
Abstract
Background
Although rehabilitation is beneficial for individuals with traumatic brain injury (TBI), a significant proportion of them do not receive adequate rehabilitation after acute care.
Objective
Therefore, the goal of this prospective and multicenter study was to investigate predictors of access to rehabilitation in the year following injury in patients with TBI.
Methods
Data from a large European study (CENTER-TBI), including TBIs of all severities between December 2014 and December 2017 were used (N = 4498 patients). Participants were dichotomized into those who had and those who did not have access to rehabilitation in the year following TBI. Potential predictors included sociodemographic factors, psychoactive substance use, preinjury medical history, injury-related factors, and factors related to medical care, complications, and discharge.
Results
In the year following traumatic injury, 31.4% of patients received rehabilitation services. Access to rehabilitation was positively and significantly predicted by female sex (odds ratio [OR] = 1.50), increased number of years of education completed (OR = 1.05), living in Northern (OR = 1.62; reference: Western Europe) or Southern Europe (OR = 1.74), lower prehospital Glasgow Coma Scale score (OR = 1.03), higher Injury Severity Score (OR = 1.01), intracranial (OR = 1.33) and extracranial (OR = 1.99) surgery, and extracranial complication (OR = 1.75). On contrast, significant negative predictors were lack of preinjury employment (OR = 0.80), living in Central and Eastern Europe (OR = 0.42), and admission to hospital ward (OR = 0.47; reference: admission to intensive care unit) or direct discharge from emergency room (OR = 0.24).
Conclusions
Based on these findings, there is an urgent need to implement national and international guidelines and strategies for access to rehabilitation after TBI.
Introduction
Around 12% of people worldwide have a history of traumatic brain injury (TBI). 1 In Europe, the annual incidence of hospital-treated TBI is 262 cases per 100 000 persons, and the 2 most frequent causes are falls and road traffic accidents. 2 TBI is a leading cause of deaths worldwide,3 -5 and a risk factor for a wide range of chronic physical, cognitive, emotional, and psychiatric problems. 6 Furthermore, TBI is associated with decreased self-care, difficulties with social relationships and diminished quality of life. 7 Therefore, rehabilitation plays a major role in the management of TBI, and multidisciplinary rehabilitation interventions are often needed in the months following injury.
Based on the definition of the World Health Organization, rehabilitation is “a set of interventions designed to optimize functioning and reduce disability in individuals with a health condition who experience some form of limitation in functioning, across the continuum of care and throughout the lifespan.” 8 Rehabilitation may be undergone in inpatient (eg, general rehabilitation unit, geriatric unit) and outpatient settings (eg, community, outpatient clinic). Although rehabilitation is widely considered as beneficial for survivors of TBI, 9 a substantial proportion of patients do not receive adequate rehabilitation after acute care.10,11 For example, a study including 508 patients with moderate-to-severe TBI from the Netherlands showed that discharge was home for 49% of the sample. 10 In the past years, several studies have investigated predictors of referral to rehabilitation in survivors from TBI.12-17 A French study of 254 cases of severe TBI showed that living alone, low socioeconomic status, preinjury alcohol abuse, low TBI severity (eg, high Glasgow Outcome Scale [GOS] scores at acute care discharge), and transfer through a nonspecialized medical ward before discharge were significant predictors for non-referral to rehabilitation. 13 Another prospective study including 566 patients with severe TBI from Switzerland found that lower scores on the Glasgow Coma Scale (GCS) at admission and at 14 days, higher injury severity scores, and older age were positively associated with inpatient rehabilitation. 16 These previous studies have several limitations that need to be acknowledged. First, without an international setting,12-17 the generalization of these previous findings may be limited. Second, the majority of these studies did not include patients with mild or moderate TBI,13-16 and thus little is known about the predictors of access to rehabilitation in these populations. Third, previous research has failed to adjust for several factors that may impact the odds for rehabilitation (eg, alcohol use,12,15 psychiatric disorders,12,15 area of injury [ie, rural or urban]12-17). Considering these limitations, new research is needed to gain a better understanding of predictors of access to rehabilitation in patients with TBI.
The present study is part of a larger European international prospective study, the CENTER-TBI study (for a complete list of participants and investigators, see the appendix). 18 Our main objective was to investigate predictors of access to rehabilitation in the year following TBI. Because TBI is a major public health concern in Europe, 19 identifying factors that may affect access to rehabilitation in this region might help reduce the associated burden.
Methods
Study Participants
Data from a large European project that aims to improve the care for patients with TBI (CENTER-TBI) were used. 18 Briefly, this was a prospective longitudinal observational study including 4509 patients with TBI of all severities from countries across Europe and Israel. 18 As the present study focused on rehabilitation in European countries, patients from Israel were excluded (N = 11), and the final sample consisted of 4998 participants aged between 0 and 96 years (Supplementary Figure 1). Inclusion criteria were (a) presentation to one of the study sites (mostly level-1 trauma centers) within 24 hours of TBI and (b) need for head computed tomography (decision based on standard clinical practices of the participating centers). TBI diagnosis was made at the discretion of the participating centers, and relied on the anamnesis, the clinical evaluation, and paraclinical investigations. Exclusion criteria were severe preexisting neurological disorders that would confound outcome assessments. Care pathways included 3 severity strata: intensive care unit (ICU) stratum (patients admitted to an ICU), admission stratum (patients admitted to a hospital ward), and emergency room (ER) stratum (patients directly discharged from ER). Lengths of follow-up differed between ICU and admission strata (ie, 12 months) and ER stratum (ie, six months). Data were collected between December 2014 and December 2017. Details about ethics approval can be found in previous CENTER-TBI publications.20,21 Finally, the study followed STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines (Supplementary Table 1), while the study registration number was NCT02210221 (https://clinicaltrials.gov/).
Data Collection, Handling, and Storage
Demographic and clinical data were collected using an online electronic form, and data were de-identified and stored on a secure database. 20 Data curation was done by a multidisciplinary data curation task force and the members of the Work Package 14. All CENTER-TBI variables are available at https://www.center-tbi.eu/data/dictionary (Data Dictionary).
Access to Rehabilitation (Dependent Variable)
Access to inpatient or outpatient rehabilitation was assessed at 3, 6, and 12 months after injury. For the purpose of this study, patients were dichotomized into those who received and those who did not receive rehabilitation care (inpatient and/or outpatient rehabilitation) within the year following TBI (ie, at 3, 6, or 12 months). Inpatient rehabilitation facilities included units specialized in TBI rehabilitation, general rehabilitation units, general long-term acute care units, and geriatric units. Outpatient rehabilitation included physical therapy, occupational therapy, psychological services, cognitive remediation, speech therapy, social work, recreational therapy, nursing services, independent living training, vocational services, peer mentoring, comprehensive day treatment, and home health. Outpatient rehabilitation was undergone in a variety of different settings (eg, community, outpatient clinic) that were not documented in the database. Finally, neither inpatient nor outpatient rehabilitation included tele-rehabilitation.
Predictors of Access to Rehabilitation (Independent Variables)
Sociodemographic Factors
Sociodemographic factors included sex (male or female), age (in years), marital status (not married/separated/divorced/widowed/other or married/living together), number of years of education completed, preinjury employment (yes or no), and region (ie, Western, Northern, Southern, Central and Eastern Europe). Following the EuroVoc classification, 22 Western Europe (N = 2308) included Austria (N = 109), Belgium (N = 315), France (N = 115), Germany (N = 185), Netherlands (N = 1006), and the United Kingdom (N = 578); Northern Europe (N = 1090) included Denmark (N = 15), Finland (N = 372), Latvia (N = 105), Lithuania (N = 45), Norway (N = 419), and Sweden (N = 134); Southern Europe (N = 973) included Italy (N = 560) and Spain (N = 413); and Central and Eastern Europe (N = 127) included Hungary (N = 43), Romania (N = 21), and Serbia (N = 63).
Psychoactive Substance Use
Psychoactive substances included tobacco, alcohol, sedative drugs, cannabis, and other illicit drugs (current use of each of these substances: yes or no).
Preinjury Medical History
Factors related to preinjury medical history were the American Society of Anesthesiologists (ASA) Physical Status score, 23 any neurological condition (yes or no), any other somatic condition (yes or no), any psychiatric condition (yes or no), previous TBI (yes or no), use of beta-blockers (yes or no), and use of anticoagulants or platelet aggregation inhibitors (yes or no). The ASA score included 4 categories: I (a normal healthy patient), II (a patient with mild systemic disease), III (a patient with severe systemic disease), and IV (a patient with a severe systemic disease that is a constant threat to life). Any neurological condition included neurological diseases and neuropathic pain. Any other somatic condition included cardiovascular, developmental, endocrine, gastrointestinal, hematological, hepatic, musculoskeletal, oncologic, otorhinolaryngological, pulmonary, renal, and other diseases. Regarding previous TBI, patients were dichotomized in those with at least 1 previous TBI and those without any previous TBI.
Injury-Related Factors
Injury-related factors included geographical area of injury (urban or rural), injury intention (ie, unintentional, intentional, undetermined), prehospital GCS score, and Injury Severity Score (ISS). The ISS is calculated as the sum of the squares of the 3 highest Abbreviated Injury Scale (AIS) scores. 24 The AIS, a scale used to describe patients’ needs for treatment, has the following categories: minor (1; no treatment required), moderate (2; requires outpatient treatment only), serious (3; requires inpatient treatment outside ICU), severe (4; requires observation and/or basic inpatient treatment inside ICU), critical (5; requires intubation, mechanical ventilation or vasopressors for blood pressure support), and unsurvivable (6; not survivable). 18 The ISS ranges from 0 to 75 with higher scores indicating more severe injuries, and the ISS is automatically assigned 75 if there is any injury with an AIS of 6.
Medical Care, Complications, and Discharge
The variables related to medical care, complications and discharge were stratum (ie, admitted to ICU, admitted to hospital ward, directly discharged from ER), intracranial surgery (yes or no), extracranial surgery (yes or no), intracranial complication (yes or no), extracranial complication (yes or no), and GCS score at discharge. Stratum is a variable that depicts pathways of care following TBI but also an overall measure of injury severity. Patients were allocated to each stratum based on the initial medical decision, and they remained in the same stratum throughout the study. However, because of potential clinical worsening, it remains possible that individuals who had been initially discharged from ER were later admitted to hospital ward or ICU.
Statistical Analyses
As there were approximatively 13% of missing data in the database, missing data were imputed using multiple imputation by chained equations (MICE). 25 Multiple imputation was preferred over single imputation because it allows the estimation of the distribution of plausible values for missing data. 26 It was hypothesized that missing data were missing at random (MAR), meaning that the propensity for a value to be missing was related to observed data but not missing data. 27 The number of imputed data sets was estimated using the prevalence of incomplete cases. 26 Thus, 80 and 70 data sets were imputed for the analyses including the overall sample and patients who had access to outpatient rehabilitation, respectively.
Differences in the sample characteristics between those who had and those who did not have access to rehabilitation in the year following injury were tested with chi-square tests for categorical variables and Mann-Whitney tests for continuous variables (ie, age, number of years of education completed, prehospital GCS score, ISS, GCS score at discharge). Mann-Whitney tests were used for continuous variables because the data were not normally distributed.
Logistic regression analyses were conducted to assess the association between potential predictors (independent variables) and access to rehabilitation in the year following injury (dependent variable). Because of the large number of potential predictors, independent variables included in the regression models were selected using a 2-stage procedure. During the first stage, variables were preselected in the 80 imputed data sets separately using a least absolute shrinkage and selection operator (LASSO) regression. Briefly, the LASSO regression is a method that shrinks unstable estimates toward zero and thus excludes irrelevant variables. 28 LASSO regression has been found to outperform other common variable selection methods (eg, stepwise selection, best subset selection). 29 During the second stage, the number of preselections per variable was calculated, and variables that were preselected more than 60 times were considered as potential predictors. Given that the literature on the combination of the LASSO regression with multiple imputations is scarce, the previous cutoff was arbitrarily chosen to allow the selection of variables that were preselected in more than 75% of the imputed data sets, and to indirectly allow a relatively large number of potential predictors to be included in the regression analysis. Ten variables were finally included in the regression model: sex, number of years of education completed, preinjury employment, region, prehospital GCS score, ISS, stratum, intracranial surgery, extracranial surgery, and extracranial complication. Among them, seven variables were preselected in all 80 imputed data sets. All variables were included in the models as categorical variables with the exception of number of years of education completed, prehospital GCS score and ISS, which were included as continuous variables. Sensitivity analyses were further conducted in different age groups (ie, <18 years, 18-65 years, >65 years) and strata (ie, admission to ICU, admission to hospital ward, direct discharge from emergency room) to study the replicability of the study findings in these subgroups. Adjusted regression models were conducted in each of the imputed datasets and results were subsequently pooled. Pooled results from the logistic regression analyses are presented as odds ratios (ORs) with 95% confidence intervals (CIs).
The statistical analysis was performed with R 3.6.2 (The R Foundation). 30 P values were corrected using the Benjamini-Hochberg adjustment method, and P values <.05 were considered statistically significant.
Results
A total of 4498 patients were included in this study. After multiple imputations, 67.0% were men and the median (interquartile range [IQR]) age was 50.0 years (30.0-66.0 years) (Table 1). The prevalence of rehabilitation within the year following TBI was 31.4% (inpatient rehabilitation: 17.8%; outpatient rehabilitation: 20.8%; both inpatient and outpatient rehabilitation: 7.2%), and was significantly different between the 3 strata (ie, admitted to ICU, 48.3%; admitted to hospital ward, 19.2%; directly discharged from ER, 10.7%; P < .001). Preinjury employment, living in Northern or Southern Europe, no preinjury use of beta-blockers, no preinjury use of anticoagulants or platelet aggregation inhibitors, rural area of injury, undetermined injury intention (ie, neither unintentional nor intentional), admission to ICU, intracranial surgery, extracranial surgery, intracranial complication, and extracranial complication were more frequent in patients who had than in those who did not have access to rehabilitation, while age, prehospital GCS score and GCS score at discharge were lower, and number of years of education completed and ISS higher in the group with rehabilitation than in the group without rehabilitation. The two most frequent inpatient rehabilitation facilities were units specialized in TBI rehabilitation (59.6%) and general rehabilitation units (43.2%; Figure 1), while the 5 most frequent types of outpatient rehabilitation were physical therapy (80.9%), occupational therapy (27.2%), psychological services (22.5%), cognitive remediation (20.9%), and speech therapy (20.9%; Figure 2). The results of the adjusted regression analysis including the 10 variables that were preselected using the LASSO procedure are displayed in Figure 3. Access to rehabilitation was positively and significantly predicted by female sex (OR = 1.50), increased number of years of education completed (OR = 1.05 [per 1-unit increase in years]), living in Northern (OR = 1.62; reference: Western Europe) or Southern Europe (OR = 1.74), prehospital GCS score (OR = 1.03 [per 1-unit decrease in the total GCS score]), ISS (OR = 1.01 [per 1-unit increase in the total ISS]), intracranial surgery (OR = 1.33), extracranial surgery (OR = 1.99), and extracranial complication (OR = 1.75). In contrast, significant negative predictors were lack of preinjury employment (OR = 0.80), living in Central and Eastern Europe (OR = 0.42), and admission to hospital ward (OR = 0.47; reference: admission to intensive care unit) or discharge from emergency room (OR = 0.24). Similar findings were overall obtained in patients aged 18 to 65 years (ie, the working age population) and in those admitted in ICU (Supplementary Table 2).
Sample Characteristics Before and After Multiple Imputations (Overall and by Rehabilitation Status).
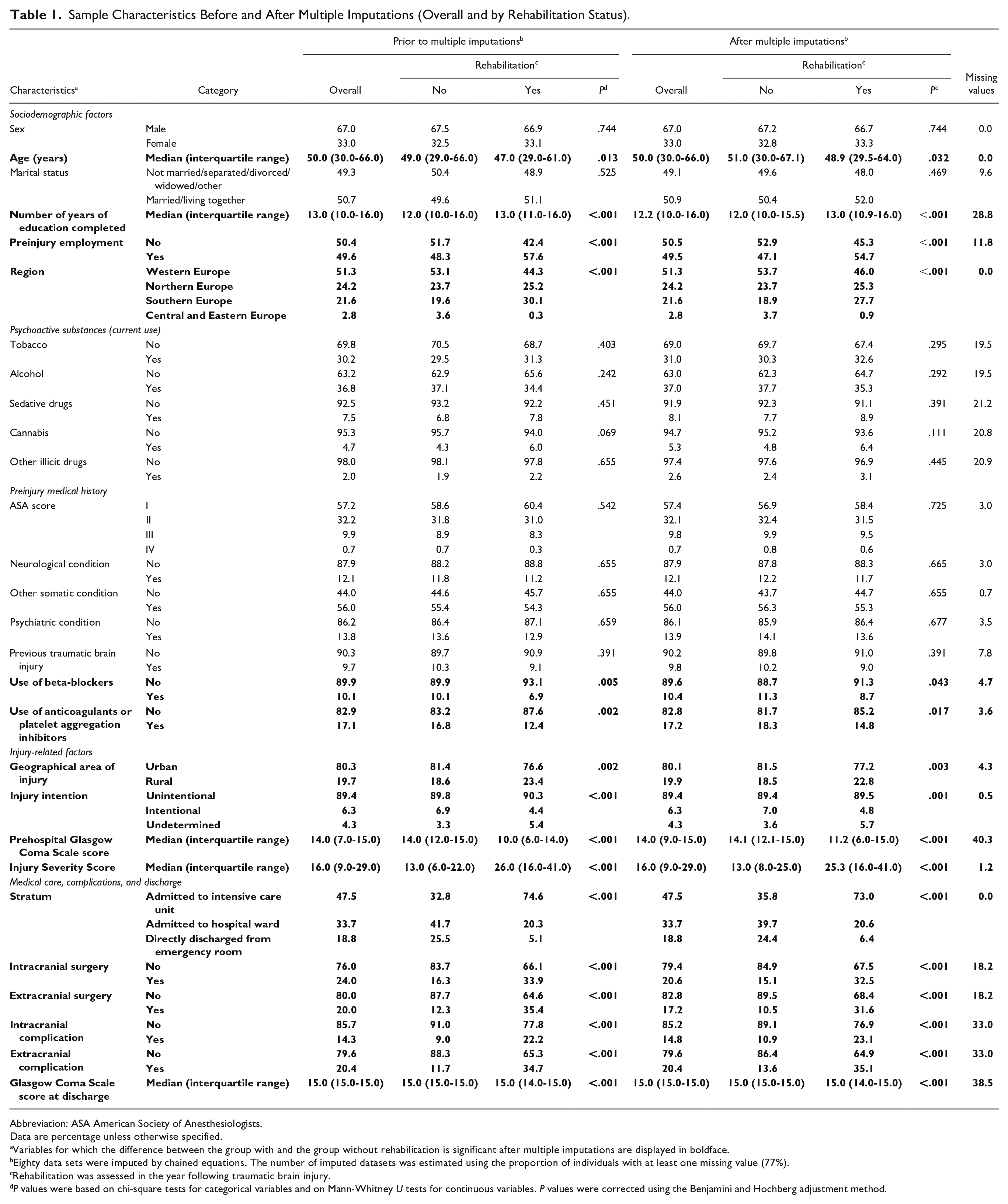
Abbreviation: ASA American Society of Anesthesiologists.
Data are percentage unless otherwise specified.
Variables for which the difference between the group with and the group without rehabilitation is significant after multiple imputations are displayed in boldface.
Eighty data sets were imputed by chained equations. The number of imputed datasets was estimated using the proportion of individuals with at least one missing value (77%).
Rehabilitation was assessed in the year following traumatic brain injury.
P values were based on chi-square tests for categorical variables and on Mann-Whitney U tests for continuous variables. P values were corrected using the Benjamini and Hochberg adjustment method.
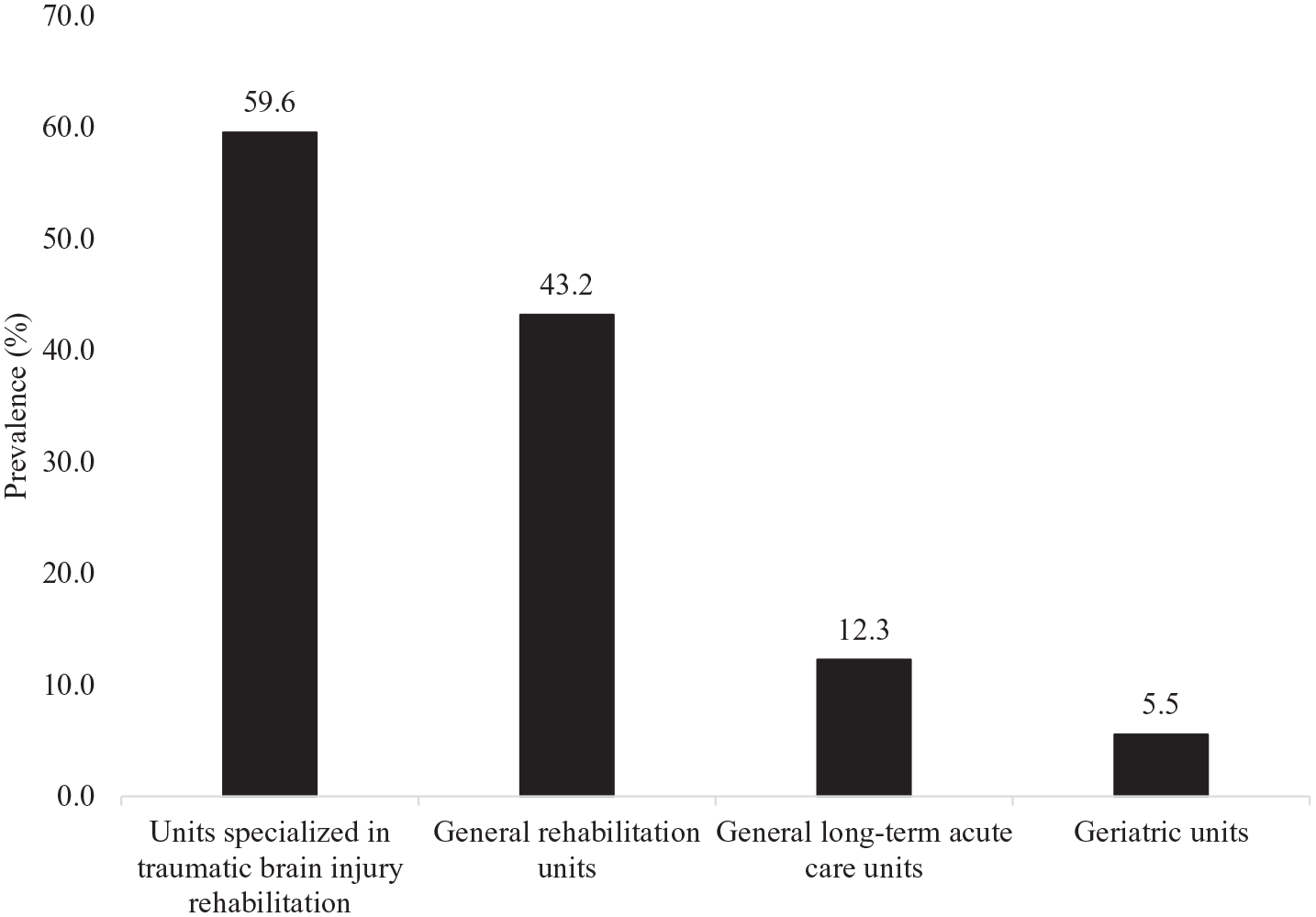
Types of medical units involved in the inpatient rehabilitation of patients with traumatic brain injury.
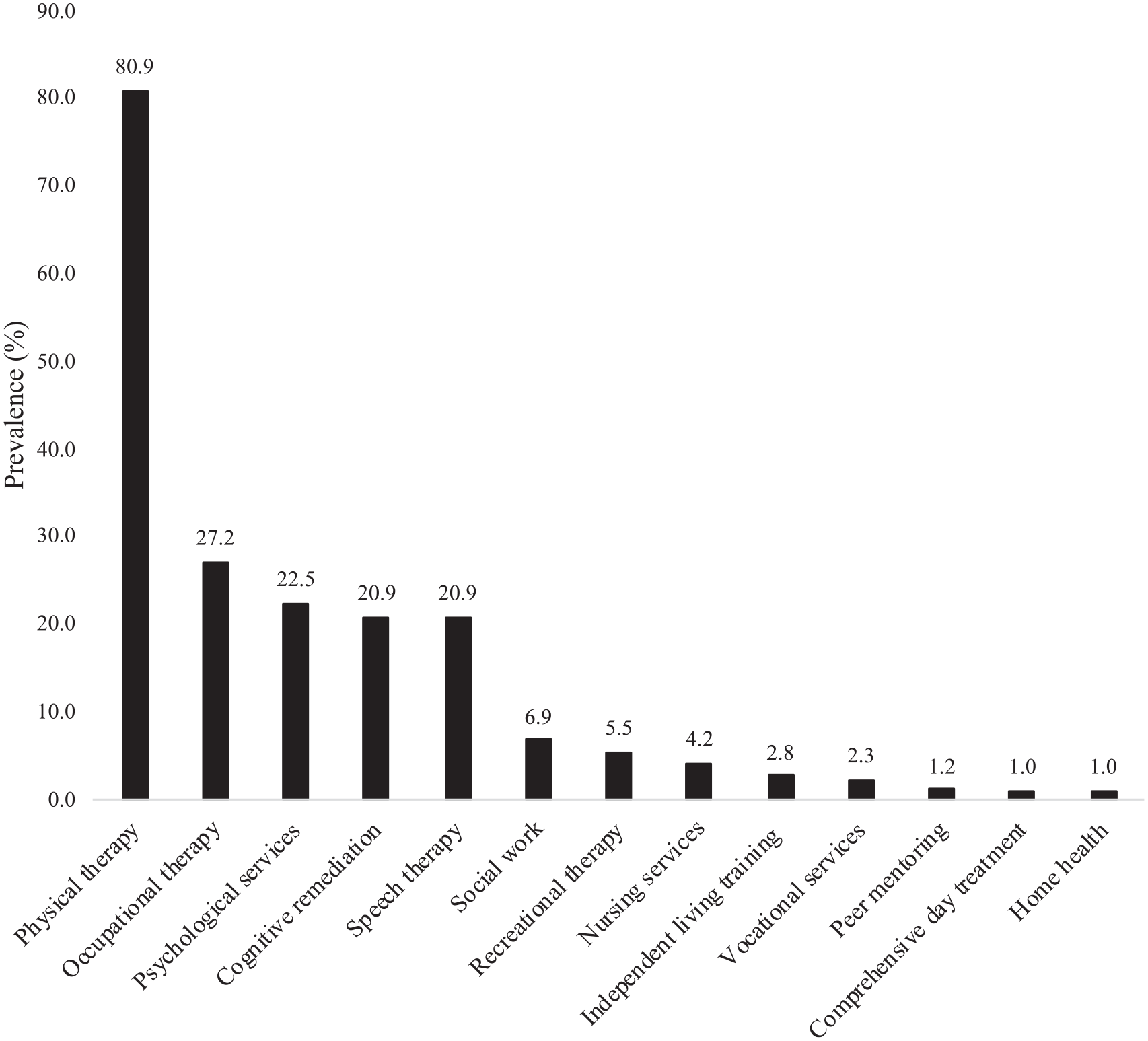
Types of outpatient rehabilitation in patients with traumatic brain injury.
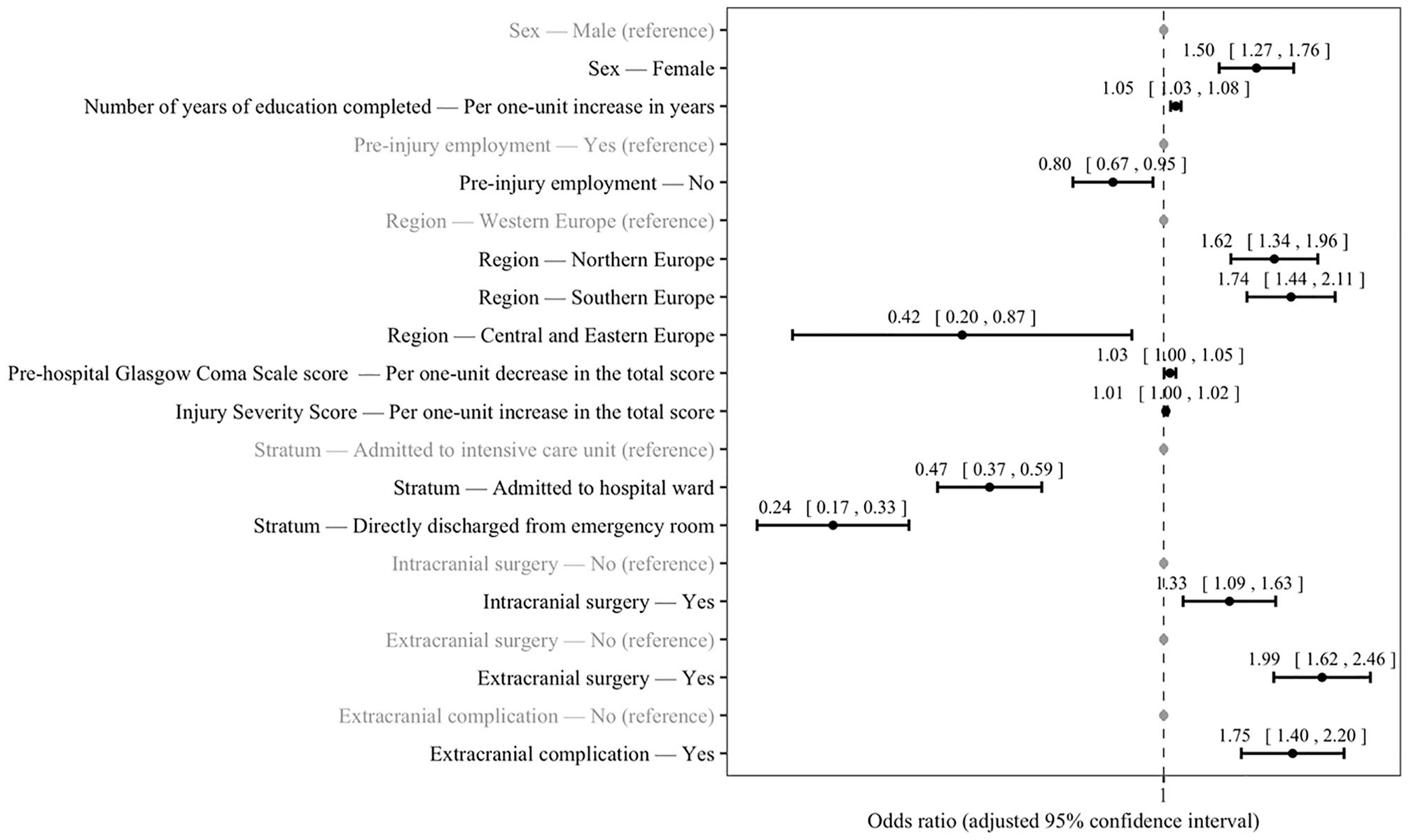
Predictors of rehabilitation in the year following the injury in patients with traumatic brain injury (LASSO penalized logistic regression).
Discussion
Main Findings
The prevalence of rehabilitation in the year following injury was around 31% in this European study. Significant predictors of access to rehabilitation were sex, number of years of education completed, preinjury employment, region, prehospital GCS score, ISS, stratum, intracranial surgery, extracranial surgery, and extracranial complication. To the best of our knowledge, this is the first international longitudinal observational study investigating predictors of access to rehabilitation in the year following TBI.
Interpretation of the Findings
It was observed that access to rehabilitation in the year following TBI was relatively low, even for individuals with severe TBI. This is in line with recent single-country studies conducted in different settings.10,11,13 In terms of the type of rehabilitation, the study results also concur with results from another secondary analysis of the PariS-TBI cohort, 14 and both studies identified physical therapy, occupational therapy, psychological services, cognitive remediation, and speech therapy as frequent types of rehabilitation after TBI. It remains however surprising that, although cognitive impairments and behavioral changes are major causes of disability after TBI, 31 access was lower for psychological services and cognitive remediation than for physical therapy in patients with TBI, and this raises concerns about the adequacy of available resources for the patients’ needs. That being said, the reasons for the lack of rehabilitation were not documented in the present study, and factors other than adequacy of available resources (eg, lack of referral to occupational and speech therapists, healthcare professionals’ assumptions about the benefits of rehabilitation for a given individual, patient reluctance to undergo rehabilitation) may be important.
There was a significant association between several sociodemographic factors and the odds of rehabilitation in the year following injury. Female sex was positively associated with access to rehabilitation in patients with TBI. Given that previous research has yielded opposite results,15,16 this finding must be interpreted with caution. However, previous studies included patients with severe TBI only, while statistical analyses were not adjusted for several confounding factors such as education and complications, and this may explain the discrepancy between this work and the literature. One hypothesis to explain the association between sex and access to rehabilitation is that men are less adherent to rehabilitation programs after TBI than women, and further studies are needed to test this hypothesis. This study further showed for the first time that educational attainment was positively associated with access to rehabilitation. As educational attainment also predicts functional recovery after moderate-to-severe TBI, 32 the present study suggests that the burden of TBI may be particularly high in people with a lower educational level. Moreover, having no preinjury employment was a risk factor for not undergoing rehabilitation compared with having a preinjury employment. This finding is in line with the literature,13,15 and underlines potential inequalities by income levels and type of health insurance in the access to rehabilitation after TBI. In addition, given that unemployment is a risk factor for lack of social support, 33 it is possible that marginalization also plays a significant role in the relationship between preinjury employment and the access to rehabilitation following TBI. The odds of rehabilitation were also higher in patients living in Southern or Northern Europe, and lower in those living in Central and Eastern Europe, rather than in those living in Western Europe. This may be explained by differences in the numbers of rehabilitation professionals and by differences in health care funding between European countries. Indeed, recent statistics indicate that the number of physiotherapists per 100 000 inhabitants is much lower in Central and Eastern European countries than in Western and Northern European countries, 34 while the most common payment systems for occupational therapy in primary care vary widely between these countries. 35 Another important finding of this study is that age was not included in the regression model after applying the 2-stage variable selection procedure, and therefore was deemed not to be a potential predictor of access to rehabilitation in the year following TBI. This finding must be interpreted with caution as previous research has obtained opposite results.12,15-17 However, previous research failed to adjust for pathways of care, 15 and it is reasonable to think that older adults are at a higher risk of not being admitted to ICU and thus at a higher risk of not having access to rehabilitation than younger adults.
One additional major predictor of rehabilitation in the year following TBI that was identified in this study was stratum (ie, admission to ICU, admission to hospital ward, direct discharge from ER), which is an indirect measure of TBI severity. The present findings corroborate the results of a cohort study of a smaller sample size identifying transfer through a nonspecialized medical ward before discharge as a risk factor for nonreferral to rehabilitation (OR = 0.08). 13 Another study of retrospective cohort design (N = 10 443 patients with TBI) further showed that variables positively associated with the risk for being directly discharged home were young age, low Charlson Comorbidity Index, short length of stay in acute care, no special care day (ie, no day spent in ICU), cause of injury other than motor vehicle collision, and rural location. 11 Finally, a retrospective study of 343 patients with moderate-to-severe TBI from the Netherlands found that one-third of the sample was directly discharged home and that approximatively 26% of individuals returning home displayed unfavorable outcomes (ie, cognitive, behavioral, physical). 36 Taking together, these findings suggest that pathways of care after TBI have a significant impact on the odds of undergoing rehabilitation in the months following injury, and that patients discharged home may be at a higher risk for no rehabilitation than those admitted to ICU and later discharged to rehabilitation units.
Another interesting result of this study is that prehospital GCS score, ISS, intracranial surgery, extracranial surgery, and extracranial complication positively predicted the odds of rehabilitation, suggesting that initial severity of clinical impairments, injury severity, polytrauma, and complications may have a long-term impact on the access to rehabilitation. Although recovery of consciousness following TBI may be a slow process, 37 previous research has indicated that a substantial proportion of patients with impaired consciousness who undergo rehabilitation are able to achieve functional independence in several domains (eg, self-care, mobility, cognition) within the decade following TBI. 38 Rehabilitation interventions for patients in a minimally conscious state may focus on sensory stimulation, postural changes, and the prevention of joint contractures. 39 In terms of injury severity and polytrauma, patients with TBI frequently have other lesions such as facial trauma and limb fracture. 40 TBI survivors with polytrauma are more likely to have access to rehabilitation compared with their counterparts with TBI only because other lesions may be responsible of additional functional limitations (eg, dysphagia associated with facial trauma, limb fracture-related pain). Finally, the positive relationship of intra- and extracranial surgery with rehabilitation may be explained not only by the severity of the initial injury itself but also by the fact that these surgical procedures often require extended bed rest, and this can potentially have multiple deleterious effects on the body (eg, undernutrition, sarcopenia, cardiorespiratory deconditioning). 41 Unfortunately, our current analysis was unable to define whether the rehabilitation delivered was because of TBI itself, intracranial/extracranial injuries, complications, or all of them.
Finally, the sensitivity analyses overall corroborated the study findings in people aged 18 to 65 years and in those admitted to ICU after brain injury. This suggests that these results may be extrapolated to the working age population and to patients with severe TBI. The fact that numerous associations were not significant anymore in other subgroups (ie, patients admitted to hospital ward, those directly from emergency room, those aged <18 years, those aged >65 years) may be explained by the fact that the sample size of these subgroups was relatively small and the analyses might thus have lacked statistical power.
Implications and Directions for Future Research
Given that rehabilitation is associated with several positive outcomes in TBI (eg, increased attention, 42 return to independent functional status, 43 improved societal participation 44 ), while TBI is a major cause of disability, 7 implementing strategies favoring rehabilitation after TBI at both national and international level is essential. One key initiative is to give patients with TBI the opportunity to undergo rehabilitation even if they are discharged home after acute care, and rehabilitation programs may be conducted in day hospital or home settings. 45 Some of these programs may incorporate tele-rehabilitation, which has recently been developed in both pediatric and adult TBI populations,46,47 and this may help overcome the problem of access to specialized rehabilitation services. As neurobehavioral changes are frequent after TBI, and as patients may show poor self-awareness, 48 initiating early multidisciplinary rehabilitation may help patients better understand their needs and the potential interest of physical or occupational therapy. Furthermore, identifying patients who would benefit the most from rehabilitation is crucial, particularly in settings where the provision of rehabilitation services is limited. Health professionals should also bear in mind that male TBI patients and those with a low educational level or without preinjury employment are at an increased risk for lack of rehabilitation, and thus sex, educational attainment, and employment should be factors to take into account when identifying the most appropriate pathway of care for these patients. Finally, at the European level, measures should be taken to harmonize the management of patients with TBI across countries, while the education of rehabilitation professionals has to be extended and rehabilitation facilities to be implemented in regions with severely unmet needs (eg, Central and Eastern Europe). 49 In terms of future research, further international studies are warranted to corroborate the presents findings, and to better understand the reasons for the lack of rehabilitation in a high proportion of patients with TBI (eg, poor geographic access, financial barriers, lack of patient adherence, fragmented pathways of care). Moreover, since there are important differences between European neurotrauma centers in terms of structural and process characteristics of in-hospital acute rehabilitation and referral to postacute rehabilitation facilities,50,51 more studies are needed to better understand these differences and their potential impact on rehabilitation outcomes. Recent evidence suggests that rehabilitation following TBI should be early and intensive, while it should be undergone in specialized units. 52 Finally, new modalities of rehabilitation have recently emerged (eg, exercise therapy), and it is important to shed light on the potential role played by these therapies in the overall management of TBI survivors. 53
Strengths and Limitations
The major strengths of this study are the use of data from 17 European countries and the large sample size. Nonetheless, this study has also some limitations. Given that there is no standardized definition for access to rehabilitation, it was arbitrary defined in the present study as access to inpatient and/or outpatient rehabilitation. Furthermore, there was a lack of data on the duration of rehabilitation, and more detailed data on rehabilitation would have also allowed better understanding of the reasons for the lack of rehabilitation. Besides, several potential predictors of interest (eg, ethnicity, income, type of health insurance, early functional deficit or disability) were not included in the statistical analyses, while some of the data on rehabilitation relied on self-reports, and thus these data might have been subject to recall bias. In addition, this study only included patients presenting to study hospitals, which were all centers interested in neurotrauma, and thus it is possible that the access to rehabilitation is even worse elsewhere. Moreover, the stratum of those who were discharged from the ED was underrepresented in this sample and patients from this stratum were followed for six months only. It was also hypothesized that missing data were missing at random (MAR) and not missing not at random (MNAR), and this hypothesis may have affected the multiple imputation of missing data and indirectly the present findings. Finally, to the best of the knowledge of the authors, there is no clear statistical guidance on how to select independent variables using LASSO regression in multiple imputed datasets, and the cutoff of 60 preselections was arbitrarily chosen.
Conclusions
About one-third of patients had access to rehabilitation in the year following TBI in the participating European countries, and in addition to expected factors, sex, number of years of education completed, preinjury employment, and region of living were significantly associated with the odds of rehabilitation. Based on these results, there is an urgent need to implement national and international guidelines and strategies for access to rehabilitation after TBI. Further studies of prospective design are warranted to corroborate these findings in other settings.
Supplemental Material
Supplementary_Files_Without_Changes – Supplemental material for Predictors of Access to Rehabilitation in the Year Following Traumatic Brain Injury: A European Prospective and Multicenter Study
Supplemental material, Supplementary_Files_Without_Changes for Predictors of Access to Rehabilitation in the Year Following Traumatic Brain Injury: A European Prospective and Multicenter Study by Louis Jacob, Mélanie Cogné, Olli Tenovuo, Cecilie Røe, Nada Andelic, Marek Majdan, Jukka Ranta, Peter Ylen, Helen Dawes and Philippe Azouvi in Neurorehabilitation and Neural Repair
Footnotes
Appendix
Author Contributions
Louis Jacob contributed to the design of the study, managed the literature searches, undertook the statistical analysis, wrote the first draft of the manuscript, and contributed to the correction of the manuscript. Mélanie Cogné, Olli Tenovuo, Cecilie Røe, Nada Andelic, Marek Majdan, Jukka Ranta, Peter Ylen, and Helen Dawes contributed to the design of the study and the correction of the manuscript. Philippe Azouvi contributed to the design of the study, managed the literature searches and contributed to the correction of the manuscript. All authors contributed to and have approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data used in preparation of this article were obtained in the context of CENTER-TBI, a large collaborative project with the support of the European Union 7th Framework program (EC Grant 602150). Additional funding was obtained from the Hannelore Kohl Stiftung (Germany), from OneMind (USA), and from Integra LifeSciences Corporation (USA). Data for the CENTER-TBI study were collected through the Quesgen e-CRF (Quesgen Systems Inc, USA), hosted on the INCF platform and extracted via the INCF Neurobot tool (INCF, Sweden). The funder had no role in the study design, collection, analysis, and interpretation of the data; writing of the report; and the decision to submit the article for publication.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.