
Abstract
Background. After a severe traumatic brain injury (TBI), some patients are discharged home without rehabilitation, although rehabilitation is assumed to improve outcome. Objective. To assess factors that predict referral to rehabilitation following acute care. This study is part of a larger inception cohort study assessing the care network in the Parisian area (France). Methods. Between July 2005 and April 2007, 504 adults with severe TBI (Glasgow Coma Scale score ≤8) were prospectively recruited by mobile emergency services. This study included 254 acute care survivors (80% male, median age 32 years). Data regarding demographics, injury severity, and acute care pathway were collected. The first analysis compared patients referred to a rehabilitation facility with patients discharged to a living place. The second analysis compared patients referred to a specialized neurorehabilitation (NR) facility with patients referred to nonspecialized rehabilitation. Univariate and multivariate statistics were computed. Results. In all, 162 patients (64%) were referred to rehabilitation, 115 (45%) of which were referred to NR and 47 (19%) to nonspecialized rehabilitation. The following factors were significantly predictive of nonreferral to rehabilitation: living alone, a lower income professional category, pretraumatic alcohol abuse, lower TBI severity, and transfer through a nonspecialized medical ward before discharge. Patients referred to specialized NR were significantly younger and from a higher income professional category. Conclusions. These results raise concern regarding care pathways because many patients were discharged to living places, probably without adequate assessment and management of rehabilitation needs. Injury severity and social characteristics influenced discharge destination.
Keywords
Introduction
Traumatic brain injury (TBI) is a major public health issue. In the United States, 5.3 million victims of TBI are left with persistent symptoms, and many require help for daily living activities. 1 Severe TBI, defined by a Glasgow Coma Scale (GCS) 2 score of 8 or less before admission to hospital, is strongly related to death, disability, and poor life satisfaction. 3 In France, 60% of severe TBI patients suffer from long-term disability, and 14% remain severely disabled. 4
Studies suggest that specialized rehabilitation benefits outcome of severe TBI5-8 and that cognitive rehabilitation enables better socioprofessional participation and quality of life. 9 Moreover, rehabilitation given in a multidisciplinary neurorehabilitation (NR) facility has been found to be more effective than rehabilitation in a nonspecialized facility 10 because of the effectiveness of cognitive evaluation and training. 9 A National Institutes of Health consensus panel 11 as well as French health authorities 12 recommend that all severe TBI patients receive specialized NR after acute care.
Few studies have reported information regarding access to inpatient rehabilitation for TBI patients. Most have shown that many patients did not receive any postacute rehabilitation13-16—as many as a quarter of severe TBI patients. 13 Moreover, only 16% of patients hospitalized for TBI of mixed severity were referred for specialized NR. 17 Other usual pathways of care included discharge home with or without outpatient rehabilitation, discharge to a nonspecialized facility, or discharge to a long-term care center. 18 Quantitative studies found several significant predictors of referral to rehabilitation: severity of TBI or associated trauma,13,16,19,20 age,13,16,19,20 marital status, 19 employment status,13,16 ethnicity, 13 length of stay in acute care, 20 and the early involvement of a physiatrist. 19 Limitations of these studies were that they included various levels of severity of TBI, and their methodology was retrospective. Referral for postacute care after TBI has not been addressed in a homogeneous, prospective cohort of severe TBI patients, who may benefit most from specialized NR services.
Our study is part of a larger regional prospective inception cohort study of severe TBI patients in the Parisian area (France). The main objectives were to assess the predictive factors of referral to rehabilitation versus discharge to a home residence or long-term care facility and to assess factors that predict referral to a specialized NR center versus a nonspecialized center.
Methods
The Paris Severe Traumatic Brain Injury study (PariS-TBI) was carried out from 2005 to 2007 in Paris and the surrounding suburbs (12000 km2 and 11.6 million inhabitants 21 ). In this area, clinical pathways are managed as following: mobile emergency services deliver medical care on site and during patient transportation toward the intensive care unit (ICU). There are 6 level I trauma centers in Paris. However, not all severe TBI patients are referred to one of these centers because 20 different hospitals can be involved in the primary admission of patients. ICUs can discharge patients home, to a rehabilitation unit, or to various surgical or medical wards according to clinical presentation or to availability of acute care beds. Most of the 47 rehabilitation wards involved in the study are not on site but in separate hospitals. Referral to rehabilitation depends both on the initiative of acute care practitioners to search for a rehabilitation center and on the ultimate decision by rehabilitation practitioners to admit—or not—the patient in their units.
Study Design
The objectives of the PariS-TBI study were to provide data regarding care network and outcome for severe TBI patients from the acute stage to 1 year after the accident. Patients were included by all mobile emergency services of the area over a 22-month period. Criteria for inclusion were patients aged 15 years or older with severe TBI (lowest GCS score before hospital admission, assessed in the absence of intubation or sedation and in the absence of other causes of coma, of 8 or less). Data from ICUs to final discharge were collected prospectively in all participating centers. Detailed data on acute care and predictive factors of early outcome and of 1-year outcome will be presented separately.
Patients
A total of 504 patients were prospectively included in the PariS-TBI cohort from July 2005 to April 2007. Brain-injured patients were mainly men (77%), and median age was 39 years: 34% were younger than 30 years, 24% were between 30 and 45 years, 21% were between 45 and 60 years, and 22% were 60 years or older. The main causes of injury were road traffic accidents (53% of patients) and falls (35%). Median delay between injury and arrival at hospital was 110 minutes (range, 37-1308 minutes). The prehospitalization GCS score was 4 or lower for 42%, 5 or 6 for 30%, and 7 or higher for 28%. The mortality rate during acute care was 49%.
At the end of acute care, there were 257 survivors who were all included in the present study; 3 patients who were transferred abroad before discharge were excluded. The majority (80%) of this sample of 254 patients was male, and the median age was 31.7 years (range, 15-98 years).
Preinjury data
The data were collected at the acute stage from information provided by relatives. Professional level was defined according to the French National Institute for Statistics and Economic Studies 22 that includes 8 categories: higher/lower managers, white/blue collar workers, self-employed, nonactive, retired, and students. Home environment was assessed as a dichotomous variable (living alone vs living with 1 or more relatives), as were pretrauma alcohol or drug abuse and psychiatric or neurological illness (yes/no). Comorbid factors were assessed using the American Society of Anesthesiologists score 23 and dichotomized as normal healthy versus presence of mild or severe systemic disease.
Injury severity data
Brain injury severity was assessed using the last GCS score evaluated before arrival at the hospital (which could differ from the GCS score used as an inclusion criterion, explaining the fact that for 2 patients the last GCS score before admission was 15). The GCS score used as a predictive variable was evaluated in accordance to guidelines. 24 For most patients, this GCS evaluation was realized without any previous sedation, whereas for 33 patients, this GCS score was assessed after intubation and sedation, but sedation was transitorily stopped before assessment. Other measures of injury severity were the following: presence of nonreactive mydriasis on admission, Marshall score from initial computed tomography or magnetic resonance imaging 25 (using a unique category for evacuated or nonevacuated mass lesions), coma duration (end of coma was defined by first spontaneous opening of eyes), and time to follow commands. Presence of concurrent orthopedic injury was recorded (yes/no).
Assessment at discharge from acute care units
Intensive care physicians assessed global outcome at discharge from intensive care using the Glasgow Outcome Scale (GOS), 26 a 4-class scale ranging from vegetative state (score of 2) to good recovery (score of 5). Patients’ baseline characteristics are shown in the first columns of Tables 1 and 2.
Pre-TBI Determinants of Place of Discharge: Rehabilitation Versus Discharge to a Living Place
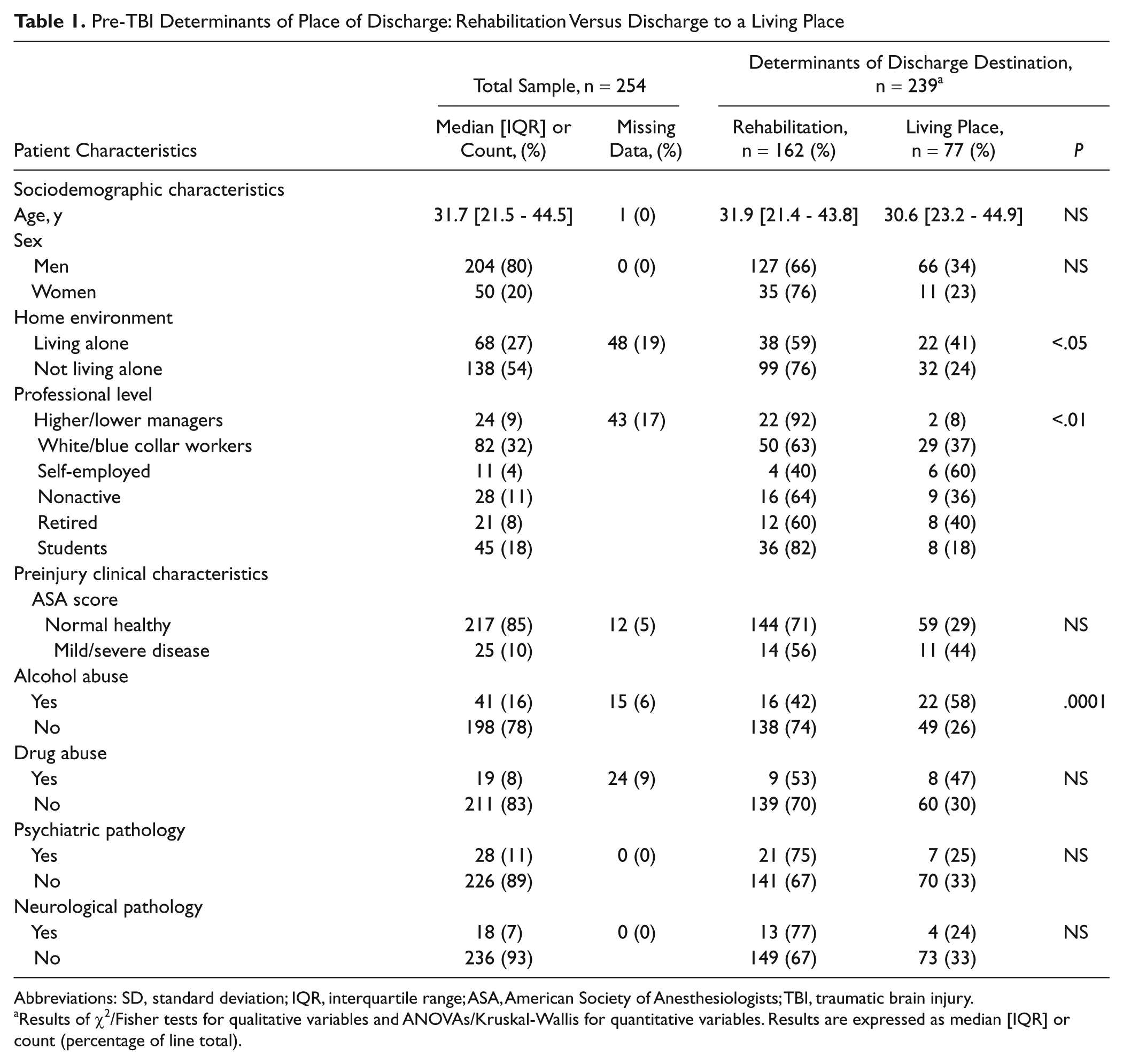
Abbreviations: SD, standard deviation; IQR, interquartile range; ASA, American Society of Anesthesiologists; TBI, traumatic brain injury.
Results of χ2/Fisher tests for qualitative variables and ANOVAs/Kruskal-Wallis for quantitative variables. Results are expressed as median [IQR] or count (percentage of line total).
Post-TBI Determinants of Place of Discharge: Rehabilitation Versus Discharge to a Living Place
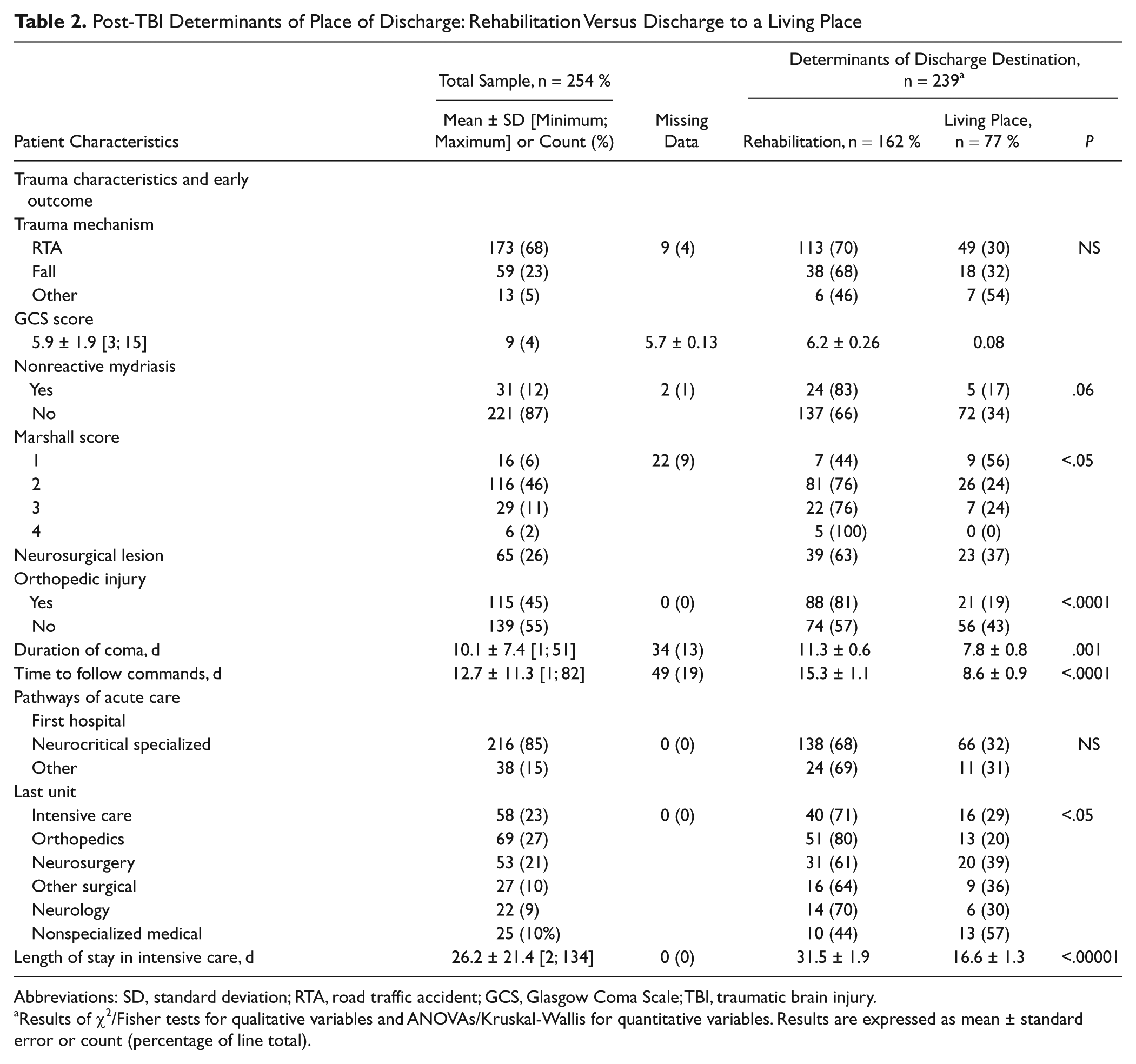
Abbreviations: SD, standard deviation; RTA, road traffic accident; GCS, Glasgow Coma Scale; TBI, traumatic brain injury.
Results of χ2/Fisher tests for qualitative variables and ANOVAs/Kruskal-Wallis for quantitative variables. Results are expressed as mean ± standard error or count (percentage of line total).
Care Pathway
In our study, acute care units refers to ICUs and all subsequent surgical or medical wards (excluding rehabilitation facilities). To describe the care pathway, several factors were recorded: the type of the first hospital, classified as “specialized neurocritical care center” (meaning teaching hospital, with a trauma care level I structure) versus “other”; the length of stay in intensive care; and the type of final acute care unit before discharge (intensive care, orthopedics, neurosurgery, other surgical ward, neurology, and nonspecialized medical ward). This last assessment was used to specify the specialty of the acute care provider who decided the place of discharge.
At the end of acute care, patients who were discharged to a permanent living place (home or long-term living facility) were classified as “discharged to a living place.” Most of them presumably did not receive adequate home service/rehabilitation (meaning either no rehabilitation or unspecific, uncoordinated ambulatory care).
Patients directly referred to a rehabilitation center or patients admitted to inpatient rehabilitation after a transitory stay home were classified as “discharged to rehabilitation.” Rehabilitation facilities were defined as specialized NR facilities if they had a neuropsychologist trained to perform cognitive evaluation and training and if TBI patients were part of their usual clinical practice. These facilities usually admitted stroke or TBI patients, without segregating patients by the diagnosis of TBI. Other rehabilitation facilities were classified as “nonspecialized rehabilitation.”
Statistical Analysis
Demographic and injury characteristics were described by means ± standard deviations or medians (interquartile range) for continuous variables and counts and percentages for categorical variables. To assess for potential bias, patients lost to follow-up (ie, patients for whom discharge destination was unknown) were compared with the rest of the sample with respect to all characteristics.
Patients in “discharge to rehabilitation” and “discharge to a living place” groups were compared using χ2 tests (or Fisher tests) for qualitative variables and analyses of variance (ANOVAS) (or Kruskal-Wallis) for quantitative variables. The α error was set at 5%. A predictive logistic model was then computed, using a stepwise hierarchical ascending strategy, with place of discharge (rehabilitation vs living place) as the binary dependent variable. The Akaike information criterion was used to compare the relative contribution of each successive step. Odds ratios (ORs) and adjusted ORs were computed with their 95% confidence intervals (CIs). Within the group of patients discharged to rehabilitation, the same strategy was used to compare patients admitted to a specialized NR facility with patients admitted to a nonspecialized facility. Statistical analyses were performed using R version 2.12.0 software.
Ethical Concerns
Patients and families were informed about the purpose of the PariS-TBI study before the data were recorded. According to French laws, the study was approved by the Consultative Committee for Treatment of Health Research Information, and written consent for participation was not necessary.
Results
Discharge destinations after acute care were as follows: 77 patients (30%) were directly discharged to a living place (71 home discharges and 6 discharges to living facilities), and 162 (64%) were admitted to a rehabilitation facility. In the rehabilitation group, 115 (45% of the whole sample) were referred to specialized NR centers and 47 (19%) to nonspecialized centers. Comparison of patients lost to follow-up (n = 15, 6% of the sample) with the remaining patients yielded no significant differences, except for the last unit of acute care. Patients discharged from intensive care or neurosurgery were rarely lost to follow-up (2% and 6%, respectively), whereas discharge destination was unknown for 19% of patients discharged from orthopedic wards and 22% of patients discharged from neurology wards.
Predictive Factors
Results of univariate tests comparing patients admitted to rehabilitation with patients discharged to a living place are summarized in Tables 1 and 2. Patients living alone had half the odds (OR = 0.5; CI95% = [0.2, 0.9]), and patients having premorbid alcohol consumption had an OR of 0.3 (CI95% = [0.1, 0.5]) of being admitted to rehabilitation. Managers and students were significantly more often referred to rehabilitation than white/blue collar workers and nonactive or retired patients. Most variables relating to injury severity were significantly associated with discharge destination. Patients with more severe brain injuries or with associated limb injuries were more likely to be admitted to a rehabilitation facility. Patients admitted to rehabilitation had stayed longer in intensive care than patients discharged home. Last acute care unit influenced discharge destination: only 44% of patients discharged from a nonspecialized medical ward were transferred to rehabilitation.
Finally, discharge destination was significantly related to GOS score at the end of intensive care (P < .00001; Figure 1). All patients in a vegetative state, 80% of patients with severe disability, 72% of patients with moderate disability, and 40% of patients with good recovery were referred to rehabilitation.
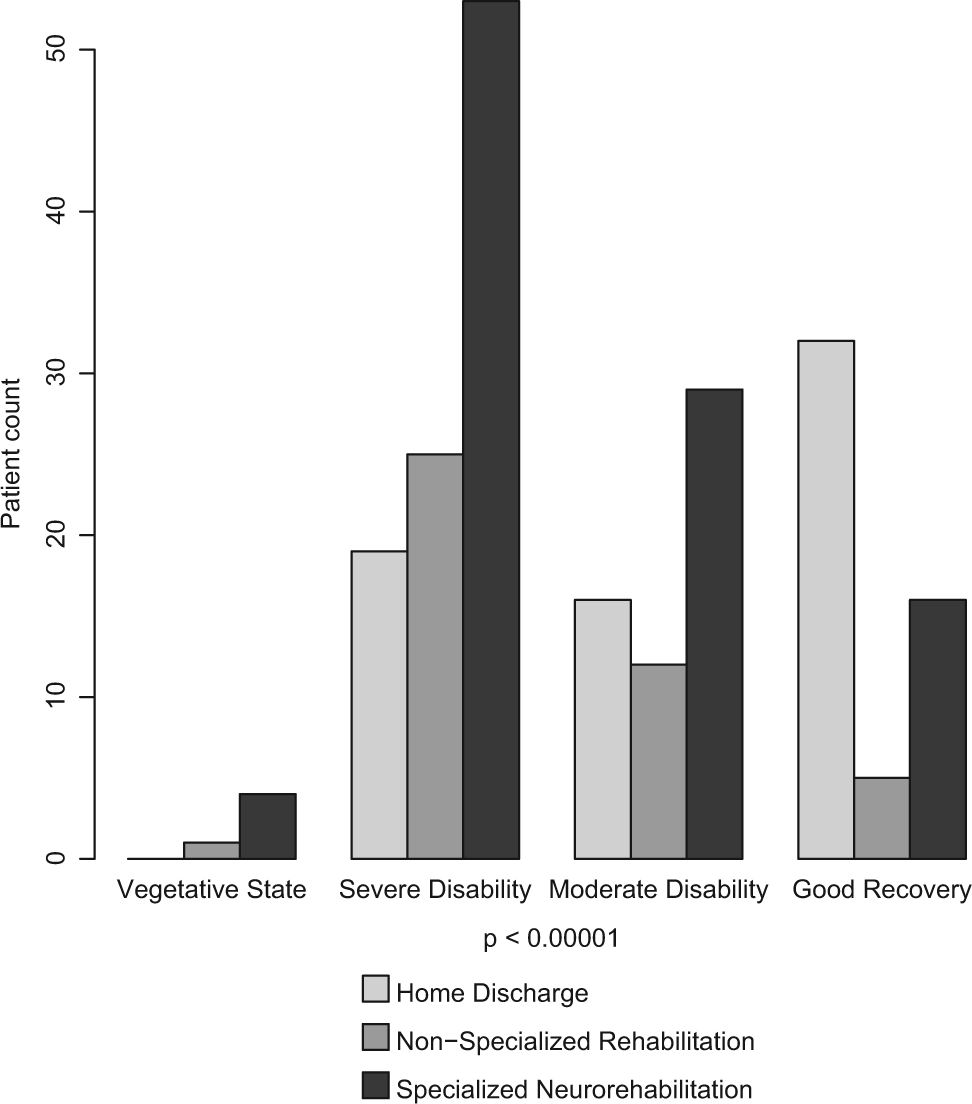
Early Glasgow Outcome Scale and postacute care discharge destination.
Results of Multivariate Analyses
To save degrees of freedom, explanatory variables that yielded significant results in univariate tests were introduced in the model based on their clinical relevance. Three hierarchical steps were used. The first step used TBI severity measures (GCS, time to follow commands, and GOS on discharge from intensive care). GCS was included in the model despite a lack of significance in univariate tests because this measure of severity is usually central in TBI management and outcome. Nonclinical variables (ie, sociodemographic characteristics) were subsequently added in the second step. The last step added last acute care unit, dichotomized as nonspecialized medical ward versus other units. Results of multivariate analyses for rehabilitation versus living place discharge are shown in Table 3. Multivariate analyses were computed on complete-case analysis, resulting in a 38% sample size reduction (n = 149). Each subsequent step had a better goodness of fit, as indicated by a better (lower) Akaike criterion, than the previous one. Among severity variables, GOS at discharge from intensive care had the highest predictive value in all 3 steps. Alcohol abuse had a significant independent predictive value in the second and third steps. Last unit of acute care added predictive information in the last step.
Results of the Logistic Regression Model: Rehabilitation Versus Discharge to a Living Place (n = 149) a
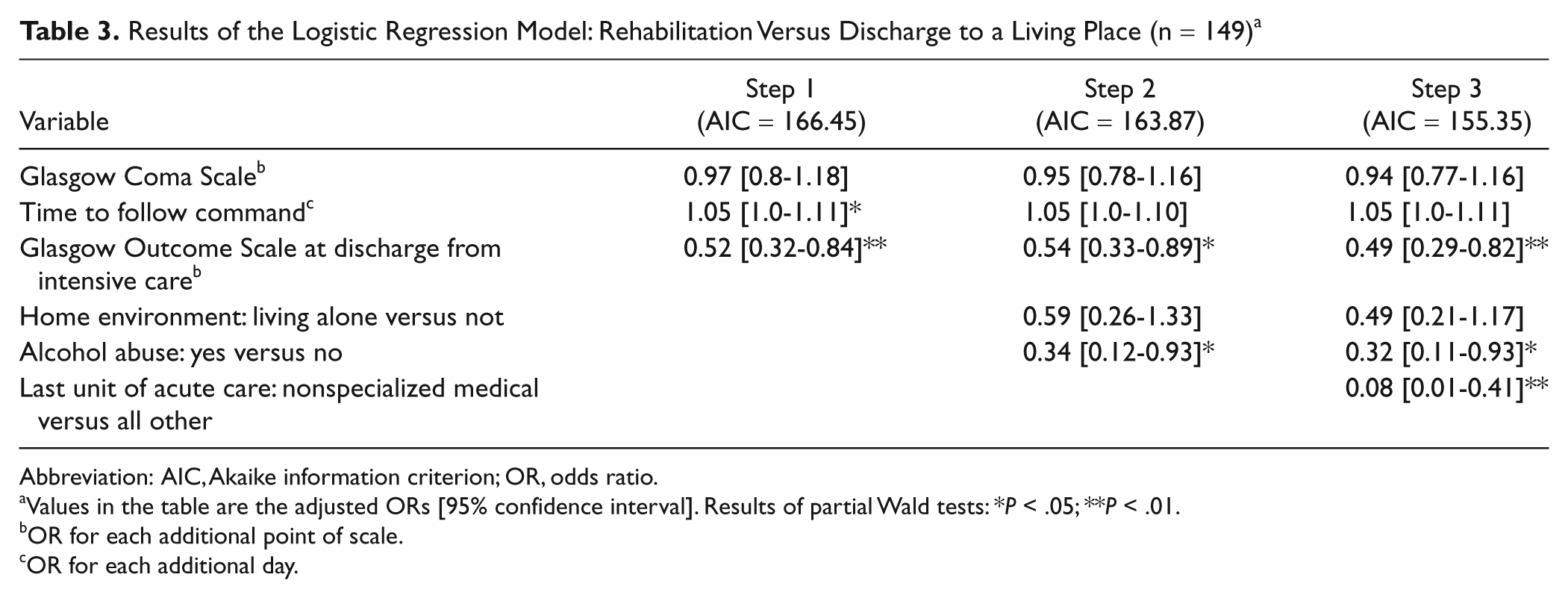
Abbreviation: AIC, Akaike information criterion; OR, odds ratio.
Values in the table are the adjusted ORs [95% confidence interval]. Results of partial Wald tests: *P < .05; **P < .01.
OR for each additional point of scale.
OR for each additional day.
Significant results of tests comparing patients transferred to a nonspecialized facility with patients transferred to a specialized NR facility are shown in Table 4. Patients admitted to specialized NR were significantly younger, had a less frequent past history of alcohol abuse (OR in the absence of alcohol abuse = 3.6; CI95% = [1.3, 10.5]), and were more often higher/lower managers.
Determinants of Type of Rehabilitation: Specialized Neurorehabilitation Versus Nonspecialized (n = 162) a
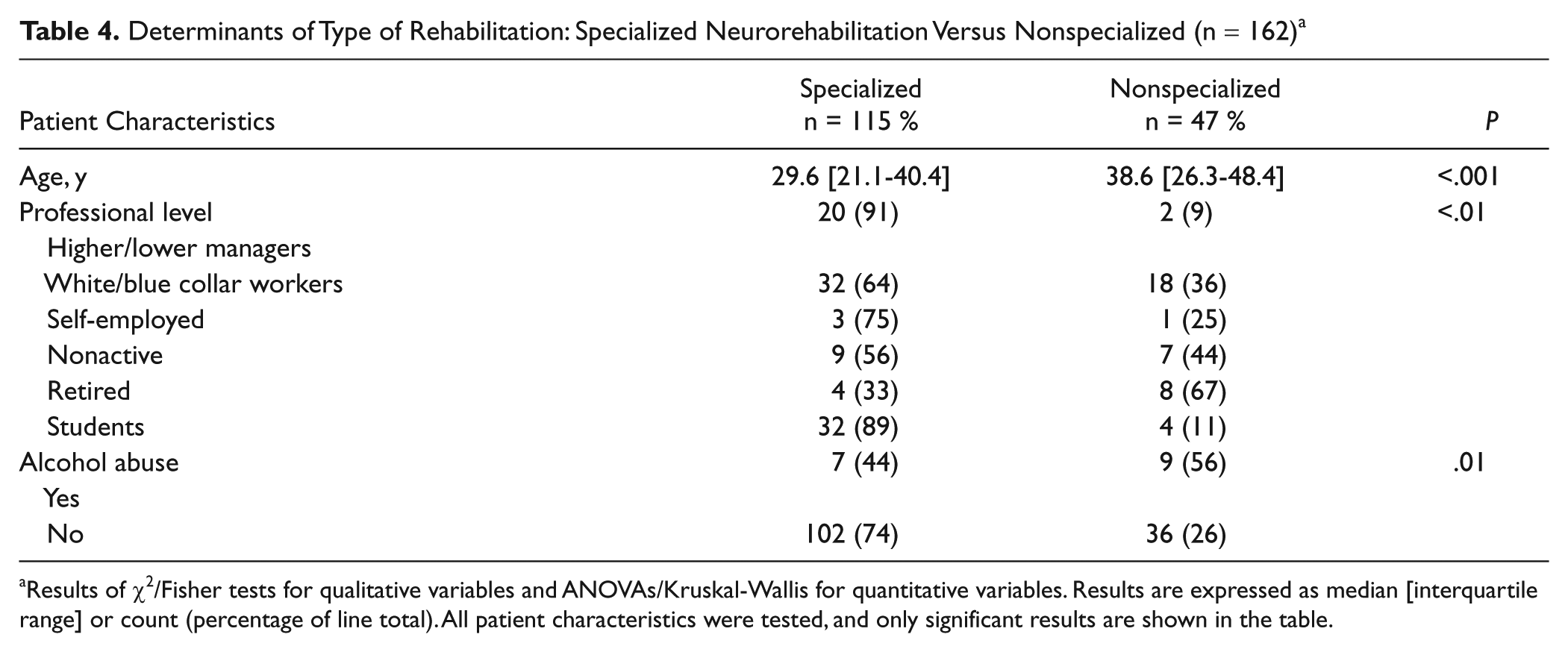
Results of χ2/Fisher tests for qualitative variables and ANOVAs/Kruskal-Wallis for quantitative variables. Results are expressed as median [interquartile range] or count (percentage of line total). All patient characteristics were tested, and only significant results are shown in the table.
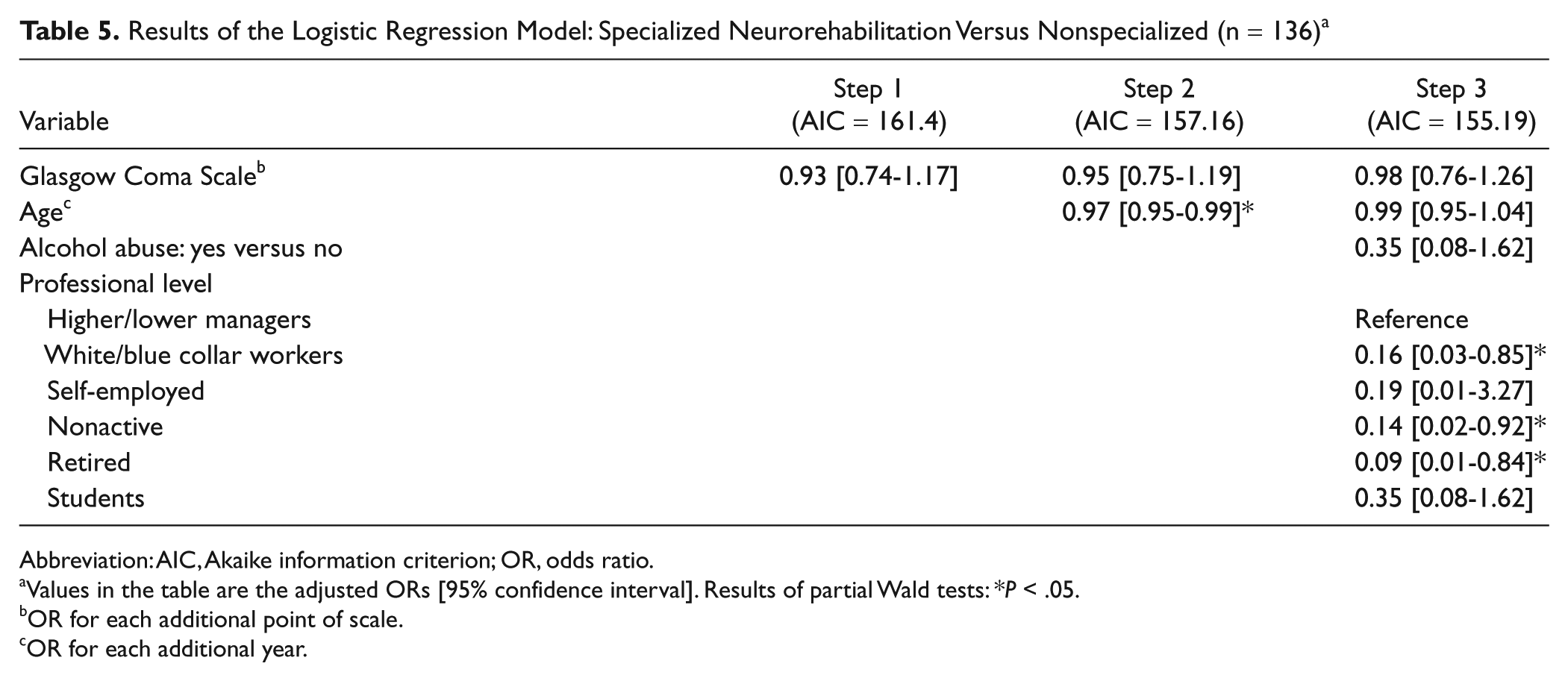
Stepwise hierarchical multivariate analysis was computed with TBI severity–related variables in the first step, age in the second step, and demographic variables in the last step. Regarding injury severity measures, only the GCS was introduced here because “time to follow command” resulted in an important sample size reduction and was not significant in univariate tests. In multivariate analyses (Table 5), sample size reduction was 16% (n = 136), and each subsequent step yielded a better (lower) Akaike criterion than the previous one. Age had an independent significant predictive value in the second step and professional category in the third.
Results of the Logistic Regression Model: Specialized Neurorehabilitation Versus Nonspecialized (n = 136) a
Abbreviation: AIC, Akaike information criterion; OR, odds ratio.
Values in the table are the adjusted ORs [95% confidence interval]. Results of partial Wald tests: *P < .05.
OR for each additional point of scale.
OR for each additional year.
Discussion
To our knowledge, this is the first study to address the determinants of postacute care referral to rehabilitation in a prospective clinical study of severe TBI patients. The major result was that in the Parisian area, nearly a third of patients were discharged without inpatient rehabilitation, and less than half benefited from specialized NR. These proportions confirm previous data on the subject 13 with a more robust methodology. Considering that specialized NR is recommended 11 after a severe TBI, this study raises concern regarding quality of care because secondary referral to neurological or vocational rehabilitation of patients who were initially discharged home is often problematic. 27 This dysfunction in postacute referral is further illustrated by the results in Figure 1. Nearly a quarter of patients presenting with severe or moderate disability at the end of intensive care, who were assumed to need rehabilitation, were discharged to a living place, presumably without adequate rehabilitation.
As noted, decisions about discharge in the Parisian setting rely on both acute care and rehabilitation practitioners. The main pressure in the acute care context is related to length of stay, whereas pressures on the rehabilitation setting lie as much in the length of stay as in the complexity of medical care and of social environment, which determine patients’ ability to return home after rehabilitation. French Health Care insurance relies on a unique payer system, which covers 99.6% of the population. 28 Emergency hospital admission is mandatory for patients with emergency life-threatening situations. Severe TBI gives subsequent access to complete coverage of related expenses, including rehabilitation. Nonlegal immigrants who have been living in France for more than 3 months can receive a state medical aid giving similar coverage in case of severe illnesses. Although no data could be collected on insurance type or citizenship in the present study, it is unlikely that decisions of referral to rehabilitation or not relied on financial or administrative considerations.
Predictors of Referral Decision: Clinical Variables
Comparisons between patients discharged to a living place and those discharged to rehabilitation highlighted several significant predictors of referral decision. Patients with a more severe brain injury were more often discharged to rehabilitation. The role of trauma severity on care pathways has been shown by previous studies on mixed-severity patients,13,16,19,20 but our study shows that this factor is central even among exclusively severe TBI patients. Variables related to initial severity showed a weaker link than variables related to early evolution and outcome. In multivariate analyses, the most powerful predictor was GOS score at discharge from intensive care. It could be that clinicians decided the place of referral mostly based on late examination of patients and that many patients with apparently good recovery were directly discharged to living places. This strategy could underestimate cognitive deficiencies, which require extensive neuropsychological evaluation and follow-up. These notions should be stressed in the training of acute care practitioners.
Concurrent orthopedic injuries gave 3 times the odds for referral to rehabilitation, which highlights the fact that patients at risk of inadequate discharge destination were those who had little apparent impairment at the end of the acute stage. It could also be assumed that patients with concurrent orthopedic injuries would be more often referred to nonspecialized facilities, but this assumption was not confirmed in the second set of analyses.
Predictors of Referral Decision: Nonclinical Variables
Injury severity was not the only predictor of discharge destination because an unfavorable social context (living alone, a lower income professional category, or a preinjury history of alcohol abuse) was also significantly associated with discharge to a living place. The effect of alcohol consumption on discharge destination was moreover independent of other variables in multivariate analyses. These results are new in the rehabilitation literature, which has mainly shown the role of social context on place of discharge through type of insurance16,29-31 or ethnicity.13,16,32 These results point out the existence of socioethical inequalities because to our knowledge, these factors do not influence the efficacy of NR, and no clinical justification exists for such selection criteria.
Factors Unrelated to Patients: The Context of Decision
Referral to rehabilitation was significantly associated with a longer stay in the ICU. This effect was partly a result of the higher initial severity of the TBI, but it could be explained, as other authors have suggested, 30 by the influence of the planned discharge arrangement on length of stay because of delays before obtaining an available bed in rehabilitation wards. A further interesting study would be to measure the number of excessive days spent in acute care and the proportion of inadequate discharges resulting from excessive waiting delays. Indeed, these delays not only affect costs and organization of acute care 33 but may also be a reason for inadequate discharge because practitioners must respond to the pressure of length of stay on acute beds in their discharge decisions. 18
Another finding was the key role of the last unit of acute care in predicting discharge destination, which was independent of other variables. This means that some patients followed an inadequate pathway after intensive care, ending in wards where practitioners were unaware of the necessity of rehabilitation and of the modalities of referral. The first place where ICU care providers discharge patients (usually acute care services) was thus part of the chain of decisions that eventually ended up in an inadequate discharge disposition. As studies on pathways of care during acute care for brain injury patients are scarce, awareness needs to be raised regarding the necessity and the modalities of better controlling these pathways.
Predictors of Rehabilitation Setting
Patients referred to specialized NR facilities were younger; were more frequently managers, rather than workers or nonactive; and had a less frequent past history of alcohol abuse. These last 2 characteristics were thus unfavorable both for discharge to rehabilitation (vs living place) and to specialized versus nonspecialized centers.
Interpretations of Discharge Decision Making
These results raise several questions regarding decision making in the allocation of rehabilitation resources. Although the ideal decision making process would rely solely on objective clinical data, the influence of nonclinical characteristics, particularly sociodemographic factors, has previously been described in various medical settings.34,35 In the rehabilitation setting, Hughes and Griffith 36 showed the role of the emotional impact of a patient’s personal story, and of the “deservedness” of rehabilitation. In stroke patients, 37 a major concern in admission selection in several different European contexts is the likelihood of the patient to be discharged home, which can be compromised by lack of support or sociological difficulties.
A qualitative model to help understand referral decisions in the context of TBI was proposed by Foster and Tilse. 20 These authors showed that, in addition to clinical factors, practitioners’ interpretations (regarding, for example, rate and extent of progress, recovery potential, safety and burden of care, potential for independence, and capacity to cope) emerged as the justifications for referral decisions. Our results, regarding the influence of age, alcohol abuse, living environment, and professional status, also suggest the strong influence of practitioners’ interpretations as justifications for referral decision. These findings highlight the subjective (or normative) aspects of referral, which reflects sociocultural, political, and economic factors, among others.
These dimensions of “deservedness” or “expected benefice” could presumably be applied to both acute care and rehabilitation practitioners because they are known to play a role in several different settings. 36 Furthermore, admission refusals from rehabilitation practitioners communicate acceptance criteria to referrers and influence later proposals of admission, thus homogenizing discharge decision making and its determinants in both settings. Finally, this study strengthens previous qualitative findings on the role of the health care context18,38 and of characteristics of the decision maker 38 in the decision process because factors such as length of stay and specialty of the final care provider played a significant role.
Strengths and Limitations
This study has several strengths. This large cohort was highly homogeneous because patients had all sustained a severe TBI over a limited period of time and were recruited and initially treated in the same geographic area. Recruitment was prospective, and the participation of all mobile emergency units of the area limited recruitment bias. The collection of a large amount of data on a prospective basis allowed multiple predictive factors to be evaluated. Possible limitations include the facts that the Parisian area and the organizational context of its health care have several specificities. Compared with smaller regions for medical care, clinical pathways around Paris are complex as a result of the multiplicity of centers. Care pathways for each patient involved up to 6 types of acute care wards before discharge. This variety contributes to the difficulties in managing clinical pathways and in training all the actors during acute care with regard to rehabilitation needs. Although some results from this study cannot be easily generalized to other health care environments, we assume that the relationship of patient characteristics to discharge destination was independent of the organizational context of the area. Most of these characteristics were related to discharge destination in other health care environments.13,14,18-20
Generalizability to other contexts of health care, particularly mixed-payer systems, is also not easy because the role of insurance type in similar studies 29 seems central. However, the present results suggest that social vulnerability influences medical decision making, even in a system that could a priori be assumed to minimize the effects of such factors by providing insurance coverage. Studies comparing different European health care systems37,39,40 reported that some sociodemographic factors were discriminatory for access to stroke rehabilitation in a manner similar to that in mixed-payer systems (such as Switzerland) rather than in single-payer systems (such as Italy or the United Kingdom). In the study by Chan et al, 29 ethnicity remained significant in multivariate models after adjustment for insurance type. Other systems may be less likely to discriminate against admission for rehabilitation. 41
Most patients discharged home did not receive home health care or rehabilitation services. However, we acknowledge that we did not obtain detailed information on this issue. Nevertheless, in a parallel ongoing study on late outcome of a subsample of the patients included in the present study, it appears that only a minority (less than 20%) of patients directly discharged home received some form of rehabilitation. Moreover, this rehabilitation, which was provided without any formal cognitive assessment, was presumably far below that recommended by current guidelines.
We used the GOS on ICU discharge, rather than on hospital discharge, for several reasons. Data on GOS at ICU discharge were more reliable, assessed by more specialized care providers, and had less missing data. Second, GOS at the time of hospital discharge could have been biased by differences in lengths of stay, which could be a result of difficulty in finding a proper discharge destination rather than clinical evolution.
Because of the size of the cohort and the complexity of data collection in multiple units and centers, a small proportion of patients (6%) were lost to follow-up, and missing data explained the sample size reductions in the multivariate models (38% for the first and 16% for the second). Comparison of patients lost to follow-up with the remainder of the cohort did not show significant differences, except for last unit of acute care, which was not surprising because information on place of discharge was easier to collect in some units than others.
Conclusion
Discharge destination after acute care for patients with severe TBI, although decided by care providers only, was often not optimal, given accepted standards. Clinical factors as well as sociodemographic characteristics may induce societal inequities in access to care.
Footnotes
Acknowledgements
We would like to thank Pr Pernot, Dr Dulou, Pr Tadie, Pr Truelle, Dr Carli, Dr Welschbillig, and Dr Zouaoui for their participation in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant of French Ministry of Health (Programme Hospitalier de Recherche Clinique 2004, AOM04084) and supported by AP-HP (Département de la Recherche Clinique et du Développement) and carried out with the support of Unité de Recherche Clinique Paris-Ouest.