
Abstract
Background. Patients with freezing of gait (FOG) have more difficulty with switching tasks as well as controlling the spatiotemporal parameters of gait than patients without FOG. Objective. To compare the ability of patients with and without FOG to adjust their gait to sudden speed switching and to prolonged walking in asymmetrical conditions. Methods. Gait characteristics of 10 freezers, 12 non-freezers, and 12 controls were collected during tied-belt conditions (3 and 4 km/h), motor switching and reswitching (increase of speed in one belt from 3 to 4 km/h and vice versa), and adaptation (adjustment to asymmetrical gait) and re-adaptation (returning to symmetrical gait) on a split-belt treadmill. Results. Following switching, freezers showed the largest increase of step length asymmetry (P = .001). All groups gradually adapted their gait to asymmetrical conditions, but freezers were slower and demonstrated larger final asymmetry than the other 2 groups (P = .001). After reswitching, freezers again showed the largest step length asymmetry (P = .01). During re-adaptation, both controls and non-freezers reached symmetrical levels, but freezers did not. Interestingly, only immediately after switching did one episode of FOG and one episode of festination occur in 2 different patients. Conclusions. Freezers have more difficulties adapting their gait during both suddenly triggered and continued gait speed asymmetry. The impaired ability of freezers during both switching and reswitching would suggest that they have an adaptive deficit rather than difficulties with asymmetry per se. Future work needs to address whether these adaptation problems can be ameliorated with rehabilitation.
Introduction
A considerable number of patients with Parkinson’s disease (PD) suffer from freezing of gait (FOG), which is a disabling clinical phenomenon characterized by a brief inability to generate effective stepping despite the voluntary wish to move. 1 Recent neuroimaging work suggests that highly integrated motor and cognitive functions of the basal ganglia and related frontal areas are differentially affected in patients with FOG compared to those without.2,3 In addition, altered neural activity of the mesencephalic locomotor region4,5 and white matter integrity changes in neurons connecting the mesencephalic locomotor region and frontal cortical regions were found to be related to FOG.6,7
Behaviorally, freezers have more pronounced gait deficits even during normal gait or more challenging situations such as turning 8 and walking through a doorway. 9 However, it is not clear to what extent these parameters are directly related to FOG. FOG has been shown to occur more frequently in situations that incur a progressive reduction in step length 10 and an increase of gait asymmetry. 11 These findings support the hypothesis that FOG can be induced by several motor deficits that accumulate up to a freezing threshold. 12
Asymmetry has also been suggested to be one of the potential triggers that could drive the motor system toward FOG, 11 as FOG frequently happens during motor tasks that require locomotor asymmetry, such as turning, 8 initiating gait, 13 and avoiding an obstacle. 14 Fasano et al 15 reported direct evidence supporting the role of asymmetry in FOG.They found that decreasing between-limb asymmetry through a 50% reduction of subthalamic nucleus stimulation voltage for the least affected limb led to reduced FOG duration and frequency. In addition, increasing asymmetry increased FOG duration. However, it was not clear in how many patients FOG was provoked in this fashion. Therefore, the direct contribution of imposing asymmetrical gait demands needs further clarification.
A split-belt treadmill, in which 2 belts can move at the same or different speeds, offers a controlled means to simulate asymmetrical tasks such as turning. It also allows the time-varying speed manipulations to resemble the gait demands encountered in daily life. Finally, it enables studying the ability of participants to respond to switching, asymmetry, and gait adaptation. 16 During the immediate switch to asymmetrical conditions, relative shortening of step length of the limb on the faster belt occurs in healthy controls. 17 Freezers were observed in the clinical setting to have difficulty altering their locomotor system according to sudden changes in the environment (ie, set-shifting). 18 This was confirmed in a treadmill study in which sudden obstacles elicited short FOG episodes. 14 Furthermore, cognitive set-shifting deficits were specifically associated with FOG severity 18 but not to PD severity. 19 Motor switching while adapting to gait speed changes in a recent study on the split-belt surprisingly did not show overt gait difficulties in freezers compared to non-freezers. 20 These negative results may be due to averaging and pooling of the epochs in which switching occurred and low belt speeds. Therefore, the first aim of the current study was to test whether freezers adjust their gait differently following sudden switching from steady walking to an asymmetrical gait. We hypothesized that switching would lead to impaired scaling of step length and larger asymmetry in freezers than in non-freezers.
The second aim of the current study was to investigate gait adaptation in response to prolonged asymmetrical load on the gait pattern. Previous studies showed that this gradual gait adaptation on split-belt might be dependent on the cerebellum. 17 This concurs with recent suggestions that the cerebellum may exert an important compensatory role during motor adaptation in PD.21,22 In addition, reduced structural connectivity between the cerebellum and other cortical centers has been reported in freezers. 7 Therefore, we hypothesized that asymmetrical walking would lead to greater gait asymmetry in freezers than in non-freezers. In line with this, we also expected that re-adaptation is differentially affected in freezers. Finally, through analyzing the relationship between clinical measures and adaptive ability, we aimed to gain insight into the gait adaptation difficulties in PD.
Materials and Methods
Subjects
The study was approved by the local medical ethics committee of KU Leuven, and all participants gave their written informed consent before the experiment. Twenty-two patients with idiopathic PD, including 10 freezers and 12 non-freezers and 12 age-matched controls were studied, who met the following inclusion criteria: patients had to be diagnosed based on the UK Parkinson’s Disease Brain Bank Criteria 23 by a neurologist. The exclusion criteria for the patients were other neuromuscular disorders, the inability to walk independently on the treadmill for 12 consecutive minutes while OFF medication and a score below 24 on the Mini-Mental State Examination (MMSE) for both patients and controls. Freezers were defined by a score equal to 1 on item 1 of the New Freezing of Gait Questionnaire (N-FOGQ). 24 Freezing episodes were confirmed during previous gait tests in OFF in the laboratory in all cases. The severity of clinical symptoms of PD patients was assessed according to the Hoehn & Yahr rating scale (H&Y) 25 and Unified Parkinson Disease Rating Scale (UPDRS) III. 26 In order to characterize the executive function of participants, we administered the Montreal Cognitive Assessment (MoCA) 27 and the auditory Stroop task to specifically probe set-shifting abilities. The latter task consisted of a high or low pitched voice saying the words “high” or “low” in Dutch. Subjects were required to indicate the pitch of the voice and to ignore the word said. Hence, the auditory Stroop required switching from congruent (identical pitch and word) to incongruent (different pitch and word do not match) stimuli.16,28 Verbal responses to the Stroop task were recorded by a microphone attached to a headphone worn while sitting. All clinical motor and cognitive testing was carried out in the morning OFF medication, after at least 12-hour withdrawal from anti-Parkinsonian medications. The side with the highest UPDRS III score was determined as the disease-dominant side. For controls, we used the non-dominant limb as a comparison, determined by response to the question, “Which leg would you use to kick a soccer ball?”
Procedure
The paradigm consisted of walking on a split-belt treadmill (Motek Forcelink, Culemborg, The Netherlands). The belts were moving either at the same (tied-belt) or different speeds (split-belt). Before measurement, retroreflective markers were placed bilaterally on the lateral malleoli. A 10-camera Vicon 3D motion analysis system (Vicon Nexus, Oxford Metrics, Oxford, UK) captured the position of the markers at a rate of 100
Samples/second. Three-dimensional ground reaction forces were sampled at 1000 samples/second through sensors embedded in the treadmill. For safety reasons, all participants wore a harness around the upper chest, which was mounted to the ceiling to prevent falls. The harness did not support bodyweight nor interfered with walking.
Before data collection, subjects were asked to walk on the treadmill for 2 minutes (at 3 km/h) to allow familiarization. They were not given any practice on the split-belt configuration. Subjects were instructed to look straight ahead and lift their hands off the rail.
Figure 1A shows step lengths of a control subject during 6 testing conditions (each lasting 2 minutes): (1) slow tied-belt condition (3 km/h); (2) split-belt walking following an abrupt increase in speed of one side in a random manner to 4 km/h (speed switching), while the other belt still moved at 3 km/h to induce asymmetry and the adaptation to this speed (adaptation phase); (3) tied belts at 3 km/h (reswitching) for 2 minutes (re-adaptation phase); (4, 5) the same adaptation and re-adaptation sequences for the other leg; (6) fast tied-belt condition (4 km/h). The 3 to 4 km/h speed contrast proved sufficiently challenging to destabilize gait as was determined during a pilot study. One freezer and one non-freezer were unable to sustain walking at the 4 km/h speed. For these subjects (and their matched healthy control), treadmill speeds were reduced to 2 and 3 km/h.
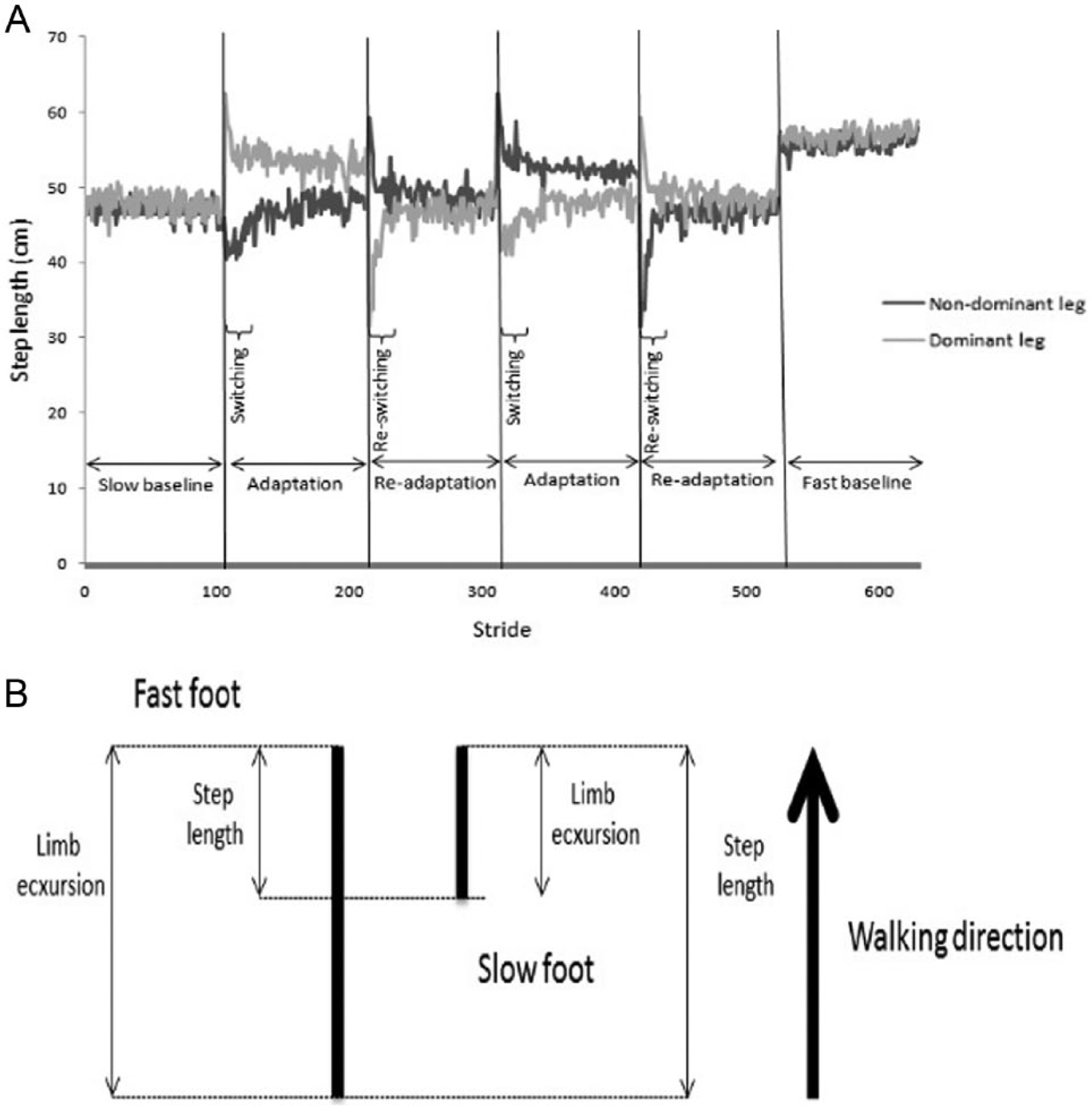
(A) Time course for the experimental paradigm showing the different tied- and split-belt conditions in a representative control subject. The y-axis represents step lengths of the 2 legs (non-dominant leg in black and dominant leg in gray) during different conditions, and the x-axis shows the number of strides over time. The paradigm consisted of testing periods of 2 minutes, including slow tied-belt, speed switching, adaptation, speed reswitching, re-adaptation, and fast tied-belt conditions for the 2 legs. During the first speed switching, the belt speed of the non-dominant leg (in black) increased from 3 km/h to 4 km/h and then returned to 3 km/h after reswitching. During the second speed switching, the belt speed of the dominant leg (in gray) increased from 3 km/h to 4 km/h and then returned to 3 km/h after reswitching. (B) Illustration of the method to calculate step length and limb excursion during switching. Step length is calculated as the anterior–posterior distance between the ankle markers at foot strike of each leg. Limb excursion is calculated as the anterior–posterior distance traveled by the ankle marker from foot contact to foot off within the same leg.
Outcome Variables
Gait events (foot strike and foot off) were detected from the center of pressure trajectories. 29 Limb excursion (the split-belt treadmill-based estimate of stride length 30 ) was calculated as the anterior-posterior distance traveled by the ankle marker from foot contact to foot off within the same leg, in the lab reference frame. Step length was determined as the anterior-posterior distance (in the lab reference frame) between the ankle markers at foot strike of each leg (Figure 1B). Step length asymmetry, suggested to be the most sensitive measure of adaptation to split-belt walking,31,32 was calculated as
Values of zero mean symmetrical walking.31,32 For split-belt walking conditions, step length asymmetry, corrected for tied-belt asymmetry, was calculated as
Step time asymmetry was calculated in the same manner. For tied-belt walking conditions, we calculated the mean of all of these variables over the entire condition, as well as the coefficient of variation (CV) (standard deviation/mean × 100) of limb excursion. The mean values of the 2 legs were used for analysis. To study the switching behavior, we calculated the difference between the mean of the last 5 strides of tied-belt walking (3 km/h) and the mean of the first 5 strides of switching/reswitching condition. In addition, to analyze the time series of adaptation and re-adaptation conditions, epochs of 10 strides were compared between groups and conditions. For Stroop performance, the error rate (number of incorrect responses/number of inputs × 100) was calculated based on manual analysis of the audiotapes by an independent tester for congruent and incongruent responses separately. All other calculations were done using custom-made Matlab programs (Mathworks, Natick, MA).
Statistical Analysis
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS), version 19.0. Sets of one-way analyses of variance (ANOVAs) were used to analyze differences in age and cognitive function between the 3 groups. Independent t-tests were used to compare disease severity and duration and falls between PD subgroups.
Differences between groups in tied-belt walking conditions were assessed using 3 × 2 (Group × Speed) repeated-measures ANOVAs. To test the switching behavior, 2 separate (for the 2 legs) 3 × 3 (Group × Condition, ie, tied-belt, switching, and reswitching) repeated-measures ANOVAs were performed for each outcome. To assess differences in adaptation and re-adaptation between groups, time series of step length and time asymmetry were divided into epochs of 10 strides (10 epochs per condition) for each subject. Two separate (for adaptation and re-adaptation) Group × Epoch repeated-measures ANOVAs were used. Tukey’s post hoc testing was used for multiple comparisons when appropriate. As an exploratory analysis, paired t-tests with Bonferroni corrections were performed to compare the values between the most and least impaired legs of patients during split-belt walking. We also compared the differences in step length asymmetry at the end of adaptation and re-adaptation with slow tied-belt speed between PD groups using independent t tests. Spearman correlations were used to assess the relationship between gait measures and clinical parameters. The α level was set at .05 to determine statistical significance, except when using Bonferroni corrections.
Results
There were no statistically significant differences between the groups in terms of age and overall cognitive function (MMSE and MoCA; see Table 1). In addition, freezers and non-freezers were matched for disease severity (UPDRS III OFF) and disease duration. There were no significant differences between the groups in Stroop performance. Freezers had significantly more falls during the last 6 months, compared to non-freezers (P = .02).
Demographic and Clinical Characteristics of 10 Freezers, 12 Non-freezers, and 12 Controls (Mean and Standard Deviation).
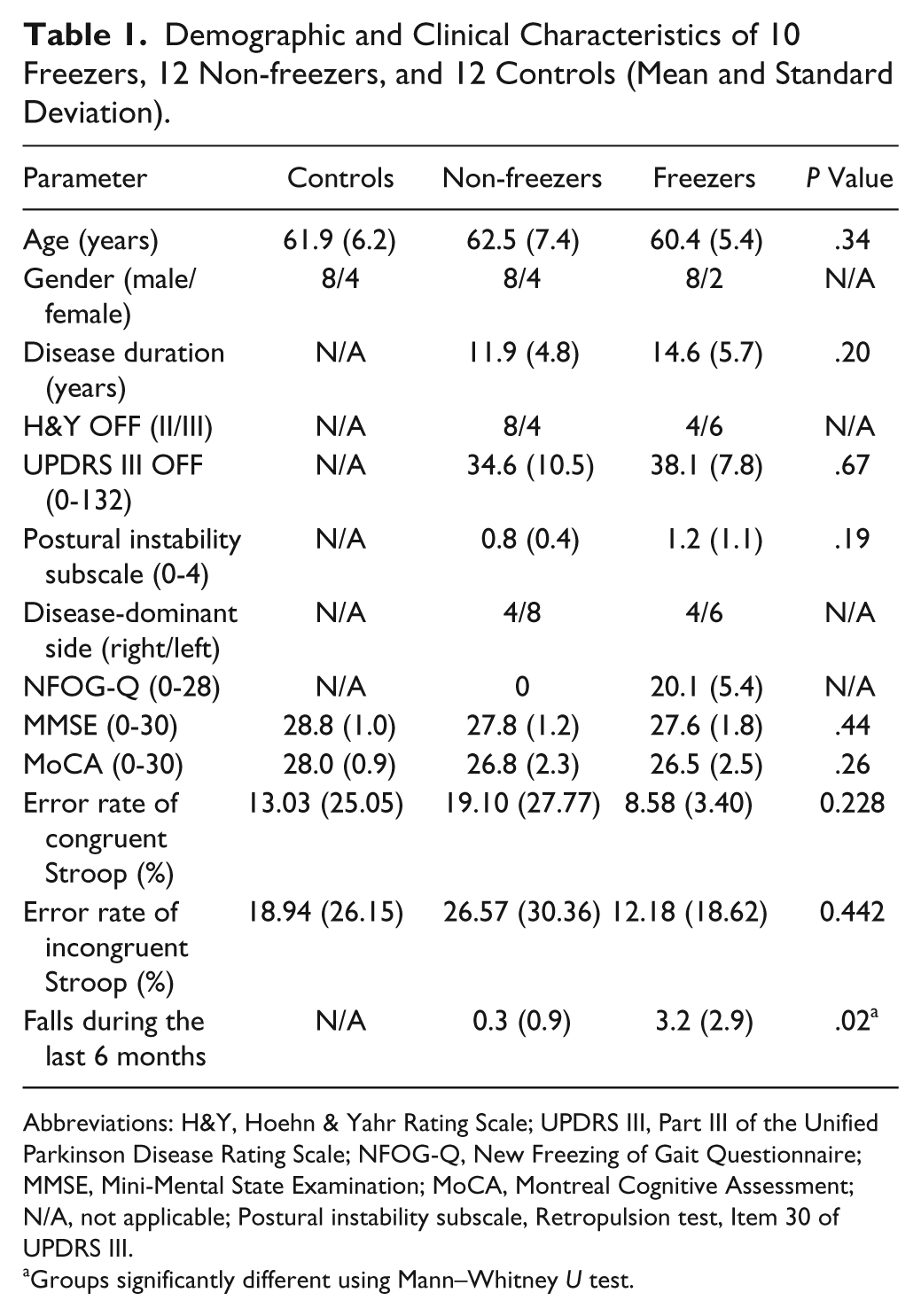
Abbreviations: H&Y, Hoehn & Yahr Rating Scale; UPDRS III, Part III of the Unified Parkinson Disease Rating Scale; NFOG-Q, New Freezing of Gait Questionnaire; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; N/A, not applicable; Postural instability subscale, Retropulsion test, Item 30 of UPDRS III.
Groups significantly different using Mann–Whitney U test.
Tied-Belt Conditions and Effect of Walking Speed
Freezers walked with significantly smaller mean and higher variability of limb excursion and larger asymmetry than non-freezers, and non-freezers than controls in both speeds (P < .05). Increasing speed decreased the variability of limb excursion only in freezers (P = .01) and non-freezers (P = .02). Step length asymmetry showed a significant decrease with increasing walking speed only in freezers (P = .03).
Split-Belt Conditions: Sudden Switching and Reswitching
Step length asymmetry was negative after the switch, due to shorter step lengths of the fast leg. After reswitching, values became positive, as the fast leg took longer steps. The changes of asymmetry during both switching and reswitching were significantly larger in freezers (significant group by condition interaction, P = .001) compared to non-freezers (P = .001), and in non-freezers compared to controls (P = .03).
Figure 2 shows the difference between the average limb excursions for the last 5 strides of tied-belt walking and the first 5 strides after the switch to split-belt condition (Figure 2A) and reswitch to tied-belt walking (Figure 2B). The increase in excursion after switching was smaller in freezers (significant group by condition interaction, P < .05), compared to non-freezers (P = .001), and in non-freezers compared to controls (P = .04). Following reswitching, freezers had a larger decrease in excursion, compared to non-freezers (P = .01), and non-freezers, compared to controls (P = .03).
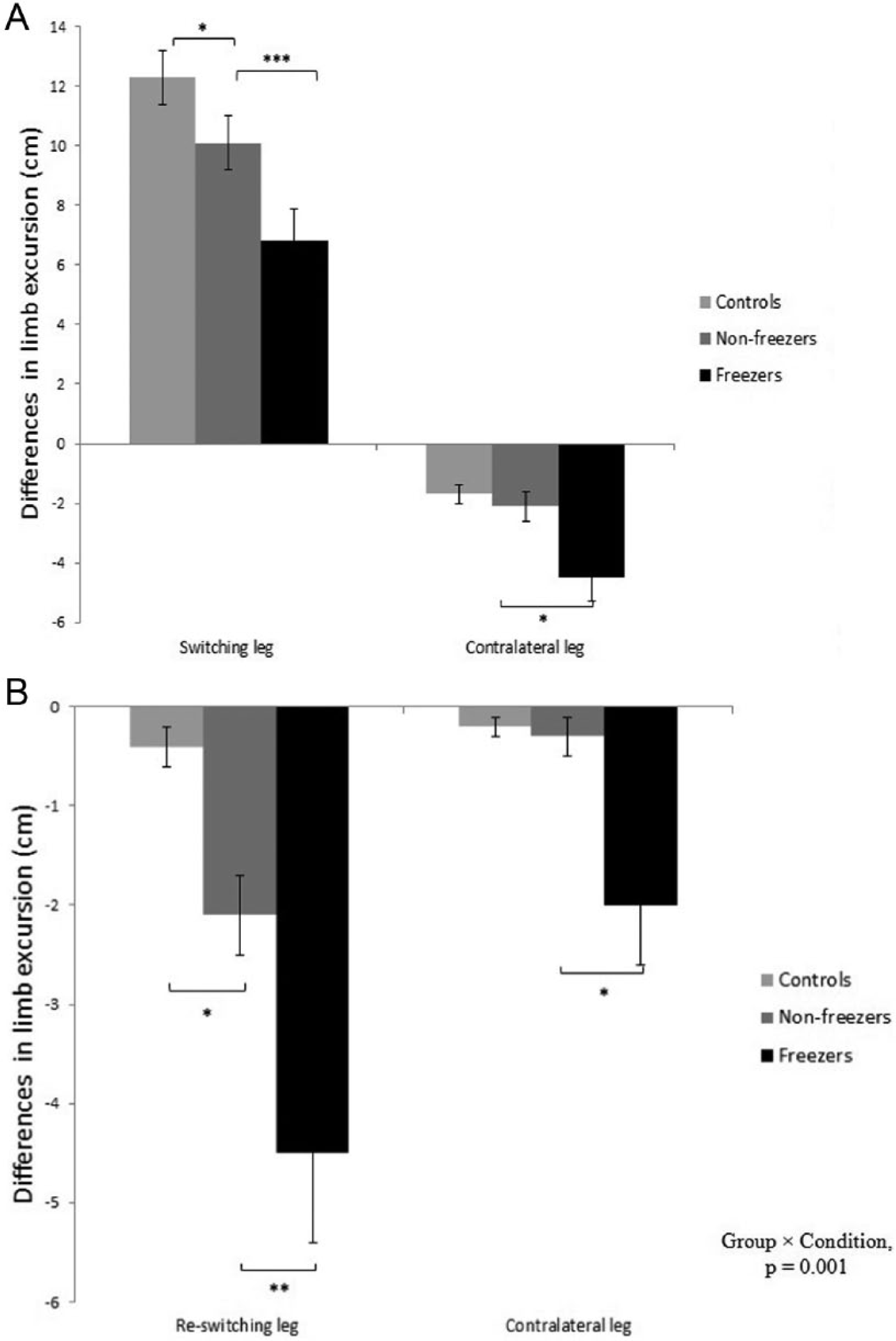
Differences in limb excursion between the last 5 strides of tied-belt walking and the first 5 strides after switching (A)/reswitching (B) and the changes in the other legs in freezers, non-freezers, and healthy controls. The mean values of the changes for the most and least affected legs of patients and dominant and non-dominant legs of controls were shown. Vertical bars represent standard error of measurements. *Significant difference at P < .05, **Significant difference at P < .01, ***Significant difference at P < .001.
Freezers had a greater decrease in limb excursions of the contralateral (slow) leg compared to non-freezers and controls (both P < .05). The exploratory analysis of the effect of disease-dominance on these results revealed that the differences between the 2 limbs did not survive Bonferroni corrections. There were no significant differences between step time asymmetry of the groups during switching and reswitching.
Gait Adaptation During Asymmetrical Gait and Re-Adaptation to Tied-Belt Condition
Figure 3 shows that freezers had a slower adaptation of step length asymmetry following the switch to split-belt walking compared to the reference groups and recovered symmetry slower (significant interaction of group by epoch, P = .001). Freezers had larger asymmetry for all epochs compared to the other 2 groups (P = .001), but the asymmetry of controls and non-freezers was only different for the first 4 epochs (P = .01).
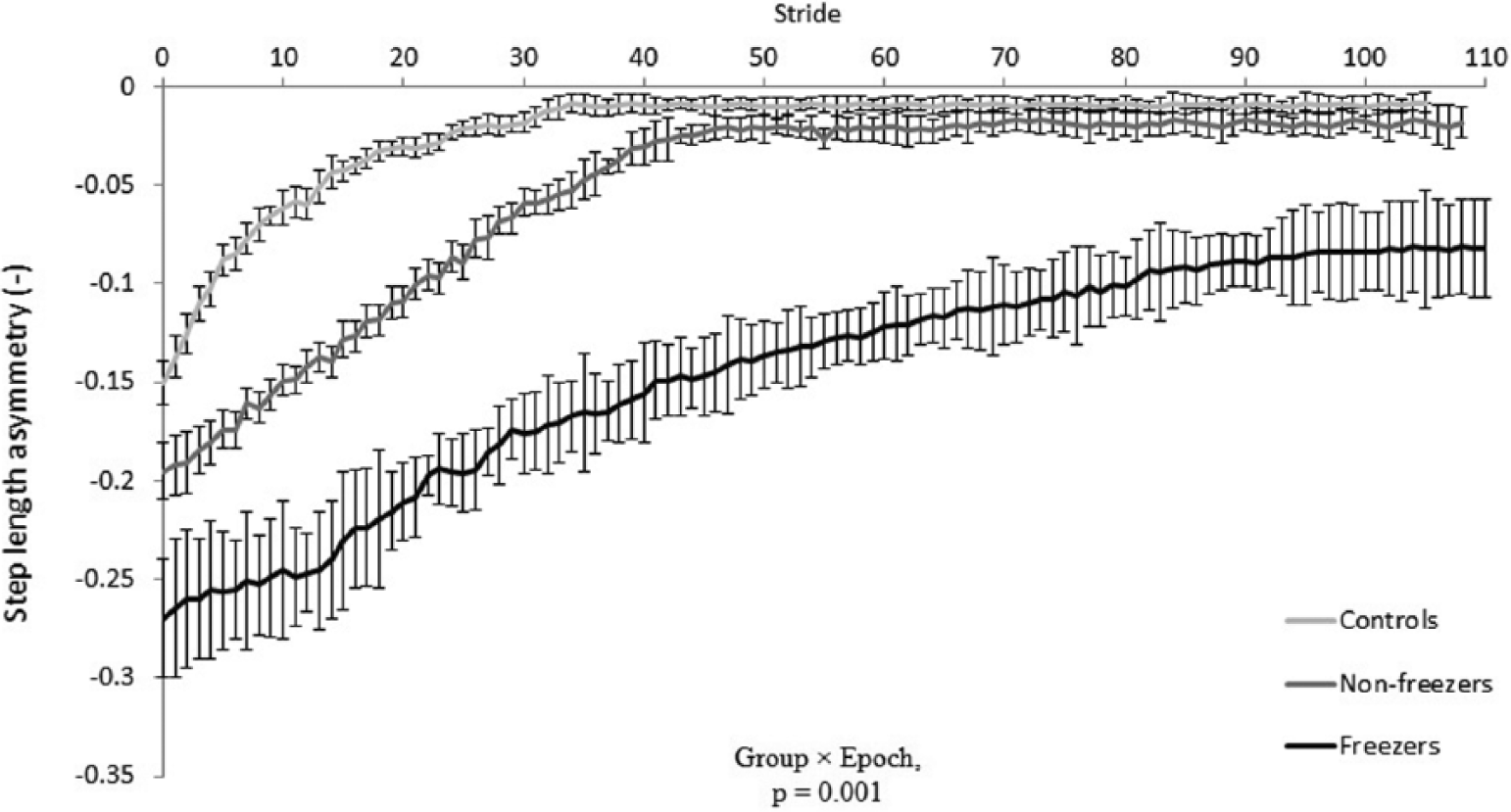
Step length asymmetry during adaptation period in freezers, non-freezers, and healthy controls. Data are represented by means of the 2 adaptation conditions. Values smaller than zero mean shorter step lengths of the fast leg. Vertical bars represent standard error of measurements.
During re-adaptation, as can be seen in Figure 4, there was a significant interaction of group by epoch (P = .001). Freezers had larger asymmetry for all epochs compared to the other 2 groups (P = .001), but there were also significant differences between asymmetry values of controls and non-freezers for the first 3 epochs (P = .01).
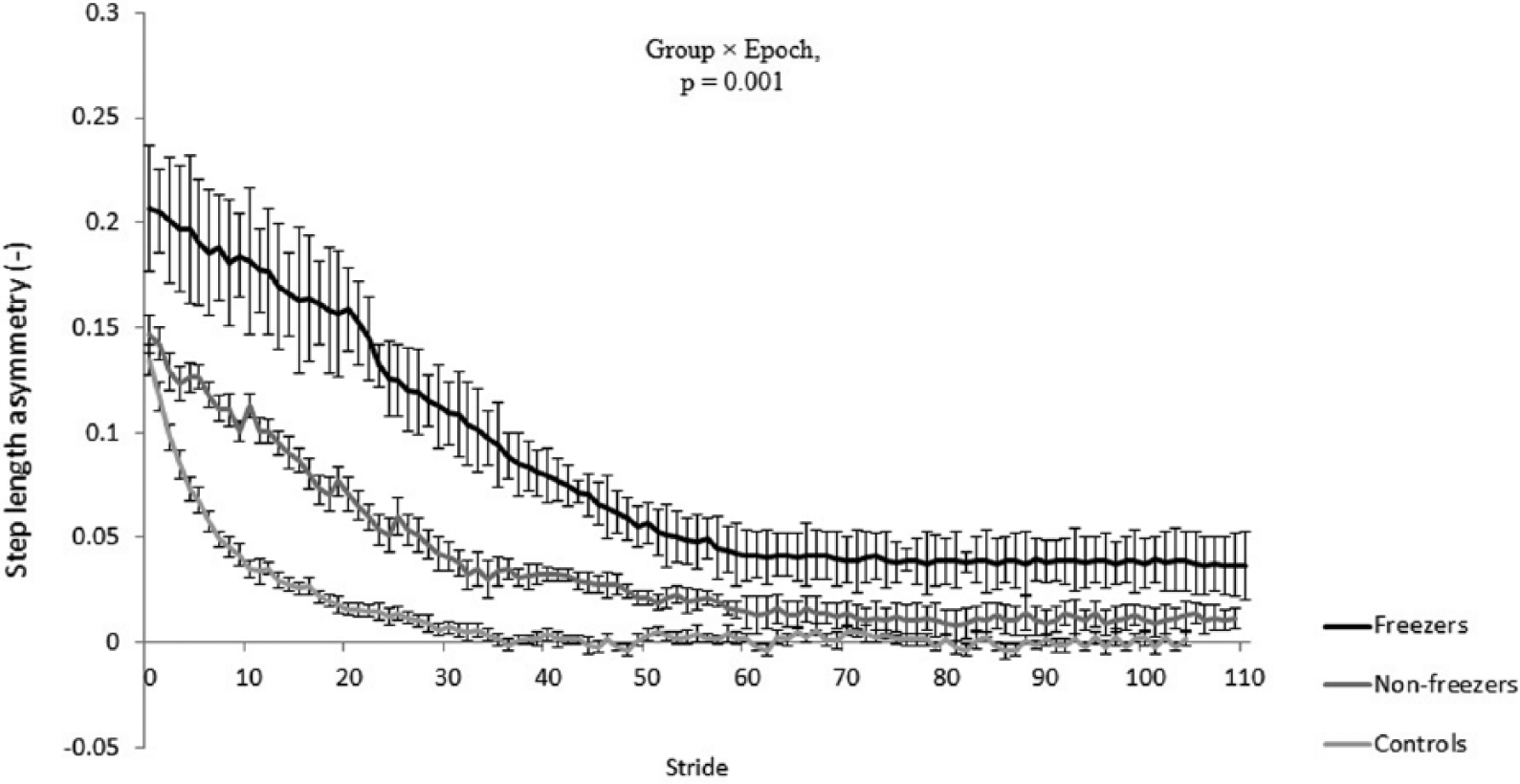
Step length asymmetry during re-adaptation period in freezers, non-freezers, and healthy controls. Data are represented by means of the 2 re-adaptation conditions. Values greater than zero mean longer step lengths of the fast leg. Vertical bars represent standard error of measurements.
Exploratory analysis of the effect of disease-dominance on the results did not survive Bonferroni corrections in any of the epochs. In the freezer group, differences in step length asymmetry at the end of adaptation and re-adaptation phases with tied-belt value were larger than in non-freezers (P = .01 and P = .03, respectively). There were no significant between-group differences for step time asymmetry during adaptation and re-adaptation.
Relationship Between Gait Measures and Clinical Parameters
A significant positive correlation was found between changes in step length asymmetry following switching and UPDRS III scores in all patients (r = .45, P = .03) and FOGQ scores in freezers (r = .56, P = .02). Higher FOGQ scores were also related to larger asymmetry values at the end of adaptation (r = .72, P < .001). There was a strong correlation between the retropulsion test (item 30 of UPDRS III, a routine measure of postural instability) in all patients with PD and step length asymmetry following switching (r = .75, P < .001), indicating that worse performance on the pull test (higher scores) are associated with larger step length asymmetry. There was no significant correlation between switching parameters and MoCA or Stroop scores.
Freezing Episodes
One patient experienced FOG (Figure 5A) and another one had a festination episode (Figure 5B), immediately after speed switching from 3 to 4 km/h for the most affected leg. Interestingly, the patients who showed these abnormalities also had larger increases of step length asymmetry (0.19 and 0.29) following switching compared to the other freezers (0.16 ± 0.04).
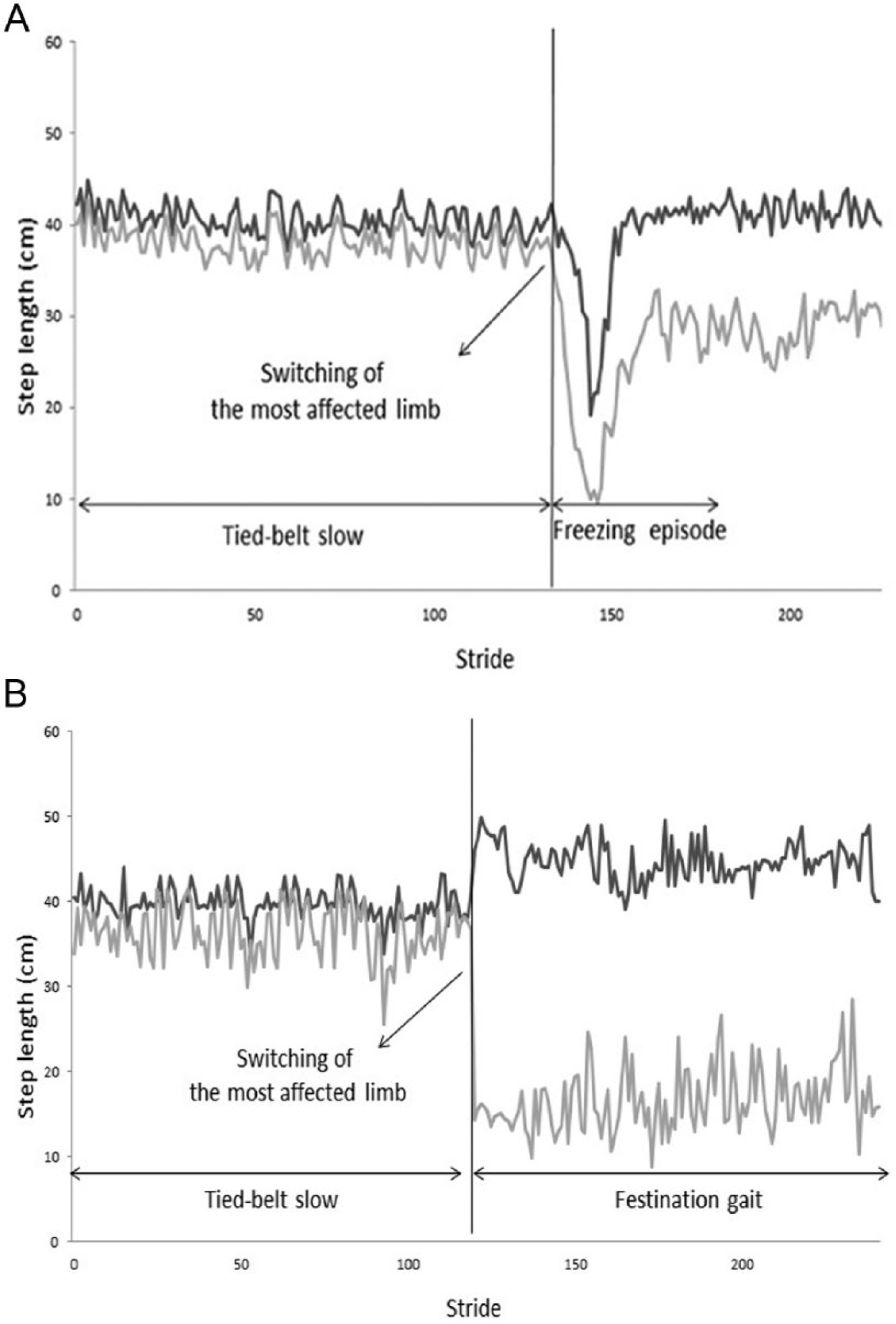
(A) Example of a freezing episode with a nearly complete loss of step length. Data are shown from a trial in which speed switching from symmetric walking to split-belt walking for the most affected leg (in gray) provoked a freezing episode. The freezing episode caused a reduction of step length below 50% of the normal step length for both most affected and least affected (in black) legs. (B) Example of festination gait after the switch from symmetric walking to split-belt walking for the most affected leg (in gray). The pattern was maintained during the whole adaptation period without any improvement of step length asymmetry. The patient showed a reduction of step length below 50% of the normal step length for the most affected leg.
Discussion
The novel finding of our study was that freezers modified their gait less well when responding to immediate switching of gait speed at one belt, compared to non-freezers and controls. Freezers also had a slower adaptation during split-belt walking and the following tied-belt walking than the other groups. Based on these results, we propose that freezers have a primary switching deficit as reduced switching performance was correlated to the severity of freezing and induced festination and freezing. In addition, switching problems may be exacerbated by the inability to adapt gait with time, which in turn may contribute to more variable and asymmetrical gait during tied-belt walking in freezers compared to non-freezers.
Sudden Switching and Reswitching
Tied-belt conditions induced gait abnormalities that were more prominent in freezers than in non-freezers, as has been reported before.11,20 In this study, we aimed to compare how PD subgroups adjust their gait following speed switching while they were unaware of the upcoming switch, causing an automatic gait perturbation. Motor switching from tied to split-belt walking caused a rapid adjustment of gait in all groups. These modifications were previously reported in healthy elderly, young subjects, stroke patients, and patients with cerebellar deficits.17,31,32 However, as we hypothesized, freezers showed a more severe switching impairment compared to the other 2 groups. Earlier studies in the cognitive domain indicated switching deficits under time pressure to be more pronounced in freezers than in non-freezers. This was interpreted as a primary deficit of automatic response processing, which did not allow timely compensation by more consciously generated executive responses. 28 Interestingly in the current study, freezers and non-freezers performed similarly on the MoCA and Stroop test, suggesting that cognitive set-shifting, a component of executive function, was similar in both groups. In addition, the split-belt switching outcomes were not correlated with MoCA and Stroop scores, suggesting that the main problem of freezers was motor switching and independent of cognitive function. Structural and functional disconnections between frontostriatal pathways in freezers may reduce freezers’ ability to keep the ongoing motor responses on-line while adjusting the motor program, resulting in inflexibility to shift from one response set to another.2,6,18 The work of Shine et al33,34 demonstrated in a virtual reality functional magnetic resonance imaging study that imposing high versus low cognitive load in freezers overloaded the information processing capacity of neural networks in freezers. This lead to breakdown of motor function, which was not apparent in non-freezers. These results were interpreted as associated with the diminished neural reserve in freezers, as evidenced by a functional decoupling between the basal ganglia and the cognitive control networks. 34
Earlier split-belt treadmill studies in healthy controls interpreted the adjustments following speed switching as modifications of the postural control system.17,32,35,36 As freezers did not differ in clinical characteristics from their non-freezing counterparts, except for frequency of falling, differences between groups may also be explained by the reduced capacity for postural adjustment in freezers, which was previously shown during sudden obstacle appearance 14 or sudden changes to platform perturbations. 37 Correlation analysis confirmed a strong association between the switching deficit and the retropulsion test in the patients. Both the basal ganglia 38 and structures at brain stem level have been reported to be involved in modulating postural adjustment and gait control. 39 In a recent study, Nonnekes et al 40 found a deficient automatic release of motor responses during the StartReact test in both gait initiation and ankle dorsiflexion in freezers only. They suggested that FOG could be due to dysfunctional pontomedullary reticular formation networks in conjunction with the pedunculopontine nucleus (PPN), involved in integrating anticipatory postural adjustments with a subsequent stepping response. Furthermore, it was proposed that time-varying gait demands, such as the switching task in this study, would further increase the computational load on these structures, leading up to gait breakdown. Hence, the possible neural mechanisms underlying the observed differences could be the differentially altered neural activity in these brainstem regions in freezers versus non-freezers, which is in line with recent neuroimaging data. 4
Adaptation and Re-Adaptation
We also aimed to compare gait adaptation of PD subgroups in response to asymmetrical walking and the following symmetrical gait. The results confirmed our hypothesis that the ability to adapt the gait pattern would be different for freezers during both phases, although reverting back to symmetrical tied-belt gait was less severely affected.
The reduced ability to adjust gait during both adaptation and re-adaptation in split-belt paradigms has traditionally been ascribed to functions of the cerebellum.17,32 A recent review suggested that altered cerebellar activity is implicated as part of the compensatory networks to generate movement in patients with PD. 21 Besides, the cerebellum and its projections to the brainstem and basal ganglia are also thought to be part of the so-called indirect gait pathway involved in modulating complex gait. 22 The deficient gait adaptation found in freezers could be related to reduced structural connectivity between the brainstem (PPN in particular) and the cerebellum, 7 which was recently highlighted using diffusion tensor imaging.6 Alternatively, the greater adaptation difficulties in freezers could be interpreted as a greater reliance on cerebellar compensatory function, which may have reached a ceiling effect earlier in freezers than in non-freezers.
Nanhoe-Mahabier et al 20 reported increased stride time variability during split-belt walking for freezers, but no differences in spatial measures between PD subgroups. These discrepant results may be explained by differences in calculating the gait parameters and the fact that they excluded the first 30 seconds of switching and analyzed the 10 consecutive strides. It has been suggested that at least 50 consecutive steps are needed to have an accurate measure of gait variability. 41 Furthermore, variability is not a greatly useful measure in split-belt walking, when the mean is slowly changing. Although freezers and non-freezers were well-matched for disease severity in this study, their patients had lower UPDRS scores and the freezers had lower NFOG-Q scores compared to the patients in the current study. Roemmich et al 36 investigated long-term adaptation and aftereffects during split-belt conditions of patients with PD in the ON state (the slow speed was 50% of the fast speed). PD patients and their matched controls adapted their gait in the same manner as reported in the current study. However, patients did not improve their gait asymmetry as in our study, which may reflect medication state and different disease profiles.
In this study, FOG episodes were rare, which is not an uncommon finding in FOG research in general1,42 and during treadmill walking in particular.14,20 Low freezing rates may be due to the fact that the treadmill acted as an external pacemaker. 43 Also, split-belt walking is different from real asymmetric gait during turning, which requires head and trunk rotation to achieve a directional change. 20 It is of note that the episodes could be predicted by the response to switching, in that patients with greater adaptive difficulties also tended to have FOG.
Our results may have implications for rehabilitation of freezers. Split-belt treadmill training has been used to improve symmetry in stroke patients. 17 The authors found that this improvement maintained with repeated exposures and partially transferred to over-ground walking. 44 Such a training protocol could be used for freezers as it may enhance the perception of leg speed and remedy gait asymmetry. Repetitive exposure to a split-belt treadmill may also be helpful to facilitate rapid adjustments and gait adaptation to novel situations. In addition, this form of implicit error-based motor learning could enhance the involvement of the cerebellum. These suppositions warrant further research.
Concluding, the results of the current study showed that fast switching to asymmetrical walking was more affected in patients with FOG compared to their non-freezing counterparts. Although it is difficult to distinguish between switching deficits and asymmetry problems in our study (as switching and asymmetrical walking happened simultaneously), the results strongly suggest that switching is a primary deficit in freezers. In addition, freezers showed more difficulty with slow gait adaptation to asymmetrical walking. These results are robust as subgroups were matched for disease severity and cognitive ability. The findings point to future rehabilitation interventions targeting these switching deficits using split-belt training.
Footnotes
Acknowledgements
The authors would like to thank Jasper Van der Donck, Aniek Bengevoord, and Pieter Ginis for their help with data collection. With great sadness we want to acknowledge the death of Farshid Mohammadi, the main author of this paper, on the 23rd of August 2014. He was a much appreciated colleague.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This research was funded by the European Commission through MOVE-AGE, an Erasmus Mundus Joint Doctorate Program (2011-2015), awarded to Alice Nieuwboer, Gert Kwakkel and Erwin E. van Wegen. Additional support for this study was provided through a grant from the Research Council of KU Leuven, Belgium (contract OT/11/091). Sjoerd M. Bruijn was supported by an F.W.O grant (G.0901.11) to J. Duysens, and a grant from the Netherlands Organization for Scientific Research (NOW#451-12-041).