
Abstract
Background
Declines in gait parameters are common with aging and more pronounced in tasks with increased executive demand. However, the neural correlates of age-related gait impairments are not fully understood yet.
Objectives
To investigate (a) the effects of aging on prefrontal cortex (PFC) activity and gait parameters during usual walking, obstacle crossing and dual-task walking and (b) the association between PFC activity and measures of gait and executive function.
Methods
Eighty-eight healthy individuals were distributed into 6 age-groups: 20-25 (G20), 30-35 (G30), 40-45 (G40), 50-55 (G50), 60-65 (G60), and 70-75 years (G70). Participants walked overground under 3 conditions: usual walking, obstacle crossing, and dual-task walking. Changes in oxygenated and deoxygenated hemoglobin in the PFC were recorded using functional near-infrared spectroscopy. Gait spatiotemporal parameters were assessed using an electronic walkway. Executive function was assessed through validated tests.
Results
Between-group differences on PFC activity were observed for all conditions. Multiple groups (ie, G30, G50, G60, and G70) showed increased PFC activity in at least one of the walking conditions. Young adults (G20 and G30) had the lowest levels of PFC activity while G60 had the highest levels. Only G70 showed reduced executive function and gait impairments (which were more pronounced during obstacle crossing and dual-task walking). PFC activity was related to gait and executive function.
Conclusions
Aging causes a gradual increase in PFC activity during walking. This compensatory mechanism may reach the resource ceiling in the 70s, when reduced executive function limits its efficiency and gait impairments are observed.
Introduction
Declines in gait parameters are common with aging and associated with changes in executive function.1-4 In comparison with young individuals, older adults demonstrate reduced executive function 5 and walk with shorter and slower steps and greater step-to-step variability.4,6 More pronounced gait impairments are observed during tasks with increased executive load,7-9 such as obstacle avoidance and dual-task walking (ie, performing a concomitant secondary task while walking). These findings suggest that deficits in executive function, which is primarily moderated by the prefrontal cortex, contribute to gait impairments. In fact, even subclinical changes in executive function are linked to diminished gait performance in community dwelling older adults. 10 Such findings have aroused interest in monitoring prefrontal cortex activity during walking.
Functional near-infrared spectroscopy (fNIRS) has been used to examine the effects of aging on prefrontal cortex activity during different walking tasks. The prefrontal cortex is part of the executive locomotor pathway11,12 and is argued to become activated when the automatic execution of walking is reduced,13,14 which may occur due to impaired neural function and increased attentional/executive task demand. Accumulating evidence demonstrate that older adults present greater activation of the prefrontal cortex than young adults during usual walking (ie, single walking).15-17 Additionally, higher prefrontal activation is associated with increased gait variability (ie, a surrogate measure of gait automaticity where higher variability equates to reduced automaticity) in older adults. 18 Such findings suggest that older adults rely on executive resources to compensate for the loss of gait automaticity.13,14,18
fNIRS studies on obstacle negotiation and dual-task walking present inconsistent results. With regard to obstacle negotiation, most studies observed that both young and older adults increase prefrontal activation during obstacle negotiation relative to usual walking,18-20 with repeated reports of greater activation by the older adults.17,18,21 However, Lin and Lin 22 observed reduced prefrontal activity during obstacle negotiation relative to usual walking in young adults (older adults were not enrolled). Regarding dual-task walking, results are even more inconsistent. Although most studies reported that both young and older adults increase prefrontal activation during dual-task walking relative to usual walking, they differ on the level of activation reported in between-group comparisons.18,23,24 Fraser et al 23 observed a similar increase in cortical activation during dual-task walking in young and older adults. In contrast, Holtzer et al 24 observed greater prefrontal activation in young compared to older adults and Mirelman et al 18 observed the opposite. Furthermore, Beurskens et al 25 reported little change in prefrontal activity with a dual-task in young adults and decreased activity in older adults. Inconsistent findings might be explained, in part, by the different secondary tasks used in these studies. It should also be noted that all the cognitive tasks used in the mentioned studies involved speech, which may introduce artifacts to the fNIRS signal and compromise the results. 16 Increases related to speaking do not represent neurovascular coupling alone, hence may not represent greater cortical activation. 26 Discrepancies between study findings and methods highlight the need for further investigation. In addition, previous studies did not use a strictly cognitive task. Thus, the present study proposes the use of a nonverbal cognitive task (digit vigilance). Such task has been shown to increase prefrontal activity while standing but not during treadmill dual-task walk 27 ; so investigation of prefrontal response to this task during overground walk is required.
The existing studies are also limited by not considering the aging process in a broader spectrum. They present comparisons limited to extremes of age (young adult vs old adult). As such, it is necessary to understand the changes that occur along the aging process, considering several age groups not studied yet. The application of fNIRS technique during walking in individuals of different ages can contribute to the identification of the moment (age group) when aging-related changes affect prefrontal activity during walking. Therefore, the primary aim of this study was to investigate the effects of aging on prefrontal cortex activity during usual walking, obstacle crossing, and dual-task walking. We also examined the effects of aging on gait and the associations of prefrontal activity with measures of gait and executive function. We hypothesized that age influences prefrontal cortex activation during walking, with the older age groups showing greater activity in all walking conditions compared with younger age groups. We also hypothesized that lower activation of the prefrontal cortex is related to better gait performance and executive function.
Methods
Participants
Ninety individuals participated in the study, including 15 healthy participants in each of the following age-groups: 20-25 (G20), 30-35 (G30), 40-45 (G40), 50-55 (G50), 60-65 (G60), and 70-75 years (G70). The recruitment of participants in the first 5 years of a decade was used to have a clear separation between consecutive groups. Such approach avoided having individuals with age difference of 1 year or less in different groups. Exclusion criteria included: history of orthopedic problems that made it impossible to comply with the experimental protocol and diagnosis of dementia (Montreal Cognitive Assessment score ≤17). 28 The present study was approved by the local research ethics committee and participants provided written informed consent prior to participation.
Procedures
Initially, the following demographic information was collected: age, sex, height, and weight. Cognition were assessed through validated pen-and-paper tests/questionnaires. Global cognition was assessed with the Montreal Cognitive Assessment (scores range from 0 to 30 and greater scores signify better global cognition), which includes questions in several cognitive domains. Executive function was measured with the modified Wisconsin Card Sorting Test 29 and the Trail Making Test. 30 The modified Wisconsin Card Classification Test consists of 48 response cards and 4 stimulus cards. The participant is asked to match each consecutive response card to a stimulus card according to a particular principle (color, number, or shape of the symbols printed on the cards). The participant is informed about accuracy, but not told the scoring principle. When the participant has made 6 consecutive correct sorts, the sorting principle changes. The parameters scored were the following: completed categories (scores range from 0 to 6), number of perseverative errors (ie, when the participant persisted in the same category as that of the previously incorrect response) and failure to maintain the set (ie, when the participant made an error after 3 or more consecutive correct responses). In the Trail Making Test, the participant is required to connect, as quickly and accurately as possible, a sequence of 25 consecutive targets/dots printed on a sheet of paper, using a hand-drawn pen. The Trail Making Test consists of 2 parts: in part A, the targets to be connected are all numbers (from 1 to 25); in part B, the targets combine numbers and letters and the participant must alternate between them (1, A, 2, B, 3, C, etc). The time taken to complete each part was recorded using a manual stopwatch; the time difference between the 2 parts was used as a measure of executive function.
After, participants were prepared for fNIRS recordings. A portable fNIRS system (OctaMon fNIRS system, Artinis Medical Systems) was used to measure changes in oxygenated (HbO2) and deoxygenated (HHb) hemoglobin concentrations in the prefrontal cortex. It uses continuous wave diodes with wavelengths of 760 and 850 nm and interoptode distance of 35 mm. Data were recorded at a frequency of 10 Hz. An 8-channel arrangement with 10 optodes, consisting of 8 transmitters and 2 detectors (4 transmitters and 1 detector per hemisphere), covered Brodmann areas 9, 10, and 46 in both right and left hemispheres. After the Cz and Fpz positions were determined on the participant’s head, a neoprene head-cap (fiber holder) marked with labels of the international 10-20 electroencephalography system and predetermined locations for the optodes was placed on the participant’s head.
Before the walking assessment, a cognitive task (used for dual-task walking) was applied in 5 baseline trials with participants seated. The cognitive task consisted of a digit vigilance task, where a researcher provided the participants with a given number class (ie, odds or evens). Next, random numbers (from 1 to 9) were played over a speaker for 30 seconds, while participants counted mentally how many times the given number class occurred. Participants then called out the counted number class at the end of the 30 seconds. Participants were instructed to not close their eyes voluntarily and were not allowed to count the numbers using their fingers.
Overground walking was tested in 3 experimental conditions: usual walking, obstacle crossing, and dual-task walking. In all conditions, participants walked at their normal and comfortable pace on a cone circuit (total distance = 26.8 m) with 2 parallel 7-m long straights. A 5.74-m long electronic walkway with pressure sensors (GAITRite, CIR Systems Inc) was positioned in the center of one of the straights to record spatiotemporal gait measures. In the obstacle crossing condition, 4 foam obstacles (depth × width × height = 3 × 60 × 15 cm) were positioned every 6.7 m (an obstacle was positioned immediately at the end of the GAITRite registration area). In the dual-task condition, participants walked while performing the digit vigilance task. At the end of each trial the participants should express how many odd or even numbers they heard in the audio. Fifteen randomized walk trials were performed, with 5 trials for each experimental condition. Each trial started with 30 seconds of standing still, followed by a “ready-go” instruction and 30 seconds of walking. The performance (ie, error score) in the digit vigilance task was quantified by the percentage of the absolute error (difference between the correct answer and the response given by the participant) in each trial. The error score [(absolute error/correct response) × 100] was calculated for baseline and dual-task walking.
Functional Near-Infrared Spectroscopy Analysis
The fNIRS system measured optical density of the raw signal and converted this to HbO2 and HHb using the modified Beer-Lambert law in the Oxysoft software (Artinis, Netherlands). The differential path factor (DPF) was calculated according to the age of each participant. Artifact corrections and filtering were performed according to recent recommendations for the processing of fNIRS signal. 16
fNIRS data were preprocessed using the time series analysis routine available in the NIRS-SPM software (NIRS-SPM, http://www.nitrc.org/projects/nirs_spm), 31 which included the following steps: (a) filtering: high-frequency noise was reduced/removed by a low-pass filter based on canonical hemodynamic response function 32 and (b) detrending: a wavelet algorithm (wavelet minimum description length detrending algorithm) was used to decompose the signal into global trends, hemodynamic response, and noise components. 33 Then, the preprocessed signal was exported to Matlab (MATLAB and Statistics Toolbox Release R2015a, The MathWorks, Inc., Natick, Massachusetts, USA) for additional processing steps using a custom algorithm. Channels were averaged per region of interest (ie, right and left prefrontal cortex) and normalized by dividing them by the corresponding maximum signal amplitude of the whole experiment. This procedure was used to reduce the differences in amplitude between individuals. 34 The task was divided into 2 periods: rest (10 seconds of standing still before starting to walk, with the exception of the 5 seconds immediately before the walk—which were excluded from the analysis to avoid anticipatory responses) and task (period between 5 and 25 seconds after start walking). The initial 5 seconds of walking were excluded due to the physiological delay in the hemodynamic response and the final 5 seconds of walking were excluded to avoid anticipatory responses to the stop command). The normalized concentrations were averaged over the rest and task periods for each region of interest and each trial. Finally, differences between rest and task periods were calculated to evaluate the relative change in HbO2 and HHb. Although we report both HbO2 and HHb concentrations, it is relevant to highlight that previous research suggest that HbO2 is more sensitive to locomotion-related activities than HHb. 35
Gait Analysis
The data of the electronic carpet were analyzed by GAITRite 4.7.5 software. The 4 steps preceding the obstacle position were considered for the calculation of spatiotemporal gait parameters. Means and variability, calculated by the coefficient of variation [(standard deviation/mean) × 100], of step velocity (ie, step length/step time), length, time, and width were calculated.
Statistical Analysis
Shapiro-Wilk tests were employed to verify data distribution. One-way analyses of variance (ANOVAs) and Kruskal-Wallis tests were performed to compare demographic and cognitive data between groups. Two-way repeated-measures ANOVAs, with group and condition as factors, were used to analyze spatiotemporal gait parameters and error scores on the digit vigilance task. Two-way repeated-measures analyses of covariance (ANCOVAs), with group and condition as factors and controlling for step velocity, were performed to analyze relative HbO2 and HHb concentrations for each hemisphere (left and right). Step velocity was used as a covariate to minimize the chance of false-positive results driven by speed-related differences in superficial blood flow. Bonferroni post hoc tests (with significance level correction: 0.05/number of comparisons) were used to locate differences where applicable. Pearson’s correlation tests were applied to explore associations between prefrontal cortical activity and gait or executive function. To avoid multiple correlations for all measures of executive function, we transformed them into a unique z score (ie, we calculated z scores for each of the 4 measures of executive function—with greater values corresponding to better executive function—and then calculated the mean z score). The level of significance was set at .05.
Results
Demographic, cognitive, and neuropsychiatric data of the participants are presented in Table 1. Two outliers who presented more than 3 standard deviations in multiple dependent variables were excluded (1 participant in each of the G20 and G70 groups), totaling 88 participants analyzed in the study. One-way ANOVAs and Kruskal-Wallis tests showed no significant differences between groups for sex, height, body weight, Montreal Cognitive Assessment (global cognition), and Wisconsin Card Sorting Test (set failure). Kruskal-Wallis tests indicated significant differences between groups for number of completed categories and perseverative errors in the Wisconsin Card Sorting Test. Post hoc tests revealed that G60 had fewer completed categories and more perseverative errors than G20, G30, G40, and G50. In addition, G70 had fewer completed categories than G20 and G30. The Kruskal-Wallis test also showed differences between groups for Trail Making Test, with G70 taking more time to complete the test than G20, G30, G40, and G50.
Means, Standard Deviations, and Statistic Results of Participants’ Demographic and Cognitive Data (n = 88).
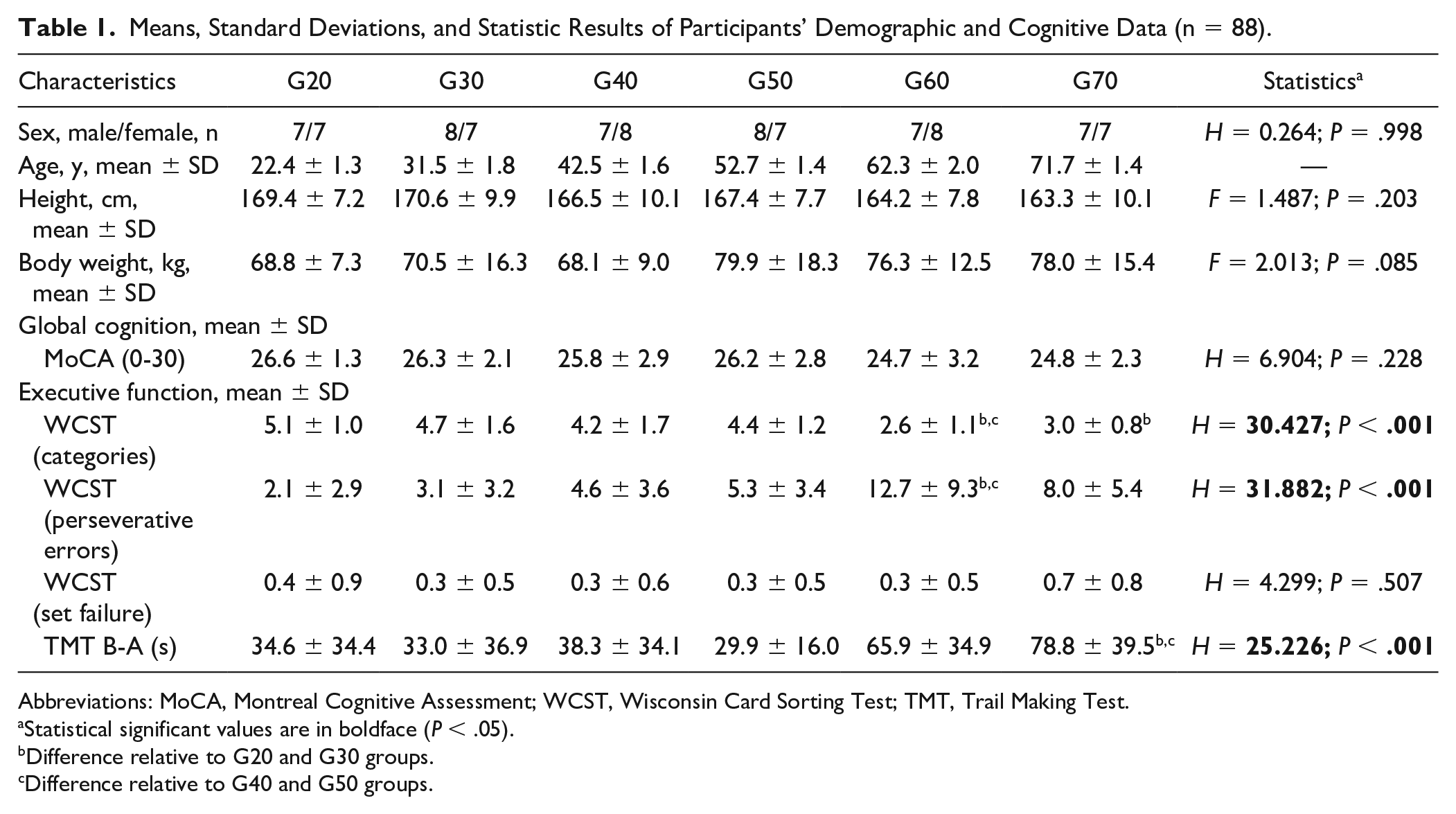
Abbreviations: MoCA, Montreal Cognitive Assessment; WCST, Wisconsin Card Sorting Test; TMT, Trail Making Test.
Statistical significant values are in boldface (P < .05).
Difference relative to G20 and G30 groups.
Difference relative to G40 and G50 groups.
Prefrontal cortex activity
Significant 2-way interactions (group × condition) were observed for relative HbO2 levels in the left (F10, 158 = 2.041; P = .032) and right prefrontal cortex (F10, 158 = 2.729; P = .004). Post hoc tests revealed between-group differences for all walking conditions (Figure 1). In the usual walking condition, G60 showed higher HbO2 level than G30 (left hemisphere: P = .002). In the obstacle crossing condition, G60 showed higher HbO2 level than G20 (left: P = .003; right: P = .001). In the dual-task walking condition, higher HbO2 levels were observed for G50 (left: P = .001; right: P < .001), G60 (left: P < .001; right: P < .001), and G70 (left: P < .001; right: P < .001) in comparison with G20; additionally, G60 showed higher HbO2 level compared with G40 (left: P = .003; right: P = .003); finally, G30 presented higher HbO2 level in relation to G20 (right: P = .003).
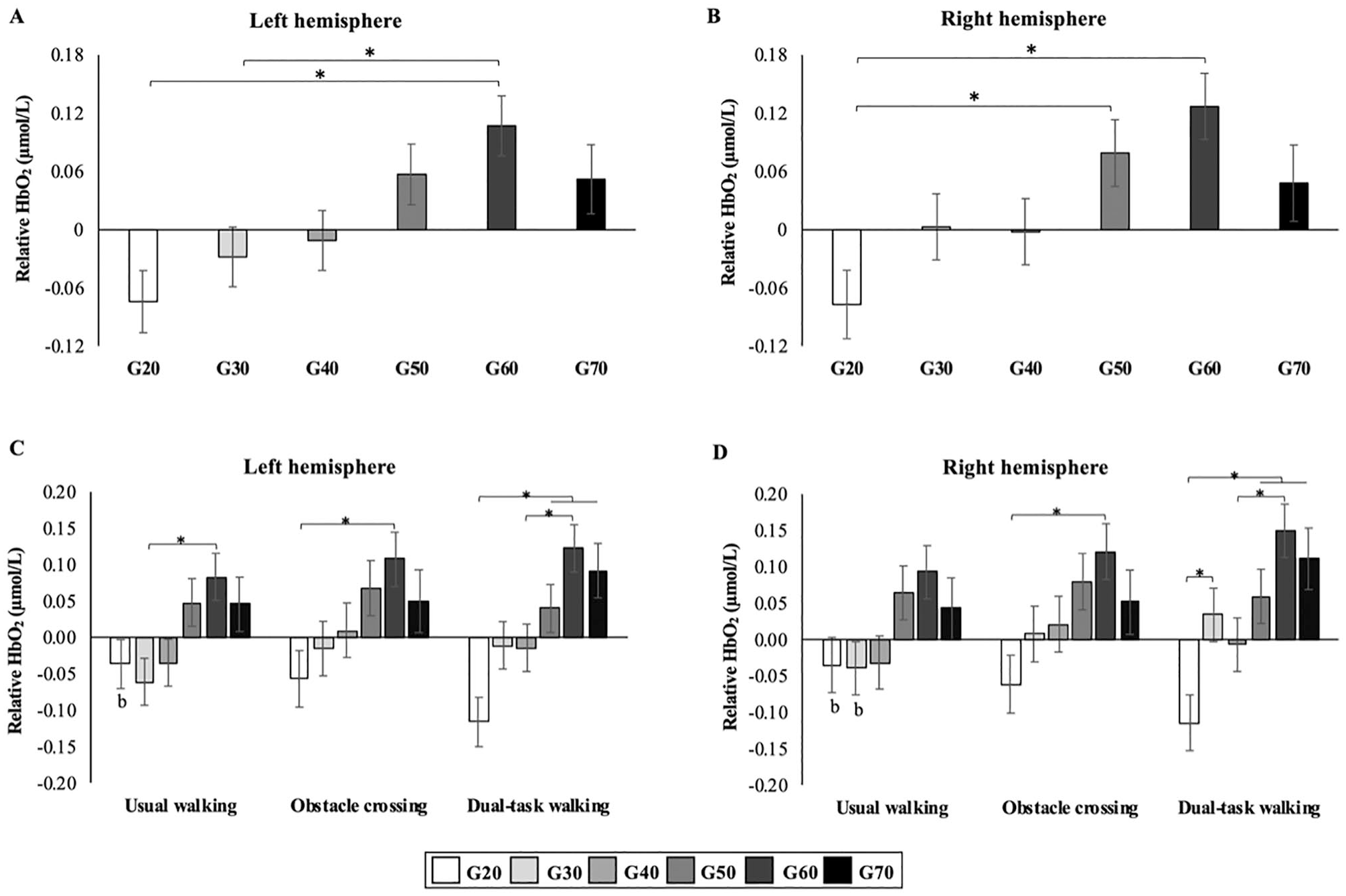
Relative HbO2 levels (mean and standard error of the mean) for left and right prefrontal cortex. Group main effects are represented in panels A and B. Group*condition interactions are represented in panels C and D. The reported values represent the difference between the experimental task and rest/baseline (quiet standing).
Regarding intragroup differences (across conditions), no significant results were observed for G40, G50, G60 and G70, although HbO2 levels showed overall slight increases in the obstacle crossing and/or dual-task walking conditions relative to usual walking. G20 decreased HbO2 levels in the dual-task walking condition in comparison to usual walking (left: P = .002; right: P = .006). G30 increased HbO2 level in the dual-task walking condition in comparison with usual walking (right: P = .01).
Group main effect was also revealed for HbO2 levels (left: F5, 79 = 4.437, P = .001; right: F5, 79 = 4.185, P = .002). G60 had higher HbO2 levels compared with G20 (left: P = .002; right: P = .001) and G30 (left: P = .041). Also, G50 presented higher HbO2 levels compared with G20 (right: P = .036). ANCOVAs did not reveal condition main effect for HbO2 levels (left: F2, 158 = 1.220, P = .298; right: F2, 158 = 1.611, P = .203).
Regarding HHb levels, ANCOVAs did not reveal significant results for group (left: F5, 79 = 0.327, P = .896; right: F5, 79 = 0.399, P = .848), condition (left: F2, 158 = 0.456, P = .635; right: F2, 158 = 0.291, P = .748) or group × condition (left: F10, 158 = 1.352, P = .208; right: F10, 158 = 1.399, P = .185). HHb levels for each age group in each walking condition are summarized in Supplemental Table S1.
Cognitive Task Performance
Group main effect was observed for the error score in the cognitive task (F5, 80 = 3.537; P = .006; Figure 2). Post hoc tests indicated that G70 group showed greater error compared to G30 (P = .023) and G50 (P = .008). ANOVA did not indicate main effect of condition (F1, 80 = 2.448; P = .122) or interaction between factors (F5, 80 = 2.067; P = .078).
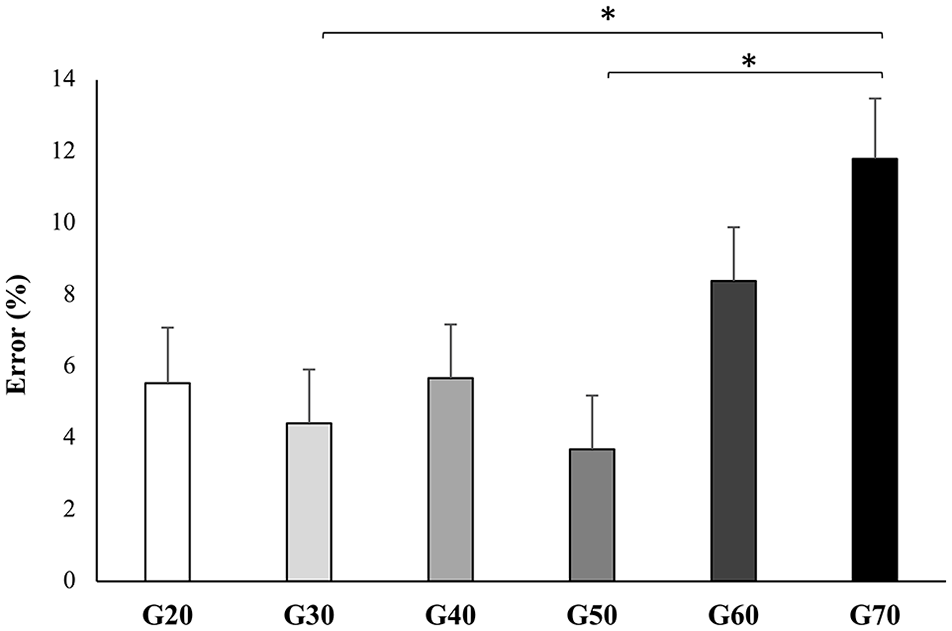
Error score (mean and standard error of the mean) in the cognitive task for each age group.
Gait Performance
Significant interactions between group and condition were observed for step width (F10, 160 = 2.067; P = .030) and step length variability (F10, 160 = 2.124; P = .025) (Figure 3). Post hoc tests revealed between-group differences only for step length variability: G70 presented greater variability than G20 and G30 in the obstacle crossing (G20: P = .001; G30: P = .003) and dual-task walking conditions (G20: P = .003). Regarding intragroup differences for step length variability, all groups presented greater variability in the obstacle crossing condition compared with usual walking (G20, G30, G40, G50, G60, G70: P < .001) and dual-task walking (G20, G30, G40, G50, G60, G70: P < .001). With regard to intragroup differences for step width, G50 and G60 showed greater step width in the usual walking (G50: P = .006; G60: P = .001) compared with the obstacle crossing condition. In addition, G40, G50, and G60 showed greater step width in dual-task walking (G40: P < .001; G50: P = .002; G60: P = .003) compared with the obstacle crossing condition. Also, G70 presented greater step width in the dual-task walking condition compared with usual walking (P < .001) and obstacle crossing (P < .001) conditions.
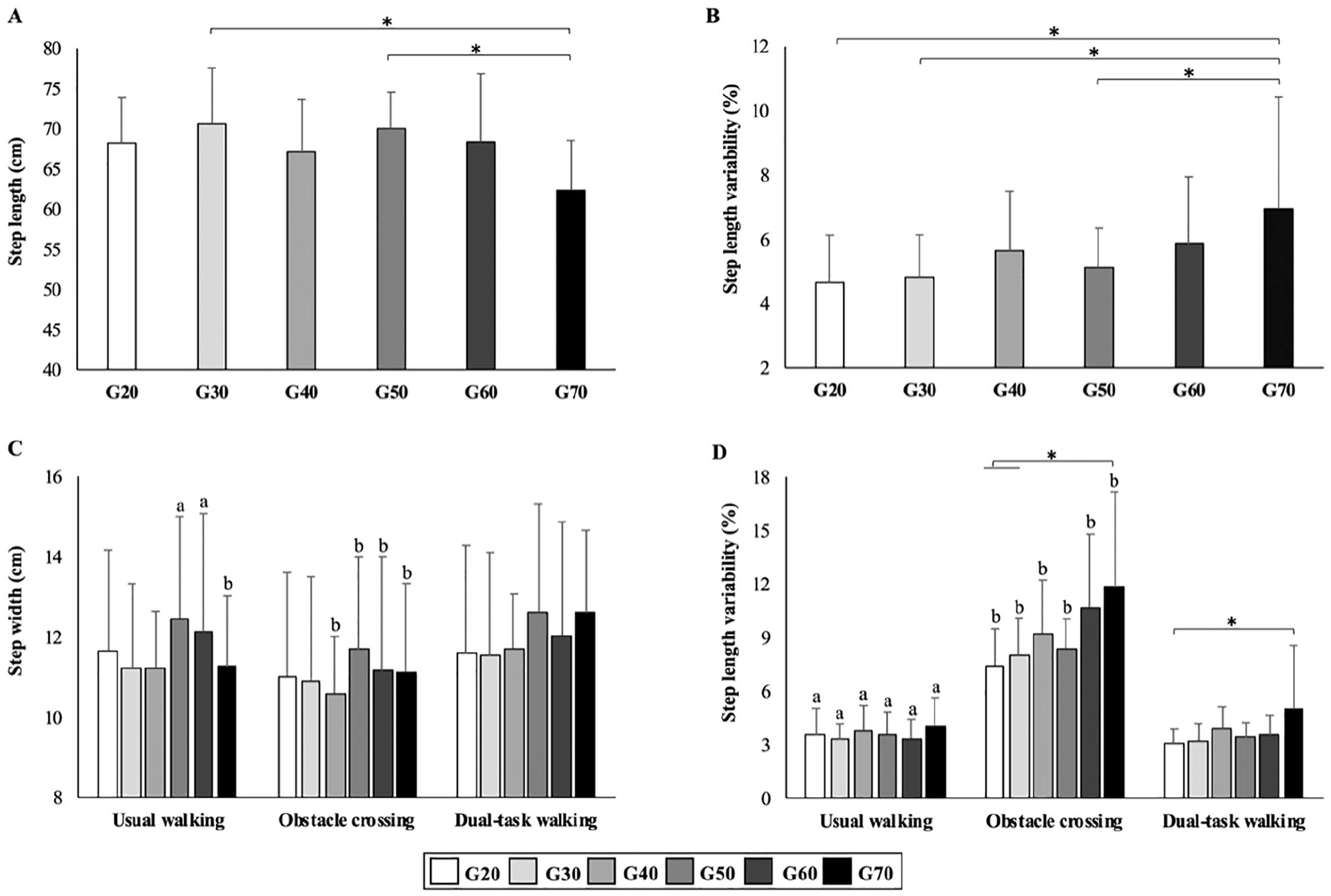
Gait variables (mean and standard deviation) with significant group main effects (panels A and B) and/or group*condition interaction (panels C and D).
Group main effect was revealed for step length (F5, 80 = 2.869; P = .020) and step length variability (F5, 80 = 4.388; P = .001) (Figure 3). Post hoc tests indicated that G70 presented shorter step length compared with the G30 (P = .015) and G50 (P = .032). Also, G70 presented greater step length variability than G20 (P = .002), G30 (P = .005), and G50 (P = .025).
Condition main effect was revealed for step velocity (F2, 160 = 25.940; P < .001), step length (F2, 160 = 12.134; P < .001), step duration (F2, 160 = 19.991; P < .001), step width (F2, 160 = 35.686; P < .001), step velocity variability (F2, 160 = 11.631; P < .001), step length variability (F2, 160 = 217.998; P < .001), step duration variability (F2, 160 = 14.038); P < .001), and step width variability (F2, 160 = 24.024; P < .001). Post hoc test results are summarized in the Supplemental Table S2. Averages and standard deviations of gait variables in all walking conditions are summarized in Supplemental Table S3.
Association Between Prefrontal Cortex Activity (Relative HbO2 Level) and Executive Function or Gait Variables
There were significant negative associations between executive function and relative HbO2 levels for all walking conditions (Figure 4). Also, HbO2 levels were significantly associated with multiple gait parameters (Figure 4), mainly in the dual-task walking condition (ie, step velocity, step duration, step width, and step width variability). For the usual walking condition, only step duration variability was significantly correlated with HbO2 level (Figure 4). For the obstacle crossing condition, only step width was significantly correlated with HbO2 level (Figure 4). Overall, better gait performance was associated with lower HbO2 level. However, all the significant associations were in the “weak” range (r = 0.2-0.4).
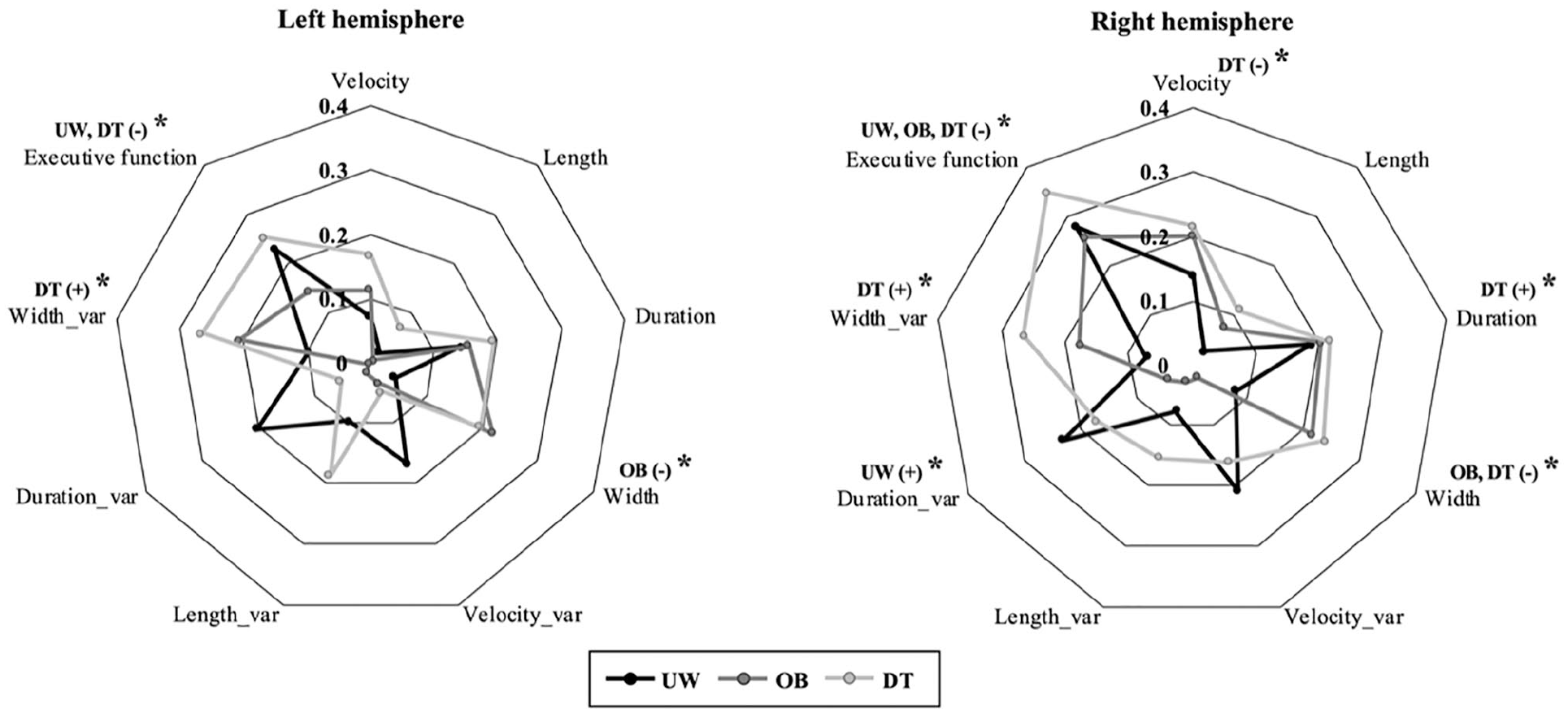
Associations between relative HbO2 levels and measures of gait and executive function.
Discussion
This study investigated the effects of aging on prefrontal cortex activity during different walking tasks (ie, usual walking, obstacle crossing, and dual-task walking) and explored the association of prefrontal activity with gait parameters and executive function. The results suggest that the aging process leads to a gradual increase in prefrontal activity during walking (Figure 1), which confirmed our first hypothesis. Overall, young adults exhibited the lowest level of prefrontal activity. Notably, the age in which increased prefrontal activity reached significance was dependent on the walking task performed, with the dual-task condition leading to increased prefrontal activity at younger age. The use of the executive locomotor pathway as a compensatory mechanism for the control of locomotion seems to become inefficient in the 70s. In addition, we observed significant associations of prefrontal activity with gait and executive function, but correlation coefficients were weak.
Effects of Aging on Prefrontal Activity, Gait, and Executive Function: An Integrated View
The increased prefrontal activity during walking caused by aging is influenced by the locomotor task performed. In the usual walking and obstacle crossing conditions, increased activation of the prefrontal cortex was observed only in G60. In the dual-task walking condition, increased prefrontal activation was observed in G30, G50, G60, and G70. These findings suggest that greater involvement of the executive locomotor pathway11-13 occurs earlier in life when tasks with increased executive load are performed. Specifically, the proposed dual-task likely imposed greater executive/attentional demand than the obstacle condition.
Use of the executive locomotor pathway as a compensatory mechanism for the control of locomotion becomes inefficient in the seventh decade of life. Although multiple age groups (ie, G30, G50, G60, and G70) presented increased prefrontal activity in at least one of the tested walking conditions, only G70 presented impairments in gait. Compared with other groups, G70 had reduced step length across all conditions and increased step length variability in the obstacle crossing and dual-task conditions. It is noteworthy that these behavioral findings are in line with previous studies showing more pronounced age-related gait impairments in tasks with increased executive load.7-9 Current findings suggest that individuals younger than 70s were able to maintain adequate gait performance even if they needed to increase prefrontal activity. On the other hand, those in the 70s were unable to use the executive locomotor pathway efficiently and gait performance dropped.
Gait impairments observed in G70 may be associated with a “ceiling” of prefrontal executive resources. This interpretation is supported by the fact that both the Trail Making Test and the Wisconsin Card Sorting Test revealed reduced executive function in G70. Additionally, only G70 had increased error score in the digit vigilance task. Our findings are consistent with the Compensation-Related Utilization of Neural Circuits Hypothesis (CRUNCH), which has emerged from the literature on cognitive aging. It postulates that older adults have increased brain activity in comparison to young adults at submaximal levels of task demand, which is beneficial to preserving taskperformance.36,37 However, this brings older adults closer to the ceiling of brain activation resources. As task demand increases, a resource ceiling can be reached, leading to insufficient processing and decreased task performance. 38 We propose that older adults in G70 already (or nearly) reached the resource ceiling during usual walking—as they did not show increased prefrontal activity relative to younger groups and had reduced step length. Because they did not have more executive resources available, the increase in executive load (caused by planning the obstacle crossing and performing a secondary concomitant task) led to additional gait impairment (ie, increased step length variability). One may ask why this interpretation does not apply to individuals in the 60s if they also had reduced executive function as measured by the pen-and-paper tests. First, they performed similar to all younger groups in the digit vigilance task. Second, they had increased prefrontal activity in all walking conditions and no gait impairment. Therefore, G60 was able to use prefrontal executive resources available to maintain gait performance at a level comparable to younger groups in all the walking conditions tested. Accordingly, increased prefrontal cortical activity has been proposed as a preclinical sign of (future) gait impairments and falls in high-functioning older adults. 39
Prefrontal cortex activity is associated with gait and executive function. As expected, we observed significant correlations between HbO2 levels and gait measures (for all walking conditions) or executive function in our sample. Overall, our findings suggest that those with better gait and executive function had lower HbO2 levels during walking, which is in accordance with previous studies. 18 The observed weak correlation coefficients suggest that not only prefrontal cortical activity explains differences/changes in gait and executive function across the different age groups.
Figure 5 illustrates an integrated interpretation of the current results regarding the effects of aging on prefrontal cortex activity during walking, executive function, and walk performance. The aging process leads to increased involvement of the executive locomotor pathway (ie, increased activation of the prefrontal cortex during walking15,16,18), which is a compensatory mechanism for the decline in gait automaticity that occurs with aging.13,40 Appropriate levels of executive function are required for the efficiency of this compensatory mechanism. However, executive function starts to decline in the sixth decade of life (as measured by pen-and-paper tests) and reaches limiting levels in the 70s. Notably, the use of the executive locomotor pathway as a compensatory mechanism becomes inefficient in the 70s and then gait impairments are observed. When executive load of the task is increased, gait impairments become more pronounced as the system may have already reached the ceiling of executive resources available.
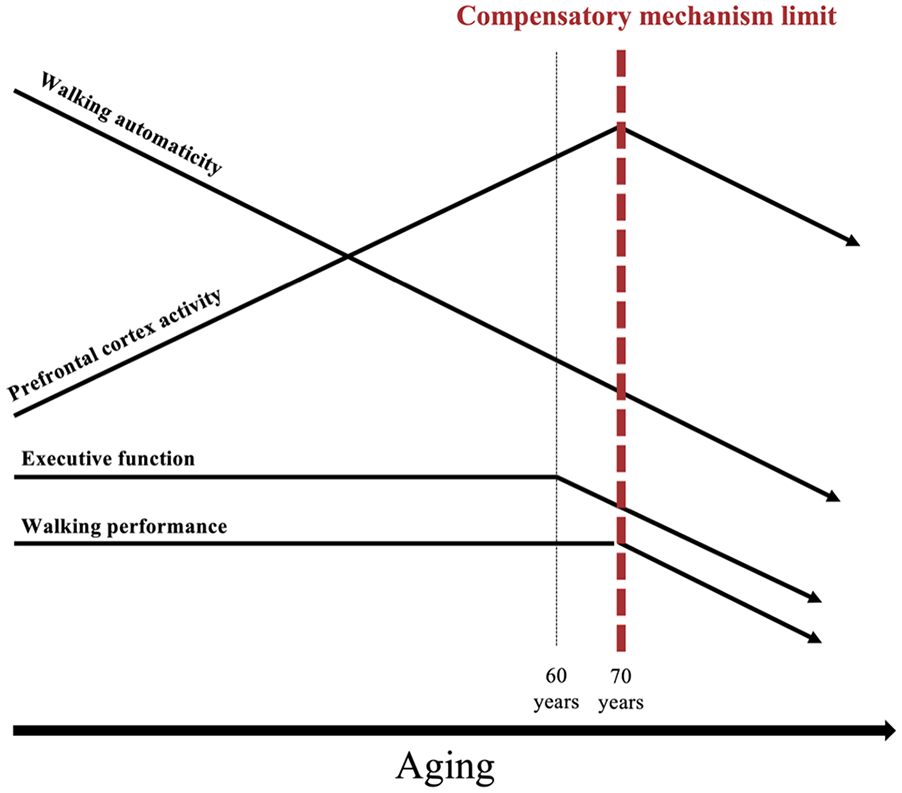
Illustration of an integrated interpretation of the current results regarding the effects of aging on prefrontal cortex activity during walking, executive function and gait performance. Please refer to the text for detailed explanation.
Study Limitations
Limitations apply while interpreting current findings. Although this study brings new insights to the literature related to the effects of aging on prefrontal activity during walking, it has inherent limitations of a cross-sectional design. As such, longitudinal studies are needed. It should be noted that potential confounders related to lifestyle (ie, drinking and smoking habits, physical activity level, cognitive/executive training, etc) were not controlled. Since our fNIRS system does not have short-separation channels, we cannot rule out possible contamination of the signal by superficial blood flow.
Conclusion
The aging process causes a gradual increase in the involvement of the executive locomotor pathway during walking. Prefrontal activity is influenced by the locomotor task performed, with increased activity being observed at younger ages for dual-task walking. Our findings also highlight a possible association of prefrontal activity with gait parameters and executive function. The system may reach the resource ceiling in the 70s, when reduced executive function limits the efficiency of the executive locomotor pathway and gait impairments are observed.
Supplemental Material
Supplemental_Material – Supplemental material for Prefrontal Cortex Activity During Walking: Effects of Aging and Associations With Gait and Executive Function
Supplemental material, Supplemental_Material for Prefrontal Cortex Activity During Walking: Effects of Aging and Associations With Gait and Executive Function by Priscila Nóbrega-Sousa, Lilian Teresa Bucken Gobbi, Diego Orcioli-Silva, Núbia Ribeiro da Conceição, Victor Spiandor Beretta and Rodrigo Vitório in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the National Council for Scientific and Technological Development (CNPq) (grant number: 166467/2017-0), the São Paulo Research Foundation (FAPESP) (grant number: 2014/22308-0; 2016/21499-1), and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
ORCID iDs
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.