
Abstract
Objective. This is the first study to examine Wolf Motor Function Test (WMFT) tasks among EXCITE Trial participants that could not be completed at baseline or 2 weeks later. Methods. Data were collected from participants who received constraint-induced movement therapy (CIMT) immediately at the time of randomization (CIMT-I, n = 106) and from those for whom there was a delay of 1 year in receiving this intervention (CIMT-D, n = 116). Data were collected at baseline and at a 2-week time point, during which the CIMT-I group received the CIMT intervention and the CIMT-D group did not. Generalized estimating equation (GEE) analyses were used to examine repeated binary data and count values. Group and visit interactions were assessed, adjusting for functional level, affected side, dominant side, age, and gender covariates. Results. In CIMT-I participants, there was an increase in the proportion of completed tasks at posttest compared with CIMT-D participants, particularly with respect to those tasks requiring dexterity with small objects and total incompletes (P < .0033). Compared with baseline, 120 tasks governing distal limb use for CIMT-I and 58 tasks dispersed across the WMFT for CIMT-D could be completed after 2 weeks. Common movement components that may have contributed to incomplete tasks include shoulder stabilization and flexion, elbow flexion and extension, wrist pronation, supination and ulnar deviation, and pincer grip. Conclusion. CIMT training should emphasize therapy for those specific movement components in patients who meet the EXCITE criteria for baseline motor control.
Keywords
Introduction
Considerable evidence has been amassed over the past 15 years indicating that forced use of the upper extremity or the integration of forced use with specific behavioral components of shaping and repetition, called constraint-induced movement therapy (CIMT), can lead to improved function among patients classified as having mild to moderate stroke of varying chronicity.1-10 Moreover, comparable improvements seem to occur if the nature of CIMT administered is more intense over 2 weeks11-13 or distributed over time using one of several modified forms.14-21 The Wolf Motor Function Test (WMFT) has often been used as an outcome measure 22 to evaluate CIMT.8,23-25 This functional evaluation assesses timed performance of structured tasks restricted to 2 minutes, a practical limit that ensures tasks are afforded a long, reasonable performance window. During the EXCITE Trial, we noted that patients receiving CIMT often acquired the ability to complete tasks within 2 minutes when compared with patients receiving usual care. 6 However, tasks that still could not be completed following CIMT, together with a description of their movement components, have never been examined. Such an effort would help identify specific aspects of motor retraining that could be emphasized in future investigations to achieve even more substantive improvements. This study represents the first attempt to identify and assess the movement components of those tasks.
Methods
Analysis by Participant
WMFT data for each of the 15 specific timed tasks from the EXCITE trial 25 were examined to identify participants who could not complete each task within 120 s. In EXCITE, participants were divided into 2 groups who either received 2 weeks of training during the target period (immediate, CIMT-I, n = 106) or did not have training during the target period (training was delayed for 12 months CIMT-D, n = 116). Participants in the immediate group had a mean age of 61.72 years (range, 31.4-81.3 years), and 60% of them were male. Participants in the delayed group had a mean age of 66.11 years (range, 30.3-89.8 years), and 50% of them were male. The CIMT-D group received treatment as usual during the target period but did not receive CIMT until a year later. For this analysis, data were categorized as either “completed” or “failed to complete.” We report the changes in these categories within and between groups following randomization before and after the 2-week CIMT intervention for the CIMT-I group during which time the CIMT-D group received no therapy.
Analysis by Task
For the CIMT-I and CIMT-D groups, an analysis of all tasks identified each participant’s ability to complete each task once within the specified 120-s limit at pretest and posttest (2 weeks later). For each task within the CIMT-I and CIMT-D groups, the range of completions at posttest for participants who initially could not complete the task at pretest was identified. The number of occurrences across tasks that could be completed before but not after the target period, called regressions, was also specified.
Statistical Analysis
In the WMFT, the participant is given 2 minutes to perform each task. If the task is not completed in this time, a score of “121” is entered, which should be regarded as a truncated or right-censored time value.
Task completion was determined for each participant and classified in binary fashion as either not completed or completed. The total array of binary values was then examined for each of the 15 timed WMFT items. The data are repeated binary values (preintervention and postintervention), and therefore, the generalized estimating equation (GEE) model for the analysis of repeated binary data was used (PROC GENMOD in SAS 9.22). Similarly, the number of tasks not completed was examined using the GEE model for the analysis of repeated Poisson or count values. The 2 factors in the analysis, Visit (pretarget and posttarget period) and Group (CIMT-I and CIMT-D), were assessed. The main term of interest in the analysis is the Visit (time) × Group (group) interaction. The data were also assessed for Group effects, which indicate that, for both Visits, a difference between Groups is found. The analysis also examined the Visit effects, which indicate that, for both Groups, a difference between Visits is found. The analyses were adjusted by controlling for functional level, affected side, dominant side, age, and gender as covariates, because these factors have been involved in the subject assignment process as detailed elsewhere, 25 and for multiplicity by making a Bonferroni correction that takes the traditional P value (.05) and divides it by the number of possible candidates (n = 15 tasks). Thus, significant P values were set at .0033 (.05/15 = .0033).
Results
A total of 82 tasks among 35 CIMT-I participants and 38 tasks among 19 CIMT-D participants could not be completed either at baseline or 2 weeks later. For all tasks among all participants, changes in the proportion of tasks not completed within 120 s for CIMT-I and CIMT-D participants at baseline as compared with after the 2-week target period (during which time the CIMT-I group received training and the CIMT-D group did not) are shown in Table 1, which also identifies all tasks by number. The proportion of tasks that could not be completed after the target period declined in both groups. The proportions for the CIMT-I group show a larger reduction. Among CIMT-I participants, 13 out of 15 tasks were completed equally or more often after therapy. In contrast, 9 out of 15 tasks were completed equally or more often among CIMT-D participants after the target period. Also, 9 out of 15 tasks could be completed more often among CIMT-D participants after the target period. Some tasks (tasks 1, 5, and 8) show a ceiling effect, in that the proportion of “failing to complete” was actually 0 at the baseline visit.
Proportion of Incomplete Task Performance for the More Affected Side
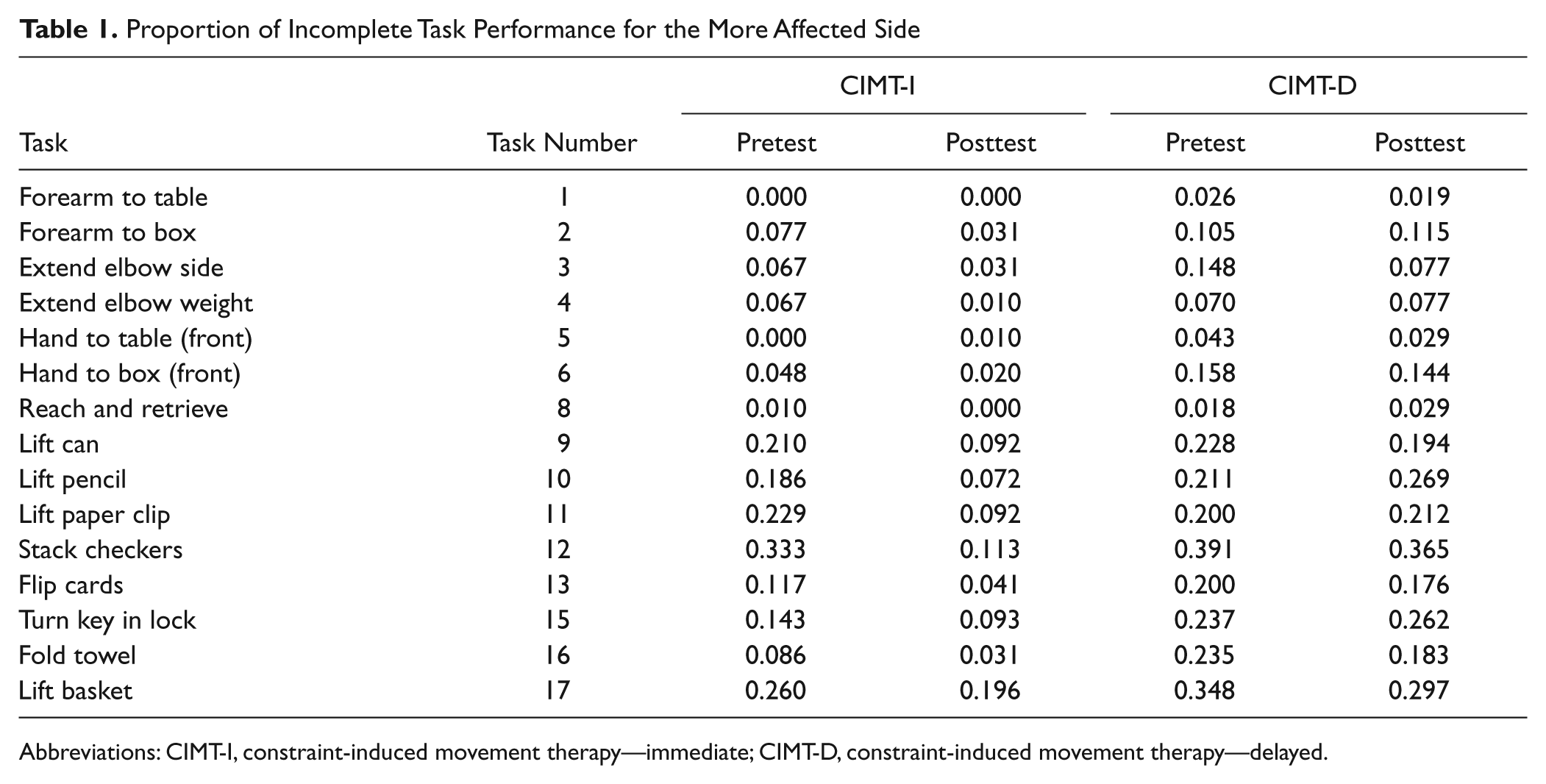
Abbreviations: CIMT-I, constraint-induced movement therapy—immediate; CIMT-D, constraint-induced movement therapy—delayed.
In Table 2, we present the GEE analysis examining Group, Visit, and the interaction for these factors (adjusting for gender, age, functional level, and concordance). The analysis suggests the extent to which the CIMT-I group improved over time more than the CIMT-D group. The interaction was significant at the Bonferroni-corrected test value for tasks 10, 11, and 12 as well as the total incompletes. Other tasks (2, 4, and 9) showed a P value less than .05 but were not significant following the Bonferroni correction. In all cases, the reduction in incomplete tasks was larger for the CIMT-I group than for the CIMT-D group.
P Values for Changes in Task Completion by Group, Visit, and Group × Visit Interaction for the More Affected Side
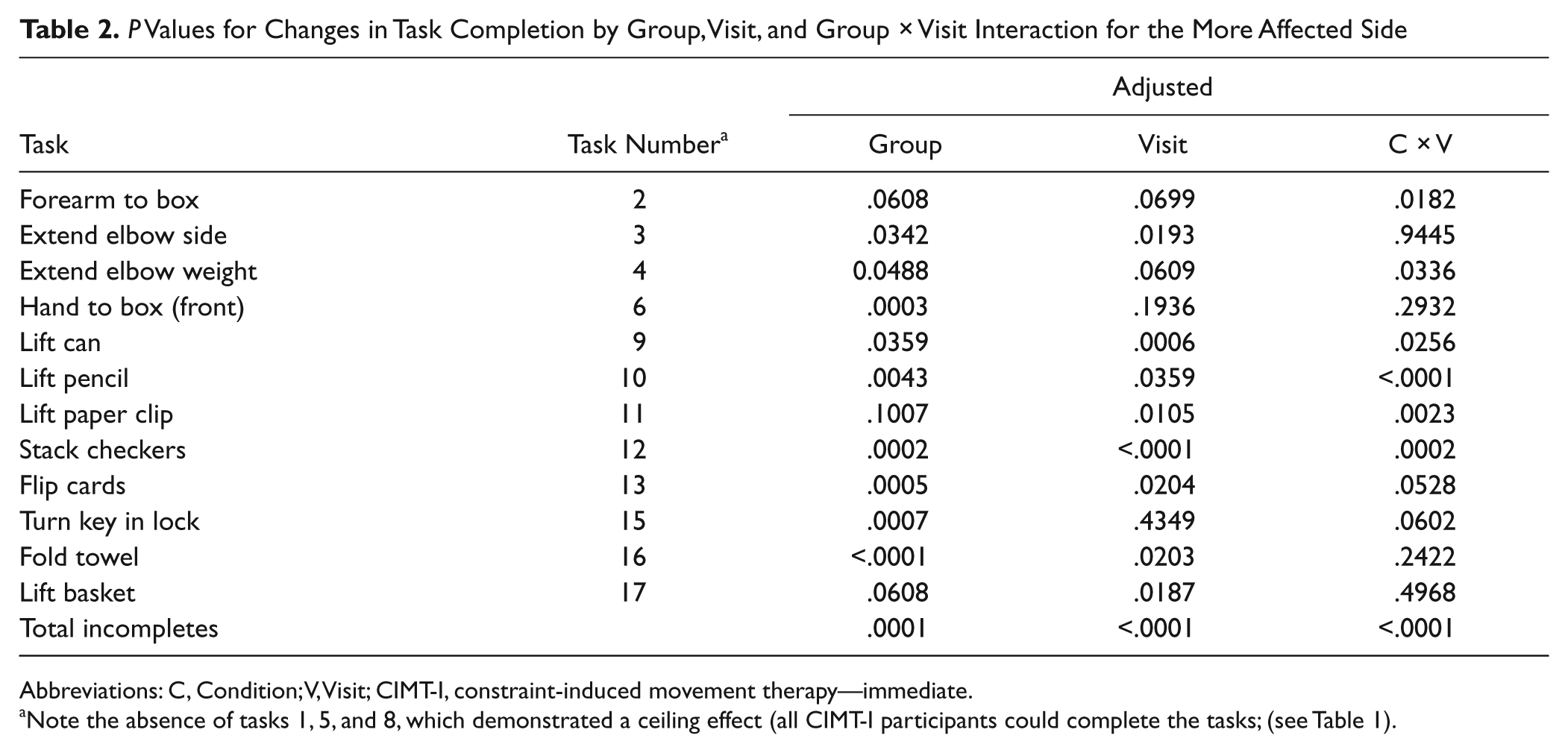
Abbreviations: C, Condition; V, Visit; CIMT-I, constraint-induced movement therapy—immediate.
Note the absence of tasks 1, 5, and 8, which demonstrated a ceiling effect (all CIMT-I participants could complete the tasks; (see Table 1).
Table 3 shows the number of participants who regressed for all tasks, by group designation. In all, 13 CIMT-I and 25 CIMT-D regressions were seen. The largest number of regressions occurred for tasks 4 and 10 within the CIMT-D group. There was only 1 incident of regression for these 2 tasks within the CIMT-I group, which did not experience any regressions for tasks 1, 2, 8, 10, and 15. In all, 10 of 15 tasks could not be performed among some CIMT-I participants after treatment, but only 2 of them (tasks 11 and 17) had multiple participants, totaling 5 regressions. The number of regressions seen among these tasks invites the need to further explore the movement components that should be emphasized in future CIMT training so as to minimize such occurrences.
Number of Regressions by Tasks for CIMT-I and CIMT-D Groups for the More Affected Side
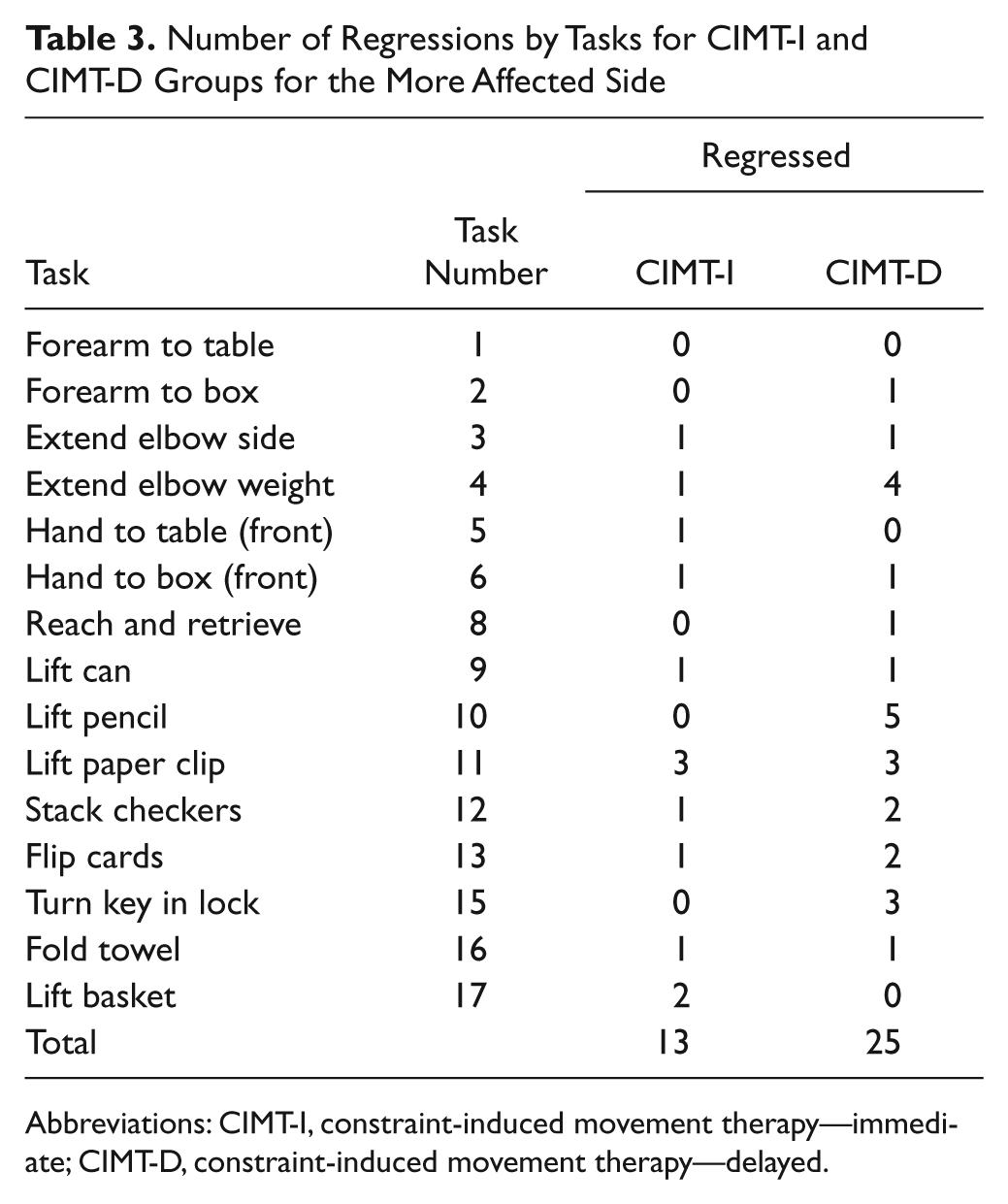
Abbreviations: CIMT-I, constraint-induced movement therapy—immediate; CIMT-D, constraint-induced movement therapy—delayed.
Table 4 depicts the total number of participants who could perform tasks at posttest but not pretest as well as those who still could not perform tasks at posttest, by task and group designation. CIMT-I participants could complete 120 tasks, and CIMT-D participants could complete 58 tasks. No change in performance was seen among 61 and 206 tasks for CIMT-I and CIMT-D participants, respectively. Tasks 9 to 13 and 17 showed the largest number of achievable occurrences for CIMT-I participants, whereas tasks 3, 12, 16, and 17 could be completed most frequently at posttest by the CIMT-D group. Tasks 9, 12, 15, and 17 were the most frequently unachievable for the CIMT-I group and tasks 9 to 13 and tasks 15 to 17 for the CIMT-D group. The most frequently occurring incomplete tasks need to be analyzed further to explore their movement components so we can determine potential training strategies to improve on them.
Overall Changes in the CIMT-I and CIMT-D Groups From Baseline to 2 Weeks Later for the More Affected Side
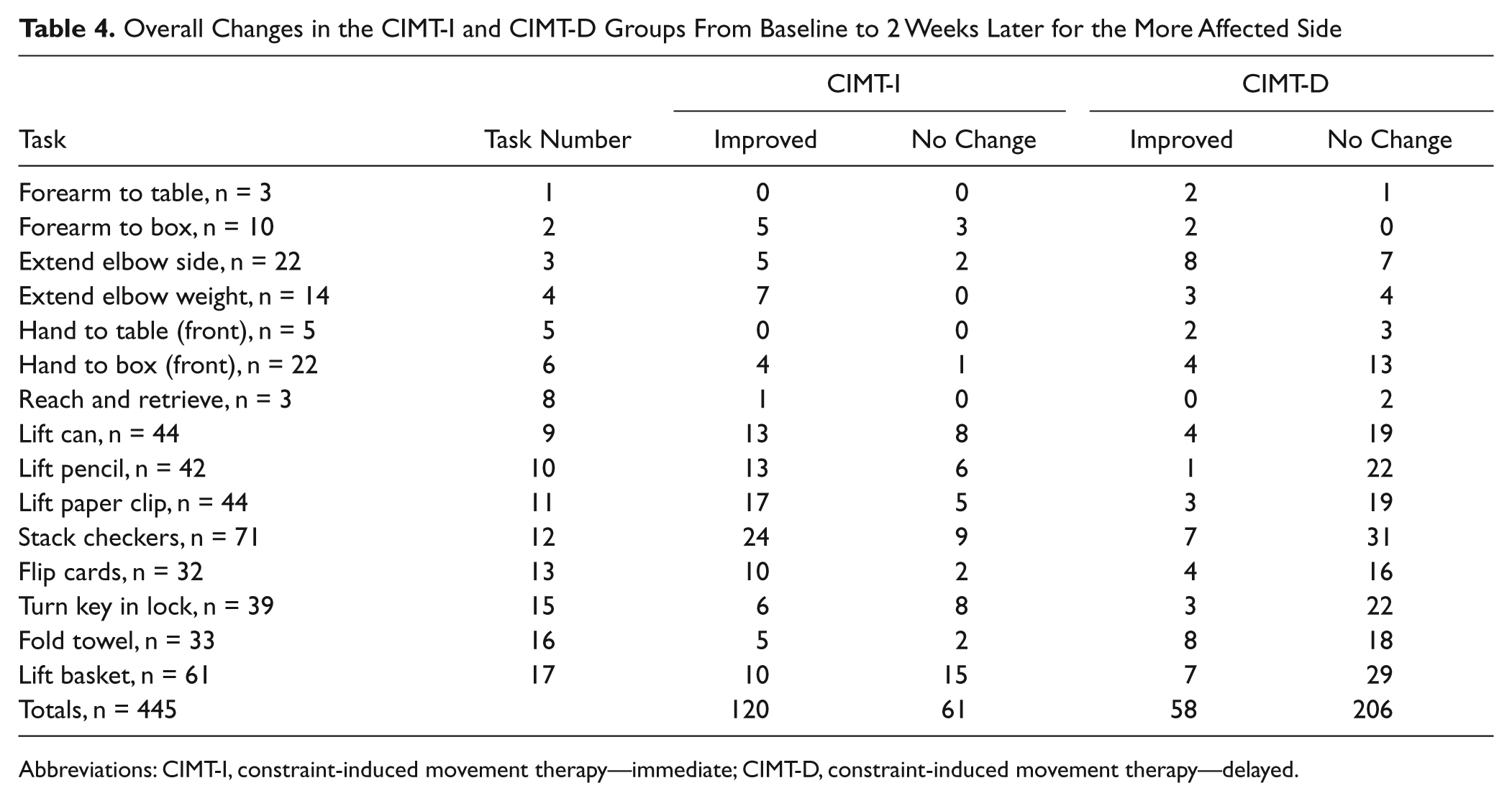
Abbreviations: CIMT-I, constraint-induced movement therapy—immediate; CIMT-D, constraint-induced movement therapy—delayed.
Discussion
Both CIMT-I and CIMT-D groups showed a reduction in the proportion of tasks that could not be completed 2 weeks after enrollment in the study. Spontaneous recovery26,27 may have contributed in part as a result of regained function in both groups; however, the CIMT-I group showed a greater decline in the proportion of incomplete tasks compared with the CIMT-D group (Table 1). The substantial improvement in the ability to complete tasks in the CIMT-I group suggests that early CIMT training among subacute patients versus no CIMT training yields more positive results when using the WMFT as an outcome measure and that CIMT might facilitate task-specific improvements, even during a time when spontaneous recovery may be present. Several studies have provided evidence that early rehabilitation after a stroke results in an increase in motor function.28-31 When examining human32-34 and subhuman primate35-37 stroke models, earlier intervention has resulted in greater rehabilitation-induced forearm or hand cortical map reorganization, whether examined using intracortical microstimulation,36,38 transcranial magnetic stimulation,31,39-42 or functional magnetic resonance imaging34,41,43-45 procedures.
Successful reacquisition of tasks 10 to 12 was more prominent among CIMT-I participants (Table 2). The movement components for these tasks require distal dexterity if they are to be completed successfully. All 3 of these tasks demand fine finger movements (pincer or disc grip) to manipulate the small objects (pencil, paper clip, checkers, and playing card). Previous CIMT studies involving poststroke patients with inclusion criteria comparable with those patients evaluated in the current study have used focal transcranial magnetic stimulation to map activation of distal muscles of the upper extremity, including the abductor pollicus brevis, 39 the extensor digitorium communis, 31 and the finger flexor and finger extensor muscle group. 43 Because many of these muscles are implicated in WMFT task performance, emphasizing tasks during CIMT training intervals that engage movements using these muscles could foster greater improvement and the ability to subsequently complete WMFT tasks that could not be done prior to the CIMT intervention. Throughout task practice involving manipulation of objects, emphasis should continue to be placed on proximal stability and minimizing compensation of the upper extremity. However, the intent should not be to train participants to fulfill WMFT task criteria but, rather, to use the observed limitations as a vehicle to specify elements requiring emphasis during functionally related movement reacquisition.
In the midst of controversy about whether or not compensation should be promoted, we do not advocate or encourage this behavior. First, the stroke survivors in our study are considered mild to moderately impaired; thus, the optimization of restoration is a worthy and potentially achievable goal, which may not be true for the more moderately and severely impaired. 46 Additionally, although compensatory movement is better than succumbing to lesser function, it is hugely beneficial for the patient if he or she is educated in how their efforts differ from their “normal” movements. When patients are made aware of this difference early in their recovery process, they are better able to practice with the weaker muscles while preventing overuse of more hyperactive muscles, in the context of practicing with less compensatory movement. The notion of “‘normal’ is better” has limited direct evidence, and if indeed achieving the greatest amount of function is the driving motivation, patients may be more inclined to use their affected arm if it “looks” more normal during the time of use. Furthermore, without proximal stability, there are greater compensatory movements elicited by the poststroke patient. Most probably, this patient population would value the ability to complete a task using compensatory movements than not complete them at all. This perspective suggests that more emphasis could be placed on the structured practice of movements that limit compensatory movements if we hope to retrain the patient to function as close as possible to their prestroke state. Although compensatory movements are valued because they bring back some functional independence to poststroke patients, would it not be prudent to explore the more positive effects of a learned movement pattern that limits compensation? When providing treatment to a patient, the EXCITE trial valued the importance of focusing on attempting a task emphasizing the “normal” movements rather than allowing compensatory movements.
CIMT training likely affects changes in motor map areas that contribute to the improved precision and coordination of the distal upper extremity required to complete such dexterous tasks. Table 5 is provided to help gain an impression of movement components contributing to task performances. This effort serves to identify putative kinematics associated with tasks 10 to 12 for which between-group differences were observed. Table 5 also shows movement components for the other 12 tasks that did not show statistically significant differences between the 2 groups individually but for which overall differences between groups was seen (Table 2). Collectively, the movement components within this table could serve as a template against which more precise task-specific training could be encouraged as a basis for promoting more favorable changes in WMFT scores and concomitant functional restoration.
In this context, data from Table 3 allow a unique perspective. Instead of concentrating on tasks that patients are able to reacquire after CIMT, this table highlights regressions, which are the tasks that participants could complete at pretest but could not complete at posttest. There were almost twice as many instances of regression for task completions in the CIMT-D group (25) as there were for the CIMT-I group (13). In addition, the CIMT-I group had 5 tasks without any regressions, compared with only 3 in the CIMT-D group. However, at least 1 CIMT-I participant was still unable to complete 1 of 10 tasks after receiving CIMT intervention. Many factors may contribute to the regressions seen in these tasks, including fatigue, acquired weakness over time, cognitive compromise, compensatory movements used at baseline but not used during the reevaluation, or limited practice provided on the specified movements during CIMT. Regardless of the factor(s), to create an effective intervention, identifying the tasks and determining the movement components comprising those tasks that remain difficult for patients to complete, even after CIMT, is important. Consequently, the results obtained from these data, may help generate aspects of CIMT training that include more treatment on the movement components that define tasks 3, 4, 5, 6, 9, 11, 12, 13, 16, and 17 to foster better improvement. These movement components include pronation, supination, and ulnar deviation at the wrist as well as internal and external rotation of the shoulder (Table 5). For example, to improve on tasks that might embrace the movements contained in task 12, which include shoulder stability and internal and external rotation, elbow flexion and extension, forearm pronation, and pincer grip, clinicians might consider task practice involving these movements. Moreover, tasks 11 and 17 have proven to be more frequently difficult for patients; therefore, the movement components of these tasks, including hook/pincer grips and wrist stabilization (Table 5) should be especially emphasized in future CIMT training. For example, an activity that incorporates finger grip in conjunction with sustained wrist stabilization is placing and removing small pegs from a pegboard. Tasks 11 and 17 may be difficult because of the extreme sizes of the objects patients must manipulate. For example, the small paper clip requires complex finger dexterity, whereas a considerable amount of shoulder strength and neuromuscular control are needed to lift the large basket. A study by Woodbury et al 47 tested, as its original hypotheses, whether the WMFT items measure a single trait and progress in difficulty. This study’s results suggest that 14/15 assessment items did measure a single trait, and the hypothesized progression of difficulty in the item order was supported. The supported item order relates to this study and can be observed in Table 5. As one goes from task 1 to task 17, it can be observed that the movement components required to complete each functional task correctly begin more proximally and then progress to a combination of both proximal and distal components. Task practice modifications that might enhance functional gains could include activities involving repetitive lifting of household objects of different weights, shapes, and sizes during training, which may prove to be beneficial in achieving functional gains.
WMFT 15 Tasks With Specified Movement Components a for the More Affected Side
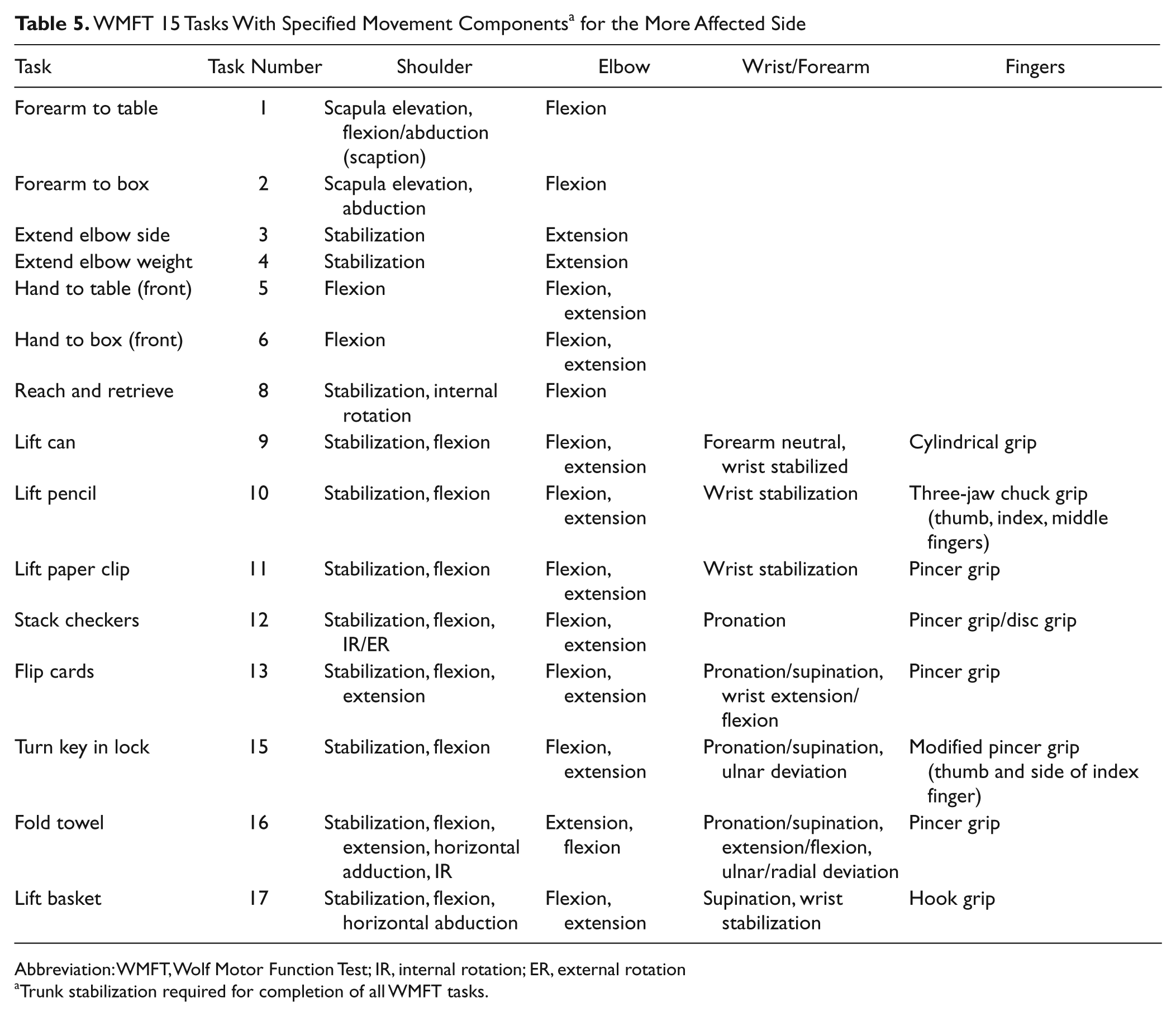
Abbreviation: WMFT, Wolf Motor Function Test; IR, internal rotation; ER, external rotation
Trunk stabilization required for completion of all WMFT tasks.
Results in Table 4 reveal that CIMT-I participants showed a significantly larger improvement in the number of completed tasks than the CIMT-D participants. However, specific tasks (especially tasks 15 and 17) remained difficult for participants to complete at posttest regardless of whether or not the CIMT intervention was provided. Tasks that show a significant number of incompletes at posttest should be further examined to determine the movement components required to perform each task in order to make recommendations on ways to improve CIMT training in the future.
Of the tasks that remain difficult to complete across groups, one can speculate that the common movement components include shoulder stabilization and flexion; elbow flexion and extension; wrist pronation, supination, and ulnar deviation; and a pincer grip. Moreover, the movement components required to perform the task that regressed after CIMT include shoulder flexion, and elbow flexion and extension (Table 5). On grouping these movements together, one can infer that movements showing the least improvement occur more proximally than distally and require proximal stabilization more frequently than proximal mobilization. The CIMT training protocol specifically prohibited training for WMFT tasks. Although never explicitly discussed among CIMT therapists across EXCITE locations, the possible concern that overemphasis of shoulder joint static and dynamic activities could result in shoulder pain with a subsequent limitation imposed on distal joint activities may help explain why less effort might have been directed toward some WMFT tasks requiring better shoulder stabilization or motion. This possibility appears to be unlikely, however, because our analysis of pain and fatigue among EXCITE participants showed little change over time. 48 In light of this consideration, future CIMT interventions should emphasize more frequent but cautiously dosed proximal stabilization exercises as a precursor to achieving functional gains but performed within a functional context. Unilateral wall holds are often used in clinical practice to promote shoulder stabilization. Ways in which unilateral wall holds can be incorporated into functional training of the affected upper extremity include placing objects on a shelf, placing clothing on wall hooks, or holding a board in place as someone else hammers. These activities may be added to CIMT training to improve a patient’s ability to complete the functional tasks assessed during the WMFT.
Limitations
The interpretation of movement contributions to WMFT task performance was based on observation rather than kinematic analyses. Unfortunately, kinematic evaluations before and after CIMT are limited at this time. Wu et al 49 showed that there were improvements in motor control strategies after measuring changes in reaction time, movement time, total displacement, and peak velocity among stroke survivors performing a specific reaching task with the more affected upper extremity, whereas Caimmi et al 50 showed that stroke survivors displayed better shoulder and elbow coordination following CIMT. However, Massie et al 51 have shown that compensatory movements persist after CIMT. In addition, restricting compensatory trunk motion during CIMT can improve outcomes. 52 Collectively, these are suggestive of improved upper-limb movement that may engage compensatory strategies. Considerably more kinematic analyses within and between proximal and distal upper-extremity joints are needed, even among able-bodied individuals, to better understand specific movement components that comprise the WMFT, as a basis for validating our impressions. Building on the findings of these studies will foster greater specificity in both directing instruction to patients during CIMT and better distinguishing compensatory from restitute movement behaviors. Our retrospective analysis of EXCITE trial data 6 also prevented the acquisition of missing data in a timely fashion. As a result, 31 of the 514 data points had to be excluded from the current study. The extent to which these missing data could influence our results is uncertain.
Future Studies
The nature of WMFT implicates an overlap in movement components for several distal tasks. Future efforts should undertake formal kinematic studies across tasks to better delineate changes in specific movement components seen in stroke survivors before and after CIMT. 53 This information could better inform clinicians regarding specific joint movement components requiring rehabilitative emphasis within the CIMT interval. Moreover, comparing temporal and spatial aspects of kinematics for a population with stroke with those of an age-matched able-bodied population would further contribute to improved specification of training directed toward minimizing compensatory strategies. In this context, the Functional Ability Scale within the WMFT represents a reasonable effort to assess quality of movement but lacks the sensitivity inherent in kinematic evaluations to better inform clinicians about how to specify training components. Better comprehension of limb and trunk movement 54 aberrations during task training might permit clinicians to more effectively limit compensatory behaviors while targeting movement components that remain difficult for patients to perform in efforts to achieve the greatest functional improvements.
Finally, our laboratory will compare changes among incomplete WMFT tasks between the CIMT-I and CIMT-D groups after the latter has received CIMT training, 1 year later. Such an effort will further delineate the role of time and the delivery of other therapies on the impact that CIMT training might have on changes in ability to complete WMFT tasks that could not be done either at the time of enrollment or after all participants have received CIMT. Differences in reacquisition of task completion between CIMT-I group members within 3 to 9 months poststroke and CIMT-D participants 1 year later when compared with the data reported here may reveal the persistence of movement deficits and further direct the specification of training during the CIMT interval.
Conclusion
This retrospective study is the first attempt to analyze which timed tasks of the WMFT showed the least amount of improvement when performed by participants in the EXCITE trial. In light of these results, there is a pattern of movement components that patients had difficulty performing to complete some tasks in the allotted time (120 s). Therefore, one can conclude from these results that future CIMT interventions should increase emphasis on proximal upper-extremity stabilization during therapy and on creative ways to enlist specific movements governing shoulder joint rotation, wrist pronation/supination, and variable-size object manipulation in patients who meet the motor entry criteria for CIMT.
Footnotes
Acknowledgements
The critical comments offered by Carolee J. Winstein, PhD, PT, FAPTA, on previous drafts of this manuscript are very much appreciated.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data presented in this article were derived from work supported through NIH grant R01 HD37606.