
Abstract
Background
Most of the current literature around amputation focuses on lower extremity amputation or engineering aspects of prosthetic devices. There is a need to more clearly understand neurobehavioral mechanisms related to upper extremity amputation and how such mechanisms might influence recovery and utilization of prostheses.
Objective
This scoping review aims to identify and summarize the current literature on adult traumatic upper limb amputation in regard to recovery and functional outcomes and how neuroplasticity might influence these findings.
Methods
We identified appropriate articles using Academic Search Complete EBSCO, OVID Medline, and Cochrane databases. The resulting articles were then exported, screened, and reviewed based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) guidelines.
Results
Eleven (11) studies met the study criteria. Of these studies, 7 focused on sensory involvement, 3 focused on neuroplastic changes post-amputation related to functional impact, and 1 study focused on motor control and learning post-amputation. Overall, these studies revealed an incomplete understanding of the neural mechanisms involved in motor rehabilitation in the central and peripheral nervous systems, while also demonstrating the value of an individualized approach to neurorehabilitation in upper limb loss.
Conclusions
There is a gap in our understanding of the role of neurorehabilitation following amputation. Overall, focused rehabilitation parameters, demographic information, and clarity around central and peripheral neural mechanisms are needed in future research to address neurobehavioral mechanisms to promote functional recovery following traumatic upper extremity amputation.
Introduction
Nearly 185 000 amputations occur in the United States each year, resulting in approximately 2 million Americans living with limb loss today.1,2 The main causes of limb loss include trauma, vascular disease, and cancer. 1 In the current literature, there is a well-known lack of research on upper extremity amputation compared to lower extremity amputations. In November 2021, a search for “upper limb amputation” in PubMed, results in a total of 7794 articles compared to “lower limb amputation” which results in 19 022 articles.
For most amputees, the use of prostheses can be a way to support improvements in daily living. 3 Unfortunately, upper limb amputees have high rates of prosthesis rejection ranging from 16 to 66%. 4 Furthermore, upper limb prostheses are commonly used for non-functional aesthetic purposes. 5 Given the state of amputation rehabilitation, it is helpful to gain a clearer vision of the present state of the literature in upper limb amputation to identify important concepts to support patient-centered rehabilitation needs.
In order to gain a better understanding of the current state of rehabilitation research in adults with traumatic upper extremity amputation, this review seeks to (1) identify and summarize the current body of rehabilitation research and its relation to functional outcomes and recovery, (2) identify and summarize what populations of people are represented in the current body of research, and (3) identify how neural plasticity has been considered in relation to 1 and 2.
Four main hypotheses were formulated. First, it was hypothesized that limited research would be available regarding the current state of neurorehabilitation research in upper limb loss. This is based on the assumption that the lack of rehabilitation protocol development for persons with upper limb loss is due to lack of available research. Second, it was hypothesized that research conducted by the US Department of Veterans Affairs (Veterans Affairs Medical Centers, VAMC) would provide be the most common patient population found in the literature due to high incidence of amputation 6 and have well-established systems of care for persons with limb loss. 7 Evidence suggests that such strong systems of care with multidisciplinary treatment approaches are optimal for neurorehabilitation outcomes after upper limb amputation.8,9 Third, it was hypothesized that there would be minimal focus on the role of the rehabilitation team (eg, physiatry, physical/occupational therapists) involved in patient care in the studies found. This is, in part, driven by the first hypothesis and the lack of clear knowledge around neurobehavioral aspects of upper extremity amputations. Such knowledge usually precedes the establishment of rehabilitation protocols. Lastly, it was hypothesized that any treatment or intervention mentioned in the current literature would be highly individualized to the characteristics of the patient.
Methods
Scope of Search
In this scoping review, peer-reviewed articles were extracted from three databases including Cochrane, Academic Search Complete EBSCO, and OVID Medline. These databases were chosen for their comprehensive journal repository databases with peer-reviewed literature. We did not utilize databases that might have citations of grey literature (eg, Google Scholar).
Study Selection
EBSCO host, OVID Medline, and Cochrane were searched using the following search terms: (upper limb OR upper extremity OR upper quarter) AND (amputation OR amputee OR limb loss) AND (rehabilitation OR therapy OR recovery) AND (structural changes OR neural OR functional changes OR neuroplasticity OR neural plasticity). This included publications listed to these search engines between 1980 and 2020, with a final publishing data of September 28, 2020. The resulting articles were then exported to EndNote (Clarivate, London, UK) where duplicates were removed and then to Covidence (Melbourne, Australia) where the articles were screened using PRISMA guidelines for Scoping Reviews (PRISMA-ScR). 10 Our protocol was reviewed internally by Emory University School of Medicine and Georgia Tech.
A total of 3 reviewers independently screened all articles at 2 different screening checkpoints. Both screening checkpoints were administered and tracked using Covidence. Our search strategy generated a total of 183 papers, and 4 duplicates were removed. In order for a study to pass a screening checkpoint unanimous agreement was necessary by all 3 reviewers. The first screening checkpoint was the title/abstract screening and the second screening checkpoint was full text screening. In the first screening checkpoint, 103 articles were excluded. In the second screening checkpoint we excluded 64 articles for the following reasons: international (25), engineered device/control focus (17), review articles (9), non-traumatic (congenital) amputation (7), lower limb amputation (2), inability to access article (2), published prior to 1980 (1), and survey study (1). This process resulted in twelve (12) papers that adhered to all exclusion and inclusion criteria. One final paper was removed due to no persons with upper limb loss used as participants, leaving a total of 11 papers for the final review (Figure 1). All manuscripts were published in peer-reviewed journals. Reference lists were scanned which failed to reveal any additional citations. (a) PRISMA via Covidence and (b) inclusion and exclusion criteria used in the study during full text screenings.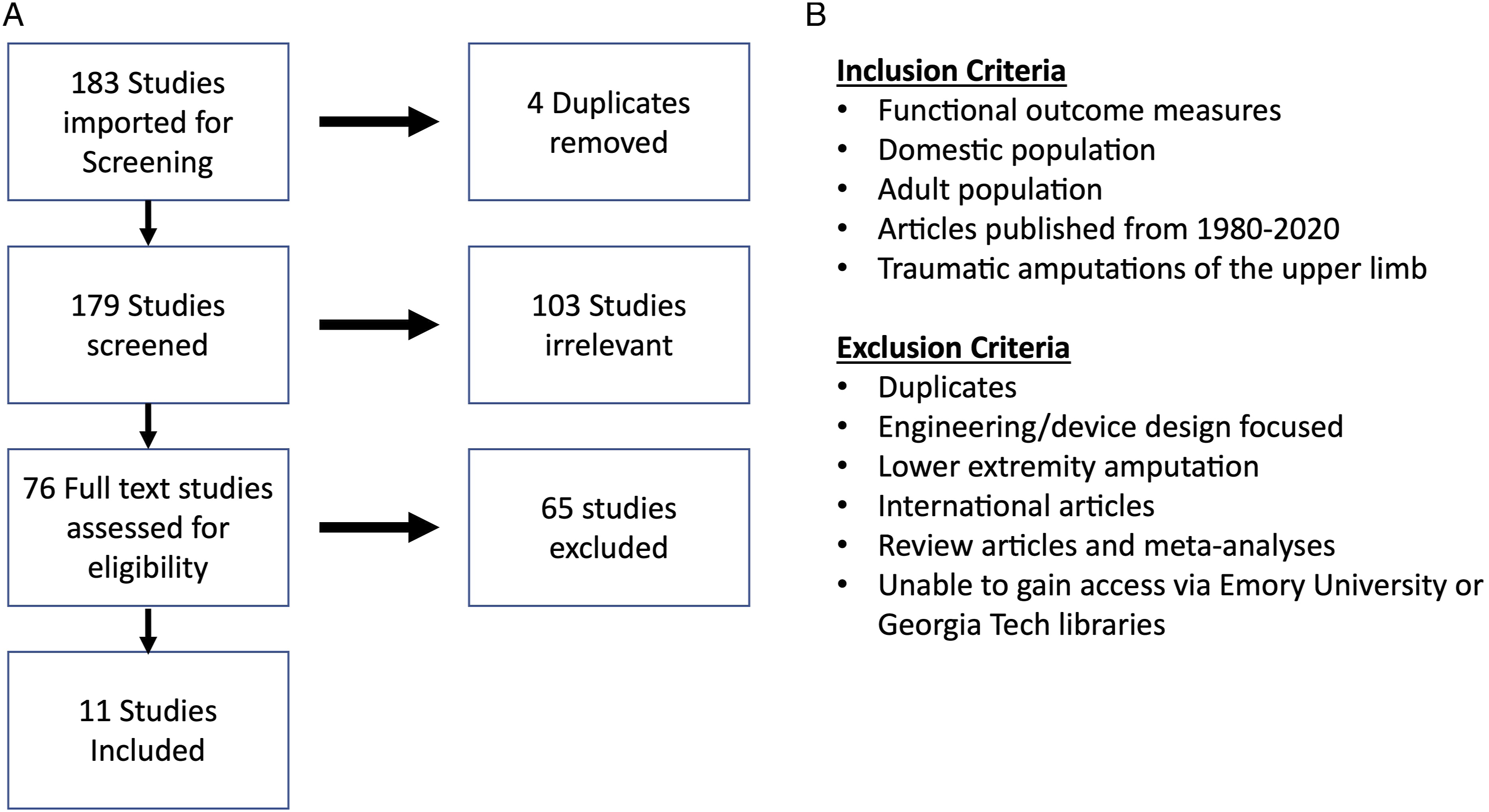
The decision to exclude international articles is due to differences within international healthcare and insurance systems that have direct relevance to impact various factors of our studies. According to the World Health Organization (WHO), the healthcare systems present in different countries are “strongly influenced by the underlying norms and values prevailing in the respective societies.” 11 As well, the causes of amputation and demographics can differ dramatically between countries12,13 which could influence results. According to the US Census, approximately 92% of the US population is covered by insurance, with 68% on private plans and 34% on public plans (Medicare, Medicaid, or Veterans Affairs). 14 Research has suggested structural differences in neuromotor rehabilitation between healthcare systems in the United States and Europe, which can significantly impact outcomes. 15 In the United States, persons from vulnerable populations (lower median income and reliance on Medicaid or with no insurance) have a greater likelihood of amputation, 16 with status as an ethnic monitory being a crucial variable.17,18 Due to these differences in healthcare structure, quality, and demographics, it was concluded that international articles would be inappropriate to include as functional outcomes, course of care, and populations receiving care may differ significantly.
Development of Concepts
Concept 1: Evaluate the impact of rehabilitation structures and therapy on functional outcomes and recovery
The aim of Concept 1 was to outline the existing research regarding rehabilitation processes following a traumatic upper extremity amputation and how rehabilitation may impact functional outcomes and recovery with prostheses measured by outcome measures or subjective assessment.
Concept 2: Populations of people represented in the current body of research
The aim of Concept 2 was to summarize the demographics of individuals with amputation involved in amputation research in the United States and if there were any gaps in populations being studied.
Concept 3: How neural plasticity has been considered in relation to both 1 and 2
The aim of Concept 3 was divided into two parts. The first part was to identify how central and peripheral neural mechanisms have been considered in current research following an upper extremity amputation. Cross examining these results, the second part was to identify how studies addressed interactions of sensory and motor function in order to evaluate central and peripheral relationships with neuroplasticity.
Results
Concept 1: Evaluate the impact of rehabilitation structures and therapy on functional outcomes and recovery
Rehabilitation structure
Of the eleven articles included in this review four studies mentioned the use of a rehabilitation professional in the use and training with adults of upper limb amputation. Three studies included that the participants partook in occupational therapy sessions19-21; however specific parameters and protocols were not included. Kuiken et al described the use of “3 months of weekly OT” for the study’s participants, 21 while Lipschutz et al 20 stated participants had “several weeks” of OT. Resnick et al described the use of virtual reality and a “standard training protocol” 19 that consisted of progression of functional tasks which began with grasp and release of variously sized and shaped objects, followed by more complex functional activities, and lastly progressed to body-centered training all led by an OT. Only one study mentioned participants completing physical therapy sessions and described the sessions as including: active range of motion (ROM) of shoulder within normal limits in all degrees of motion, as well as manual muscle testing grades. 22 The length and specific protocols used in physical therapy sessions were not explicitly stated in this study. Overall, it is unclear how well integrated the rehabilitation environments are in these studies.
Although there were few studies that discussed the use of professional rehabilitation training, the use of “training” or “practice” was mentioned in five out of the eleven studies.19-21,23,24 Of those five studies, three included the use of a rehabilitation professional as described above.19-21 The descriptions of the training or practice varied significantly between each study. Akhtar et al 24 only mentioned the implementation of repetitive reaching testing trials including 48 reaches for participant practice for training and testing. Resnik et al 19 described the use of training participants to “generate appropriate muscle activation patterns,” stating one participant received seven hours of training on pattern recognition (PR) device use, while the other participant received 11 hours of training on direct control (DC) device use, and 12 hours of training on PR device use. Participants in Lipschutz et al 20 received “several weeks of occupational therapy learning the various operations of the prosthesis.” Information from that occupational therapist was then shared with the participants local OT so additional training could continue when they returned home. Schabowsky et al 23 included visual feedback to encourage peak velocities for reaching tasks, and included 30 trials of reaching movements to allow for familiarization. Then the participant performed 120 more trials considered the “training condition” which included perturbations. In Kuiken et al, 21 the participant received daily training over a 2-week period and was sent home for 5 weeks to practice with prostheses before testing began. The participant was also allowed practice trials of each test for “several minutes” before recording data of the subject’s performance.
Functional outcomes
Functional outcomes used in each study.
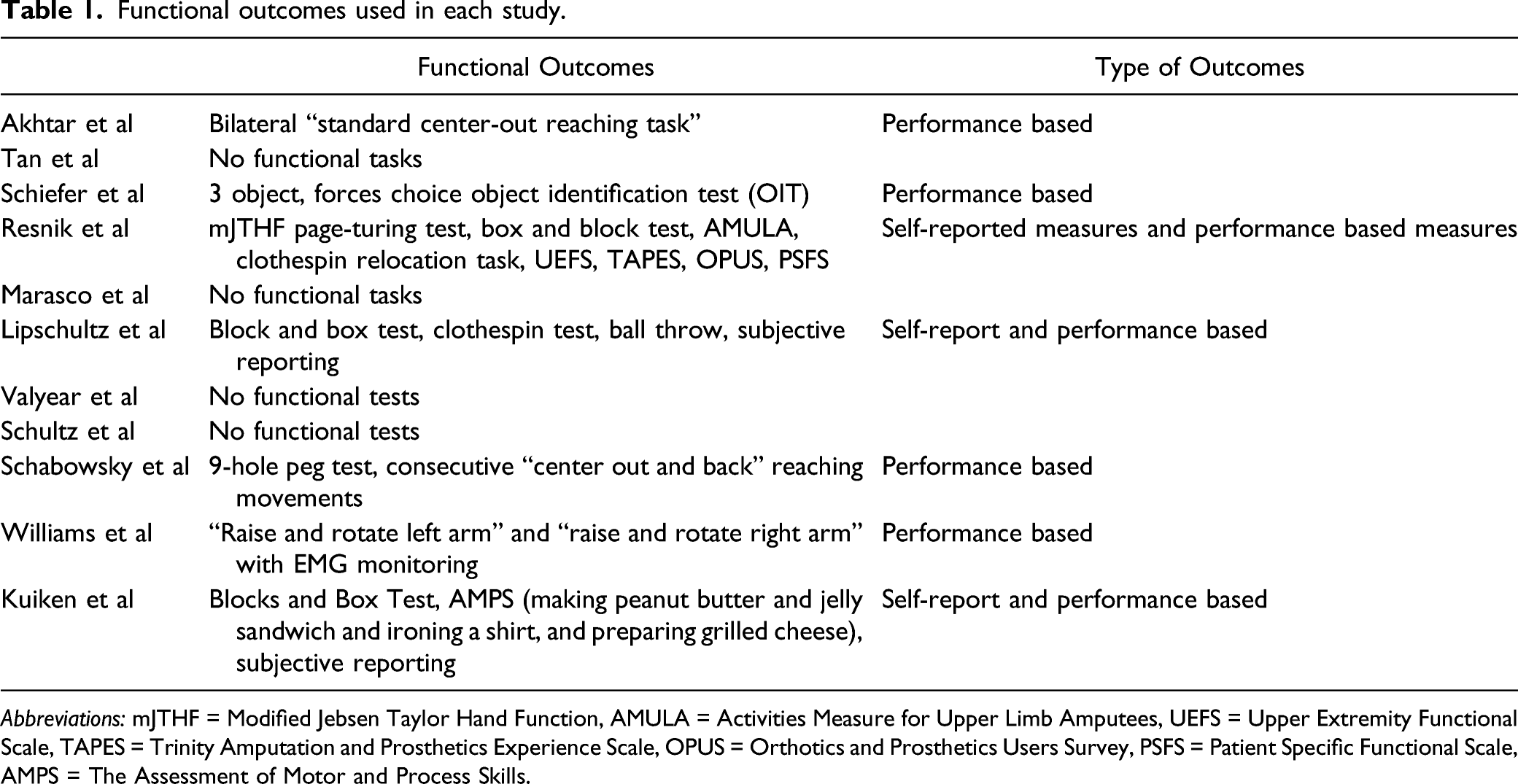
Abbreviations: mJTHF = Modified Jebsen Taylor Hand Function, AMULA = Activities Measure for Upper Limb Amputees, UEFS = Upper Extremity Functional Scale, TAPES = Trinity Amputation and Prosthetics Experience Scale, OPUS = Orthotics and Prosthetics Users Survey, PSFS = Patient Specific Functional Scale, AMPS = The Assessment of Motor and Process Skills.
Concept 2: Populations of people represented in the current body of research
Clinical setting
It was hypothesized there would be a predominance of studies performed in the VAMC setting in the reviewed publications. The available literature suggests this a misconception, as a minority of publications screened mention military/veteran cases. Specifically, 10 of the 46 total participants (21.7%) found in all 11 studies were noted to be part of a study conducted in the VAMC setting.23,25,26 It is difficult to make strong conclusions about whether participants outside of the VAMC setting were Veterans, as this was not noted in the non-VAMC studies.
Sample sizes
The number of participants in each study ranged from 1 to 19 persons with upper limb loss. The most common number of participants (mode) was 2 persons with upper limb loss (in 4 of the 11 publications reviewed, see Table 1). The age of participants ranged from 24 to 70 years of age, with middle-aged persons with upper limb loss being the most represented. A majority of the population represented in the literature appears to be male, with 28 male participants and 12 female participants (see Table 1). As for amputation level, there were 4 shoulder disarticulation, 17 transhumeral, 24 transradial amputations, and 1 partial hand amputation, with transradial amputations most reported. For context, partial hand amputation has been estimated to account for 92% of upper extremity amputations, while transradial amputations are the most common major upper extremity amputation. 27
Time since injury
Time since mechanism of injury (MOI) can impact interpretations of neurorehabilitation. Akhtar et al, Shiefer et al, and Schultz et al excluded information regarding time since MOI.24,25,28 Furthermore, Lipschutz et al 20 describes time since MOI as “shortly after,” does not quantify the interval. Overall, even though the chronological length of each study is documented in all cases, and most studies include time since MOI, there are few details that support drawing any conclusions about how time from MOI influences neuroplasticity or neural repair.
Prosthesis use history
Seven of the 11 studies mentioned prosthesis use in relation to their participants in some form. Of these 7, they discussed (1) the type of devices their participants were using prior to their study, (2) if they used their own devices during the study, (3) if new devices were utilized specifically for the study, and (4) if new devices were prescribed as a result of the study, or a combination of 1-4.
In Schiefer et al, 25 both their participants were to use their own myoelectric sockets with a prosthetic hand and their standard agonist/antagonist control scheme. Additionally, the prostheses these participants used during object identification had a single degree of freedom while the second and third digits were mechanically linked. Schabowsky et al 23 also elected to have all 8 participants use their own devices during data collection. This consisted of 6 body-powered prostheses with a split hook, 1 body-powered prosthesis with a hand, and 1 myoelectric prosthesis with a hook. Lastly, Williams et al 22 involved 5 participants who used their own devices during the study, including 4 body-powered prostheses with a split hook, and 1 iLimb. However, it was noted that these participants reported very infrequent use of their devices in daily life. Resnik et al 19 did mention their participants originally used myoelectric prostheses. Specifically, the 46 year-old male had a manual wrist rotator and iLimb terminal device while the 27-year-old female had an iLimb terminal device. However, the researchers in this paper had the persons with limb loss use 2 degrees of freedom transradial prostheses with commercial wrist rotators and an active terminal device during testing.
Characteristics found in populations of persons with limb loss represented in all final 11 studies.
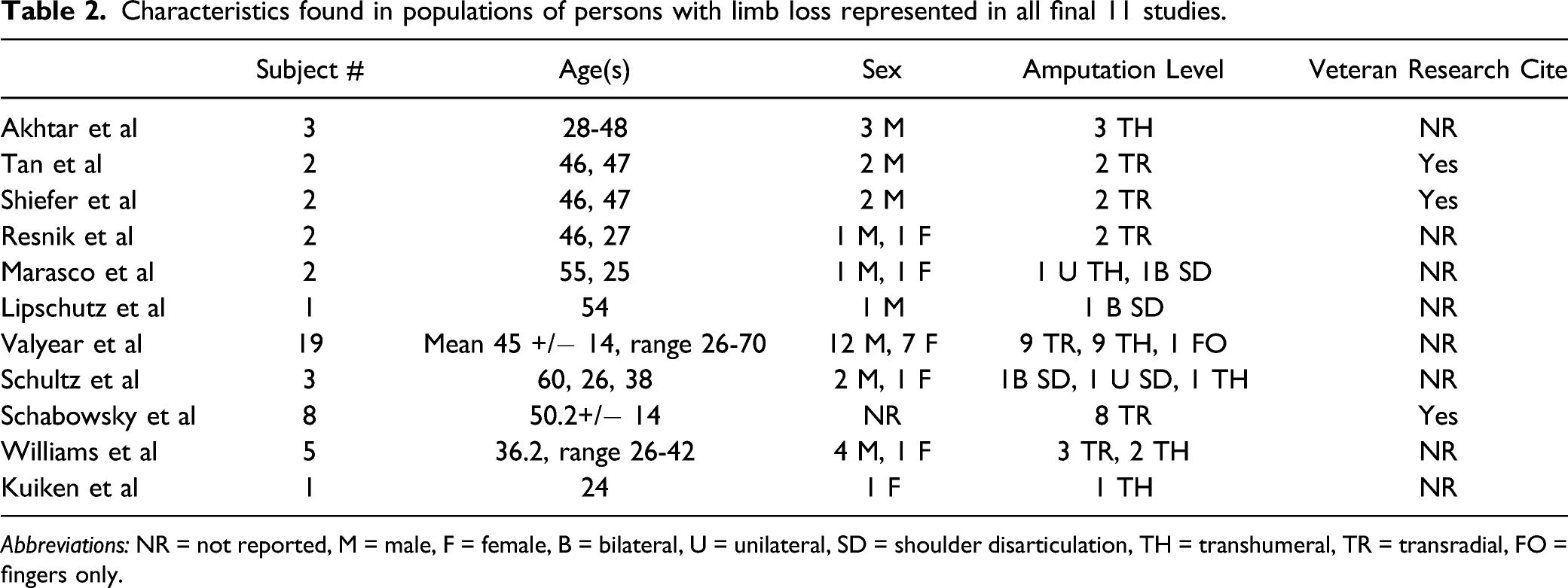
Abbreviations: NR = not reported, M = male, F = female, B = bilateral, U = unilateral, SD = shoulder disarticulation, TH = transhumeral, TR = transradial, FO = fingers only.
Phantom sensation
Characteristics of neuroplastic involvement within included studies; peripheral and/or centrally mediated, as well as sensory or motor driven. Recorded length of time between MOI and initiation of study/number of participants included for comparison.
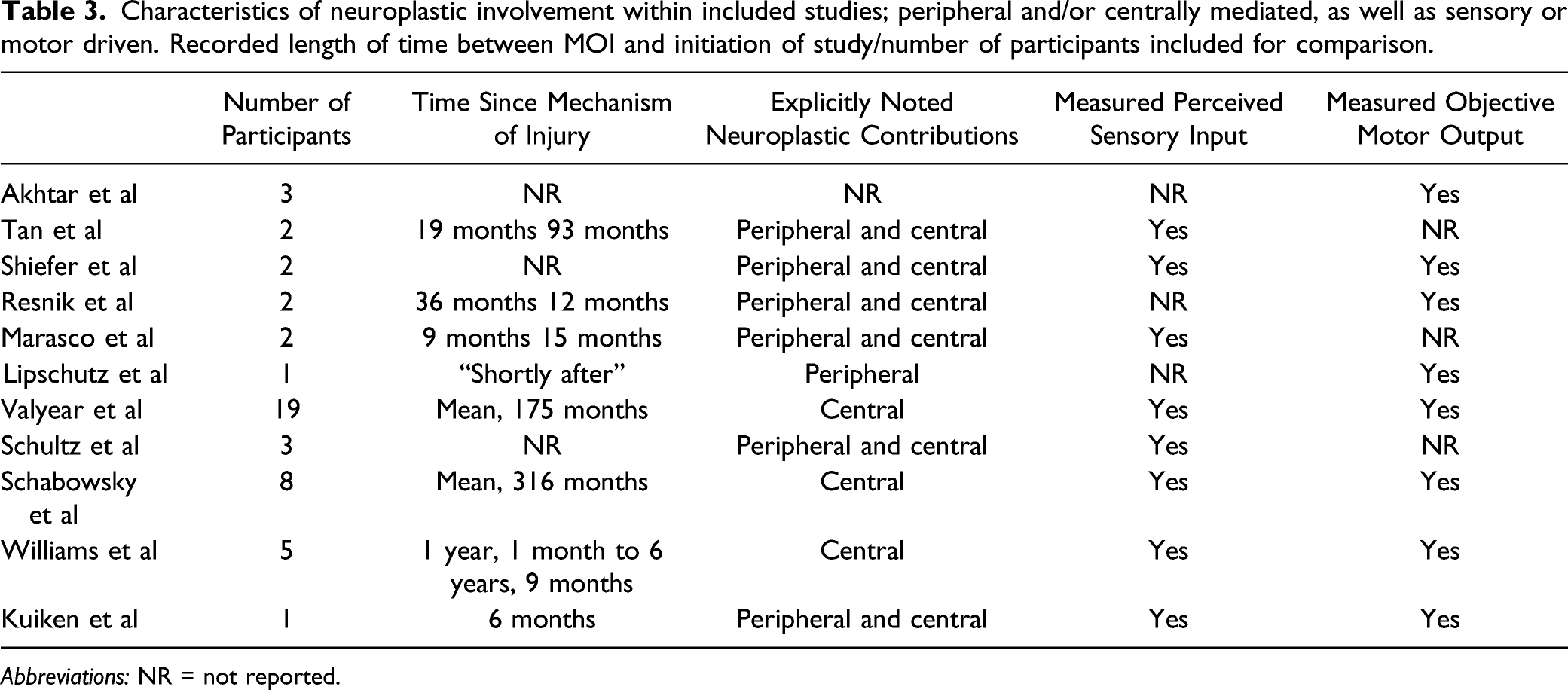
Abbreviations: NR = not reported.
Other identifiers
Certain critical metrics were not assessed in the identified studies. This includes ethnicity, socioeconomic status, insurance coverage, family support, home environment, and occupation.
Concept 3: How neural plasticity has been considered in relation to both 1 and 2
Upon investigation of the included literature, neuroplasticity has been represented in all but one study. Six discussed both peripheral and central neuroplastic contributions,19,21,25,26,28,30 while three only discussed central components,22,23,29 and two only discussed peripheral components20,24 in this population (Table 3).
Central mechanisms
Loss of afferent sensory information results in shifting cortical representation of the affected limb as well as the homotopic cortical area in the opposite hemisphere.22,29 Notably, Valyear et al 29 found that amputees showed greater activity in the former sensory hand area during stimulation of the intact hand, with no loss of tactile acuity. Crucially, these effects were unrelated to time since amputation, prosthesis use or pain. This suggests a persistent neuroplasticity that emerges following amputation which may endure. Cortical reorganization is thought to occur at two different time scales, an acute phase when reorganization is the result of unmasking latent neural circuits, and a delayed chronic phase of delayed reorganization perhaps due to axonal sprouting.34,35 The resulting effects include activation of ipsilateral motor and sensory areas when moving the intact hand, as seen in other studies.36,37 Williams, et al noted an expansion of sensorimotor areas to more posterior parieto-occipital regions when performing a reaching task with the amputated (right) limb, while use of their intact (left) arm demonstrated higher ipsilateral sensorimotor activity. 22 Such cortical changes have been associated with better performance on motor tasks with the intact hand, and are thought to be a functional adaptation.36,37 Overall, these changes in sensory representation do not affect the ability of participants to perform tasks with their affected limb.23,29
Unlike the proposed minimal impact of sensory reorganization, disuse of the amputated limb in activities of daily living (ADLs) does have a negative impact on the amputee’s ability to perform tasks using the affected limb with a prosthesis, as evidenced by performance on the nine-hole peg test. 23 Here, it was hypothesized that this could have been due to a role-reversal of the limbs post-amputation. Non-dominant limbs are thought to perform the role of stabilizer with dominant limbs performing dynamic aspects of a task. 38 With dominant limb amputation, the unaffected formerly non-dominant limb may become the functionally dynamic limb, causing the formerly dominant limb may take a different functional role. 22
Peripheral mechanisms
Of the papers identified, the peripheral nervous system is harnessed by TMR, where participants have the ability to excite axotomized nerves that previously innervated muscle and sensory receptors in amputated limbs. 20 When the axotomized nerves were used to innervate sectioned pectoral muscles, after a healing period the participants were able to initiate contraction of the muscles. This ability illustrates the retention of cortical viability in initiating efferent activity through the axotomized nerves. 20 Another study has shown that nerves used to innervate the pectoral muscles can also innervate the skin covering the muscle leading to perceived sensations formerly attributed to the now-missing hand. 21 Thus, while cortical reorganization is shown to occur due to deafferentation, viability of efferent and afferent nerve pathways to the periphery are retained. As the studies that dealt with peripheral mechanisms did so through the lens of sensory and motor systems, the next section will elaborate more on ascending and descending processes that relate to sensory and motor systems.
Sensory and motor outcomes
Measuring both sensory input and motor output is crucial to obtaining a holistic view of rehabilitation potential in amputation. Five of eleven studies analyzed both sensory and motor contributions21-23,25,29; however, only two studies, related these variables to both central and peripheral nervous systems.21,25 These two papers express common terms suggestive of an optimal approach toward rehabilitation research in this population. It is important to note the inclusion and/or exclusion of sensory and motor systems in current upper extremity limb loss literature, as both systems are necessary for purposeful human movement, and functional recovery.
Surgical reinnervation allowed Kuiken et al 21 to evaluate a custom prosthesis for simultaneous control of the hand, wrist and elbow. They found that 7 weeks after fitting and training, the patient improved in both motor and process scores, and performed significantly better compared to using a conventional myoelectric prosthesis. Another study found that patients exhibited greater functional performance and greater ease of use of a myoelectric prosthesis when operated via direct control compared to pattern recognition control, but the effect was not maintained at a 1-week follow-up. 19
When patients were exposed to artificial sensory feedback, task accuracy significantly improved, regardless of time since amputation. 25 Here, applied pressure feedback of tactile and proprioceptive information led to integration that supported improved object discrimination. This information originated via neural stimulation suggestive of remapping of sensory inputs that also helps to shape motor control (object manipulation and grasp confidence).
Patients have also demonstrated the perception of vibration, the differentiation of sharp and dull sensation, graded pressure, and temperature in their phantom hand. 21 These results were mimicked by Tan et al, 26 showing that surgical implantation of cuff electrodes on the median, ulnar, and radial nerves provided sensation response in the phantom limb, and were selective to pressure, vibration or tapping, and light moving touch, but sensation did not extend to proprioception. One reinnervation study exploring specificity found that a patient was able to orient gratings at thresholds similar to their contralateral normal side and controls and could even localize point stimuli more accurately on their reinnervated side compared to their contralateral normal side. 30 Another study found that after targeted reinnervation surgery, some patients showed vibration detection thresholds that were significantly higher than their contralateral chest, intact upper arm, forearm, and hand, and exceeded the 95% confidence intervals of healthy controls at certain stimulation frequencies. 28
Discussion
The goal of this scoping review was to identify and summarize the current literature on adult traumatic upper limb amputation in regard to recovery and functional outcomes, and how neuroplasticity might influence these findings. Overall, we were able to identify outcome-based research related to upper limb loss. There were few insights on neuroplasticity, and how it may impact rehabilitation. It was abundantly clear that insights into these remaining questions are limited, most notably due to variability around the goals of the studies, levels of amputation, and types of (and experience with) prostheses. This presents a challenge for any gold standard randomized clinical trial focused on persons with limb loss. An inherent limitation is the low number of qualified studies that were identified in this review.
While several of the identified studies harness the peripheral system with some degree of success, how the interaction of the central and peripheral systems change over time 39 and through the course of rehabilitation 40 remains unclear. While it is clear that amputation promotes motor and sensory changes at the cortical level that involve both hemispheres,22,29 it is unclear what this means for utilization of new technologies or rehabilitation to promote the use of prostheses. It remains unknown whether these cortical changes are truly maladaptive or can be harnessed to promote rehabilitation. 41 Research has argued that targeted reinnervation can support establishment of frontoparietal activity and connectivity to levels complementary to persons without amputation. 42 However, reinnervated motor units show smaller surface area and shorter action potential durations compared to persons without amputation 43 with similar patterns of synaptic input in reinnervated muscles as compared to persons without amputation. 44 This compels a stronger need to understand the interactions of central and peripheral nervous system before and during rehabilitation or surgical approaches to better understand how neural adaptations to amputation might influence central and peripheral structures. The link between time since MOI and neuroplasticity has yet to be determined and is a possible avenue for identifying peripheral or centrally mediated mechanisms post-amputation.
Although the data show increased scores on functional outcome measures in some of the included studies,19-21,23 the role that training or rehabilitative intervention plays remains unclear. Due to various factors influencing outcomes, including introduction of new prostheses, surgical interventions, and task practice and training throughout these studies, the true impact of training on functional outcome scores remains unclear. For example, assessment of neuroplastic changes both centrally and peripherally could provide further detail on the impacts of formal training on functional outcomes. Included studies did not always objectively measure neurologic changes in regard to training. Of those that did, it remains unclear whether improvements in functional outcomes or participant perception of improved function is linked to any specific neural mechanisms. 29
Implications for Future Research and Neurorehabilitation
Although the mechanism of injury, surgical intervention, level of amputation, intrinsic demographics, and environmental construct of each amputee varies, the scope used to analyze these variables toward human functional recovery could incorporate similar ideology between studies. To support comparisons of published results, formative research-oriented protocols would allow for construction of evident conclusions, and enhanced neurorehabilitation parameters in this population. The development of such an approach could provide space for novel intellectual property. Once established, a protocol for future studies can allow documentation of vital information, including, but not limited to, the role of rehabilitation professionals, rehabilitation parameters, demographic information, and neuroplastic phenomena.
In this scoping review, we identified gaps in the current domestic literature around neurorehabilitation for persons with upper limb loss. This included a lack of research regarding professional rehabilitation training and treatment, role of peripheral and central neurological processes, and the current use of small sample sizes and unrepresentative participants. Future research can prioritize analyzing rehabilitation parameters, demographic information, and evaluating neuroplasticity in relation to outcomes for persons with upper limb loss. This could significantly improve quality of life and function for those with upper limb loss and improve our understanding of intersections of neurobehavior with technology in the rehabilitative processes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.