
Abstract
Background. Clinical care and randomized trials of rehabilitation or surgery for symptomatic lumbar spinal stenosis with neurogenic claudication (LSS) are complicated by the lack of standard criteria for diagnosis and outcome measurement. Objective. To evaluate whether manual muscle testing (MMT) can detect transient lower-extremity weakness provoked by walking in patients with likely LSS. Methods. A total of 19 patients with symptoms and MRI findings suggestive of LSS were tested for a decline in lower-extremity strength, using the British Medical Council scale of MMT, by comparing strength at rest to a change in strength within 60 s of completing a 400-foot walk. They were retested after reclining supine for another 2 minutes. This examination was repeated following decompressive lumbar surgery. Results. All patients developed bilateral weakness in the distribution of their LSS, but always including the hip extensors and knee flexors, when tested immediately after the provocative walking test. Most patients were not aware of weakness or change in gait during the walking task. They recovered to baseline strength after resting supine. The patients did not improve with physical therapy. When examined within 8 weeks after decompressive laminectomy, no one developed weakness during the 400-foot walk, and daily lower-extremity pain had resolved. Conclusions. A careful repetitive motor examination can detect transient paraparesis in patients with definite LSS. This finding supports the diagnosis and the functional severity of LSS while providing an objective outcome measurement for physical therapy and surgical interventions that goes beyond symptoms of pain.
Introduction
Neurologists, physiatrists, and orthopedic and neurosurgeons are often asked to evaluate and manage patients with back pain and gait impairment. Symptomatic lumbar spinal stenosis that causes neurogenic claudication (LSS) has a prevalence >200 000 and has become the most frequent indication for spinal surgery in the United States in persons >65 years old. 1 For example, among 430 participants in a secondary analysis of community-dwelling older adults in the Boston RISE study, 176 (41%) reported symptoms of neurogenic claudication, and 54 of these (31%) also met the study’s imaging criteria for LSS. 2 Those with LSS had greater impairment of trunk endurance, leg strength (by a 1-repetition maximum contraction), and knee range of motion, but these were rather small absolute differences. By their self-reported measures, however, those with and without LSS declined similarly in mobility over 2 years. This study points to the difficulties in how best to diagnose and manage this common condition.
Clinical trials of nonsurgical interventions for the pain of LSS, such as physical therapies, medications, acupuncture, cognitive-behavioral training, bracing, and other techniques, compared with decompression surgery, have not clearly shown different outcomes, but the quality of most such studies was low per a Cochrane analysis. 3 In the intention-to-treat analysis for the Spine Patient Outcomes Research Trial that compared decompressive surgery to no specific care, including various physical therapies and medication, the former experienced less pain postoperatively, but physical functioning between groups did not differ. 4 However, the as-treated analysis, carried out in part because of the high number of nonadherent cross-overs to surgery during the trial, did detect self-reported improvement in activity that persisted for 2 years. Another randomized clinical trial of decompression versus formal physical therapy also had a lot of nonadherence to assignment but could not detect any differences in self-reported pain or physical functioning outcomes. 5 A trial that compared decompression with decompression plus fusion for LSS did reveal significant gains in association with surgery 6 but no differences between the 2 techniques. These trials beg the question of whether the diagnostic criteria for LSS and the most frequently used outcome measurement tools are as reliable and clinically meaningful as necessary for future research and for patient care decision making.
The diagnosis and subsequent management of LSS relies on clinical judgments that integrate symptoms, signs, imaging findings, and comorbid conditions. 1 Many causes of back and leg pain, sense of leg weakness, and gait impairment can masquerade as LSS and, based on many prospective studies, no single symptom or sign points to the diagnosis.7-11 For example, the sensitivity of individual symptoms and signs range from 0.4 to 0.8, with specificities from 0.6 to 0.9. 8 The most common symptoms include buttock or lower-extremity pain induced by standing and walking with the back in extension, but diminished by bending forward and ceasing upon sitting. Spinal magnetic resonance imaging (MRI) has a sensitivity of about 0.9 and specificity of about 0.7, if symptoms are typical and the midline anteroposterior central canal diameter is <10 mm. 1 Additional criteria to allow a more definitive diagnosis for patient care or for entry into a randomized clinical trial of a surgical, drug, or physical therapy would be welcome.1,8 Greater certainty about a large subgroup of patients who truly do have the syndrome could also better define the most clinically important primary outcomes to be expected of any intervention.
The European neurosurgeon Verbiest 12 provided one of the first thorough descriptions of LSS and neurogenic claudication. 7 He emphasized, along with the symptoms of pain with posture, that walking and standing led to reduced power in the legs. When seated or recumbent, he noted, the neurological examination generally revealed no weakness. A 1972 review also described leg weakness that was found only immediately after walking. No subsequent clinical trials or diagnostic consensus statement, of which there have been many, 7 has included testing strength at the time of neurogenic claudication symptoms. By performing this simple test routinely to help rule in LSS, we found evidence for a diagnostic tool that also provides a clinically relevant, objective outcome measurement.
Methods
This case series includes 19 patients (age 71 ± 8 years) referred to 1 neurorehabilitation clinic over 8 years, who were subsequently diagnosed with probable LSS and whose symptoms ceased following lumbar decompressive surgery, suggesting a correct diagnosis. As part of their physical examination when considering the diagnosis of LSS, we tested all patients before and immediately after walking 400 feet at their usual pace with the thoracolumbar spine comfortably extended.
The British Medical Council Scale of Manual Muscle Testing (MMT) that uses 5 grades of resistance was performed before, immediately after (completed within 1 minute), and 3 minutes after a 400-foot walk. Positioning for MMT of each leg was carried out as follows: (1) seated on the exam table—resistance to hip flexion starting from 90° toward 60°, proximal leg adduction, lower leg knee extension starting from 90° flexion toward 120° extension, ankle dorsiflexion and inversion, and large toe extension; (2) tested supine—hip flexion by whole leg elevation at 20° above the table, and plantar flexion; (3) tested prone—whole leg elevation off the table from the hip at 20° extension, and knee flexion at 45° from full extension. These positions enable better leverage for testing muscle groups that ought to be far stronger than the examiner’s arm and shoulder. The deep tendon reflexes at the knees and ankles and pinprick appreciation over the posterior and anterior legs were tested after each MMT. This test-walk-test-retest sequence was repeated again for confirmation of the findings at each visit.
Results
The frequency of relevant diagnostic findings is shown in Table 1. Symptoms had been present for 7 to 30 months and had usually worsened over recent months in terms of earlier onset of stereotyped deep achiness or burning/tingling of the anterior or posterior legs or buttocks after walking. Mobility had been reduced to progressively shorter walking distances as well. Three patients fell during a walk; one had 3 falls and now used a walker. Three patients described rather subtle neurogenic claudication pain that did not interfere with the distance walked, but like most of the other patients, they too gave examples of imbalance or a sense of leg weakness or fatigue while walking on level and especially uneven ground.
Primary Symptoms and Findings That Resolved With Decompressive Surgery in 19 Patients With the Diagnosis of Lumbar Spinal Stenosis With Neurogenic Claudication.
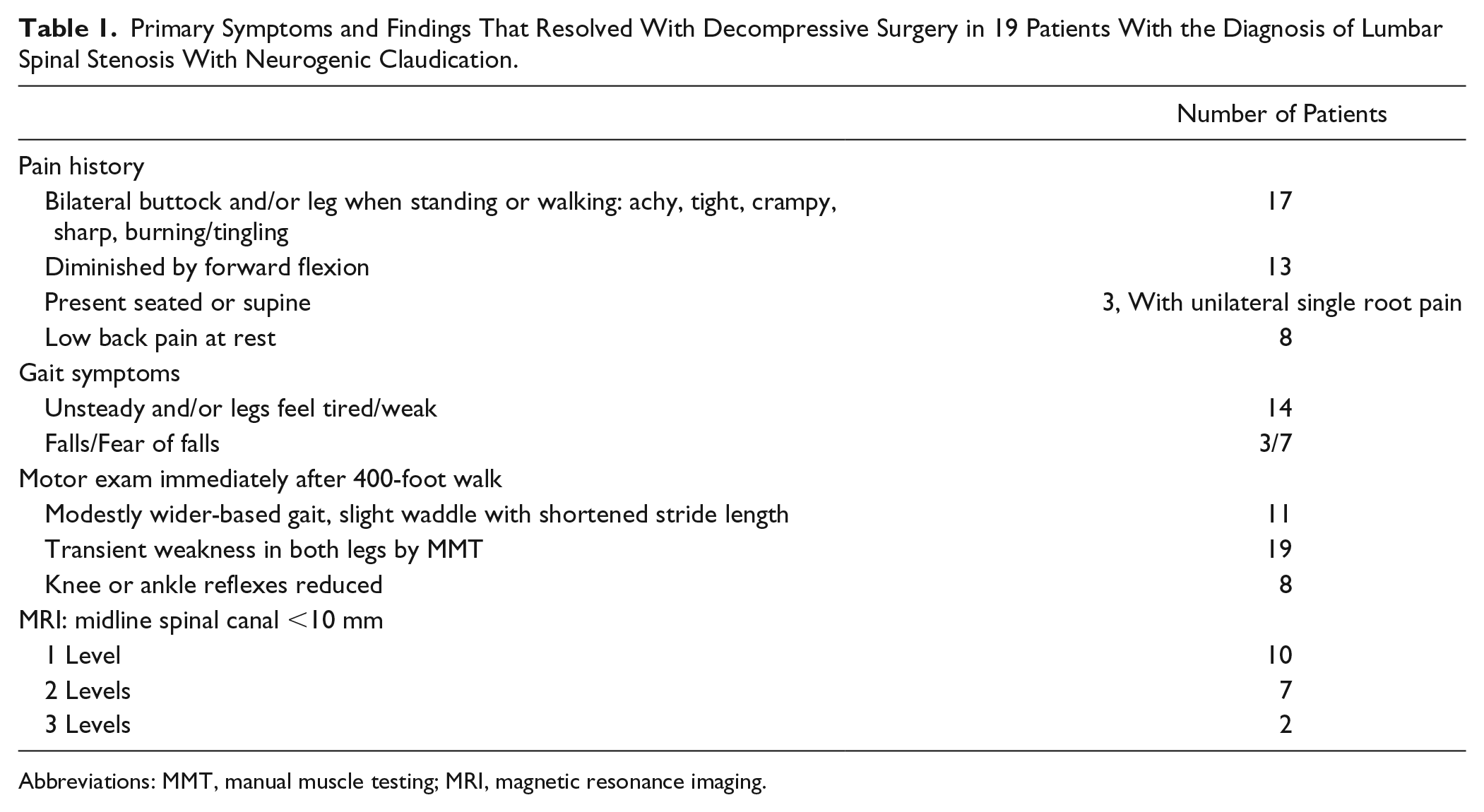
Abbreviations: MMT, manual muscle testing; MRI, magnetic resonance imaging.
At rest, 2 patients had likely unilateral L5 radicular pain with 4/5 strength in the extensor hallucis longus and hamstring muscles on that side. Another had mild weakness in a unilateral L4 distribution. All others had no weakness at rest. Strength after walking in bilateral lower-extremity groups, depending on the level of the disease, declined from 5/5 to 4 or 4-/5 (a modest to minimal effort to overcome resistance). In all patients, regardless of the level(s) of the LSS by MRI, the gluteal, hamstrings, and gastrocnemius muscles, tested while the patient was prone, became bilaterally affected. After a 2- to 3-minute supine rest, all patients fully recovered from the walking-induced weakness. The provocative test was then repeated, so that the patient could better appreciate the change in strength induced by walking and try to relate this to previously described symptoms. The MMT again uncovered paresis with rapid resolution. The effects of the provocative walk test were consistent at each of at least 3 subsequent visits. Of note, only 14 had onset of the typical severity of symptoms of radiating pain, imbalance, or sense of weakness during the 400-foot walk, which for these patients was a shorter distance than what typically led them to stop walking. Indeed, 11 were unaware of leg weakness during the first provocative walk, and only 5 of these appreciated a sense of weakness, unsteadiness, or onset of taking a shorter stride even during the second provocative walk. Merely standing in lumbar hyperextension for 2 minutes also induced transient weakness that was similar in distribution to what was found after the 400-foot walk in 6 patients.
In patients with a stenosis at L2-3, supine hip flexion (L3, iliopsoas) weakened during the provocative walk. With a stenosis at L3-4, the hip flexors tested when seated weakened along with ankle dorsiflexion and knee extension (L4, tibialis anterior and quadriceps), often with a decrease in the knee jerk. If only L4-5 or L5-S1 canal levels were narrow, the gluteal, hamstring, extensor hallucis, and the gastrocnemius groups transiently weakened. These groups also weakened with higher level canal stenosis. One or both ankle jerks variably diminished, mostly with a stenosis at L4-5 or L5-S1. Thus, the highest symptomatic level of a multilevel LSS, present in 9, could usually be surmised. A Romberg test was normal in all participants at rest, but a mild increase in truncal sway with eye closure was noted in several patients immediately after the 400-foot walk (this test was not performed routinely, however, postwalk). By observation, stride length tended to modestly shorten with a widened base by the end of the provocative walking test.
Treatments in our patients prior to surgery included physical therapy for 4 to 8 weeks for all, epidural injections at the presumed level of radicular pain in 9, nonsteroidal anti-inflammatory medications in all, and opiate analgesics in 2 when active. After much consideration based on a personal assessment of the impact of pain and weakness on their mobility-related quality of life, the 19 patients chose surgery; so they are the basis for this case series. Surgeries included a 1- or 2- or 3-level laminectomy as indicated by the symptoms, MRI canal features, and provocative walk MMT, plus a fusion in six. At surgery, a lateral recess stenosis seemed to be the site of nerve root entrapment for those patients who had radicular symptoms at rest. Weakness in that distribution had increased during the provocative walking test along with root levels below the anatomical location of the LSS.
By 6 to 8 weeks postsurgery when next examined, no patient used analgesics, and all walked for at least 20 consecutive minutes a day for exercise without limitation. The provocative walking test no longer induced weakness or pain. Four additional patients not included in Table 1 with similar histories and positive rest versus provocative walking tests have not had surgery for >1 year. They have accommodated to their pain by taking frequent seated rest stops and use caution when walking, especially on uneven ground, now that they are more aware of leg weakness that causes a decline in balance and gait.
Discussion
This selected case series of patients with LSS reveals the highly reproducible finding of transient bilateral leg paresis identified by a provocative walking test. The change was straightforward and binary—maximal resistance briefly declined to resistance that was easily overcome. Optimal positioning of the patient during the MMT enabled reproducibility of the examination. The distribution of weakness involved the cauda equina roots below the most upper level of spinal canal compromise based on MRI (see Table 1). As in this case series, symptoms of LSS tend to develop when the midline anteroposterior central canal diameter is <10 mm. 2 Along with other clinical and imaging features, the definitive diagnosis of LSS was based on the absence of pain symptoms and walking-induced weakness following decompressive surgery.
Whereas repeated MMT in relation to walking, which induces the stereotypical symptoms of each person’s LSS, seems like a reasonably obvious strategy, 13 a test of strength during symptoms has not found its way into routine care or clinical trials. The MMT must be carried out methodically and quickly to be revealing immediately after a 400-foot walk. Of note, the 400-foot walking distance used here was an arbitrary one, used in our neurorehabilitation clinic for practical reasons across patients with gait or balance complaints. If there is high suspicion for LSS, but pain with paresis is not induced by 400 feet, one might continue the walk until neurogenic claudication occurs.
In an era when technology and neuroimaging offer valuable insights, however, a standard test of strength may offer ground truth to help rule in or rule out this diagnosis, explain much of the disability induced by the disease, and serve as a measurable outcome. So far, this has not been attempted. In a literature review of LSS, the authors found that physical examination tests taken in isolation were not as useful as symptoms. 8 The examinations across studies were carried out at rest, however. Strength testing, however, has been recommended as part of the evaluation for LSS, with an emphasis on grading the knee flexors and extensors, ankle dorsiflexors and plantarflexors, and the extensor hallucis longus at rest.1,8,11 None of the large randomized clinical trials of therapeutic interventions for LSS have reported a MMT, even at rest.1,3-6 A recent Delphi consensus process developed and tested criteria for LSS compared with 2 other lumbar spine–related causes of pain and found only 1 test of strength, a squat and stand, to contribute to the correct diagnosis. 7 The group did not discuss a MMT at the time of symptoms. On the other hand, the detailed case studies from the 1970s published by Verbiest 12 found that the symptoms of LSS that differed the most compared with sitting were pain and loss of power. He described a motor deficit in 112 of 143 cases during the pain of intermittent claudication. One strategy to test the utility of the provocative walking test would be to include it in a randomized clinical trial that compares interventions for LSS, then use a regression analysis to weigh its sensitivity and specificity to the diagnosis (as in stratification of individuals based on presence or absence of weakening) and outcome (recovery from weakening compared with usual primary outcomes).
Trials have emphasized self-reports of pain and mobility or pain-related quality of life because outcome measurement tools such as the Short Form-36 and Oswestry Disability Index 1 may not capture the transient weakness that can impair balance and walking ability. Self-reports about weakness, imbalance, or gait difficulty may not be as sensitive, especially for clinical trials, as an objective measure of strength at the time the patient experiences symptoms.
As in several of our patients, others have been reported to experience little if any discomfort, but present instead with “subjective feelings of weakness,” abnormal sensations, or fatigue affecting the lower extremities.1,8-11 Indeed, we often found weakness after a 400-foot walk before the neurogenic claudication pain began or was bothersome and before the patient was aware of paresis. A wide-based gait and abnormal Romberg test were the most specific physical examination findings in several reviews of LSS but present in only about 30% of individuals.1,8-11 These tests, performed after the patient has been upright, probably reflect weakness in the hip girdle muscle groups, although sensory root compression could contribute. A direct test of strength after walking, however, offers a more reproducible and biologically sound way to detect such weakness and to best explain a slightly waddling gait with shortened stride length, as found in our series. Other provocative tests such as treadmill walking and lumbar extension loading or use of accelerometers to detect changes in gait parameters and postural sway have been suggested to better establish the diagnosis 1 but may add unnecessary complexity to what can be brought out with an overground walk.
A positive provocative test in a patient who meets other suggestive criteria for LSS may also predict that physical therapies will fail to lessen walking-induced pain or weakness that arises from transient multiroot compression. Other sources of pain from, for example, joint and musculoligamentous sources may lessen with physical therapy that aims to increase range of motion, core and limb strength, and fitness. Once episodic transient paraparesis is recognized and its potential impact appreciated, management may include a cane or rolling walker for safety and to enable forward bending that lessens compression of roots by the longitudinal ligament, along with counseling about greater care on descending stairs or walking downhill (when back extension increases), when stepping off a curb, or walking on uneven ground as well as a recommendation for seated rest stops as needed.
This study is limited by its small sample size and selection bias related to the flow of referrals to a single university clinic. Thus, the incidence of demonstrable walking-induced paraparesis is uncertain, but one may anticipate that the provocative test will detect most if not all patients who ought to consider decompressive surgery. The MMT as performed is more structured and rapid than practiced by most clinicians, so assessment of its reliability will be necessary before the simple procedure can augment decision making and outcome assessment. Further prospective testing for the onset of leg weakness during a provocative walk followed by recovery at rest is clinically important for further study because the finding may serve as a sine qua non for the diagnosis of disabling motor impairment from LSS and as one of the entry criteria and outcome measures for controlled trials of interventions.
Conclusion
A careful MMT before and after a provocative walking test may increase the likelihood of correctly making the diagnosis of symptomatic LSS. Perhaps just as important, this objective sign may serve as a more naturalistic way to assess its severity and monitor disease progression over time. Onset of provoked weakness that limits and endangers mobility is perhaps as strong a sign as pain when considering a candidate for surgery. A positive walking test, of course, is not an absolute indication for a surgical intervention. For clinical trials, the MMT may improve diagnostic entry criteria (an objective measure of provoked paraparesis) and add a clinically important and objective outcome measurement tool to supplement subjective self-reports about pain and physical functioning.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.