
Abstract
Hand loss profoundly impacts daily functioning. Reversal of amputation through hand replantation or transplantation offers an alternative to prosthetics for some. Whether recipients exhibit more extensive and natural limb use during everyday life than prosthesis users is, however, unknown.
We asked unilateral, below-elbow amputees (N = 22), hand graft recipients (transplants N = 4; replants N = 2), and healthy matched controls (N = 20) to wear wireless accelerometers distally on their forearms/prostheses and proximally on their upper arms. These units captured limb activity over 3 days within participants’ natural environments.
Graft recipients exhibited heavier reliance on their affected hands compared to amputees’ reliance on their prostheses, P < .001. Likewise, reliance on the injured side upper arm was also greater for hand graft recipients than amputees, regardless of whether they were wearing their prostheses, P < .05 in both cases. Hand graft recipients, like healthy controls, also relied more on forearm vs upper arm movements when controlling their limbs, P < .001.
Compared with conventional prosthesis users, graft recipients exhibited more extensive and natural functioning of the upper limbs during everyday activities. This information is an important addition to other considerations when evaluating risk-benefit of these treatment alternatives.
Introduction
Upper limb amputation has a profound impact on function and quality of life.1-3 Prostheses can improve outcomes, but despite technological advances, disuse occurs among a minority of patients,4-6 and even those who use a prosthesis often rely heavily on their intact limbs during everyday life.7-10 This tendency toward “one-handedness” contrasts with the more bilateral pattern of limb use in healthy adults, and is associated with poorer function, greater disability, and overuse injuries.2,11,12 In a small fraction of cases, it is possible to replant the severed limb surgically immediately after amputation. The increasing availability of allogeneic hand transplantation presents an alternative to prosthetic limbs even long after amputation, but this experimental procedure involves risks associated with major surgery and lifelong immunosuppression. An important consideration in evaluating these treatment options is the extent to which they restore functionality during everyday life.
The few attempts to compare functional recovery between recipients of hand replants or transplants and prosthesis users relied on standardized assessments that may have limited ability to predict function during everyday life. Despite substantial individual variability, a recent meta-analysis concludes that functional outcomes are comparable following hand replantation or transplantation, with highest levels attained in below-elbow amputees. 13 In below-elbow cases, data suggest that hand replantation 14 or transplantation 15 may yield better function, higher satisfaction, and lower levels of disability than prostheses. The critical question of whether grafted limbs restore greater use of the injured limb and more natural, bilateral upper extremity function during everyday life than prosthetics, however, remains unanswered. Advances in sensor technology make it possible to address this question.
Recent studies employing wireless accelerometers quantified limb activity in the natural world. Data support the common wisdom that while healthy adults exhibit high bimanual symmetry, unilateral amputees who use prostheses rely heavily on the intact limb during everyday life.7,9,16 It is noteworthy that similar to accelerometry studies of stroke patients, 17 investigation of amputees has failed to find significant relationships between performances on lab-based functional tests and prosthesis use in the real world. 8 These observations emphasize the critical need for investigation of upper extremity use during everyday life when comparing the functional outcomes of surgical hand grafts vs prosthetic interventions. Here, we report the first effort to do so.
We implemented a wireless accelerometry protocol to record upper extremity movements during 3 days of normal activity in current and former (ie, hand transplant or replant recipients) unilateral, below-elbow amputees, and healthy age-matched controls. Prior studies only instrumented the forearms and prostheses at the distal wrist levels to capture hand and prosthetic end-effector movements7,8 or at different levels (intact wrist and residual upper arm proximal to elbow
9
). By contrast, we also placed sensors proximally above the elbows (Figure 1), to evaluate between-group differences in upper arm and residual limb (ie, stump) movements, their relationship to hand and prosthetic end-effector control, and use of the residual limb by amputees when not wearing their prostheses. If hand grafts restore more naturalistic upper extremity function during everyday life, then we expect hand transplant and replant patients to exhibit greater reliance on the affected limb than prosthesis-using amputees. This should be evident at both the levels of the distal forearm/prosthesis and upper arms. Accelerometer Montage. As illustrated here on a healthy individual (KB), distal sensors are attached with velcro watchbands to the wrists of the forearms (or “wrists” of prostheses in the case of amputees). Proximal sensors are located above the elbows and attached with white elastic armbands.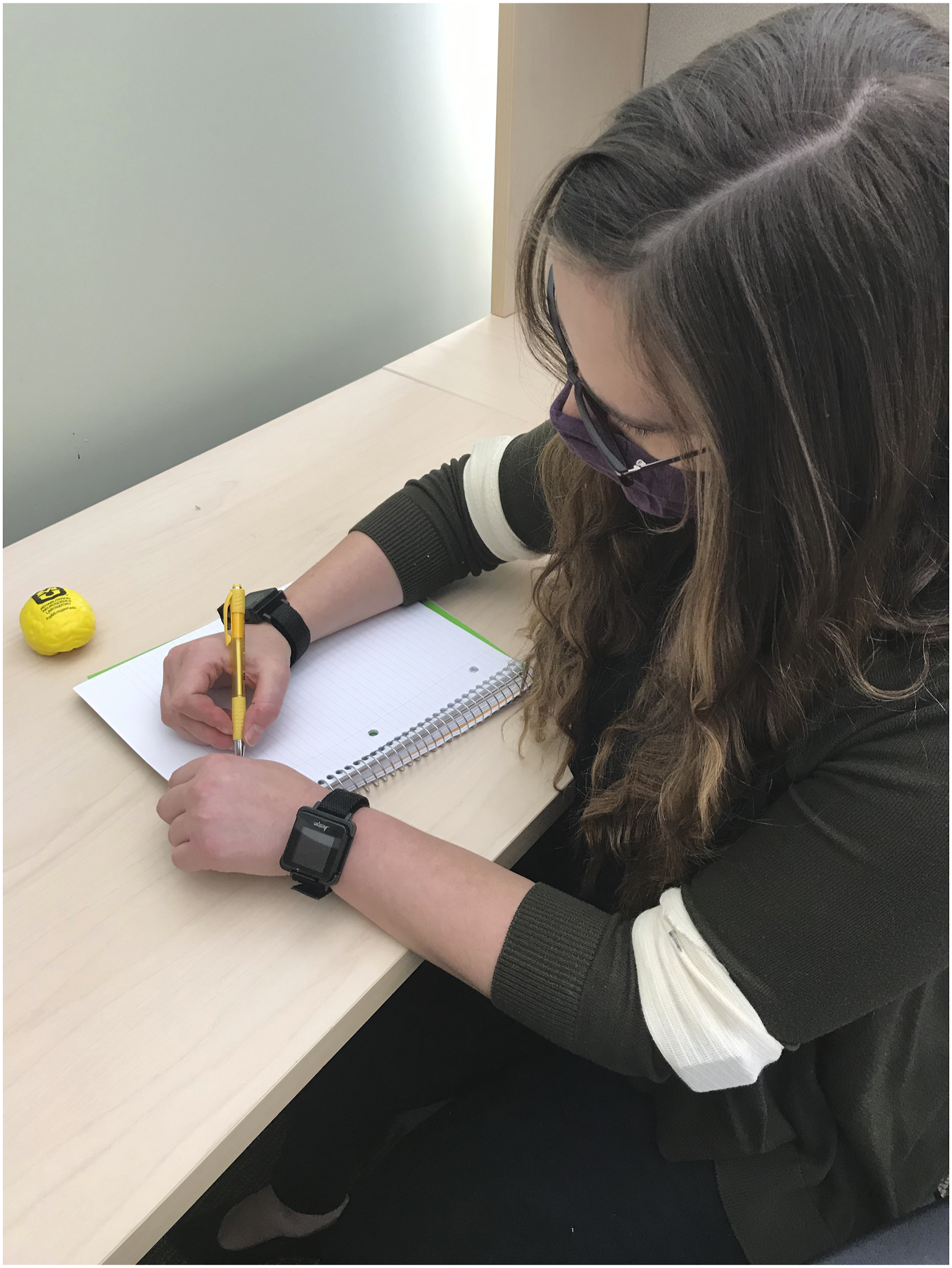
Methods
Ethics
The protocol was approved by the University of Missouri Office of Human Protections and the Human Research Protection Office at the Department of Defense and was performed in accordance with the Declaration of Helsinki. All participants provided informed consent.
Participants
Individual subject description for the hand graft group.
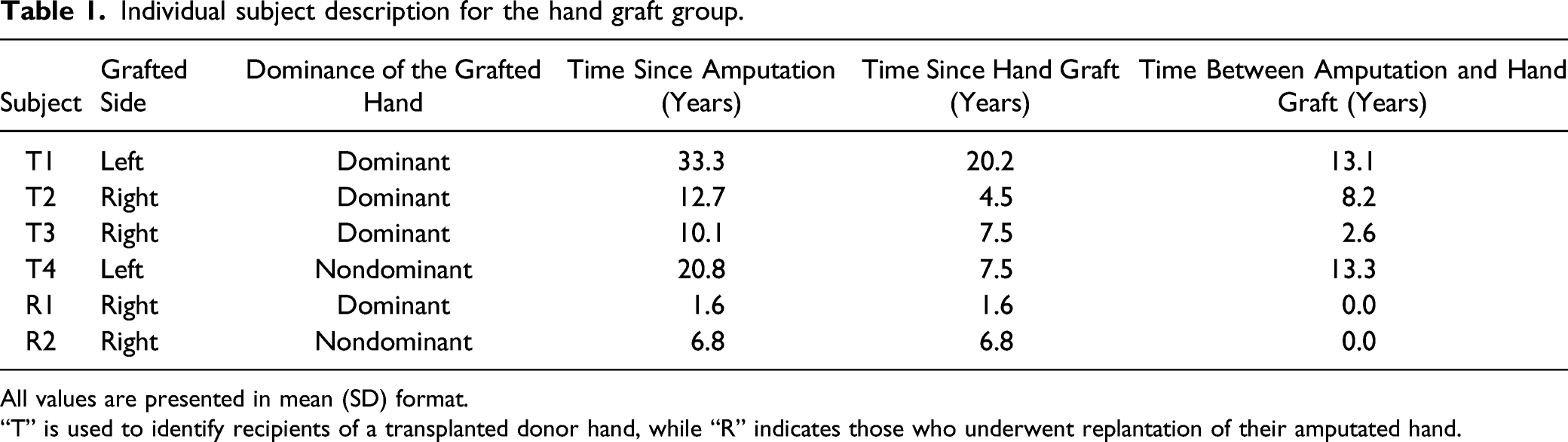
All values are presented in mean (SD) format.
“T” is used to identify recipients of a transplanted donor hand, while “R” indicates those who underwent replantation of their amputated hand.
Hand graft patients were recruited through the Christine M. Kleinert Institute (CMKI) and local clinicians. Autologous hand graft patients underwent surgical replantation of their severed hand shortly after their below-elbow amputations and received hand rehabilitation as prescribed by their physician. Allogeneic hand transplant recipients underwent transplantation of a donor hand years after their below-elbow amputation. They received intensive post-surgical hand rehabilitation as part of CMKI’s protocol. Amputees were recruited through the Hanger Clinics and local and national advertising. Amputee subjects were included if they had a unilateral, below-elbow amputation and used a prosthesis daily. We have limited data on rehabilitation time for our 16 (out of 22) amputees, all of which is self-report. Seven amputees reported receiving prosthetic training for <10 sessions (n = 7). A single amputee reported training for 11+ sessions, and the remaining 8 claimed not to have received any prosthetic training or therapy. Subjects were excluded if they had any disorder other than amputation, affecting upper extremity use such as neurologic disorders, brain injury, psychiatric illness, or acute orthopedic injuries. Controls were recruited locally in the Columbia, MO region.
Data Collection
We shipped 4 accelerometer sensors (GT9X Link, ActiGraph Corp, Pensacola, FL) and a printed activity log to subjects. These accelerometers recorded movement in x, y, and z directions at a frequency of 30 Hz. The sensors were preprogrammed to record for a 7-day window beginning on a date agreed by the subjects. Subjects wore these 4 accelerometers for 3 consecutive days during this window. The data collection included 2 weekdays and 1 weekend day to sample both occupational and leisure activities.
Our bilateral montage included 2 distal sensors located on the biological or prosthetic forearms at the level of the wrist to capture hand or prosthetic end-effector movements. The remaining 2 proximal sensors were placed above the elbows at the level of the humerus to capture upper arm movements (Figure 1). The distal sensors were worn like watches using Velcro straps, and the proximal sensors were inserted into an elastic cuff. Subjects were instructed to take the accelerometers off prior to sleeping at night and to reposition them immediately upon waking in the morning. As reported below, several individuals failed to comply and wore the devices during the night. The accelerometers were clearly labeled for consistent and correct placement between days. At the end of data acquisition, subjects returned the accelerometers and activity log to the research team using a prepaid envelope.
Data Analysis
Actilife 6.0 (ActiGraph Corp, Pensacola, FL) was used to download the accelerometer data in 1-second epochs of activity counts for each sensor. Activity count is the output unit when the raw acceleration data is filtered to enhance human movement and suppress unwanted motion, sampled and summed over a 1-second epoch, using a proprietary algorithm in Actilife 6.0. Each activity count represents .001664 g (=.0163 m/s2). Further data analysis was performed with Matlab R2019b (Mathworks, Natick, MA). Activity counts for the x-, y-, and z-axes were converted to a vector capturing the magnitude of each sensor’s movements using equation (1)
Variables of interest were computed during awake time when limbs/prostheses were being used. Although participants were asked to remove the sensors prior to sleeping at night, we used their activity logs and an automated algorithm to detect and remove periods during which they were asleep during the day or night if they did not remove their sensors. 18 For amputees, we also identified prosthesis non-wear time. The prosthesis non-wear time was computed as the time during which moving root mean square of the activity magnitude for the prosthesis sensor had an average value of 0 for a minimum of 30 consecutive minutes. Segments of prosthesis activity magnitude containing non-wear were eliminated when examining prosthesis activity for amputee subjects. Our four-accelerometer montage made it possible to analyze the residual upper arm activity when the prosthesis was on vs off by analyzing the proximal sensors’ activity with respect to the prosthesis non-wear. Consistent with the prior research, 8 measures of limb/prosthesis usage were described only when at least 1 side sensors were in motion.
Upper Limb Activity in Time Domain
Upper limb usage was analyzed using bilateral and unilateral limb use times for hand/prosthesis (ie, distal) sensors only (and not the proximal arm sensors).19,20 Hand/prosthesis activity time was computed when there was movement in either or both distal sensors (activity magnitude >0 in at least 1 side). Unilateral activity was identified as activity in the distal sensor on 1 side (activity magnitude >0) and no movement in the contralateral distal sensor (activity magnitude = 0). Similarly, bilateral activity was identified when both distal sensors were in motion (activity magnitude >0).
Interlimb Reliance During Daily Activities
Interlimb reliance was determined using %median reliance on the affected side for proximal (upper arm) and distal (hand/prosthesis) levels separately.
8
When at least one side is moving, reliance on the affected/prosthetic side is computed using equation (2) for hand graft patients and amputees. For control subjects, we computed %median reliance on dominant and nondominant side by replacing affected side activity magnitude with either dominant or nondominant side activity magnitude, respectively. Median reliance on the affected side of >50% indicates greater reliance on the affected than unaffected side in overall daily activities. A 0% and 100% median reliance on the affected side would suggest unilateral activity in the unaffected and affected sides, respectively. Values between 1 and 99% indicate bilateral activity
Intralimb Segment Reliance During Daily Activities
Intralimb reliance was determined using %median reliance on forearms/prostheses. When at least 1 side is moving, the relative movements of the forearm/prosthesis vs upper arm in the affected limb and unaffected limb were calculated using equation (3). Median reliance on forearm/prosthesis of >50% indicates greater reliance on the forearm/prosthesis than upper arm during upper limb movement
Statistical Analysis
One-way ANOVAs were used to determine group differences (hand graft recipients, amputees, controls). Separate one-way ANOVAs were run for comparisons against control dominant and nondominant hands. Pair-wise comparisons were performed with Bonferroni adjustment. Side differences in intralimb reliance (affected vs unaffected or dominant vs nondominant) were examined using paired sample t-tests. One-sample t-tests determined if inter- or intralimb reliance deviated significantly from 50% in each group. Due to the small sample size in the hand graft group, Welch’s t-tests were used to evaluate effects of side of injury and type of hand graft. In the hand graft group, nonparametric Spearman’s correlations were used to examine the relationships between age, time since hand graft, amputation-graft interval and unilateral hand activity times, bilateral hand activity time, interlimb reliance, and intralimb reliance. Parametric Pearson’s correlation was used for similar relationships in the amputee group. SPSS version 27 (IBM, Armonk, NY) was used for statistical analysis. Significance was set at P < .05.
Because we found differences in activity magnitude between the dominant and nondominant limbs of controls at both the distal/forearm (t (19) = 6.497, P < .001) and proximal/upper arm (t (19) = 3.406, P = .003) levels, these data were kept separate in our analyses. In the amputee group, neither forearm/prosthesis nor upper arm activity was influenced by dominance of the affected limb, or by the type of prosthesis. Data were therefore collapsed across these variables for subsequent analyses. Because we also failed to detect significant differences in the hand graft group, we likewise collapsed across the side affected (dominant vs nondominant) and type of graft (autologous replantation vs allogeneic = transplantation).
Active time involving the forearm/prosthesis did not differ significantly between the groups; however, they did differ in the amount of time they were awake, F (2,45) = 6.384, P = .004. Specifically, on average, the hand graft group was awake longer than healthy controls, P = .004). For this reason, we chose to normalize data for each individual participant relative to their waking time for subsequent analyses.
Results
Unilateral and Bilateral Hand and Prosthetic End-Effector Activity
Variables of interest including interlimb reliance, intralimb reliance, and activity time profile for the amputees, healthy control dominant and nondominant sides, and hand graft recipients.
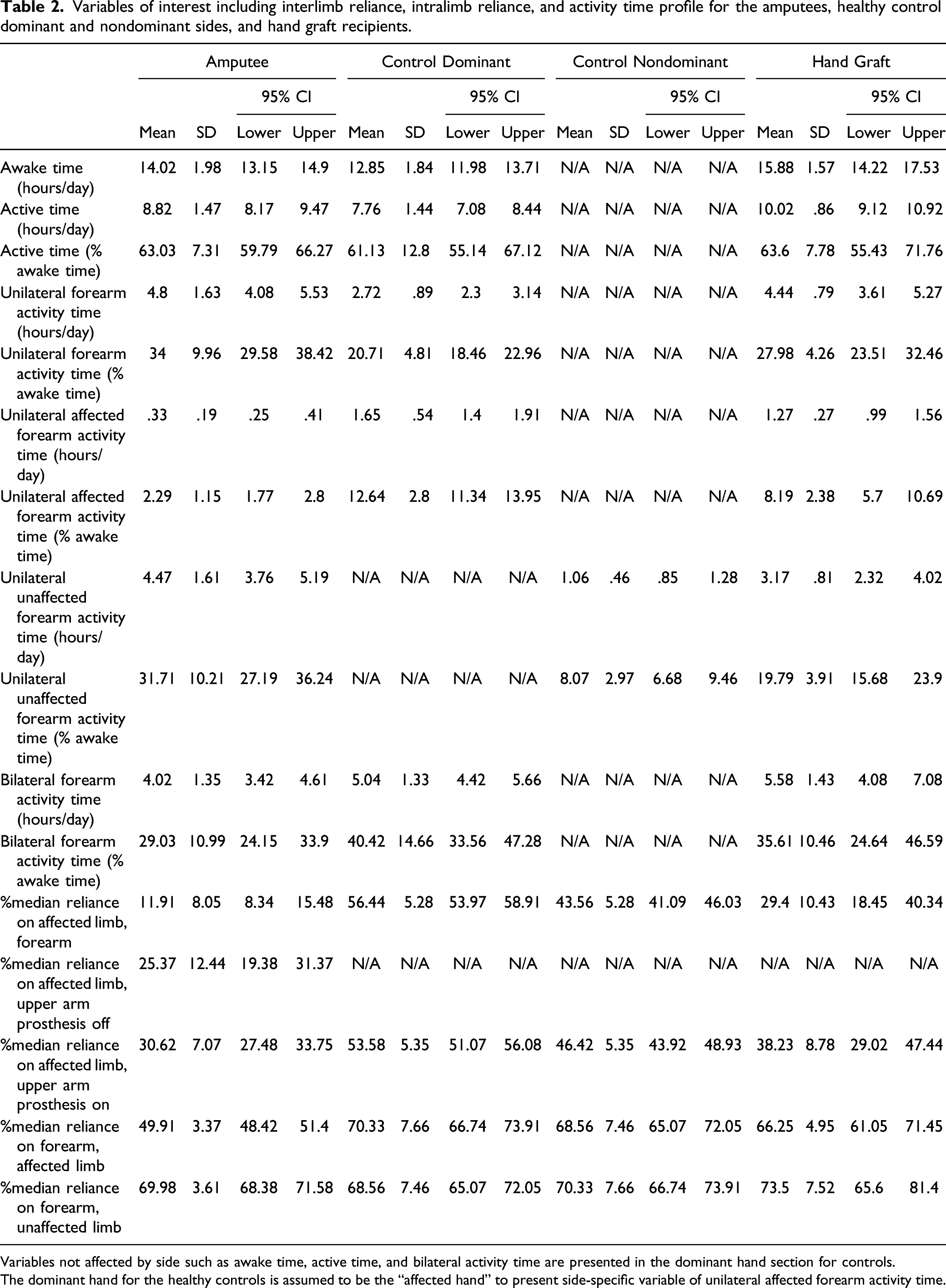
Variables not affected by side such as awake time, active time, and bilateral activity time are presented in the dominant hand section for controls.
The dominant hand for the healthy controls is assumed to be the “affected hand” to present side-specific variable of unilateral affected forearm activity time.
Time spent in unilateral activity with the healthy hand also differed between the groups when tests included data from either controls’ dominant (F (2, 45) = 26.774, P < .001, η2 = .543) or nondominant (F (2, 45) = 38.146, P < .001, η2 = .255) sides (Table 2). Consistent with their engaging in less compensation with the uninjured side, the hand graft group showed lower activity with their healthy hands compared to amputees, P < .001. Nevertheless, the hand graft group did exhibit considerably more unilateral activity involving their uninjured hands than controls’ dominant (P = .004), but not nondominant sides.
Healthy controls spent more time in bilateral vs unilateral activity (t (19) = −2.646, P = .016, Cohen’s d = 19.681). We failed to detect similar differences in either the hand graft or amputee groups, however. The groups also differed in the amount of time they spent in bilateral activities, F (2, 45) = 4.293, P = .02, η2 = .141; Table 2). More precisely, amputees spent significantly less time in bilateral activities than healthy controls (P = .016), whereas the hand graft group did not differ significantly from either controls or amputees.
Interlimb Reliance on the Biological vs Prosthetic Forearms
As detailed in the method section, we next computed %median reliance in order to investigate the symmetry of bilateral limb use in the 3 groups.
8
Consistent with prior studies,8,17,21 data from the distal sensors revealed that healthy adults exhibit a high degree of bilateral symmetry in use of their 2 limbs. In contrast to these earlier investigations, however, we did find evidence for greater reliance by controls on their dominant vs nondominant sides, which presumably is driven by hand preferences. This is reflected in median reliance on dominant side being significantly greater than 50% (t (19) = 5.454, P < .001, Cohen’s d = 5.281; Figure 2). In keeping with what we found for overall activity, neither patient group showed differences in %median reliance between their dominant vs nondominant sides. Instead, reliance on the injured side was significantly below 50% for both the hand graft (t (5) = −4.841, P = .005, Cohen’s d = 10.426) and amputee (t (21) = −22.191, P < .001, Cohen’s d = 8.052) groups (Figure 2). Interlimb reliance for the distal sensors showing less “single-handedness” after hand graft than prosthesis users. Scatter-box plots showing %median reliance on the affected side (distal sensors) for hand graft group, amputee group, and healthy controls during daily activities. The dashed line at x = 50% indicates equivalent reliance on each limb. Values greater than 50% (on the right side of the dashed line) indicate greater reliance on the affected/prosthetic side. Values below 50% (on the left side of the dashed line) indicate greater reliance on the unaffected side Individual subjects’ data points are depicted using circles. Filled circles represent subjects whose dominant side was affected, whereas unfilled circles represent subjects whose nondominant side was affected. Median values for each group are indicated by the dotted line inside the box, while group means are depicted by the solid line inside the box. The 25th and 75th percentiles are captured by the boundaries of each box. Whiskers extend to extreme values within mean +/−2.7σ. The shaded regions represent +/− 95% confidence intervals (95% CI) around mean values for each group.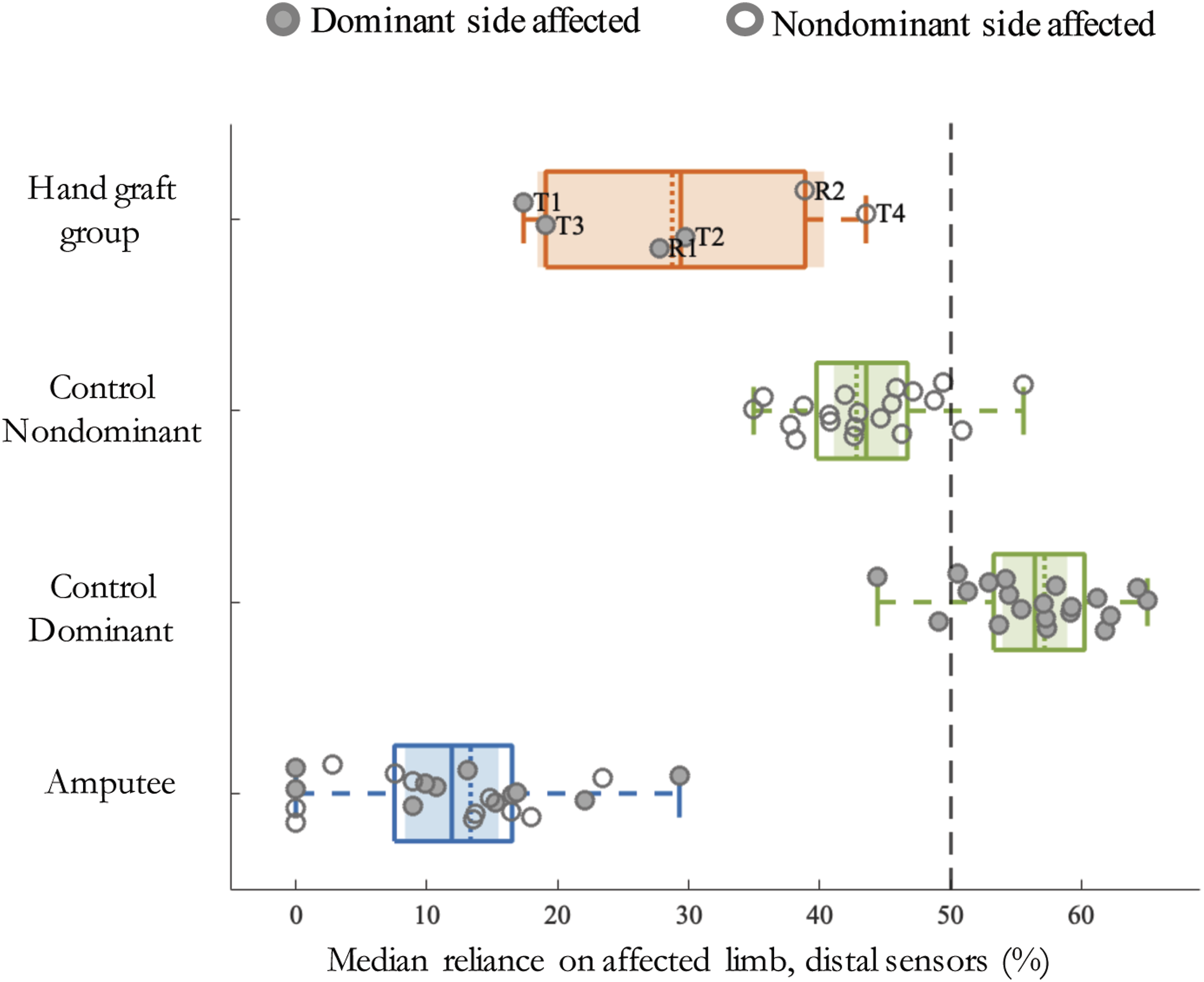
The 3 groups differed in the extent to which they relied on the affected hand/prosthesis when comparisons of data acquired from the distal sensors involved either controls’ dominant (F (2, 45) = 192.663, P < .001, η2 = .895) or nondominant (F (2, 45) = 97.279, P < .001, η
2
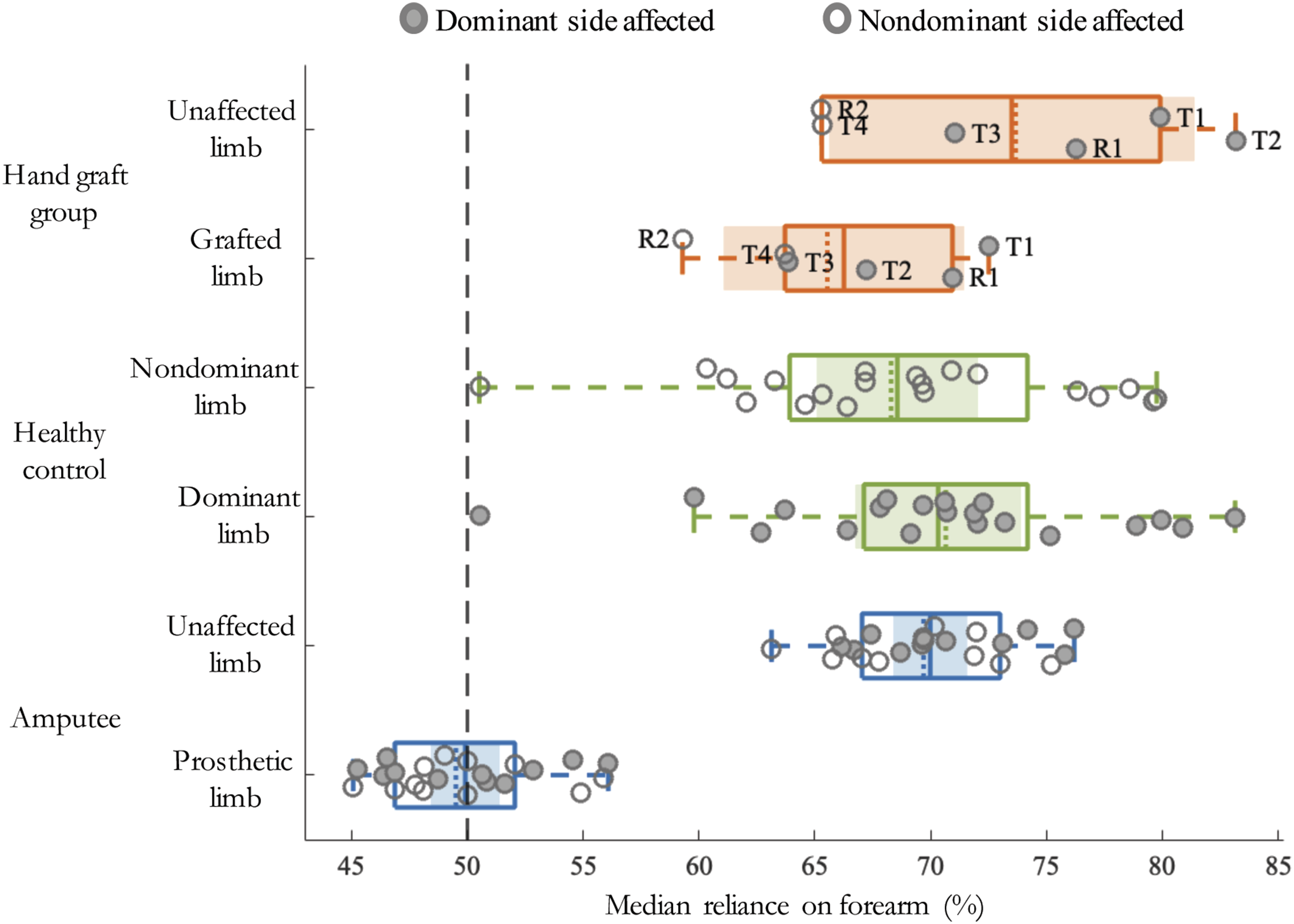
= .812) hands (Figure 2, Figure 3, Table 2). On average, replant and transplant patients relied 147% more on their grafted hands than amputees relied on their prostheses (P < .001, Figure 2, Figure 4). Importantly, this is consistent with the hypothesis that hand graft patients exhibit less “one-handedness” and greater bimanual hand use than amputees using prostheses. Reliance on the grafted hand nevertheless fell short of healthy controls’ reliance on either their dominant (P < .001), or nondominant (P < .001) hands, indicating a failure to return to an entirely normal pattern of interlimb use post-graft. Intralimb reliance was normal in the hand graft group. Intralimb reliance for hand graft group, amputee group, and healthy controls’ affected/prosthetic limb and unaffected limb vs. controls’ dominant and nondominant limbs. Dashed line at x = 50% suggests equivalent contribution from biological forearm/prosthetic and upper arm segments during daily activities. Values greater than 50% (on the right side of the dashed line) indicate greater reliance on the forearm/prosthetic segment. Values below 50% (on the left side of the dashed line) indicate greater reliance on the upper arm segment. Individual subjects’ data points are depicted using circles. Filled circles represent subjects whose dominant side was affected, whereas unfilled circles represent subjects whose dominant side was affected. Box shows median values (dotted line inside the box), mean values (solid line inside the box). Bounds of the box show 25th and 75th percentile, whereas whiskers extend to extreme values within mean +/−2.7σ. Shaded patch represent 95% CIs around mean values for each group. Interlimb reliance for the proximal sensors showing less “single-handedness” after hand graft than prosthesis users. Scatter-box plots showing median reliance on the affected side (proximal sensors) for the hand graft group, amputee group, and healthy controls during daily activities. Dashed line at x = 50% suggests symmetric interlimb reliance. Values greater than 50% (on the right side of the dashed line) indicate greater reliance on the affected/prosthetic side. Values below 50% (on the left side of the dashed line) indicate greater reliance on the unaffected side. Individual subjects’ data points are depicted using circles. Filled circles represent subjects whose dominant side was affected, whereas unfilled circles represent subjects whose nondominant side was affected. Median values for each group are indicated by the dotted line inside the box, while group means are depicted by the solid line inside the box. The 25th and 75th percentiles are captured by the boundaries of each box. Whiskers extend to extreme values within mean +/−2.7σ. The shaded regions represent +/− 95% CI around mean values for each group.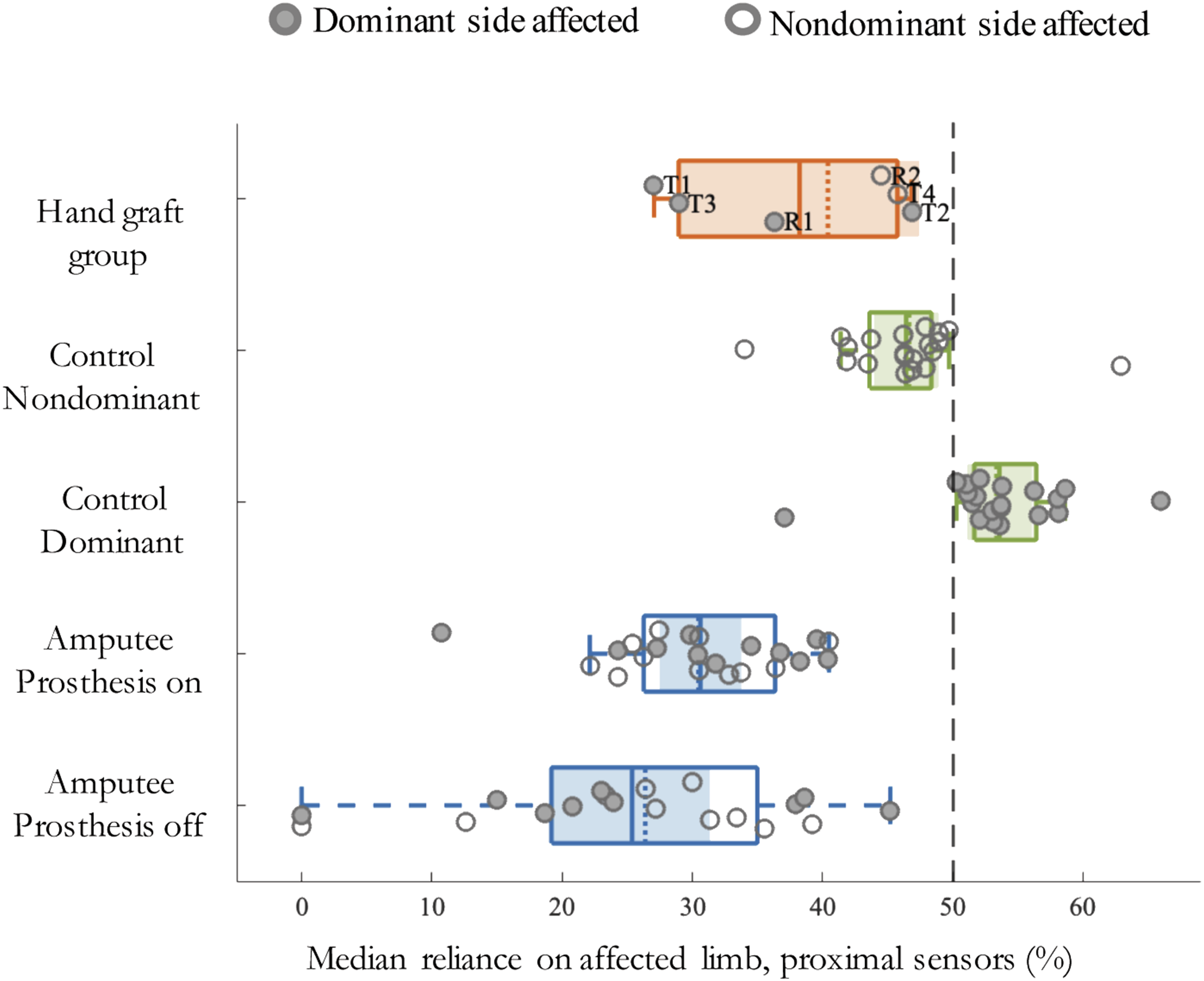
Following earlier work, 7 we used Archimedean spiral graphs to represent variation in %median reliance on the hands/prosthetic end-effectors across the 3 days for the individual hand graft recipients and representative amputee and control participants (see Supplementary Figure 1). These particular amputee and control cases were chosen because their %median reliance values were closest to the means of their respective subject groups. It is evident in these plots that patterns of limb use across time vary considerably between individuals, as would be anticipated given differences in their activities. When compared against the amputee case, the greater reliance by the hand graft group on the affected limb is evident here as well. It is also apparent that graft recipients still show greater reliance on their unaffected vs affected hands when compared to the representative control subject’s division of labor between dominant and nondominant sides.
Interlimb Reliance on the Upper Arms
Consistent with the distal level, data from the proximal sensors revealed that healthy controls also showed greater reliance on their dominant upper arms, with %median reliance significantly greater than 50%, (t (19) = 2.988, P = .008, Cohen’s d = 5.354; Figure 4, Table 2). In contrast, hand graft and amputee groups did not differ significantly in their reliance on the dominant vs nondominant upper arms. Instead, greater reliance on the unaffected vs affected side upper arm was detected in the hand graft patients (t (5) = −3.285, P = .022, Cohen’s d = 8.775), and in amputees both while wearing (t (21) = −12.854, P < .001, Cohen’s d = 7.073) and also while not wearing (t (18) = −8.631, P < .001, Cohen’s d = 12.436) their prostheses (Figure 4
Across the 3 days, amputees wore their prostheses an average of 78.9% of waking hours (11.1 h ± 1.8/day, range 2.9–15.1 h). When the analysis of upper arm activity was restricted to the period during which the prosthesis was being worn, hand graft and amputee groups again differed in their reliance on the affected side compared against either controls’ dominant (F (2, 45) = 63.408, P < .001, η2 = .738) or nondominant (F (2, 45) = 29.734, P < .001, η2 = .569) sides (Figure 4). Graft recipients averaged 25% greater reliance on the affected side than did the amputee group, (P = .049, Figure 4). Similar to what was observed at the distal hand level, both graft and amputee groups relied less on the affected side upper arm than controls relied on either their dominant or nondominant upper arms (P < .001 in both cases; Figure 4).
Because below-elbow amputees are known to use their residual limbs functionally in the absence of a prosthesis, we also evaluated the period during which the device was not being worn. When the analysis of proximal sensors’ activity was restricted to the period during which the prosthesis was not being worn, hand graft and amputee groups differed in their reliance on the affected side compared against either controls’ dominant (F (2,42) = 43.905, P < .001, η2 = .676) or nondominant (F (2, 42) = 24.537, P < .001, η2 = .539) sides. As reflected in median reliance below 50% (t (18) = −8.631, P < .001, Cohen’s d = 12.436), when the prostheses were not being worn, amputees continued to rely less on their unaffected vs injured upper arms (Figure 4). By comparison, the hand graft group averaged 50.7% more reliance on their affected side upper arm than did amputees during the period in which they were not wearing their prostheses, P = .017 (Figure 4). Reliance on the affected side upper arm by both hand graft and by amputee patients again fell short of controls’ reliance on their dominant or nondominant upper arms, P ≤ .033 in both cases.
Intralimb Reliance on the Biological or Prosthetic Forearms vs Upper Arms
Control of the location of the hand or prosthetic end-effector in the workspace involves coordinated movements of the forearms and upper arms. Our placement of sensors distally on the biological and prosthetic forearms, and also proximally on the upper arms allowed us to capture within-limb activity patterns. For all 3 groups, limb dominance had no effect on the extent to which they relied on the forearms/prostheses vs upper arms. Groups differed, however, in their reliance on the forearms/prostheses vs the upper arms when the patient groups’ injured sides were compared with either controls’ dominant (F (2, 45) = 70.085, P < .001, η 2 = .757) or nondominant (F (2,45) = 62.445, P < .001, η2 = .735) limbs. As indicated by median reliance on the forearm being greater than 50%, control subjects relied more on their forearms vs upper arms for both the dominant (t (19) = 11.867, P < .001, Cohen’s d = 7.659) and the nondominant limbs (t (19) = 11.126, P < .001, Cohen’s d = 7.460; Figure 3, Table 2). This reflects greater use of forearm movements in hand control during everyday activities. This same pattern was observed for the hand graft patients on both the affected (t (5) = 8.036, P < .001, Cohen’s d = 4.954) as well as the unaffected (t (5) = 7.651, P = .001, Cohen’s d = 7.524) sides, and for amputees with their unaffected sides (t (21) = 23.390, P < .001, Cohen’s d = 3.785). On their injured sides, amputees exhibited equivalent median reliance on the prosthetic forearm and upper arm. This suggests a less natural movement pattern with greater involvement of the upper arm in prosthesis end-effector control. By comparison, the hand graft recipients averaged 32.7% greater reliance on the affected forearm than what was observed for amputees, P < .001.
Further indication of a return to more natural patterns of intralimb coordination in hand graft patients can be seen in the fact that reliance on their affected side forearms vs upper arms did not differ significantly from what was observed in either controls’ dominant or nondominant sides. When compared with their own injured limbs, both hand graft (t (5) = −3.735, P = .014) and amputee (t (21) = −18.919, P < .001) groups showed less reliance on their grafted or prosthetic forearms vs their upper arms.
Finally, we failed to detect any significant relationships between age, time spent as an amputee, or the interval between amputation and receipt of the hand graft on either inter- or intralimb reliance.
Discussion
Evidence from lab- and clinic-based assessments suggest that amputees who undergo autologous hand replantation or allogeneic transplantation may exhibit higher levels of function compared with prosthesis users.14,15 Whether this extends to everyday life, however, is unknown, and addressing this question is important in weighing the risk-benefit ratios of these interventions.
To address this issue, we employed a novel wireless accelerometry protocol involving sensors positioned distally on the forearms/prostheses and proximally on the upper arms to evaluate upper limb use over 3 consecutive days. This novel protocol was a step further than previous work that used either only wrist-worn accelerometers on opposite limbs8,17,21 or sensors worn at the wrist level on the intact side and on the residual limb (upper arm) on the affected side. 9 We reasoned that if surgical hand grafts restore more naturalistic function during everyday life, then hand graft patients would exhibit greater reliance on the affected limb than amputees using prostheses. We found evidence consistent with this hypothesis and also additional limb use differences between hand graft recipients and amputees during everyday life, as discussed in detail below.
Data from distal sensors captured differences between our groups in use of healthy hands, grafted hands, and prosthetic end-effectors. While controls spent more time in bilateral vs unilateral activities, this was not the case for either hand graft patients or amputees. Hand graft recipients, however, engaged in more unilateral activity with their injured sides and less activity with their healthy hands than amputees using prostheses. Unilateral use of the affected hand by graft recipients was comparable to the healthy controls’ use of their nondominant hand.
During bimanual activities, the hand graft group averaged 147% more reliance on their grafted hands than amputees did on their prostheses. This is not to say, however, that hand graft recipients resume entirely normal limb use. In fact, reliance on the grafted hand was less than healthy controls’ reliance on either their dominant or nondominant hands.
Our amputee group excluded those who do not use prostheses. Among this below-elbow sample, we found a wide range of daily prosthesis use, from 2.9 to 15.1 hours per day. Although these individuals relied heavily on their intact hands, use of the prosthesis accounted for 12% of their unilateral activity and contributed to 30% of bimanual action. These results from individuals employing mechanical, myoelectric and passive devices are generally consistent with earlier findings from below-elbow myoelectric prosthesis users.8,22
Overall, these findings indicate that our hand graft recipients exhibited less over-reliance on the unaffected limb (“one-handedness”) than prosthesis users, instead making greater use of the affected hand during everyday life. This is an important observation because, as noted earlier, one-handedness is associated with a variety of negative outcomes, including poorer function, greater disability, and overuse injuries.2,11,12 Based on this result, we predict that hand graft patients will, on average, exhibit fewer of these negative outcomes than amputees who use prostheses. One potential reason is differences in the types and amounts of therapy that these 2 populations receive, and this is an important topic for future investigation.
We also collected data from proximal sensors located above the elbows on the upper arms. These data revealed important differences between groups in use of the upper arms. Compared with amputees during the time in which they were wearing their prostheses, the hand graft recipients averaged 25% more involvement of the affected side. This increased to 50.7% more reliance on their affected side upper arm when compared with the period during which amputees were awake and active but not wearing their prostheses. Similar to the hand, however, use of the affected upper arm by hand graft recipients fell short of controls’ use of either their dominant or nondominant upper arms.
Our use of sensors on the hands/prostheses and upper arm segments allowed us to assess intralimb coordination in these groups. Because of the degrees of freedom provided by the joints, the forearm can be moved independently of the upper arm when controlling hand position in the workspace. Like healthy controls, hand graft patients relied more on movements of the forearms vs upper arms on both the affected and unaffected sides. This was also true for the unaffected limbs of amputees, but not for the side with the prosthesis. Here, we found nearly equal reliance on movements of the upper arm and prosthetic forearm. This data indicate that grafted hand enables more natural patterns of limb use than conventional prostheses. Using prostheses require greater reliance on upper arm movements to control the end-effector position. It is possible that this less natural pattern of limb use in adults contributes to the more limited function on standardized measures reported in prosthesis users vs either hand replant or transplant patients.14,15 Interestingly, this heavier reliance on the proximal arm movements to control hand position is reminiscent of what we do as infants when learning to reach for objects. 23 In this early stage of life, the problem of controlling hand position is simplified by locking out some of the many degrees of freedom available in the arm; most notably at the elbow. As skill develops, these additional degrees of freedoms are allowed to vary and provide flexibility in the control of hand position.
This study is limited by a relatively small sample size, especially in the hand graft group. This makes it difficult to interpret the substantial individual variability that we detected in limb use within patient groups. Unsurprisingly, we failed to detect any clear relationships between individual variability in limb use and other variables such as time spent as an amputee prior to hand transplantation, the amount of prosthetic experience of the amputees, or the type of device they use. Additional work with larger samples is needed to evaluate whether these findings reflect reliable patterns across a wider range of individuals. Although we lack objective data on our amputee samples’ rehabilitation programs, it is safe to assume that our hand graft recipients went through a more extensive rehabilitation. This may have influenced differences in use of the affected limbs that were observed between these groups and is an important issue for future study. We also have only 1 female amputee in this study. This is below national average of 25%. 24 While upper limb movements differ between men and women (higher musculoskeletal load in women 25 ; higher mean acceleration in women 26 ), the asymmetry of upper limb movements measured through accelerometry in stroke survivors was not affected by sex. 27 Similarly, we do not expect that our findings of upper limb use symmetry are less applicable to a bigger hand graft recipients and amputee population due to our uneven gender representation.
Lastly, it is important to stress that limb use is but one consideration when comparatively evaluating these interventions. In a recent review, for example, the factors most strongly related to satisfaction with hand transplant were patient commitment and expectations. 13 Likewise, recent data indicate that the physiologic rejection rates of allogeneic hand transplants approximate the abandonment rates associated with limb prostheses. 15 The former relates to the collective risks of lifelong immunosuppression and associated health risks, while the latter is characterized by the absence of sensory input, the heat and pressures of prosthetic sockets, and limited functional dexterity. Our data suggest that both pathways restore a measure of bilateral function to the end user, with these gains more pronounced among those with hand transplantation.
Understanding the limb use during everyday life in this broader context will be key in making decisions about the best interventions for individual amputees.
Supplemental Material
sj-pdf-1-nnr-10.1177_15459683211062889 – Supplemental Material for Greater and More Natural Use of the Upper Limbs During Everyday Life by Former Amputees Versus Prosthesis Users
Supplemental Material, sj-pdf-1-nnr-10.1177_15459683211062889 for Greater and More Natural Use of the Upper Limbs During Everyday Life by Former Amputees Versus Prosthesis Users by Scott Frey, Binal Motawar, Buchanan Kelli, Christina Kaufman, Phil Stevens, Carmen Cirstea, and Sean Morrow in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgments
We thank Drs. Catherine Lang and Marghuretta Bland for providing initial help with accelerometry procedures and analyses.
Author Contributions
SHF conceptualized and designed the study. SHF and BM wrote the manuscript. BM and SHF analyzed the data and BM prepared figures and tables. KB coordinated the project, data collection, and organization. CK and PS identified and recruited participants and gave input on the manuscript. CMC and SM assisted with data collection and preprocessing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Department of Defense grant # MR140043 to S.H.F.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.