
Abstract
Background. The effect of levodopa on recovery from aphasia is controversial. Objective. To determine whether levodopa enhances the effect of intensive computer-assisted therapy (CAT) of anomia in the postacute stage of aphasia. Methods. Double-blind multiple case study with intrasubject crossover design comparing the effect of levodopa (100 mg) versus placebo, each given for 2 weeks. Subjects. Twelve patients with onset of aphasia from 2 to 9 weeks after stroke or traumatic brain injury were compared on naming performance on items trained and not trained with CAT. Subjects were randomized to either levodopa or placebo first, separated by a 1-week washout, and then switched to the other drug intervention for the second 2-week CAT intervention. The subjects also received routine aphasia therapies during these periods. Results. All patients improved their naming performance for items trained by CAT in both periods (P = .001). No significant difference was found between the placebo and levodopa phases. Conclusion. Administration of levodopa for 2 weeks during the postacute stage of aphasia did not augment the positive effects of subacute intensive language treatment with CAT for a spoken naming task.
Introduction
Demonstration of benefit of aphasia treatment in the acute and postacute stages is difficult to separate from spontaneous recovery; in addition, it depends on the selection of the outcome measure. Speech therapy is a generally accepted treatment modality. 1,2 Treatment intensity seems to be an important predictor of outcome. 3 One way of increasing treatment intensity is computer-assisted therapy (CAT) of aphasia. CAT allows increasing the number of treated items and repetitions per item. CAT has proven its efficacy as a complement to traditional treatments of aphasia. 4,5
Pharmacological treatment can improve recovery after a cerebral lesion. Studies have assessed substances such as amphetamine 6,7 or drugs acting on the dopaminergic system (such as levodopa 8 and bromocriptine 9-12 ), piracetam, 13,14 and substances influencing GABAergic, serotoninergic, and cholinergic systems. 15,16 Levodopa is given orally and then metabolized in the brain to dopamine (95%) and norepinephrine (5%). 8 Decarboxylase inhibitor, which does not cross the blood–brain barrier, blocks periphery metabolism and avoids systemic effects.
Synapses are modifiable, and changes in synaptic strength (long-term potentiation and long-term depression) are a putative mechanism underlying plasticity. 17 Synaptic strength is modulated by dopaminergic input, 18 an observation that may explain why the dopamine system is important for motor learning. Levodopa shortened the training time required to form motor memory in young healthy volunteers and restored the ability to form a motor memory in elderly subjects to a level similar to that observed in younger subjects. 19 Compared with placebo, levodopa also significantly improved procedural motor learning in patients with chronic stroke. 20 Levodopa 100 mg once a day for 3 weeks associated with physiotherapy was significantly better than placebo in reducing motor deficit in stroke patients. 21
In healthy subjects, levodopa 100 mg for 5 days accelerated word learning. 22 Case reports suggested that dopaminergic drugs may also have positive effects on recovery from aphasia. 9 In group studies, positive effects of bromocriptine were reported in nonfluent chronic aphasic patients with significant improvement on word retrieval, 12 in the lexical index, verbal fluency, and pause reduction 23 or in verbal latency and reading comprehension. 11 Levodopa 100 mg from Monday to Friday for 3 weeks, 30 minutes before speech therapy, improved language abilities in patients with motor aphasia in a subset of language tasks (verbal fluency and repetition) assessed on an aphasia screening battery. 8 Other studies found no effect of a dopamine receptor agonist bromocriptine started at 5 mg and increased to 15 mg daily for a period of 8 weeks 10 or started at 3.75 mg and increased to 60 mg daily 24 for a period of 7 weeks in patients who had nonfluent aphasia.
The goal of the present study was to evaluate the effects of levodopa on recovery from anomia in patients with aphasia from stroke or traumatic brain injury, within 2 to 9 weeks after onset, who were receiving CAT in addition to individual traditional therapy sessions. To avoid the bias of intersubject variability, we use intrasubject comparison across 2 treatment phases. Patients underwent 2 periods of anomia therapy with CAT, each performed with a different word list. Each period was associated with the administration of either levodopa 100 mg or placebo.
Methods
General Procedures
We performed a multiple case study with double-blind placebo–levodopa intrasubject crossover design. Evaluations at baseline and after each treatment period were performed with a naming battery already used in previous studies. 5 The order of administration of levodopa and placebo was randomized across subjects.
Subjects
Patients hospitalized in the Division of Neurorehabilitation of the University Hospital of Geneva, who suffered from aphasia after stroke or traumatic brain injury, were selected. Inclusion criteria were presence of anomia with normal to mildly impaired comprehension. Exclusion criteria were executive or apraxic dysfunctions that might interfere with the handling of keyboard or mouse, stereotypies or perseverations dominating the aphasic symptoms, or Parkinson’s syndrome requiring dopaminergic treatment. Patients were informed about the study procedure and gave written consent. The study was approved by the local ethics committee and the Swiss agency for therapeutic products.
Seventeen subjects met the inclusion criteria and were recruited to participate in the study. Five subjects did not complete the study or were discharged for protocol deviation (inadequate CAT or pharmacological treatment) or insufficient level of French. Demographic data and aphasia subtype for the 12 patients included in the study are given in Table 1.
Subjects’ Demographic and Clinical Data
Specific Procedures
Patients received the standard clinical treatment (4-5 hours of speech therapy per week) and additional daily CAT sessions (Monday to Friday) during the study period. As far as possible in the weekly planning, the patients underwent the CAT sessions in the morning and the traditional therapy session in the afternoon. The traditional therapy avoided targeting anomia and especially the items used in CAT.
CAT and assessment material consisted of 2 sets of 72 words (frequent items for severe anomia) or 2 sets of 50 words (overall less frequent words for milder anomia) and their associated black-and-white line drawings. The items in the 2 sets were matched on name agreement, lexical frequency, age at which each word was acquired, length, and syllabic structure. Healthy subjects performed above 95% correct on all lists.
During CAT periods, the patient had to write (by using the keyboard) the word corresponding to a picture that appeared on the screen. Two help buttons were available: one provided the pronounced word and the other provided help on each letter of the word. 5 Oral naming of all stimulus items was scored at baseline and at posttreatment assessments. Only first attempt correct response in a delay of 4 seconds was scored as correct. For each patient, the study procedure was as follows:
t1: Baseline assessment
t2: Treatment phase 1: 2 weeks of CAT on one list + levodopa or placebo
t3: Posttreatment assessment 1
t3´: 1 week washout period (only standard clinical therapy but no CAT, no levodopa, no placebo)
t4: Treatment phase 2: 2 weeks of CAT on a second list + levodopa or placebo
t5: Posttreatment assessment 2
The order of the 2 lists was counterbalanced, and the order of pharmacotherapy or placebo was randomized across patients. Pharmacotherapy consisted of levodopa 100 mg with decarboxylase inhibitor benserazide 25 mg administered in the morning 1 hour after breakfast, taken 5 of 7 days, for 2 weeks corresponding to 1 of the 2 CAT treatment periods. During the other period, placebo was administered following the same procedure. Neither the study participants nor the researchers were aware about which substance (levodopa with benserazide or placebo) was administrated in the 2 treatment phases. Randomization, production of the placebo, labels, and lot numbers were managed by the hospital’s pharmacy. Placebo and levodopa pills had the same external appearance.
Results
At baseline, naming accuracy was equivalent across the 2 lists (mean accuracy, respectively, 41% and 43%; paired t test: t(11) = 1.38, P = .19). Changes (delta or differences) in naming accuracy on each list between 2 consecutive assessment periods are shown in Figure 1. At the end of the CAT treatment period there was a significant increase in performance (F(1, 11) = 48.98, P < .0001) but no interaction with the pharmacotherapy condition (F(1, 11) < 1). Repeated-measures analysis of variance carried out on gains (difference on performance) on each list after each treatment phase confirmed an effect of CAT for treated items (interaction between list and phase: F(1, 10) = 9.6, P < .02) but no interaction with the pharmacological phase (F < 1). There was a trend for higher gains during the first treatment phase in all patients (simple effect of phase: F(1, 10) = 4.02, P = .07).
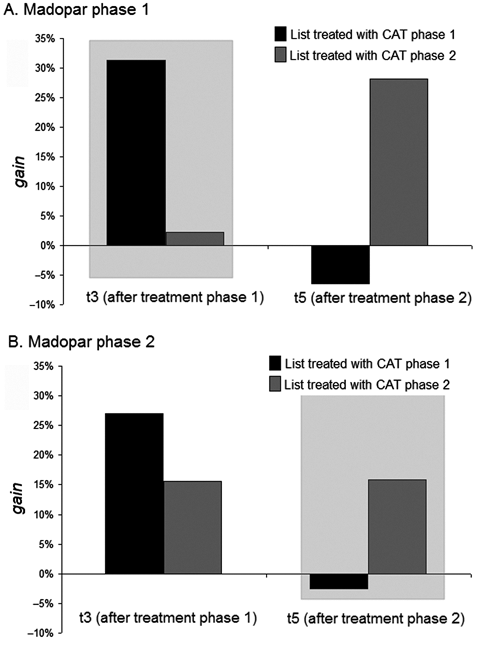
(A) Percentage of increase of correctly named items (gain) on list treated with computer-assisted therapy (CAT) in phase 1 (black bars) and on list treated with CAT in phase 2 (gray bars) when levodopa and benserazide is given in phase 1. (B) Percentage of increase of correctly named items (gain) on list treated with CAT in phase 1 (black bars) and on list treated with CAT in phase 2 (gray bars) when levodopa and benserazide is given in phase 2. t3, Posttreatment phase 1 assessment; t5, Posttreatment phase 2 assessment
Individual results are shown in Table 2. McNemar’s χ2 were calculated on the naming scores on each list for comparisons across 2 consecutive assessment sessions. All but 1 patient displayed significant improvement on the treated list after the first CAT treatment phase regardless of the pharmacological treatment phase. Five of 6 patients who did not receive levodopa during the second CAT treatment phase also improved significantly after this phase, and only 3 patients with pharmacotherapy in phase 2 displayed significant improvements during this phase. Interestingly, these 3 patients (P2, P4, and P5) entered the study at very early postonset (during the first month postonset). However, no conclusion can be drawn on time postonset effects, since patients P1, P6, and P7, who also improved during the second levodopa therapy phase, entered the study in a later postonset stage.
In sum, the individual results replicate the pattern observed in the group analysis, with most patients displaying a CAT treatment effect regardless of the pharmaco-therapy period.
Correct Naming (Percentage) at Baseline and After Each Therapy Phase on Each List and for the 12 Patients
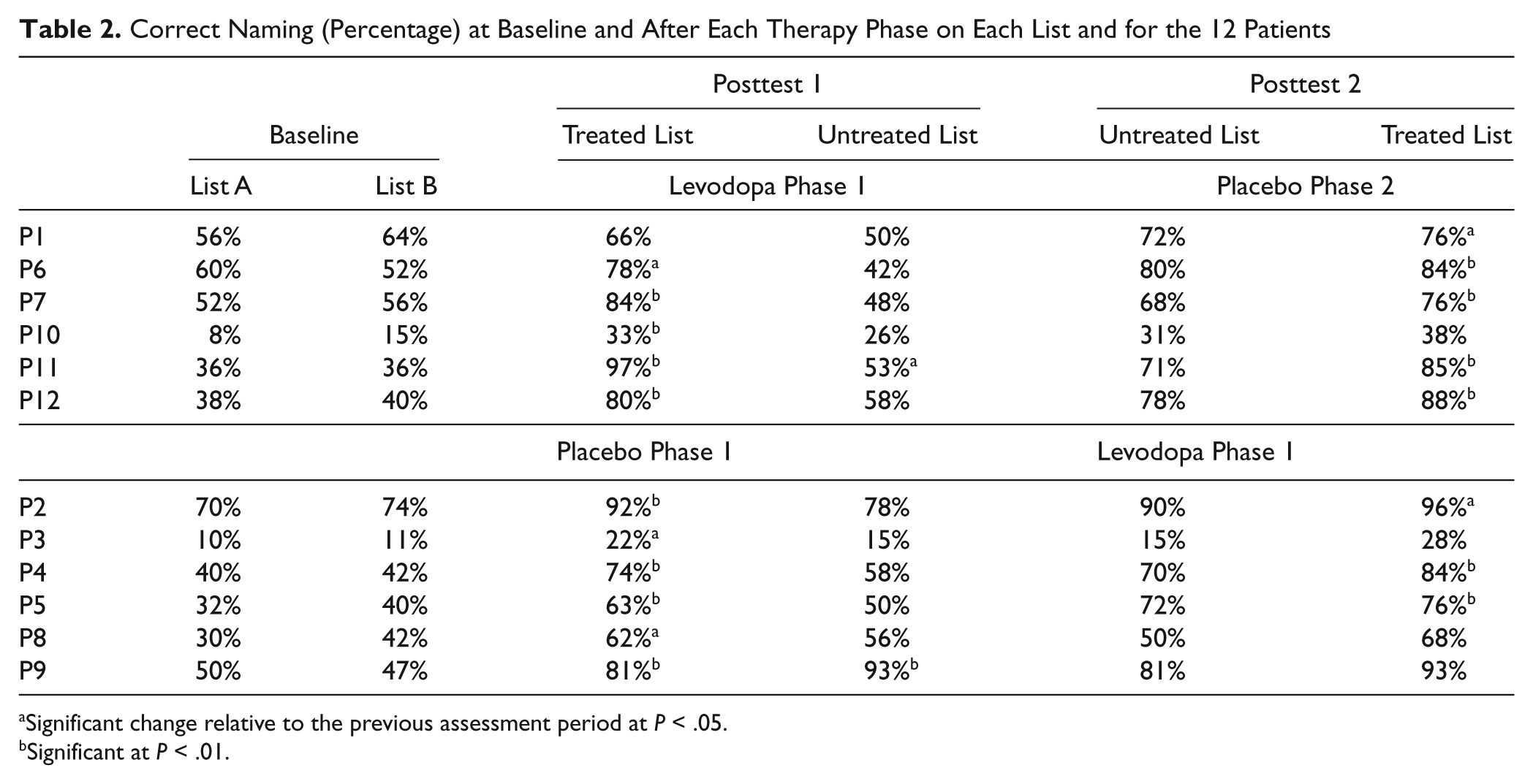
Significant change relative to the previous assessment period at P < .05.
Significant at P < .01.
Discussion
Our main finding is that although all patients significantly improved their naming performance for items treated with the CAT, administration of levodopa did not modulate the amount of improvement. These results converge with previous studies failing to show an effect of dopaminergic pharmacotherapy on recovery from aphasia 10,24 and contradict studies showing positive effects of pharmacotherapy added to language treatment. 8,11,12,23 Several factors may account for these differences across studies.
First, the type of aphasia differed across studies. The case report by Albert et al 9 and 3 studies with positive outcome included only patients with nonfluent aphasia. 11,12,23 Seniów et al 8 included patients irrespective of type of aphasia, but a significant effect of levodopa was observed only in patients with a lesion in frontal language areas. In the present study, only 4 patients had lesions involving the frontal lobe and only 2 of them had a circumscribed frontal lesion. Second, CAT sessions assure homogeneous treatment across patients and phases whereas in previous studies intensity and content of speech therapy was often underspecified and hardly comparable and could have introduced a bias. Third, the lack of an effect of levodopa in the present study might be due also to a ceiling effect caused by the fact that patients receiving intensive speech treatment might already have reached their maximal recovery potential. Fourth, the outcome measure in the present study was limited to spoken naming. Effects of pharmacotherapy were reported on word retrieval, 12 but not all language tasks and modalities have been modulated by pharmacotherapy in the same way. 8,11,23 Finally, the timing of CAT in relation to pharmacotherapy might be critical. Although the same doses were administered as those in the study by Seniów et al, 8 (100 mg), patients received the treatment after breakfast; given that the maximal blood level is achieved in 60 minutes and that the half-life is 1.5 hours, it is possible that its effect was lost in some cases, especially when CAT therapy was done in the afternoon. In the present study, 70% of the CAT treatments were carried out in the morning (30-180 minutes after levodopa/placebo) and 30% in the afternoon. It is therefore possible that the effect of levodopa has probably been poor or lost in 30% of the treatment sessions and this might be a confounding bias in our study.
In summary, the present study points to the complexity of dopaminergic treatment for aphasia in the postacute stage. In our results, levodopa does not modulate recovery when coupled with intensive treatment for anomia in the postacute phase. However, these results do not rule out that dopaminergic treatment, given 30 to 90 minutes prior to therapy, may be effective in chronic aphasic patients with an anterior lesion or that another substance might be more effective to enhance recovery from aphasia. 14,16 The type of substance, dose, time since brain injury, and the type and intensity of therapy and timing between drug administration and therapy are important factors that need more systematic exploration.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.