
Abstract
Background. The recovery of motor function following stroke is largely dependent on motor learning–related neuroplasticity. It has been hypothesized that intensive aerobic exercise (AE) training as an antecedent to motor task practice may prime the central nervous system to optimize motor recovery poststroke. Objective. The objective of this study was to determine the differential effects of forced or voluntary AE combined with upper-extremity repetitive task practice (RTP) on the recovery of motor function in adults with stroke. Methods. A combined analysis of 2 preliminary randomized clinical trials was conducted in which participants (n = 40) were randomized into 1 of 3 groups: (1) forced exercise and RTP (FE+RTP), (2) voluntary exercise and RTP (VE+RTP), or (3) time-matched stroke-related education and RTP (Edu+RTP). Participants completed 24 training sessions over 8 weeks. Results. A significant interaction effect was found indicating that improvements in the Fugl-Meyer Assessment (FMA) were greatest for the FE+RTP group (P = .001). All 3 groups improved significantly on the FMA by a mean of 11, 6, and 9 points for the FE+RTP, VE+RTP, and Edu+RTP groups, respectively. No evidence of a treatment-by-time interaction was observed for Wolf Motor Function Test outcomes; however, those in the FE+RTP group did exhibit significant improvement on the total, gross motor, and fine-motor performance times (P ≤ .01 for all observations). Conclusions. Results indicate that FE administered prior to RTP enhanced motor skill acquisition greater than VE or stroke-related education. AE, FE in particular, should be considered as an effective antecedent to enhance motor recovery poststroke.
Introduction
Stroke is a leading cause of long-term disability among older adults in the United States, 1 with approximately 5.8 million survivors experiencing residual neurological deficits. 2 Neuroplasticity is thought to underlie the relearning of lost motor function through adaptation and potentiation of neural connectivity.3,4 Rehabilitation specialists aim to facilitate neuroplasticity by prescribing motor learning–based therapies, such as constraint-induced movement therapy and task-oriented motor practice.4,5 Despite advances in rehabilitation, nearly two-thirds of individuals do not recover sufficient motor function to incorporate the more affected hand into daily activities 6 months after stroke. 6 To address this gap, field experts have called for novel rehabilitation approaches to improve outcomes and long-term functional recovery for individuals following stroke.7,8
There is evidence in the animal and human literature to suggest that aerobic exercise (AE) training may have a role in facilitating neuroplasticity.9-13 Animal models of stroke indicate that moderate- to high-intensity AE training primes the central nervous system (CNS) by creating a neural response that facilitates plasticity, thereby optimizing motor recovery.7,13-16 Accumulating data suggest AE leads to an upregulation of brain-derived neurotrophic factor (BDNF), a neurotrophin that has been implicated as a mediator of motor recovery after stroke.7,12-18
In healthy humans, AE training has been shown to influence factors associated with neuroplasticity, including increased peripheral levels of BDNF,14,19 insulin-like growth factor-1,14,20 cerebral blood flow, and enhanced synaptogenesis and neurogenesis.14,15 In humans with stroke, Boyne et al 21 found elevated peripheral BDNF responses and increased corticospinal excitability following strenuous aerobic training. From a behavioral perspective, numerous studies have demonstrated that in healthy young adults, a single bout of moderate- to high-intensity AE completed prior to motor task practice enhances motor skill acquisition.22-24 Moderate-intensity AE has also been shown to improve cognitive function and mood in healthy adults and those with chronic conditions.17,25-30 Thus, abundant evidence exists demonstrating that AE modulates the CNS to influence brain function and motor performance.
Based on previous data linking AE interventions to improvements in brain function, we sought to determine whether the neuroplastic effects of AE could be exploited to improve motor recovery in individuals with chronic hemiparesis caused by stroke. Two modes of AE training were evaluated: forced exercise (FE) and voluntary exercise (VE). FE is a novel exercise model that augments, but does not replace, the voluntary efforts of a participant to facilitate sustained AE training.31-34 Changes in central and peripheral function provide the rationale to extend FE to this population because stroke often leads to difficulty achieving or sustaining intensive AE exercise as a result of structural and metabolic changes in hemiparetic muscle, 35 profound cardiovascular deconditioning, 36 and a general decrease in cortical activation. 37 The FE approach allows participants to achieve and maintain a greater exercise rate than what they can achieve voluntarily by augmenting pedaling cadence on a stationary bicycle, thus overcoming stroke-related sensorimotor impairment. It is critical to note that FE is not passive exercise; participants must actively contribute to the activity in order to exercise within a prescribed target heart rate (HR) zone. By augmenting participants’ voluntary efforts, FE provides a consistent exercise pattern and rapid rate that may enhance afferent input and sensorimotor interactions to elicit the physiological response necessary for neuroplasticity.
The aim of this study was to determine the effects of AE combined with upper-extremity (UE) motor task practice on the recovery of motor function in adults with stroke. To examine our aim, we compared the effects of FE, VE, and time-matched task practice without an AE component. It was hypothesized that the FE paradigm would be superior to VE or time-matched motor task practice by enabling participants to attain and sustain a rate of exercise necessary to trigger a neuroplastic “priming” response, 38 creating an environment in which motor recovery is optimized.
Materials and Methods
Study Design and Population
This report is a secondary analysis of data from 2 randomized clinical trials (clinicaltrials.gov registration numbers NCT02076776, National Institute of Health, and NCT02494518, American Heart Association). Both studies were approved by the Cleveland Clinic Institutional Review Board, and all participants completed the informed consent process. Individuals 18 to 85 years of age, >6 months post–unilateral stroke who met the following inclusion criteria were eligible for participation: (1) UE Fugl-Meyer Motor Score 19 to 55 and (2) physician approval to undergo cardiopulmonary exercise (CPX) stress test. Primary exclusion criteria were as follows: (1) hospitalization for myocardial infarction, congestive heart failure, or heart surgery within 3 months of study enrollment; (2) serious cardiac arrhythmia; (3) hypertrophic cardiomyopathy; (4) severe aortic stenosis; (5) cardiac pacemaker; (6) pulmonary embolus; (7) other cardiovascular, medical, or musculoskeletal contraindication to exercise; (8) significant cognitive impairment or major psychiatric disorder resulting in difficulty to participate in the study: and (9) antispasticity injection in the UE within 3 months of study enrollment.
Outcomes of Interest
All participants underwent a CPX test using an upright cycle ergometer (Lode Excalibur Sport with Pedal Force Measurement, Lode B V, Groningen, Netherlands), interpreted by a cardiologist blinded to group allocation to determine safe cardiopulmonary response to maximum exertion. A 12-lead electrocardiogram was used to continuously monitor HR and rhythm 5 minutes prior to, during, and for 5 to 10 minutes after CPX testing.
An incremental workload protocol was used beginning at 20 W and increasing in 20-W stages every 2 minutes until attaining 100 W, at which time resistance was increased by 40 W every 2 minutes. Pedaling cadence was self-selected and participants were cued to maintain this cadence throughout the CPX test. The CPX test was terminated based on the American College of Sports Medicine maximal exertion criteria 39 or volitionally by the participant for reasons of fatigue.
Clinical outcomes evaluating motor recovery were obtained at baseline, end of treatment (EOT), and 4 weeks following EOT (EOT+4) by the same trained occupational therapist blinded to group allocation. The primary motor outcome was the Fugl-Meyer Assessment (FMA), an impairment-based measure consisting of 33 items evaluating the ability of the individual to move out of synergistic patterns toward isolated movement control. 40 Movement quality in the affected UE is compared with that in the nonaffected UE and scored using a 0 to 2 ordinal scale, in which 0 indicates no movement, 1 indicates partial movement of the affected UE, and 2 indicates movement comparable to the nonaffected UE.
The secondary motor outcome was the Wolf Motor Function Test (WMFT). 41 The WMFT is a validated measure of UE function poststroke, consisting of 15 timed tasks and 2 strength tasks. Each timed task can be classified primarily as gross or fine motor in nature and is also graded using a 0 to 5 ordinal scale rating movement quality, with higher scores indicating better movement quality.
Interventions
Following baseline testing, participants were randomized to 1 of 3 groups using a nonreplenished sealed envelope pull method. The intervention arms, described in detail in our previous publication, 42 were as follows: (1) FE + UE repetitive task practice (FE+RTP); (2) VE + UE repetitive task practice (VE+RTP); or (3) stroke education + UE repetitive task practice (EDU+RTP). All groups engaged in 90-minute sessions 3 times per week for 8 weeks.
Forced Exercise + Repetitive Task Practice
Individuals randomized to the FE+RTP group exercised for 45 minutes on a recumbent stationary cycle ergometer equipped with an electric motor and control algorithm to mechanically augment pedaling rate by 30% greater than the participant’s voluntary pedaling rate achieved during the exercise stress test.33,34,43 Each 45-minute FE session was monitored by an exercise physiologist or physical therapist and included a 5-minute warm-up, 35-minute main exercise set, and a 5-minute cooldown. Although assistance was provided in the FE mode via the motor to augment pedaling rate, it is important to note that the participant was actively contributing to the pedaling action. Participants were instructed to maintain their HR between 60% and 80% of their heart rate reserve (HRR) calculated using maximal HR achieved during the CPX with the Karvonen formula. 44 HR was continuously monitored, and study staff cued participants as needed to ensure compliance with the target HR range. Blood pressure and rate of perceived exertion were obtained every 10 minutes, and cadence and power were recorded every 5 minutes. Following a 10-minute rest period, participants completed a 45-minute session of UE RTP.
RTP emphasizes highly repetitious blocked practice tasks that are functional, goal oriented, and relevant to the individual. 45 The approach to RTP was modeled after Lang, Birkenmeier, and others.46-48 Tasks included gross and fine-motor components involving proximal and distal motor control; for example, reaching to a shelf positioned at knee height, and grasping a plastic cup and placing it on a shelf positioned at shoulder height. The RTP activities were administered by a neurological physical therapist who tailored each task to ensure appropriate difficulty and relevance. During the 45-minute RTP session, the therapist typically selected 3 to 5 tasks and targeted 70 to 100 repetitions of each task.
Voluntary Exercise + Repetitive Task Practice
The VE+RTP sessions were conducted in an identical manner to the FE+RTP sessions, except participants in the VE+RTP group exercised for 45 minutes on a stationary recumbent cycle ergometer at a self-selected cadence without assistance from a motor. Target HR range was identical to the FE+RTP group, at 60% to 80% of HRR. Exercise monitoring and RTP sessions were also conducted in a manner identical to that in the FE+RTP group.
Stroke Education + Repetitive Task Practice (Edu+RTP)
The control group underwent a time-matched intervention consisting of a 45-minute session of stroke-related education followed by a 45-minute session of UE RTP. Each education session covered a different stroke-related topic, such as stroke pathology, nutrition, pharmacology, fatigue, and so on. The RTP sessions were administered in a manner identical to that in the FE+RTP and VE+RTP groups.
Statistical Analysis
Randomized groups were compared on participant demographics, using ANOVA for normally distributed variables, the Kruskal-Wallis test for nonnormally distributed continuous variables, or the χ2 test for categorical variables. The effects of intervention were assessed using separate linear mixed-effects models for each outcome, each including a random intercept, a main effect term for time, and a group-by-time interaction term. Each model adjusted for baseline differences between randomized group by including the baseline assessment as part of the outcome vector and by excluding the group main effect term from the model. 49 For each outcome, the group-by-time interaction was assessed at the 0.05 significance. To meet model assumptions, WMFT total performance time, gross motor performance time, and fine-motor performance time were log transformed.
Regardless of statistical significance, post hoc contrasts were performed for each model estimating the change from baseline to EOT and from baseline to EOT+4 within each randomized group. Within each outcome, pairwise comparisons were Bonferroni corrected to maintain a 5% type I error rate per outcome. All analyses were conducted using R version 3.4.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 40 participants ranging from 6 to 101 months poststroke were included in the analyses. A flow diagram is presented in Figure 1. Participant demographic and medical characteristics are summarized in Table 1. Intervention-related variables, including dosage of RTP (number of repetitions), cycling cadence in revolutions per minute (RPM), and AE intensity (percentage HRR and power) are also summarized in Table 1. All 3 groups were administered comparable RTP dosages. The 2 AE groups exercised for similar times at comparable aerobic intensities: 60% HRR and 59% HRR for the FE+RTP and VE+RTP groups, respectively. In all, 44% of the FE and 50% of the VE participants achieved 60% HRR or greater during the AE training. Cadence was significantly higher for the FE+RTP group compared with the VE+RTP group, at 74 versus 59 RPM, respectively.
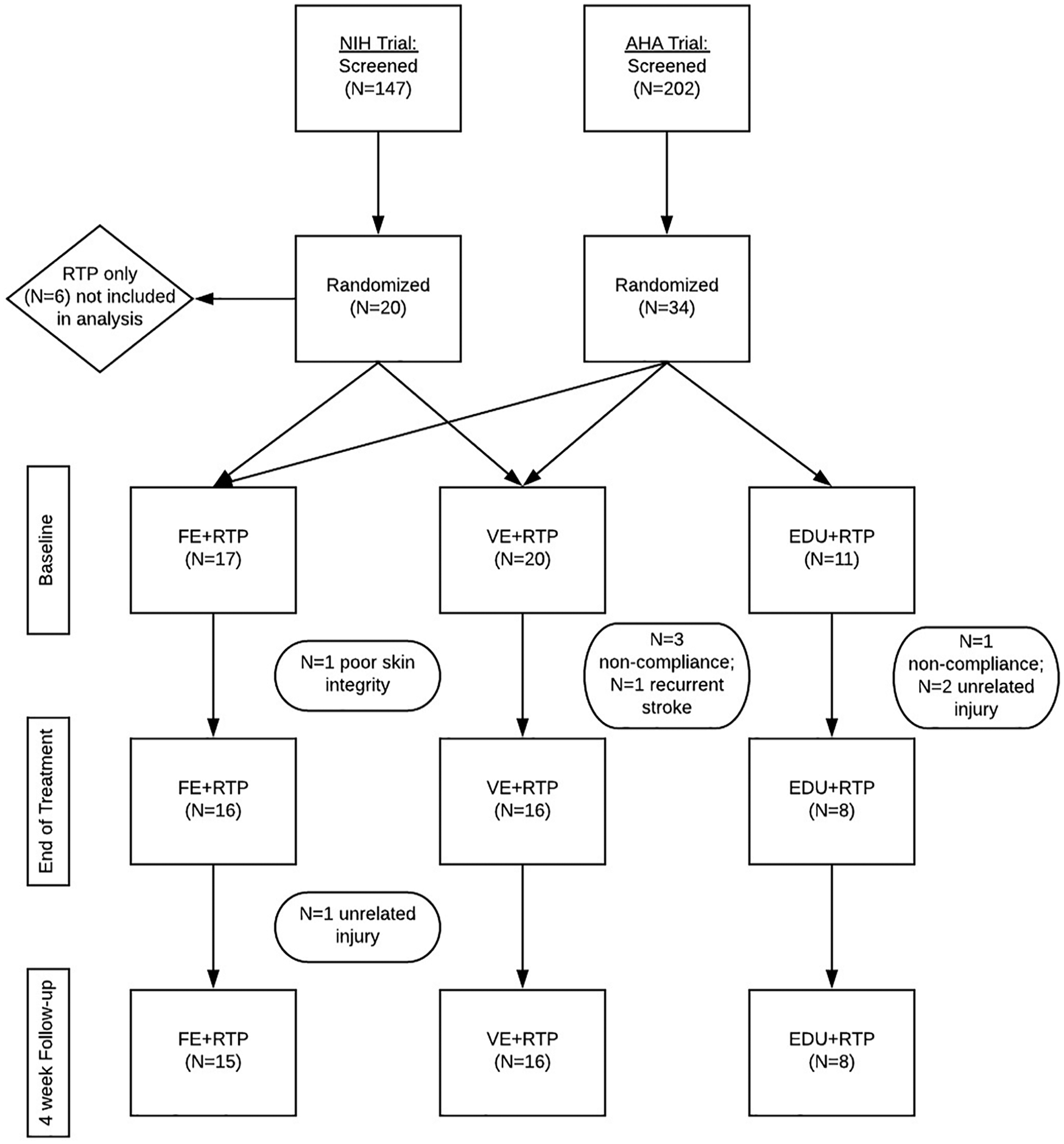
Flowchart depicting the 2 randomized clinical trials included in this analysis.
Participant Demographics and Intervention Variables by Randomized Group. a
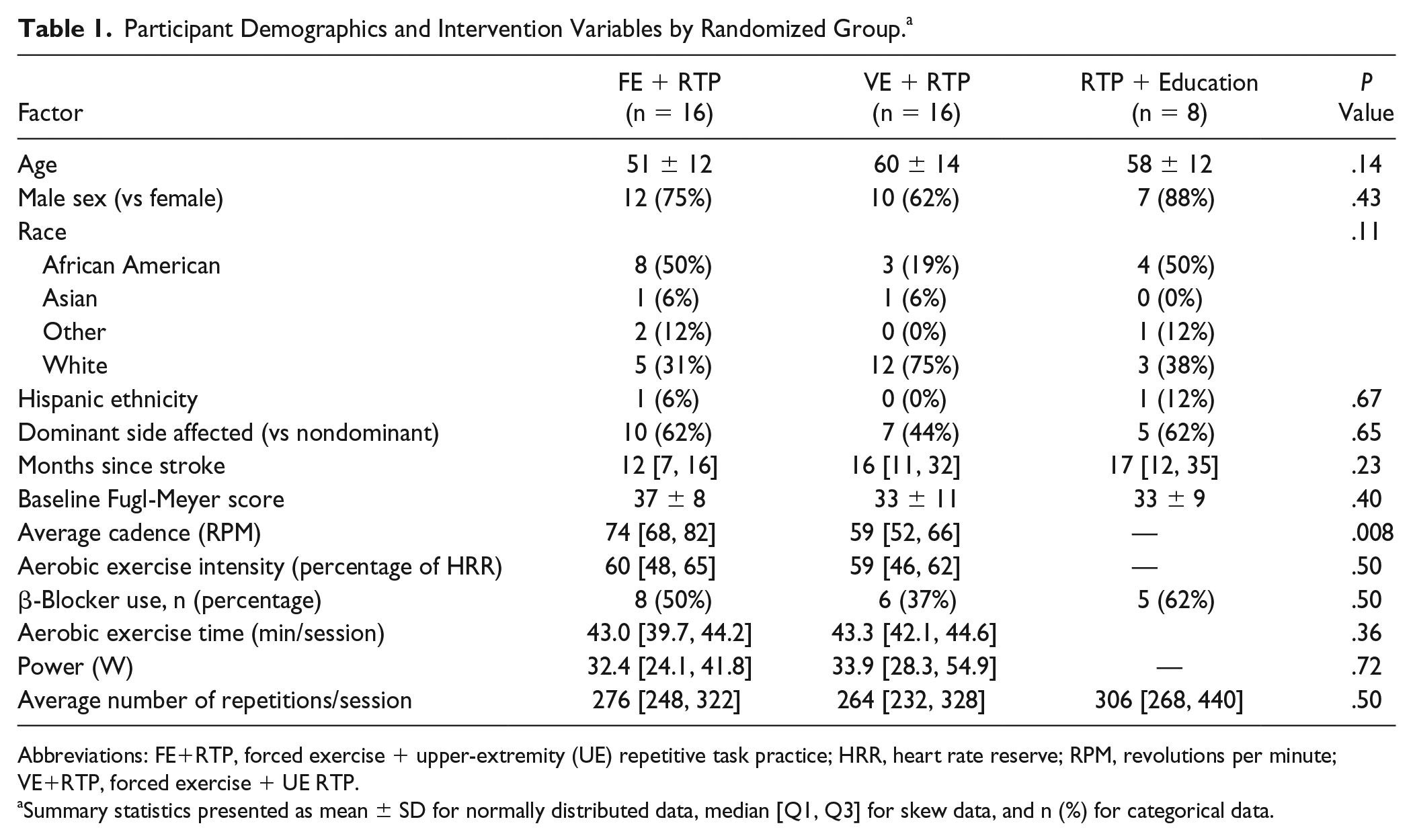
Abbreviations: FE+RTP, forced exercise + upper-extremity (UE) repetitive task practice; HRR, heart rate reserve; RPM, revolutions per minute; VE+RTP, forced exercise + UE RTP.
Summary statistics presented as mean ± SD for normally distributed data, median [Q1, Q3] for skew data, and n (%) for categorical data.
FE+RTP Group Exhibits Greatest Improvement in FMA
Group by time and within-group results for all motor outcomes at 3 time points (baseline, EOT, and EOT+4) are shown in Table 2. There was a significant group-by-time interaction in the FMA score favoring the FE+RTP group (P = .001). Post hoc pairwise comparisons revealed that improvements by the FE+RTP group were significantly greater than the VE+RTP group from baseline to EOT and baseline to EOT+4 (P < .05). All 3 groups improved significantly by a mean of 11, 6, and 9 points for the FE+RTP, VE+RTP, and Edu+RTP groups, respectively. Changes in FMA scores are shown in Figure 2.
Outcomes at Each Evaluation Time Point by Randomized Group (ie, FE + RTP, VE + RTP, and RTP + Education). a
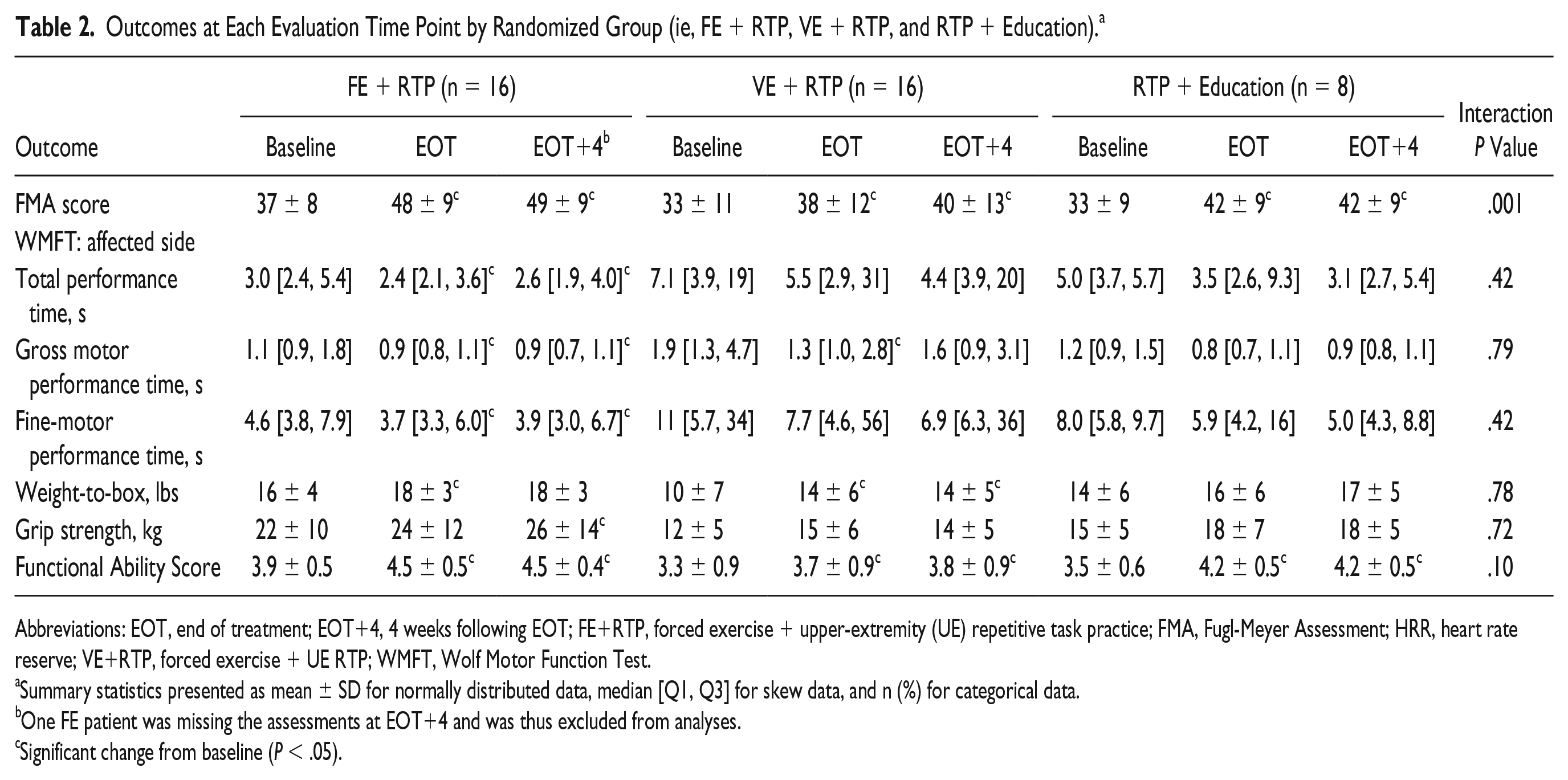
Abbreviations: EOT, end of treatment; EOT+4, 4 weeks following EOT; FE+RTP, forced exercise + upper-extremity (UE) repetitive task practice; FMA, Fugl-Meyer Assessment; HRR, heart rate reserve; VE+RTP, forced exercise + UE RTP; WMFT, Wolf Motor Function Test.
Summary statistics presented as mean ± SD for normally distributed data, median [Q1, Q3] for skew data, and n (%) for categorical data.
One FE patient was missing the assessments at EOT+4 and was thus excluded from analyses.
Significant change from baseline (P < .05).
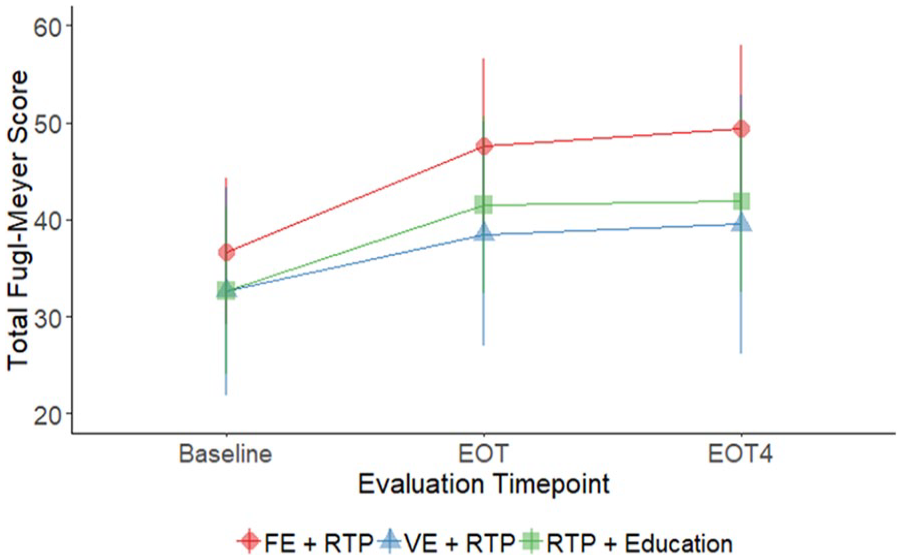
Line plot depicting means and SDs of Fugl-Meyer scores at baseline, EOT, and EOT+4. A significant interaction effect was found, indicating that improvements were greatest for the FE+RTP group (P = .001).
Improved Motor Function for All Groups Measured by WMFT
No evidence of a treatment-by-time interaction was observed for any of the WMFT outcomes (Table 2). However, total, gross motor, and fine-motor performance time for the WMFT significantly improved from baseline to EOT and from baseline to EOT+4 for the FE+RTP group (P ≤ .01 for all observations). The VE+RTP group experienced a significant improvement in gross motor performance time from baseline to EOT (P = .03). Functional ability score significantly improved from baseline to EOT and from baseline to EOT+4 for each of the 3 randomized groups (P < .001 for all observations). Grip strength significantly increased from baseline to EOT+4 for the FE+RTP group (P = .01) but did not change in the other groups.
Discussion
The benefits of AE training in individuals poststroke have almost exclusively been evaluated using cardiovascular end points.8,36,50 Improving cardiovascular fitness is clearly important and critical in overall health and in secondary stroke prevention. However, understanding how AE could be used to facilitate motor recovery has not been systematically evaluated and reflects a missed opportunity in rehabilitation practice. Greater improvements in clinical measures of motor recovery indicate that FE may be optimal in “priming” the CNS for motor skill acquisition associated with a RTP intervention.
Forced AE Facilitates Motor Recovery
Numerous questions remain regarding what exercise parameters induce the optimal effect in terms of facilitating motor recovery poststroke. As such, it is important to differentiate among the variables that define exercise intensity. In our study, we classified exercise intensity according to aerobic intensity (measured as percentage HRR), rate intensity (speed or cadence), and power intensity (W), in addition to duration (min/session). As it relates to AE, both groups exercised at similar aerobic intensities: 60% HRR for the FE group and 59% HRR for the VE group. Furthermore, power produced for both AE groups was similar at 32.4 and 33.9 W for the FE and VE groups, respectively, as was exercise duration. The only training variable that differed between the 2 AE groups was cadence or the rate of pedaling. On average, the FE group cycled 22% faster than the VE group: 74 compared with 59 RPM, respectively. In animal models of ischemic stroke, treadmill training and wheel running are predominant modes of AE intervention. When investigating the optimal rate of exercise, moderate rate exercise (30%-50% of maximal running speed) has been found to be most efficacious in reducing lesion size, decreasing inflammation, and facilitating neurogenesis. 51 Moderate- to high-rate running speeds for shorter durations using a FE mode optimized ipsilesional and striatal angiogenesis. 51 Additionally, we have found that increased pedaling rate was positively correlated with CNS cortical and subcortical functional connectivity and improved motor function in individuals with PD.33,43,52,53 The FE approach augments the voluntary efforts of individuals with stroke-related sensorimotor impairment, enabling participants to maintain a consistent exercise pattern and rapid rate that appears to be critical in motor recovery. The precise mechanism responsible for improved motor recovery in the FE+RTP group is unclear; however, it is plausible that moderate- to high-rate exercise induces neurophysiological and vascular changes in the CNS comparable to those seen in animal models to facilitate neuroplasticity.
The Impact of RTP Dose and Intensity
Examining the motor task practice aspect of our intervention, all 3 groups completed comparable dosages of RTP, with the FE+RTP, VE+RTP, and Edu+RTP groups averaging 276, 264, and 306 repetitions per 45-minute session, respectively. In a recent report, Lang et al 48 unexpectedly found no dose-response effect and only modest improvements in motor function when administering 100, 200, 300, or individual maximal repetitions of RTP, 4 times/wk over 8 weeks. Although a direct comparison of outcomes is not appropriate because of variations in study design, it is noteworthy to mention that although our RTP intervention involved 25% fewer sessions and 45% less time, we used a more rate-intensive RTP intervention, achieving a rate of ~350 to 400 repetitions/h. This more intensive approach to RTP may have contributed to the improvements observed in clinical measures of motor function. Lang and others have acknowledged that the intensity of RTP training is a potentially important variable that has not been systematically investigated but should be considered in the motor recovery equation.48,54
Considerations for Clinical Translation
An important consideration in the development of the intervention evaluated was its potential for clinical translatability and adoption. Our criteria for participation included individuals with broad ranges of UE function and did not exclude those with stable cardiovascular comorbidities. Given that we did not observe a relationship between baseline level of motor function and change in impairment, this combined AE+RTP approach appears to be efficacious for individuals with mild to moderate hemiparesis. The 45-minute duration of RTP was chosen because it is clinically feasible; however, we strongly recommend considering the rate of RTP administration as an important variable. 54 Our approach included minimal rest between sets and tasks, resulting in relatively continuous engagement of task practice while achieving ~350 to 400 repetitions/h.
With proper screening and monitoring, individuals with chronic stroke and cardiovascular comorbidities were able to safely exercise at moderate to high aerobic intensities for 45 minutes. Our protocol included CPX testing to determine the participant’s response to maximal activity. According to the American Heart Association/American Stroke Association physical activity recommendations for stroke survivors, graded exercise testing is recommended to assess functional capacity and cardiovascular response to exercise. 50 Finally, current reimbursement models in the United States do not consider AE training as a skilled, reimbursable treatment for individuals with stroke. Nonetheless, we seek to advocate for patients and challenge payers by presenting scientific evidence that exercise is not only good for one’s health but can facilitate brain function and potentially reduce disability.18,55
Limitations
There are limitations associated with the current study—namely, results reflect a compilation of 2 smaller-scale randomized clinical trials. The RTP dosages were not identical for the 3 groups, and the VE group exercised just lower than the prescribed aerobic intensity of 60% HRR, achieving 59% HRR. Additionally, the FE group as a whole was younger and presented with higher baseline FMA scores. Although these demographic and intervention-related characteristics were not statistically different among groups, it is possible that the characteristics of the FE group were ideally suited to respond to a FE intervention. Influence of lesion size, location, or the effect of genetic characteristics on neuroplasticity poststroke were not considered in the randomization of participants.7,56 Future larger studies are planned to determine if demographic factors may influence response to FE. Finally, whereas we hypothesize potential mechanisms (eg, increased peripheral levels of BDNF, insulin-like growth factor-1, cerebral blood flow, and enhanced synaptogenesis14,19,20) that may be responsible for the changes in motor recovery evident with the FE+RTP group, neurotrophic factors were not measured. Future studies will utilize imaging and other modalities to elucidate the mechanism underlying improvement with FE and VE.
Summary
Our findings indicate that the completion of FE prior to UE RTP enhanced motor skill acquisition greater than VE or stroke-related education. These initial results provide rationale to integrate high-rate AE, FE in particular, into models of stroke rehabilitation to improve motor recovery.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JLA has authored intellectual property associated with the algorithm used in the control of the forced exercise cycle. The remaining authors declare no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This study was supported by the National Institute of Neurological Disorders and Stroke (R03HD073566) and the American Heart Association (15MCPRP25700312).