
Abstract
Background
Effective and sustainable exercise training methods for improving balance poststroke are needed.
Objective
To evaluate the effect of Baduanjin Qigong for improving balance after stroke.
Methods
This was a single-blinded randomized controlled study in which only the assessor was blinded. Fifty-eight people with chronic stroke (mean age: 62.5 ± 11.8 years) were randomly assigned to the experimental (n = 29) or control group (n = 29). The experimental group underwent 8 weeks of supervised Baduanjin training (3 sessions per week). This was followed by home-based practice of the same exercises 3 days a week for another 8 weeks. The control group underwent 2 sessions of supervised conventional fitness training in the first week, followed by home-based exercise practice 3 days a week until the end of week 16. All outcomes were measured at baseline, week 8, and week 16.
Results
Significantly greater improvements in the Mini-Balance Evaluation Systems Test (Mini-BESTest), composite equilibrium score (Sensory Organization Test), 5 Times Sit to Stand, and Timed Up and Go test were detected at week 8 in the experimental group than in the control group (P < .017). Further improvement in the Mini-BESTest was observed from week 8 to 16 in the experimental group (P < .001). Other outcomes (Limit of Stability, Fall-Efficacy Scale, Modified Barthel Index, Stroke-Specific Quality of Life) showed no significant results.
Conclusion
Baduanjin is effective in improving balance, leg strength, and mobility and is a safe and sustainable form of home-based exercise for people with chronic stroke.
Introduction
Balance dysfunction is common after stroke1-4 and is an important factor contributing to decreased walking ability and increased fall rate.1,5 Various exercise therapies have been used to manage balance dysfunction in individuals with stroke.6-8 Sustainability and adherence to exercise upon returning to community living are common challenges. Many training methods involve complex instructions and movements. These often require the supervision of health care professionals, adequate space, additional resources, and devices of considerable expense (eg, robotics, virtual reality).6-8 Because stroke is a chronic condition, a simple, easy-to-learn exercise program that can be conducted at home or in community-based settings is needed to enhance or maintain balance ability in a sustainable manner.
Baduanjin Qigong is a traditional Chinese exercise and is as popular as Tai Chi within the Chinese community. 9 It is rooted in the concept of Qi, which is an energy flow through a corporeal meridian system. 10 According to the philosophy of traditional Chinese medicine, an uninterrupted flow of Qi is essential for health and well-being. It is believed that “Qigong” (Qi: flow of energy; gong: work or exercise) facilitates the movement of Qi throughout the body, thereby improving health. 10 Similar to Tai Chi, Baduanjin Qigong is characterized by slow and fluid movements, mental focus, and controlled breathing. 9 The movements involved in Baduanjin require the individual to reach beyond the base of support, change the base of support between bilateral and unilateral stance, and perform movements in a sustained squatting posture. 9 These maneuvers challenge balance and require muscle strength to be executed successfully, thus making Baduanjin a potentially useful method for improving balance and leg strength. This may in turn confer benefits on other related functions such as mobility and activities of daily living.
Although Tai Chi and Baduanjin share similarities, there are distinct differences. Tai Chi is a form of Chinese martial art characterized by principles of attack and defense. It contains numerous, complex movement patterns and often takes several months or even years to master the skills. For example, the Ng style, one of the most popular Tai Chi styles, has 108 forms. 11 Baduanjin Qigong, on the other hand, has 8 movement forms, which are relatively less demanding. Baduanjin Qigong may thus be more appropriate for people with motor or cognitive deficits. 9 Assistive equipment is also not necessary during Baduanjin. These advantages make Baduanjin a potentially suitable form of exercise training for individuals with stroke in both home and community-based settings.
The scientific evidence regarding the use of Baduanjin Qigong in stroke rehabilitation is limited. Systematic reviews by Chen et al 12 (9 studies) and Lyu et al 13 (21 studies) showed that traditional Chinese exercises (Tai Chi, Baduanjin, and others) improved balance in people with stroke. However, the quality of overall evidence was considered very low, and the results were not specific to Baduanjin. Only 2 of the reviewed studies were Baduanjin exercise trials. A systematic review and meta-analysis by Zou et al 9 specifically addressed the effects of Baduanjin training poststroke and found that Baduanjin induced a significant improvement in balance. However, assessors were not blinded, and overall risk of bias was high in all 6 randomized trials (8 articles) included in the review. Furthermore, only 1 or 2 outcomes were measured in these trials. Another limitation is that only 1 of the reviewed studies (2 articles) involved people with chronic stroke, which did not measure balance and mobility.14,15 A comprehensive evaluation of the effects of Baduanjin on different aspects of physical functioning after stroke is currently lacking. The efficacy of unsupervised, home-based Baduanjin programs is also unknown.
To address the knowledge gaps and limitations of previous Baduanjin studies in stroke, an assessor-blinded randomized controlled study was undertaken to investigate the effects of a 16-week Baduanjin Qigong practice program on balance, mobility, leg strength, fall efficacy, activities of daily living, and quality of life among people with chronic stroke. It was hypothesized that 8 weeks of supervised Baduanjin training would lead to significant improvement in the aforementioned outcomes among people with chronic stroke compared with conventional exercise training. It was also hypothesized that the treatment effect induced by Baduanjin training within the first 8-week period would be sustained following an additional 8 weeks of unsupervised home-based practice.
Methods
Study Design
This was an assessor-blinded randomized controlled trial with 2 treatment arms (Baduanjin vs conventional exercise training). This study was registered at ClinicalTrials.gov (NCT02999464). Ethical approval was granted by the institutional review board of the clinical institution in which the study was conducted (Approval Number: KC/KE-16-0063/ER-2) and the Human Research Ethics Subcommittee of the university that the principal investigator was affiliated with (Approval Number: HSEARS20151013001).
Participants and Sample Size
Adults with stroke were recruited from an outpatient center of a local hospital using convenience sampling by a researcher not involved with the group allocation, intervention, or outcome assessments. The inclusion criteria were as follows: (1) a diagnosis of stroke >3 months, (2) stable medical condition, (3) able to stand for more than 15 minutes, (4) able to take anteroposterior and lateral steps without assistance or walking aid, (5) able to follow simple verbal commands, and (6) Modified Rankin Scale (MRS) score of ≤3 (1: No significant disability despite symptoms, able to carry out all usual duties and activities; 2: Slight disability, unable to carry out all previous activities, but able to attend to personal affairs without assistance; 3: Moderate disability, requiring some help, but able to walk without assistance). 16 The exclusion criteria were as follows: (1) other neurological disorders, (2) previous Qigong experience, (3) cognitive impairment as indicated by Abbreviated Mental Test score <7, 17 and (4) other severe illnesses (eg, cancer). All participants gave written informed consent before participation in the study. The study participants were enrolled between December 2016 and February 2018.
The sample size estimation was performed using G Power 3.1 software (Universität Düsseldorf, Germany). None of the previous Baduanjin studies used the Mini-Balance Evaluation System Test (Mini-BESTest) as a primary outcome. 9 Therefore, previous results for balance using the Berg Balance Scale (BBS) and functional mobility using the Timed Up and Go (TUG) test were used to estimate the required sample size. Most studies showed that traditional Chinese exercises induced a significant effect on BBS (Hedges’ g: 0.56-6.34) and TUG (Hedges’ g: 0.73-2.22), with medium to very large effect sizes.9,13 For the purposes of our study, a more conservative approach using the smallest value within this range was assumed (Hedges’ g = 0.56, equivalent to f = 0.28 for ANOVA analysis). Based on a 2 × 3 two-way repeated measures analysis of variance (ANOVA), with an α value of .05, power of 80%, and an attrition rate of 15%, the minimum sample size required to detect a significant Group × Time interaction effect would be 56 participants (28 in each group).
Randomization
Eligible participants were randomized to either the Baduanjin or control group (ie, conventional exercise training) using sequentially numbered sealed opaque envelopes. All randomization procedures were performed by a researcher who was not involved in the recruitment of participants, exercise training, or outcome evaluation. Given that the participants were recruited continuously as the trial progressed rather than at a single point in time, a permuted-block randomization method was used to ensure equal sample sizes between groups over time.18,19 Whenever 4 individuals were successfully recruited, the randomization procedure (ie, block size = 4) was conducted with an allocation ratio of 1:1 (ie, 2 assigned to the experimental group, 2 to the control group).18,19 Because we were able to recruit 6 participants for the last block, these participants were randomized to groups as 1 block (block size = 6; 3 assigned to the experimental group, 3 to the control group).
Intervention
The experimental group engaged in 8 weeks (3 days per week) of Baduanjin training in an outpatient physiotherapy department. All Baduanjin training was provided by a physiotherapist who was also a Baduanjin instructor. Each session was approximately 50 minutes in duration, consisting of 10 minutes of warm-up exercises, 30 minutes of Baduanjin practice, and 10 minutes of cool-down exercises. The Baduanjin program involved 8 exercises (forms; Figure 1). After the 8-week supervised training period, participants practiced the same exercises unsupervised from home 3 days a week for another 8 weeks. Thus, the total exercise duration was 150 minutes per week. This protocol was chosen because most previous Tai Chi or Baduanjin trials reporting benefits in persons with stroke had a program duration of 6 to 24 weeks, with a total exercise time of 120 to 300 minutes per week.9,12,13
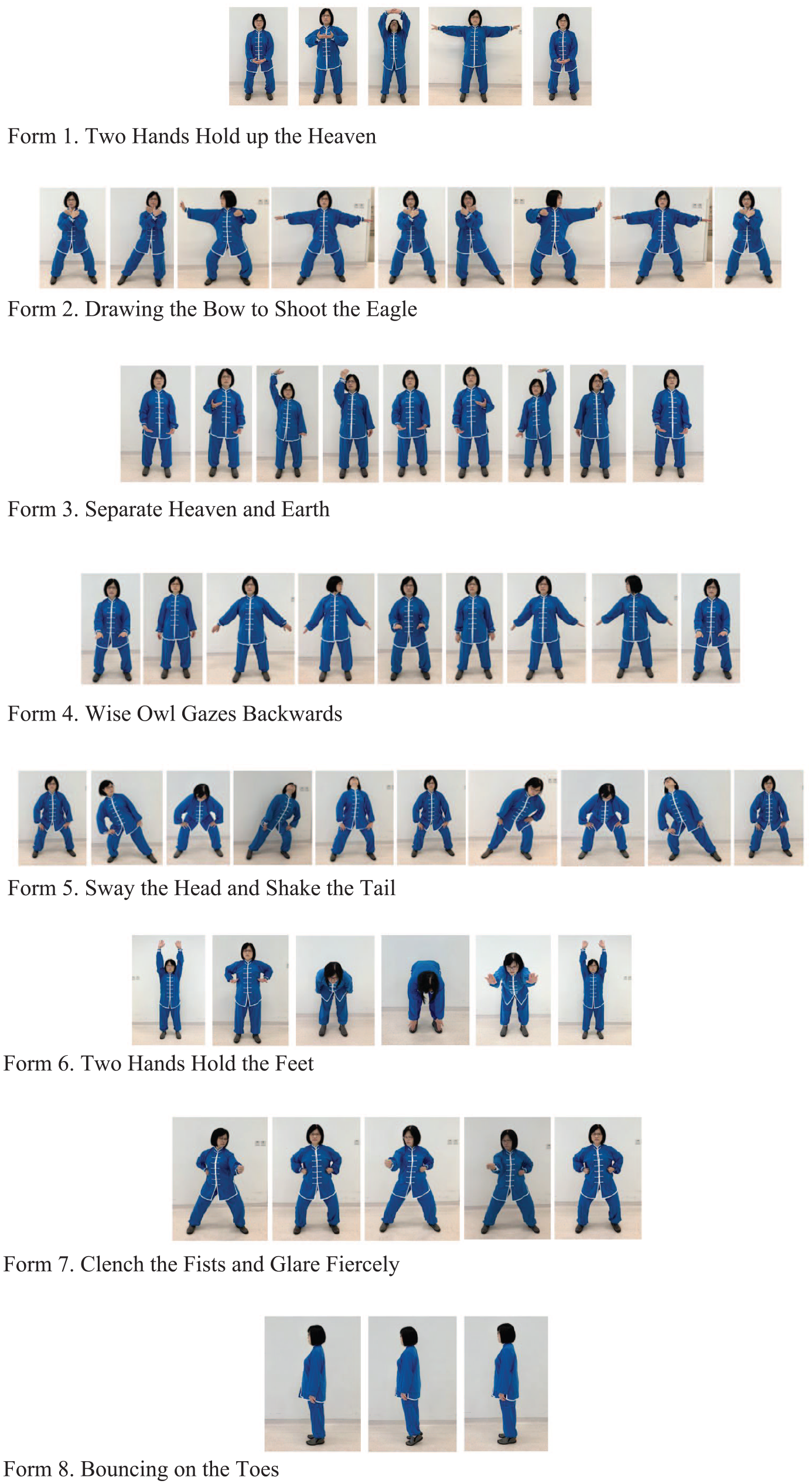
Eight forms of Baduanjin.
Control group participants were taught upper- and lower-limb stretching, strengthening, weight shifting, and breathing exercises. All control group participants received 2 sessions of supervised training conducted by a physiotherapist within the first week. The duration of each session was the same as in the Baduanjin group (50 minutes). Participants were instructed to do the same exercises at home at a session frequency of 3 days a week until the end of week 16.
To facilitate home-based practice, leaflets with exercise illustrations were provided to both groups of participants. In addition, a weekly phone call was made by the researchers to check the physical health status of the participants in both groups, to confirm whether the exercise protocols were being followed, and to address any concerns regarding the program.
For both groups, attendance was recorded during the supervised sessions. To measure adherence to the home-based exercise component, an exercise diary was given to each participant to record whether they performed the prescribed exercises as scheduled.
Outcome Assessments
Demographic data were obtained from medical records and participant interviews during the baseline assessment session. The MRS was used to indicate the severity of stroke-induced disability at baseline. 16 All outcome assessments were conducted in an outpatient physiotherapy unit by a physiotherapist with more than 5 years of clinical experience who was blinded to the group allocation. The following primary and secondary outcomes were assessed at 3 time points (ie, baseline, week 8, and week 16).
Primary Outcome
Mini-Balance Evaluation Systems Test (Mini-BESTest): The Mini-BESTest is a reliable and valid 14-item tool for assessing dynamic balance in people with chronic stroke (score range: 0-28).20,21 A higher score denoted better balance ability. It measures 4 domains of balance function: anticipatory postural adjustment, reactive postural control, sensory orientation, and dynamic gait. These represent important functional aspects of balance required to accommodate various challenges encountered during community ambulation. 22 Because our target participants were community-dwelling individuals with chronic stroke, a more comprehensive assessment of dynamic balance was required. There are also an increasing number of studies using the Mini-BESTest despite the relatively short time frame since its inception in 2010. 21 For these reasons, the Mini-BESTest was chosen as the primary outcome. Other balance or mobility assessments were chosen as the secondary outcomes because they were either single-item assessments (ie, Limit of Stability Test, 5 Times Sit to Stand [FTSTT], TUG) or measures of static standing balance (ie, Sensory Organization Test) and, therefore, provided a less comprehensive picture of balance function and may have a more limited role in directing treatment.20,22
Secondary Outcomes
Limits of Stability Test
The Limits of Stability Test is a valid and reliable measure of dynamic postural stability, 23 which measures the farthest distance an individual can move away from a vertical position without altering the base of support, taking a step, or falling. 24 Participants were asked to remove footwear, socks, and any ankle-foot orthoses and stand barefoot on the Smart Balance Master System (NeuroCom System Version 7.0.6, NeuroCom International Inc, Clackamas, OR) with an upright posture. Each participant was protected by a harness, with their arms placed alongside their body and their feet in a designated position on the device force platform. Participants were instructed to lean their body toward a target displayed on a computer screen by shifting their center of gravity within their original base of support as far, precisely, and rapidly as possible for an 8-s duration. Reaction time was the time in seconds from the cue appearance and the center of gravity movement onset toward the target position. The end-point excursion was the extent of the center of gravity movement and was calculated as a percentage of the built-in norm (NeuroCom software). The reaction time and end-point excursion of the 8 targets spaced at 45° apart around the center of gravity were registered and averaged by the system software. The mean reaction time and end-point excursion values were used for analysis. Shorter composite reaction time and larger composite end-point excursion indicated better dynamic postural stability.
Sensory Organization Test
The Sensory Organization Test is a reliable and valid measurement used to evaluate the sensory organization of balance control. 25 The starting position was the same as the Limit of Stability Test (NeuroCom System Version 7.0.6, NeuroCom International Inc, Clackamas, OR). In each 20-s trial, participants were asked to maintain an upright standing posture. The system detected the path of the center of gravity. After a practical trial, participants underwent 3 trials in each of the 6 sensory conditions (eyes open, eyes closed, eyes open with sway-referenced surround, eyes open with sway-referenced support surface, eyes closed with sway-referenced support surface, eyes open with sway-referenced surround and support surface). An equilibrium score was generated for each sensory condition. 26 The composite equilibrium score was the average of the 6 sensory conditions, with scores ranging from 0 to 100 (0 = sway beyond limits of stability; 100 = no sway).
Five Times Sit to Stand
The FTSTT test is a measure of functional muscle strength and balance27,28 and has demonstrated reliability and validity in assessing individuals with stroke. 28 Participants were asked to stand up and sit down 5 times as rapidly as possible with their arms folded and their back against a standard armchair. A practice trial was given before data collection. Less time to completion was indicative of better performance.
Timed Up and Go
The TUG test is a reliable and valid timed walking test used to assess functional mobility. 29 Participants were asked to “rise and stand from a standard armchair, walk a distance of 3 meters, turn around, walk back to the chair, and sit down.” 29 The time taken to complete the test was documented. Less time to completion was indicative of better functional mobility.
Fall Efficacy Scale—International
A validated Chinese version of the Fall Efficacy Scale—International was used to assess fear of falling (score range: 16-64). 30 Higher scores indicate greater fear of falling.
Modified Barthel Index
The Modified Barthel Index was used to assess independence in performing activities of daily living (score range: 0-100). 31 Higher scores indicate greater independence.
Stroke-Specific Quality of Life
The Stroke-Specific Quality of Life Scale is a valid and reliable patient-reported outcome assessing the health-related quality of life for people with stroke (score range: 49-245). 32 Higher scores indicate better quality of life.
Statistical Analysis
All data were analyzed with SPSS software (version 26.0, IBM, Armonk, NY). Baseline differences in demographic characteristics and outcome measures between the experimental and control groups were compared using independent t-tests, Mann-Whitney U tests, or χ2 tests, depending on whether the criteria for parametric statistics were met. For each outcome, 2-way repeated-measures ANOVA (mixed design; within-subject factor: time [3 levels]; between-subject factor: group [2 levels]) was used to compare the effect between experimental and control treatments. Baseline characteristics that showed significant between-group differences served as covariates (ie, analysis of covariance). Post hoc analyses were performed if a significant Group × Time interaction effect was found. Post hoc within-group differences at various time points were analyzed using paired t-tests. Between-group comparisons for change scores were done using independent t-tests. Statistical significance was defined as P <.05 (2-tailed). The significance level of the post hoc analyses was adjusted to P <.017 (ie, 0.05/3; Bonferroni correction) as a result of multiple comparisons.
Exercise program adherence was compared between the 2 groups for the first period (weeks 1-8), second period (weeks 9-16), and the full study duration (16 weeks) using Mann-Whitney U tests. Within-groups change in exercise adherence between weeks 1 and 8 and weeks 9 and 16 was assessed using Wilcoxon tests.
An intention-to-treat approach with the last observation carried forward method was first used for data analysis. Any missing observations were substituted by the last available data. This was followed by a per-protocol analysis, in which only participants who completed all assessments were included in the analysis. If the results generated from the intention-to-treat analysis and per-protocol analysis were similar and led to the same conclusion, confidence in the study results was increased. 33
Results
The first study participant was enrolled in December 2016. A total of 58 participants met the inclusion criteria and were randomly assigned to either the experimental (n = 29) or control group (n = 29). Two participants in the experimental group and 5 individuals in the control group dropped out for different reasons (Figure 2). Another participant in the control group was found to be participating in another study after baseline assessment and was thus excluded from the per-protocol analysis. There was no significant difference in attrition rate (χ2 = 2.320; P = .128). The remaining 50 (experimental:control = 27:23) participants completed all outcome assessments. The last participant completed the outcome assessments in June 2018.
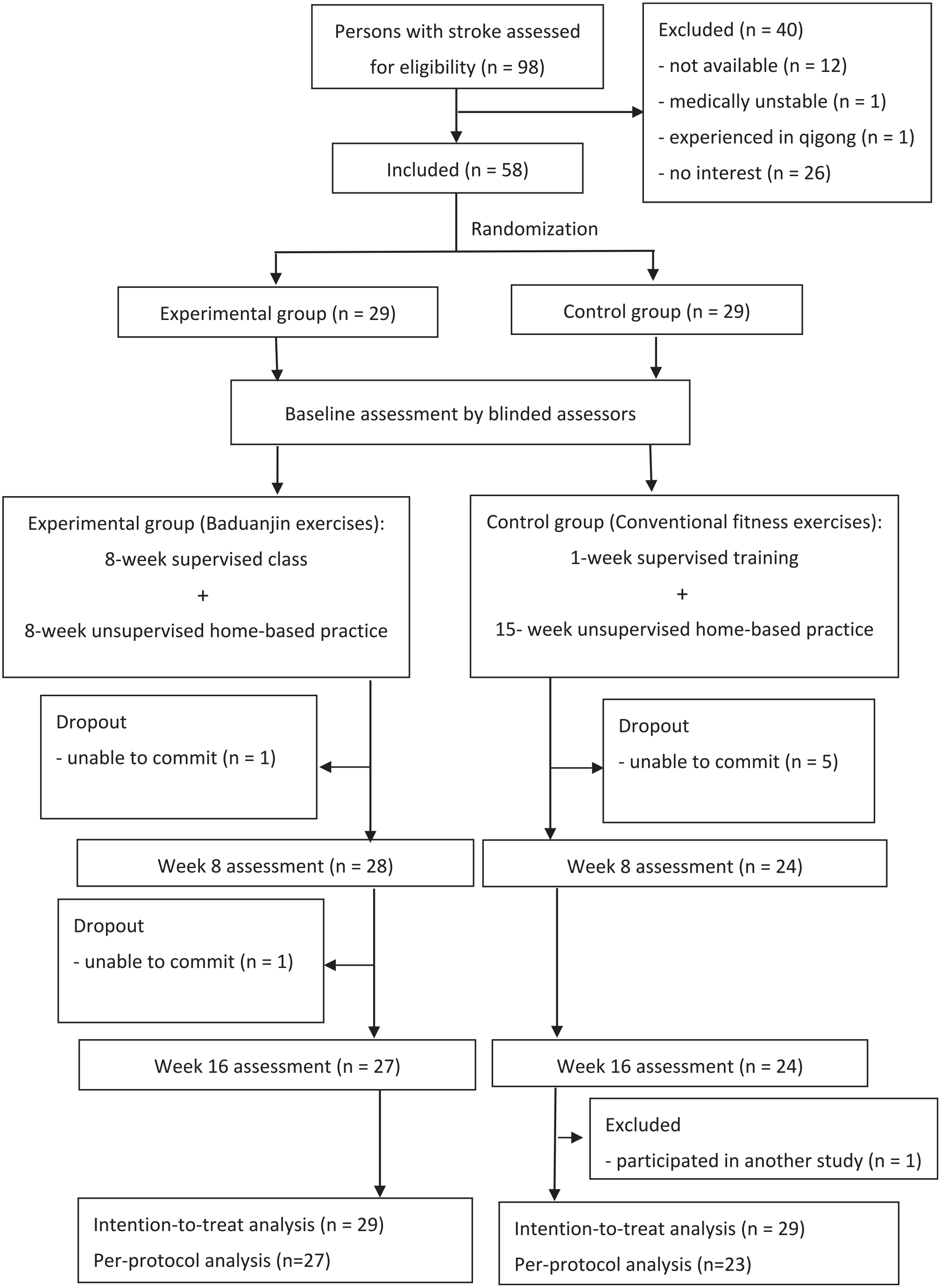
CONSORT flowchart diagram.
Table 1 describes the demographic characteristics of the participants. In general, the number of participants who had MRS ratings of 1, 2, and 3 were 23 (39.7%), 23 (39.7%), and 12 (20.7%), respectively. The mean Mini-BESTest score of the total participant sample was 18.1, indicating a moderate deficit in balance function. 34 The average TUG score (17.8 s) also indicated impaired functional mobility. Furthermore, it was well above the cutoff point attributed to fall risk among people with chronic stroke (14 s), suggesting that our participants were generally at risk of falling. 35 There were no significant between-group differences in key demographic characteristics (eg, age, sex, stroke onset, MRS scores; P > .05). Most outcomes did not significantly differ between groups at baseline (P > .05). The control group had a slightly higher Mini-BESTest score by an average of 2 points (P = .040) and a shorter time to complete the FTSTT by an average of 3.6 s (P = .028; Table 2). These variables were, thus, entered as covariates in our ANOVA model when analyzing the treatment effect. Between-group baseline comparisons generated similar results after excluding dropouts (Supplemental Table 1).
Demographic and Clinical Characteristics of Participants.

Intention-to-Treat Analysis (n = 58): Time × Group Interaction and Time Effect.

Abbreviations: Mini-BESTest, Mini Balance Evaluation Systems Test; LOS, limits of stability; RT, reaction time; EPE, end-point excursion; SOT, Sensory Organization Test; ES, equilibrium score; FTSTT, 5 Times Sit to Stand test; TUG, Timed Up and Go test; FES-I, Fall Efficacy Scale—International; MBI, modified Barthel index; SS-QOL, Stroke-Specific Quality of Life Scale.
Significant difference compared with baseline (paired t test, P < .017).
Significant result (ANOVA, P < .05).
We were able to obtain the exercise logs of all participants except for the dropouts (experimental: n = 27; control: n = 23). For experimental group participants, the attendance rate for supervised sessions during weeks 1 to 8, weeks 9 to 16, and the entire 16-week study period was high (>90%; Table 3). There were no significant between-group differences in exercise adherence rates for any of the 3 periods (P > .05). Also, none of the groups demonstrated any significant change in exercise adherence between weeks 1 to 8 and weeks 9 to 16 (P > .05). None of the participants, regardless of group assignment, reported adverse effects.
Exercise Adherence Rate.

Intention-to-treat analysis revealed a significant Time × Group interaction (P < .001) for the Mini-BESTest (Table 3), composite equilibrium score (ie, Sensory Organization Test; P < .001), FTSTT (P < .001), and TUG (P = .015). Post hoc analyses indicated that these outcomes improved significantly in the experimental group (P ≤ .017) between baseline and week 8. The Mini-BESTest scores continued to improve from week 8 to week 16 in the experimental group (P < .001). The composite equilibrium score (P < .001), FTSTT (P < .001), and TUG (P < .001) did not significantly improve during the home-based period but were significantly better compared with baseline scores (P ≤ .017). In contrast, the control group showed no significant change in these outcomes over time. The only exception was the composite equilibrium score, which showed a significant decrease at week 8 (P = .006) but returned to baseline values by week 16 (P = .372). For post hoc comparisons of change scores between groups, the experimental group demonstrated significantly greater improvement in the Mini-BESTest (P < .001), composite equilibrium score (P = .001), FTSTT (P < .001), and TUG (P = .005) at week 8, which was also maintained at week 16 (P < .001; Table 4). Neither the Time × Group interaction nor the time effect was significant for the other outcomes (Table 3).
Change Scores and Effect Sizes.

Abbreviations: Mini-BESTest, Mini Balance Evaluation Systems Test; LOS, limits of stability; RT, reaction time; EPE, end-point excursion; SOT, Sensory Organization Test; ES, equilibrium score; FTSTT, 5 Times Sit to Stand test; TUG, Timed Up and Go test; FES-I, fall efficacy score-international; MBI, modified Barthel index; SS-QOL, stroke-specific quality of life scale.
Significant difference compared with the control group (independent t-test, P < .017).
Significant at 95% level of confidence.
The above analyses were repeated after excluding dropouts (ie, per-protocol analysis; n = 50). The results (experimental group: n = 27; control group: n = 23), were similar to those generated by the intention-to-treat analyses (Supplementary Tables).
Discussion
The results indicated that the Baduanjin group showed a significant improvement in the Mini-BESTest score, composite equilibrium score, FTSTT, and TUG in comparison to the control group after the 8-week training period. These outcomes remained better than the control group after another 8 weeks of home-based Baduanjin practice.
Improvement in Balance Function
The Mini-BESTest score improved significantly after 8 weeks of Baduanjin training. It continued to improve between weeks 8 and 16, suggesting that the home-based practice also improved balance ability. In this study, mean improvement in the Mini-BESTest score for the experimental group was 5.6 points greater than for the control group after 16 weeks of Baduanjin training (Table 4). The minimal clinically important difference value of the Mini-BESTest was found to be 4 points for balance disorders. 36 Our results indicate that Baduanjin training contributed to a clinically meaningful change in Mini-BESTest scores. The dynamic nature of the Baduanjin exercises may partially explain why the experimental group had a clinically meaningful improvement in the Mini-BESTest, which is a measure of dynamic balance.
The experimental group also had greater improvement in the composite equilibrium score derived from the Sensory Organization Test at week 8 and at 16-week follow-up, suggesting that the sensory organization component of balance was enhanced after Baduanjin training. After 16 weeks of Baduanjin practice, improvement in the composite equilibrium score was 9.1% higher in the experimental group than the control group (Table 4), which exceeded the minimal detectable change value found in patients with vestibular disorders (8%). 37 Effective balance control involves organization and integration of sensory information. During Baduanjin practice, different senses are required to engage in different Qigong movement forms (Figure 1). For instance, in practicing the Two Hands Held Up the Heavens, The Wise Owl Gazes Backward, and Clench the Fists and Glare Fiercely forms, a wide field of view is required for looking at the hands, looking backward, and looking at the fist, respectively. The vestibular system is also involved when performing the head and neck movements in The Wise Owl Gazes Backward and Sway the Head and Shake the Tail. Engaging in repetitive Baduanjin exercises may have enhanced balance ability in our participants by improving the integration of sensory information required for effective balance control.
Four previous Baduanjin studies in stroke have incorporated balance as an outcome measure. These studies reported a significant improvement in BBS scores after 6 to 12 weeks of Baduanjin practice in people with subacute stroke, with an overall standardized mean difference of 2.39.9,38-41 Although smaller than those reported in subacute stroke trials, the standardized mean differences obtained in our study at week 16 were still considered large (1.63 and 1.06 for the Mini-BESTest and composite equilibrium score, respectively; Table 4). The differences in participant characteristics (eg, chronicity) and balance outcome measures used may have contributed to the different effect sizes reported. Nevertheless, our results in people with chronic stroke are largely in line with previous studies demonstrating the efficacy of Baduanjin training for improving balance function poststroke.
Improvement in Leg Strength and Mobility
The FTSTT performance improved significantly in the experimental group after 8 weeks of training and was well maintained at the 16-week follow-up point. At the end of the 16-week study period, the improvement in FTSTT gained by the experimental group was 5.4 s more than the control group, which exceeded the minimal clinically important difference value of 2.3 s established in people with vestibular disorders (Table 4). 42 The results thus suggest that Baduanjin training induced clinically meaningful changes in leg strength and balance.
Baduanjin exercises also require the individual to move to and away from a semisquatting posture with coordinated concentric and eccentric knee-joint muscle control. The combination of concentric and eccentric contractions during training has been shown to be more effective for improving muscle strength than concentric training alone. 43 Movements during Baduanjin practice also resemble those required in many daily activities (sit-to-stand, transfers, picking up objects from the floor, managing stairs, etc), which may account for the improvement in FTSTT among the experimental group participants.
The TUG performance also improved significantly in the experimental group relative to the control group at week 8 and week 16. The improvement in balance ability (Mini-BESTest, composite equilibrium score) and leg muscle strength (FTSTT) may partly explain the observed gain in functional mobility (TUG). These factors have been shown to be highly correlated with mobility function.29,44 The improvement in TUG performance observed in the experimental group was, on average, 3.5 s faster than the control group at week 16. This is comparable to the minimal detectable change of the TUG (2.9 s) in people with chronic stroke. 45 Although the quality of evidence was considered very low, a meta-analysis (based on 4 studies) showed that Tai Chi was effective in improving TUG performance in people with stroke, with a standardized mean difference of 2.59. 13 None of the previous Baduanjin trials measured leg strength or mobility. 9 Thus, our study is the first to demonstrate that Baduanjin training is effective in improving leg strength and mobility poststroke.
Other Outcomes
No significant between-group difference was detected in other secondary outcomes (eg, Modified Barthel Index, Stroke-Specific Quality of Life, etc). A previous study reported that 12 weeks of Baduanjin training improved Barthel Index scores in persons with chronic stroke. 15 Two previous studies also reported better quality of life (as measured by the Health Organization Quality of Life and 36-Item Short Form Survey) after 6 to 12 weeks of Baduanjin training.14,46 There are several reasons that may explain the discordance between our results and those of previous studies. First, the experimental treatment duration was longer in previous studies. The Baduanjin training was also added to usual care (eg, education, other exercises), whereas the control group received usual care only. In our study, each of the 2 treatment arms had different types of exercise training, but the prescribed exercise frequency and duration were equivalent. Second, the lack of treatment effect on Modified Barthel Index scores may be the result of a ceiling effect. The mean Modified Barthel Index scores of both groups were >90/100 at different time points, indicating that the participants in this study were quite independent in their daily activities. Finally, only balance and mobility outcomes were used to estimate the sample size of this study. This study may be underpowered to detect significant treatment effects in some of the secondary outcomes. A multicentered study with a larger sample size is warranted to further examine the therapeutic effects of Baduanjin on these outcomes in people with stroke.
Supervised Training Versus Unsupervised Home-Based Practice
Whether the benefits gained from supervised Baduanjin training can be enhanced or maintained by home-based practice is an important question. This is an essential aspect of chronic disease self-management and living a healthy lifestyle. Only the Mini-BESTest scores showed significant improvement during the home-based exercise period in the experimental group. The degree of improvement was also less in the home-based practice period than after the first 8-week supervised training period (Table 4). Although the composite equilibrium scores, TUG and FTSTT showed significant improvement for these outcomes in the first 8 weeks, the degree of improvement in the subsequent home-based practice period did not reach statistical significance. One possible explanation of the lesser effect during the home-based practice period was that the participants’ functional status was approaching, or had already reached, a plateau at week 8. Further practice may not induce the same degree of improvement. Another explanation was the placebo effect related to the attention from and/or interaction with the Baduanjin instructor. Finally, it cannot be completely ruled out that exercise adherence during the home-based practice period might be lower than reported. Because the data on exercise adherence during the home-based period were based on subjective reports, the results may be subject to overreporting and an inherent desirability bias. Nevertheless, the sustained improvement in these outcomes observed among the experimental participants at week 16 was significantly better than that in the control group. A possible conjecture of this finding is that the benefits gained from the supervised training sessions may extend beyond this initial 8-week period with continued home-based practice.
Attrition, Exercise Compliance, and Safety
The overall attrition rate of the study was 13.7%, which was considered acceptable according to the criterion stated in the PEDro Scale, a common tool to assess methodological quality. 47 Although not statistically significant, the control group had a higher attrition rate than the experimental group. Possible reasons may be a lack of motivation, less interaction with the Baduanjin instructor, or an undervalued perception of the potential exercise benefits. However, the confounding effect of attrition should be minimal. The dropouts did not have a substantial impact on baseline demographic and clinical characteristics between groups. In our analysis of the treatment effect, the results from the intention-to-treat analysis were similar to those obtained from the per-protocol analysis.
The exercise adherence rate in this study was high in both groups throughout the study period, which was comparable to previous reports (85%-100%).48-50 The high exercise compliance observed in this study might be result of the impact of weekly telephone calls intended to reinforce the importance of regular exercise. No adverse events were reported throughout the study period, indicating that Baduanjin is a safe exercise intervention for individuals with chronic stroke.
Limitations
This study has several limitations. First, a convenience sampling method was adopted and all participants were recruited from the same hospital, which may have decreased the representativeness of the sample. The results can only be generalized to those who have demographic and clinical characteristics similar to those of our study participants. Second, blinding of the participants was not feasible in this study because of the differences in the nature of the 2 training programs. Third, the amount of supervision received by the experimental group participants (ie, 24 supervised sessions) was more than the control group (ie, 2 supervised exercise sessions). Baduanjin was a novel exercise for the participants. Therefore, more time was required for the participants to learn and master the techniques in the initial stage. This factor may have had a confounding influence on the results. Fourth, despite the randomized group allocation, there were significant differences for the Mini-BESTest and FTSTT scores at baseline, which may also be confounding factors. Nevertheless, we attempted to address this problem by using the baseline values of these outcomes as covariates. In addition, between-group differences in these outcomes at baseline were relatively small. For example, the 2-point difference in the Mini-BESTest scores between the 2 groups at baseline was below the minimal detectable change value previously established in chronic stroke populations. 20 Fifth, this study was not designed to address the question of whether the supervised Baduanjin training had a carryover effect after a period of no or less intervention (eg, no home-based practice). However, we felt that the implementation of home exercise practice after training under supervision was a better reflection of current clinical practice in stroke rehabilitation. Finally, the primary aim of our study was to establish whether Baduanjin Qigong had any effect on balance. Therefore, the exercises for the control group had a minimal amount of balance training components. Once the benefits of Baduanjin are established, further study can be done to compare whether Baduanjin Qigong is more or less effective than other types of balance training commonly used in stroke rehabilitation.
Conclusion
This study demonstrated that Baduanjin training was effective in improving balance, leg muscle strength, and mobility among people with chronic stroke relative to traditional fitness training. Baduanjin Qigong can be considered a safe and sustainable form of exercise that can be incorporated in stroke rehabilitation programs.
Supplemental Material
sj-doc-1-nnr-10.1177_15459683211005020 – Supplemental material for Baduanjin Qigong Improves Balance, Leg Strength, and Mobility in Individuals With Chronic Stroke: A Randomized Controlled Study
Supplemental material, sj-doc-1-nnr-10.1177_15459683211005020 for Baduanjin Qigong Improves Balance, Leg Strength, and Mobility in Individuals With Chronic Stroke: A Randomized Controlled Study by Mandy Yuen, H. X. Ouyang, Tiev Miller and Marco Y. C. Pang in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-1-nnr-10.1177_15459683211005020 – Supplemental material for Baduanjin Qigong Improves Balance, Leg Strength, and Mobility in Individuals With Chronic Stroke: A Randomized Controlled Study
Supplemental material, sj-docx-1-nnr-10.1177_15459683211005020 for Baduanjin Qigong Improves Balance, Leg Strength, and Mobility in Individuals With Chronic Stroke: A Randomized Controlled Study by Mandy Yuen, H. X. Ouyang, Tiev Miller and Marco Y. C. Pang in Neurorehabilitation and Neural Repair
Footnotes
Authors’ Note
Trial registry name: Effect of Qigong on Balance, Fall Efficacy, Wellbeing of People With Stroke in Hong Kong (ClincalTrials.gov, NCT02999464).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.