder of consciousness because they may have different demographic and injury characteristics (Table A.1). Because of the retrospective nature of the study, the availability or accessibility of medical information regarding their TBI as well as the rehabilitation documentation was suboptimal. For example, we excluded patients who were not assessed for spatial neglect, and the reason why they were not assessed is unknown. Approximately 27% of patients without a disorder of consciousness were not assessed for spatial neglect. However, these excluded patients did not differ from the included patients in demographic or injury characteristics (Table A.2). Even when patients were assessed, how therapists performed the Catherine Bergego Scale or the Star Cancellation Test is unknown, which may affect the sensitivity of a given assessment. In particular, the fact that the Catherine Bergego Scale assesses spatial neglect in more dimensions than the Star Cancellation Test indicates that the Catherine Bergego Scale is more sensitive 31 and also suggests that the Catherine Bergego Scale is open to greater variation in how it may be administered.34,50 This may be the reason why some patients met the criterion of spatial neglect based on the Star Cancellation Test score but not on the Catherine Bergego Scale. On the other hand, the Star Cancellation Test alone cannot identify all the patients with spatial neglect because of the complexity of the disorder, which can be manifested in various forms in different tasks (eg, line bisection, figure copying, text reading, double-simultaneous-stimulus detection). Future prospective studies should use a comprehensive battery of neglect tests and ensure that examiners follow standardized assessment procedures such as the Kessler Foundation Neglect Assessment Process8,51 to assign categorical scores on the Catherine Bergego Scale.
Another example of suboptimal retrospective information is that some patients were excluded from certain analyses because of missing certain records (eg, muscle strength). Injury and brain lesion information was not always comprehensive, and we assumed the absence of an injury if that injury was not mentioned at all in the medical record. Because of this limitation, we were unable to examine whether the poor functional improvement and outcome could be a result of the presence of spatial neglect as well as other disabling deficits likely induced after the same or adjacent brain networks were damaged.2,52,53 A much larger-scale prospective study, with patients from other postacute settings, is needed to estimate the general clinical impact of spatial neglect on postacute TBI recovery.
Conclusions
Spatial neglect commonly occurs following TBI in individuals receiving inpatient rehabilitation care. Spatial neglect impedes rehabilitation progress in both motor and cognitive domains, prolongs length of stay in an IRF, and may reduce the likelihood of returning home at IRF discharge. Future research is needed for linking specific traumatic injuries and lesioned networks to spatial neglect and related impairment.
Footnotes
Appendix
We retrospectively collected patient information of TBI admissions from February 2012 to April 2013. This collection yielded 360 admissions. One admission was excluded because of missing history and physical medical information in the patient’s charts. We then followed the exclusion criteria listed below.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Kessler Foundation and the Wallerstein Foundation for Geriatric Life Improvement.