
Abstract
Background. A new interdisciplinary postacute rehabilitation unit, the Kaifukuki (convalescent) rehabilitation ward (KRW), has been incorporated into the Japanese medical insurance system since 2000. More than 57 000 beds (45 beds per 100 000 population) are currently available nationwide. The maximal coverage for therapy sessions increased from 2 to 3 hours per day, 7 days a week, in 2006. Objective. To investigate how changes in policy affected rehabilitation outcomes of KRWs in a retrospective cohort study of 87 917 patients over 10 years. Results. The mean (standard deviation) age of the patients was 73.0 (13.8) years, and 55.4% were women. Diagnoses included stroke (47.9%); orthopedic diseases, including hip fracture (35.2%); and traumatic brain and spinal cord injury (5.4 %). Onset–admission interval (OAI) was 31.5 (18.6) days, length of stay was 75.9 (46.1) days, and 69.1% were discharged home. Daily therapy time was 79.4 (34.5) minutes. Admission/discharge scores of the Barthel Index and the Functional Independence Measure were 49.3 (31.0)/70.4 (31.9) and 75.3 (31.2)/91.7 (31.8), respectively. Year-by-year comparison revealed that older age, greater initial disability, and shorter OAI were coupled with a higher dose of rehabilitative interventions and a higher rate of home discharge. Longitudinal data from a cohort of hospitals implied a small but significant dose-dependent effect of hours of therapy on rehabilitation outcome after stroke. Conclusions. Although the organization of KRWs is in flux as the system of hospitals grows, results over the past 8 years suggest that changes in national insurance policies are affecting the quantity and organization of rehabilitation interventions and improvement in patient outcomes.
Introduction
Based on the findings from randomized controlled trials of organized stroke units, there is an international consensus that early, interdisciplinary, and more hours of rehabilitation improves activities of daily living (ADLs), walking status, and percentage of patients discharged home. 1-6 Length of stay (LOS) in inpatient rehabilitation facilities (IRFs) has been considerably shortened over the past 2 decades, especially in North America. 7 One of the possible solutions to shorter LOS is early supported discharge, where patients are managed in the community by an interdisciplinary team. 8-11 In Japan, there had been no definitive system for an inpatient facility to provide early and intensive rehabilitation. Consequently, patients with stroke often received low-intensity inpatient rehabilitation for more than 6 months. With the increasing number of elderly patients, rehabilitation resources had to be more effectively used.
The Japanese national insurance system introduced the Kaifukuki rehabilitation ward (KRW) in 2000. Kaifuku-ki represents the recovery or convalescent phase. To facilitate an interdisciplinary team approach, the KRW team had to provide patients and their families with a comprehensive monthly rehabilitation plan, including information about achieved goals, planned goals, and rehabilitative approaches to achieve the goals; discharge planning; and social resources necessary for a home discharge. Timing for discharge was set when patients reached a plateau in ADLs according to an interactive evaluation, which has facilitated home discharge of severely disabled patients with stroke. 12 The more organized rehabilitative intervention in the KRW also resulted in improved functional outcome. 13
The Ministry of Health, Labor and Welfare of Japan has defined the KRW as the main system of IRF covered by the medical insurance system. All patients who still need assistance in ADLs after treatment in acute hospitals are transferred to KRWs. The number of beds has continuously increased—3651 beds in 2000, 14 865 in 2002, 27 261 in 2004, 40 403 in 2006, 53 802 in 2008, and 57 028 in 2009—comprising 4.5% of total hospital beds in Japan (Figure 1).
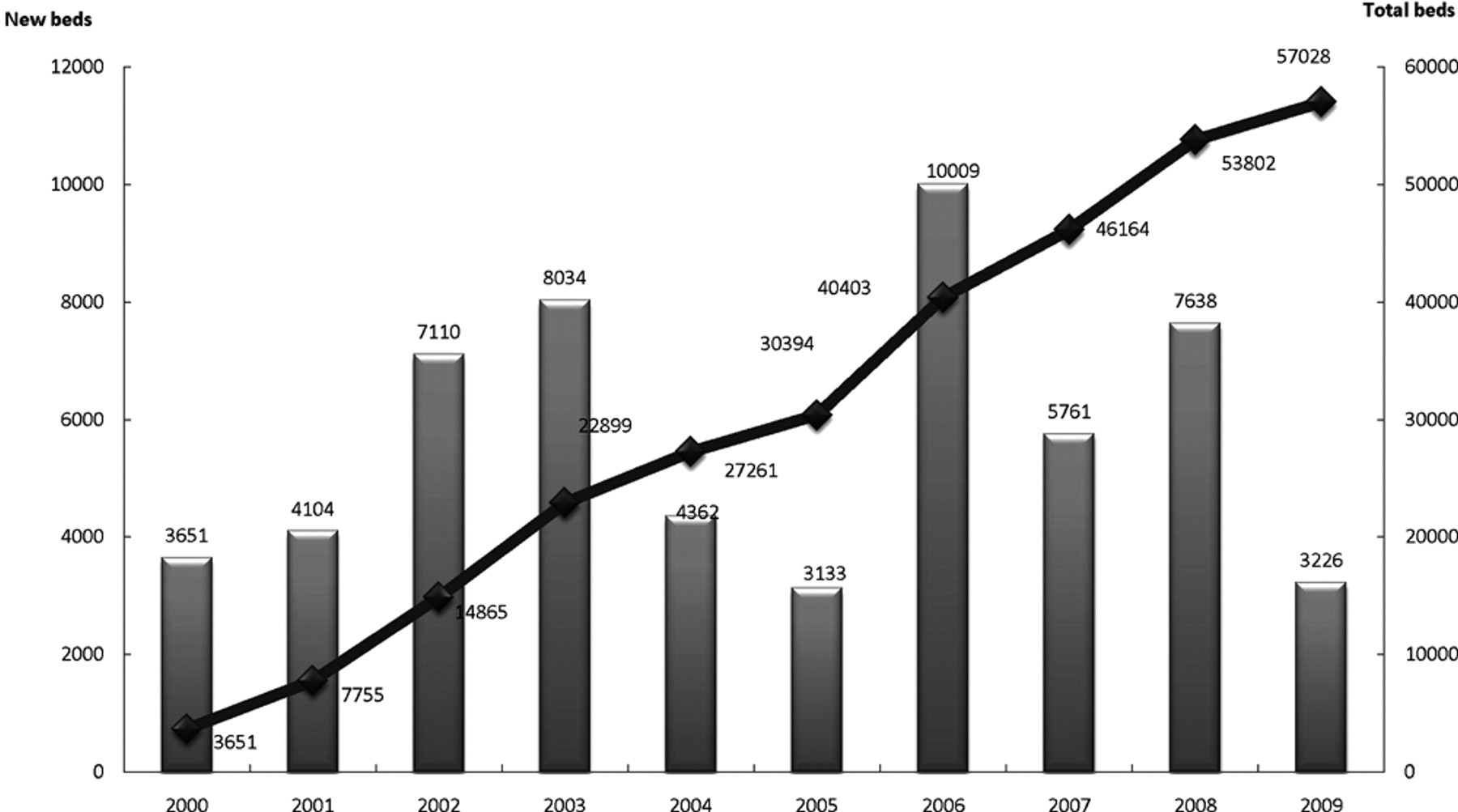
Number of beds in Kaifukuki rehabilitation wards (KRWs; there has been a constant increase in the number of KRW beds).
There have been several changes in the insurance policy for the KRW. Initially, patients within 3 months after the onset of disabling diseases, including stroke, traumatic brain injury, and other neurological diseases as well as orthopedic diseases such as hip fracture, were eligible for admission to the KRW. The maximal onset–admission interval (OAI) was shortened to 2 months in 2006 to facilitate earlier transfer to the KRW. Maximal coverage for inpatient rehabilitation increased from 2 hours up to 3 hours per day in 2006. These decisions were made based on accumulating evidence that early and intensive interventions improve rehabilitation outcome. 1-6 Currently, the maximal LOS covered by the insurance is 150 days for stroke, 180 days for stroke and other neurological diseases with severe disability and cognitive disorders, and 90 days for orthopedic diseases and the disuse/myopathy syndrome. Accordingly, the maximal duration of coverage, including acute and postacute inpatient care, for patients with severe stroke is 8 months after onset. 14 The KRW, comparable with IRFs in North America and Europe, includes extended coverage of inpatient rehabilitation up to 180 days after stroke and 3 hours of rehabilitation per day, including weekends (21 hours per week).
Because there is no similar rehabilitation system in the world in terms of LOS and intensity of rehabilitative interventions, we describe how the KRW has contributed to improving the functional outcome of patients as it has evolved.
Methods
We retrospectively analyzed 87 917 patients from the database of the annual survey for the KRW from 2001 through 2008. The data included adult patients (≥16 years old) who were discharged from a KRW in August and September each year after more than a 6-day stay on the ward. Data sheets were sent to the member hospitals of the KRW association. They were required to provide demographic data of patients; dose of rehabilitation; outcome measures, including either the Barthel Index (BI) 15 or the Functional Independence Measure (FIM) 16 ; discharge disposition; and LOS. The data collection rate improved year by year, from 46.8% (2001) to 64.1% (2009) of KRWs nationwide.
In addition to changes of maximal OAI and rehabilitation coverage in 2006, the policy introduced an incentive for KRWs that admitted severely disabled patients, who represented more than 15% of total patients and whose rate of home discharge was more than 60% in 2008. Influences of these changes of policy on outcome measures were analyzed. Because hospitals with a KRW included in the survey differed across the years, we identified the 110 hospitals that consecutively participated in the survey from 2006 to 2009. We also analyzed the serial changes of rehabilitation outcome in this hospital group.
Longitudinal changes of demographic data and outcome measures were analyzed using 1-way analysis of variance (ANOVA) or χ2 tests as applicable. Assessment of the effect of augmented therapy dose on functional outcome used a multiple stepwise regression model. Statistical analyses were performed using SPSS version 18.0J (SPSS Inc, Chicago, Illinois). Statistical significance was set at P < .05.
Results
General Description
The mean (standard deviation [SD]) age of all patients was 73.0 (13.8) years, and 55.0% were women. Age (F 8,87 908 = 102.9; P < .001) and the proportion of women (P < .001) were significantly higher in recent years (Table 1). Diagnostic categories were stroke (47.9%); orthopedic diseases, including hip fracture and disuse myopathy (35.2%); and neurological diseases, including traumatic brain and spinal cord injury (5.3 %). The proportion of stroke decreased and that of orthopedic diseases increased year by year (P < .001).
Clinical Characteristics of Patients Admitted to KRWs
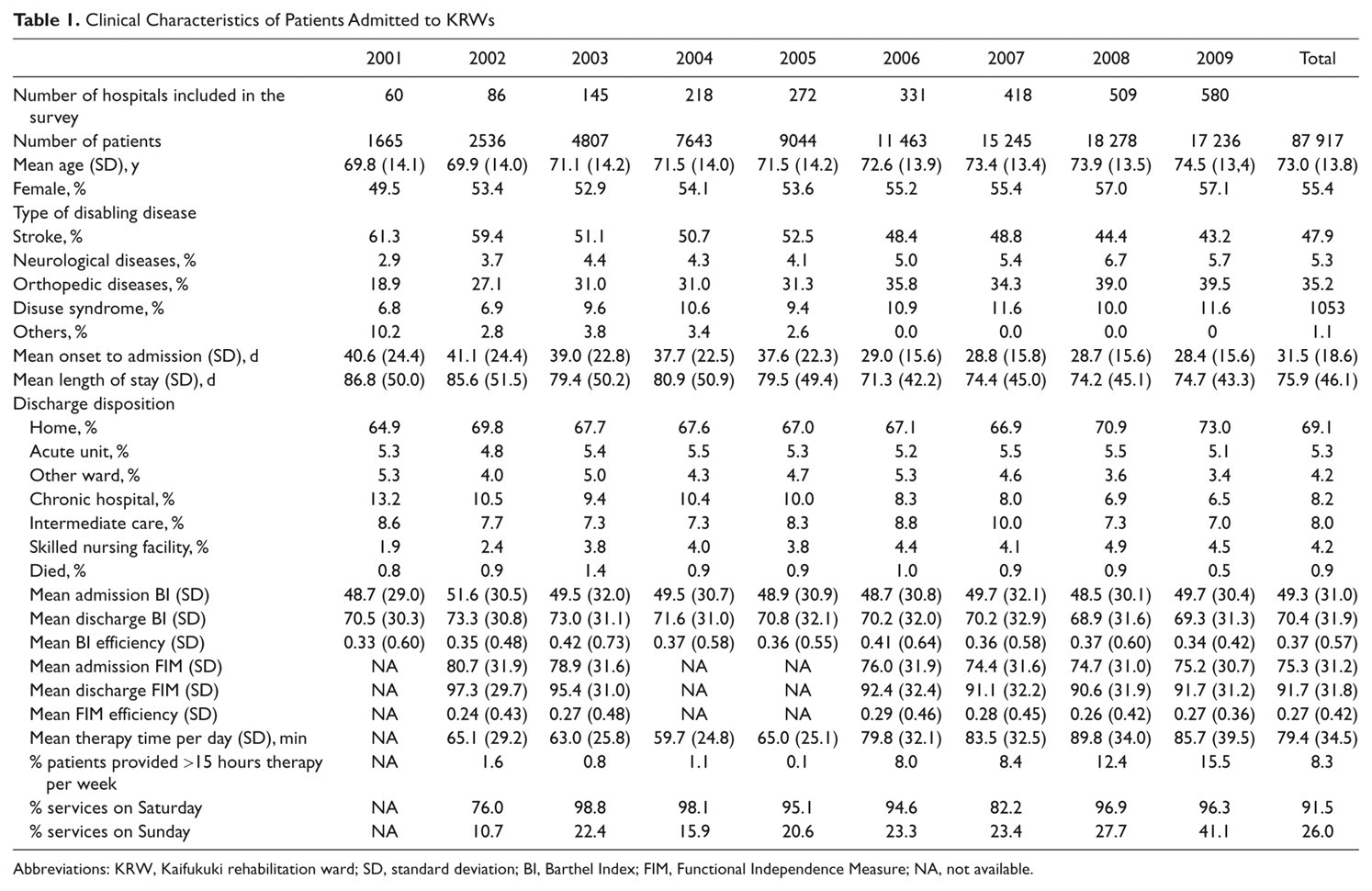
Abbreviations: KRW, Kaifukuki rehabilitation ward; SD, standard deviation; BI, Barthel Index; FIM, Functional Independence Measure; NA, not available.
Mean OAI (SD) and LOS were 31.5 (18.6) and 75.9 (46.1) days; 69.1% of patients were discharged home. The policy change for maximal OAI in 2006 resulted in significantly shorter OAIs (ie, shorter LOSs in acute hospitals; F 8,87 908 = 675.5, P < .001) and LOSs (F 8,87 908 = 68.3; P < .001). The dose of rehabilitation is expressed as the total time spent in physical, occupational, and speech therapy sessions per day in Table 1. The increase of maximal coverage for therapy in 2006 produced a significantly higher dose of therapy thereafter (F 7,77 432 = 1106.289; P < .001). Consequently, augmented therapy of more than 15 hours per week was provided to 15.5% of patients in 2009. In terms of weekend intervention, 96.3% and 41.1% of KRWs provided therapy sessions on Saturdays and Sundays in 2009 (Table 1).
Mean (SD) scores of admission/discharge BI and FIM were 49.3 (31.0)/70.4 (31.9) and 75.3 (31.2)/91.7 (31.8), respectively (Table 1). Patients with severe disability were prominent in recent years both on admission (F 5,46 039 = 14.9; P < .001 for FIM) and discharge (F 5,46 039 = 16.4; P < .001 for FIM). The policy change in 2008 resulted in higher rate of home discharge in spite of more patients with severe disability (Table 1).
Analysis of Stroke Data
Age of patients with stroke was significantly higher (F 8,41 959 = 23.1; P < .001) in recent years, and the proportion of males was consistently high (Table 2). The policy change in 2006 resulted in significantly shorter OAIs (F 8,41 959 = 379.8; P < .001). LOS shortened in 2006 but significantly increased in 2008 and 2009 (P < .001). The increase of maximal coverage for therapy in 2006 led to greater doses of therapy thereafter (F 7,36 709 = 889.7; P < .001). Therapy for more than 15 hours per week was provided to 24.6% of patients in 2009. The number of patients with severe disability increased in recent years both on admission (F 5,21 894 = 7.7; P < .001 for total FIM) and discharge (F 5,21 894 = 8.6; P < .001 for total FIM). Similar changes were also seen in admission/discharge scores of the motor component of the FIM (F 5,21 894 = 8.1; P < .001/F 5,21 894 = 8.4; P < .001). The policy change in 2008 resulted in a higher rate of home discharges in spite of there being more patients with severe disability (Table 2).
Clinical Characteristics of Patients With Stroke Admitted to KRWs
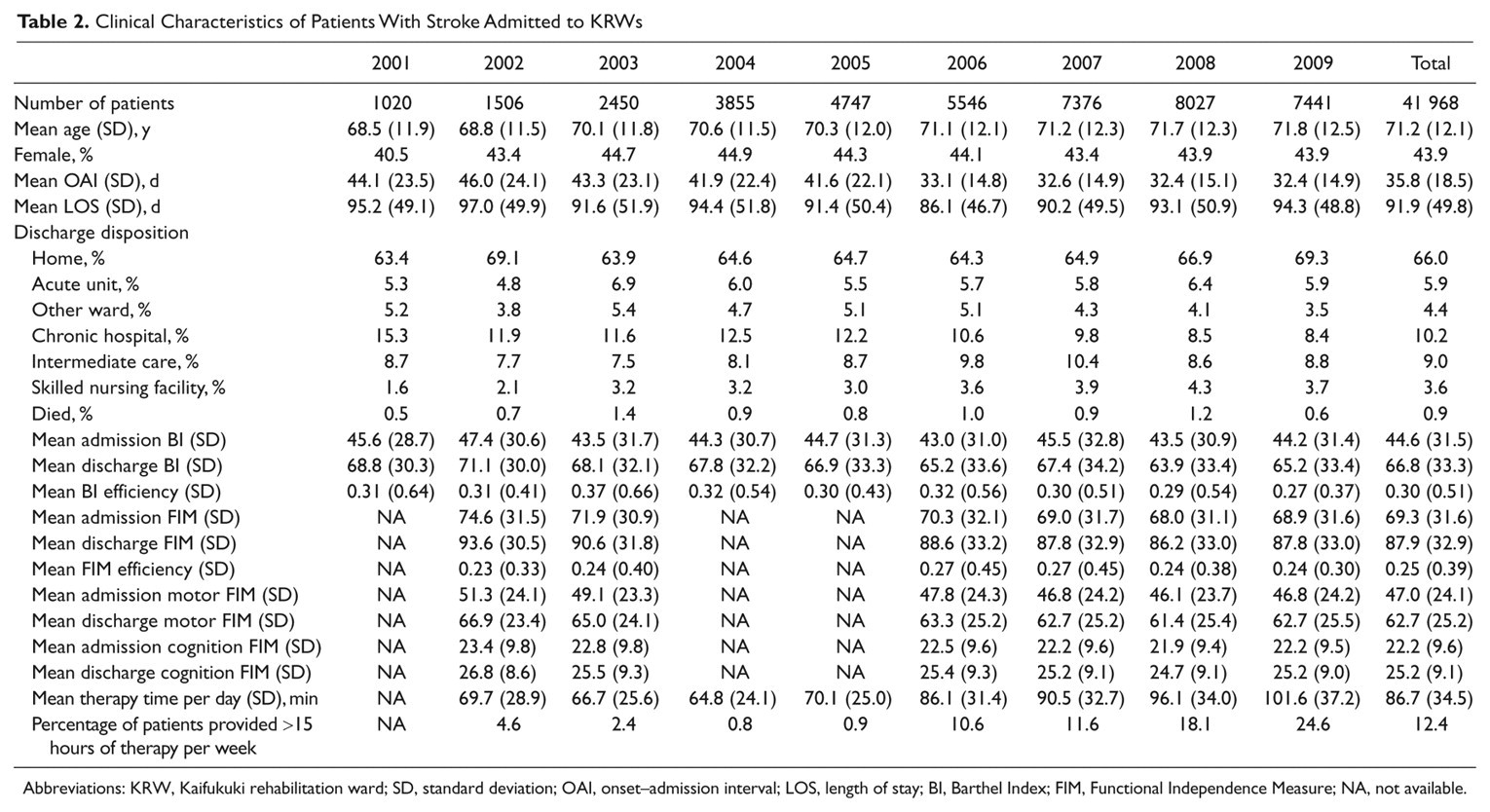
Abbreviations: KRW, Kaifukuki rehabilitation ward; SD, standard deviation; OAI, onset–admission interval; LOS, length of stay; BI, Barthel Index; FIM, Functional Independence Measure; NA, not available.
Analyses for Serial Data From the Identical Hospital Group
To investigate whether augmented therapy time affected functional outcome, we analyzed serial data of patients with stroke (n = 10 078) from the very same hospitals that consecutively participated in the survey from 2006 to 2009 (Table 3). A year-by-year comparison revealed that OAI significantly decreased (F 3,10 074 = 4.1; P < .01), whereas LOS significantly increased (F 3,10 074 = 17.8; P < .001). In terms of dose of intervention, therapy time (F 3,9414 = 265.3; P < .001) and rate of patients who were provided more than 15 hours of therapy significantly increased (P < .01). For the FIM, the total (F 3,9745 = 5.1; P < .05), motor (F 3,9745 = 3.4; P < .05), and cognition (F 3,9745 = 3.7; P < .05) scores on admission and the total (F 3,9745 = 5.2; P < .005) and motor (F 3,9745 = 6.0; P < .001) scores on discharge were significantly different among the years. However, post hoc Bonferroni testing failed to show consistent yearly changes in these measures. Of note, the gains of total FIM scores were significantly greater in 2009 than in 2006 (P < .001) and 2008 (P < .005), although FIM efficiencies were unchanged. The data also revealed that significantly more patients were discharged home in 2009 (P < .01).
Rehabilitation Outcome of Patients With Stroke From the Hospitals That Consecutively Participated in the Survey From 2006 to 2009
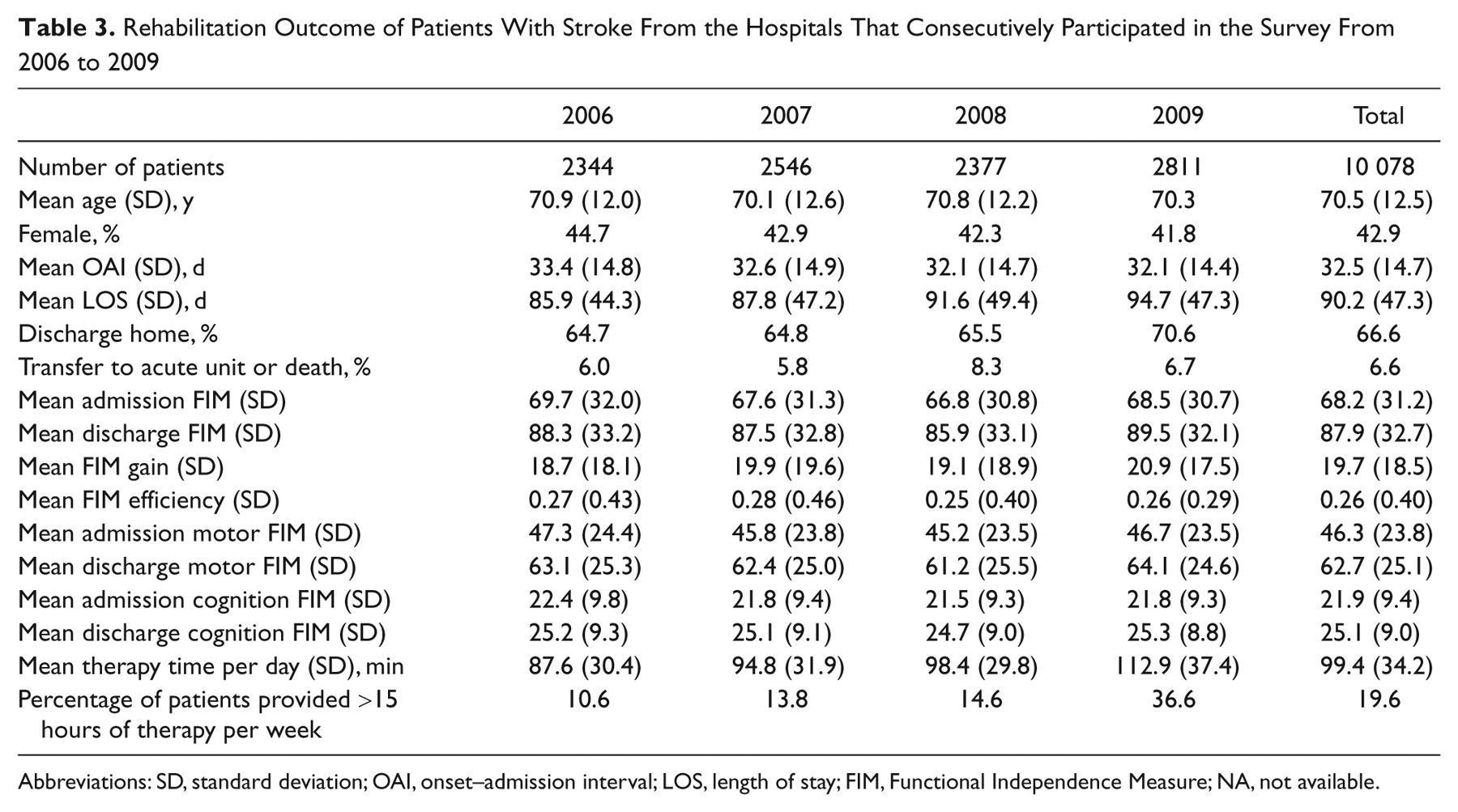
Abbreviations: SD, standard deviation; OAI, onset–admission interval; LOS, length of stay; FIM, Functional Independence Measure; NA, not available.
Thus, to test whether augmented therapy influenced functional outcome, we performed a stepwise multiple regression analysis. The model indicated that the discharge FIM score was significantly affected by daily therapy dose as well as the admission FIM score, OAI, and LOS (Table 4). However, compared with the effect of admission FIM score (87.1%), the effect of therapy dose was minor (3.6%).
Stepwise Multiple Regression Analysis for Discharge FIM Score a
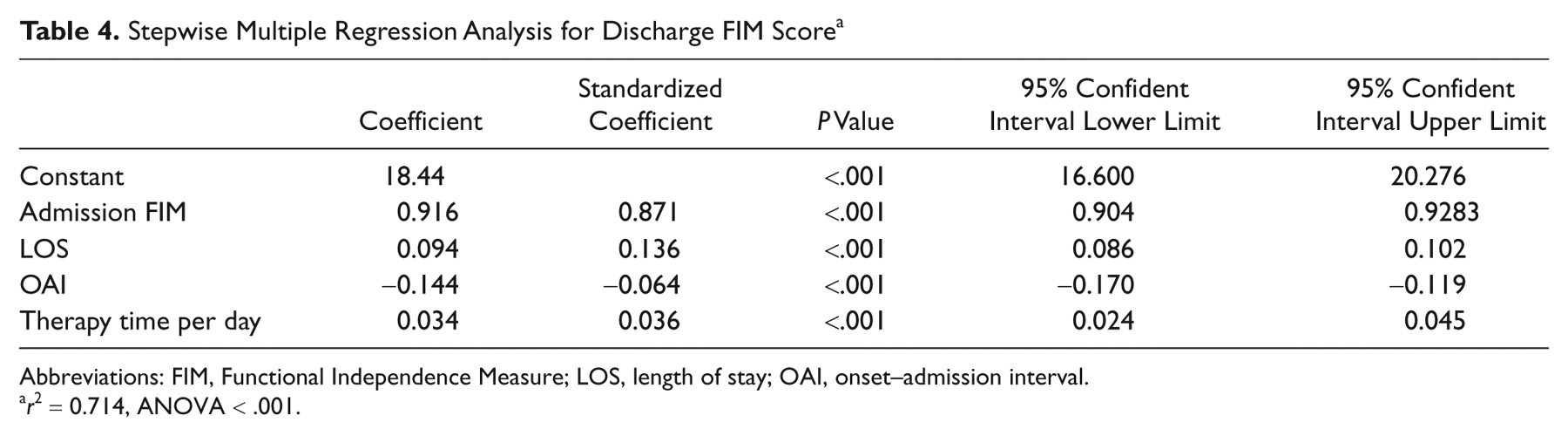
Abbreviations: FIM, Functional Independence Measure; LOS, length of stay; OAI, onset–admission interval.
r 2 = 0.714, ANOVA < .001.
Discussion
This retrospective analysis of rehabilitation outcome of the KRW system revealed that OAI, LOS, therapy dose, and discharge disposition have been significantly modified by changes in the national insurance policy in Japan. Outcome measures, including BI, FIM scores, LOS, and discharge disposition have significantly changed year by year. The OAI significantly decreased in 2006 because a new policy encouraged earlier admissions. However, in patients with stroke, LOS lengthened in recent years, probably because policies encouraged the admission of more severely disabled patients who needed a longer time to reach a plateau before discharge. Increased therapy coverage as well as an incentive for discharge home induced an improved rate of home discharge, in spite of the increased number of severely disabled patients. There was a time lag between the policy change for increased coverage for rehabilitation time and the resulting increase in actual rehabilitation time because KRW hospitals needed to employ new therapists to provide more therapy sessions. As of 2009, only 15.5% of patients were provided more than 15 hours of therapy per week, but the rate is expected to increase in the coming years.
Thus, national rehabilitation system policies are a major determinant of inpatient rehabilitation outcomes. The effects, however, are still being studied. For example, the overall effect of providing a higher dose of therapy on outcome measures is probably obscured by the considerable number of new KRWs added to the survey every year. Most newly recruited hospitals provide less organized rehabilitation than those that are more experienced and organized. The quality of rehabilitation care is probably still heterogeneous across KRWs. We tested for a dose-dependent effect on functional outcome in those hospitals that were consecutively involved in the survey from 2006 to 2009. Stepwise multiple regression analysis revealed a small but significantly positive effect of therapy dose on discharge FIM score. Although the effect was small and initial functional status was the main predictor of outcome, 17 this observation is in accordance with several studies reporting the effect of therapy dose on functional outcome. 18-20
In terms of type of disabling diseases, the proportion of stroke decreased and that of orthopedic diseases increased year by year (P < .001). This indicates that the total number of beds for patients with stroke has sufficiently increased in recent years to manage demand. The KRW association has set the target number of KRW beds as 50 beds per 100 000 population based on an incidence of stroke in Japan of 200 per 100 000, with half of the patients needing transfer to a KRW after acute therapy (100 per 100 000). Taking into account other diseases, the target number of beds is 50 per 100 000. At present, prefectures range from 22 to 130 beds per 100 000 population.
Limitations of the Study
More detailed data, including type of stroke, location of lesion, and complications during the hospital stay, are not available. We did not make these data mandatory because of the burden on sites. A more precise description of patient features may be necessary to evaluate who will most benefit from this system and to improve the quality of the KRW organized rehabilitation system. FIM efficiency was not as high as that of IRFs in the United States 7 mainly because of later admissions and longer stay. 21 This property of KRWs may cause less sensitivity to detect dose-dependent effects of hours of therapy and types of therapies.
In 2010, a new incentive has been given to KRWs that provide more than 14 hours of therapy weekly and also weekend therapy. Wards that provide less than 280 minutes of therapy per week were no longer eligible to be a KRW in 2010. These changes of policy may induce bottom-up changes in quality and intensity of services.
Conclusions
The KRW is a Japanese solution to the increasing number of elderly people who need inpatient rehabilitation after acutely disabling diseases. Longitudinal data suggest that national policy changes directly influence inpatient rehabilitation services and outcomes, with better results for patients. Consequences will be continuously monitored for future reports.
Footnotes
Acknowledgements
We thank the other members of Annual Survey Committee of Kaifukuki Rehabilitation Ward Association (Shinsuke Goto, Toshio Ohta, Isao Ito, Shin-ichi Yamamoto, Yasuki Takizawa, and Katsuyuki Kako) for their contribution to the survey. We also thank all member hospitals of KRW association for submitting precise data for the annual survey.
Part of the material in the manuscript was presented at the 6th World Congress of Neurorehabilitation; March 21, 2010; Vienna, Austria.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.