
Abstract
Background. The PREP2 algorithm combines clinical and neurophysiological measures to predict upper-limb (UL) motor outcomes 3 months poststroke, using 4 prediction categories based on Action Research Arm Test (ARAT) scores. The algorithm was accurate at 3 months for 75% of participants in a previous validation study. Objective. This study aimed to evaluate whether PREP2 predictions made at baseline are correct 2 years poststroke. We also assessed whether patients’ UL performance remained stable, improved, or worsened between 3 months and 2 years after stroke. Methods. This is a follow-up study of 192 participants recruited and assessed in the original PREP2 validation study. Participants who completed assessments 3 months poststroke (n = 157) were invited to complete follow-up assessments at 2 years poststroke for the present study. UL outcomes were assessed with the ARAT, upper extremity Fugl-Meyer Scale, and Motor Activity Log. Results. A total of 86 participants completed 2-year follow-up assessments in this study. PREP2 predictions made at baseline were correct for 69/86 (80%) participants 2 years poststroke, and PREP2 UL outcome category was stable between 3 months and 2 years poststroke for 71/86 (83%). There was no difference in age, stroke severity, or comorbidities among patients whose category remained stable, improved, or deteriorated. Conclusions. PREP2 algorithm predictions made within days of stroke are correct at both 3 months and 2 years poststroke for most patients. Further investigation may be useful to identify which patients are likely to improve, remain stable, or deteriorate between 3 months and 2 years.
Introduction
Recovery of upper-limb (UL) function after stroke is important for regaining independence in activities of daily living. 1 Early prediction of UL outcome may increase rehabilitation efficiency by tailoring therapy for individual patients. 2 However, making accurate predictions for individual patients based on clinical measures alone can be difficult. 3
The PREP2 algorithm combines clinical and neurophysiological measures within a few days of stroke to make predictions for UL functional outcomes at 3 months poststroke (http://www.presto.auckland.ac.nz). 4 Patients are predicted to achieve 1 of 4 functional UL outcome categories: Excellent, Good, Limited, or Poor. These UL functional outcome categories are based on ranges of scores on the Action Research Arm Test (ARAT), which were previously established through hypothesis free cluster analysis 5 and subsequently refined (Table 1). 4 Information that can be offered to patients in each predicted outcome category is provided in Table 1. This includes the expected level of UL function by 3 months poststroke and a suggested rehabilitation focus.
PREP2 Prediction Category Description and Suggested Rehabilitation Focus.
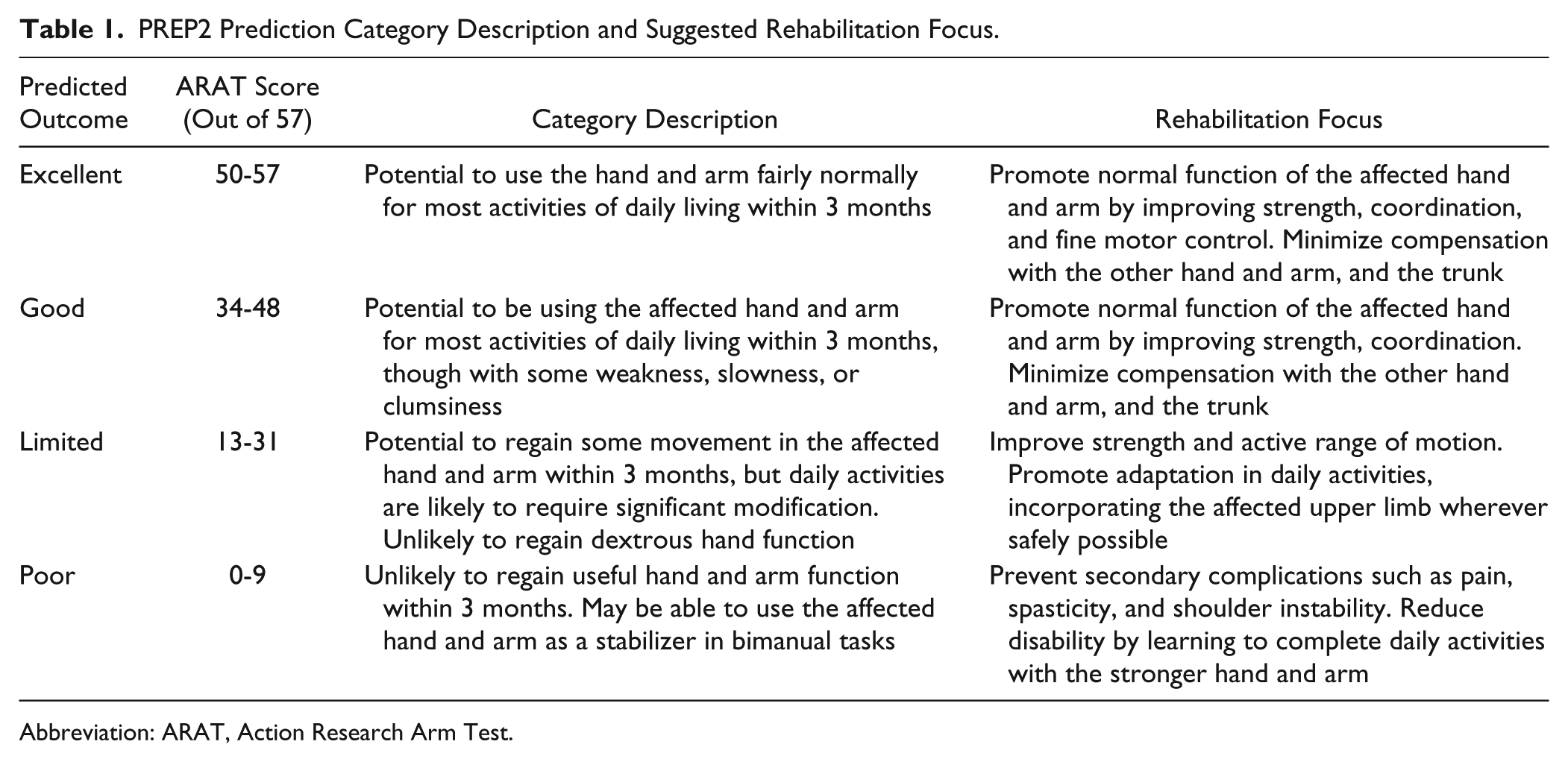
Abbreviation: ARAT, Action Research Arm Test.
The PREP2 algorithm starts by grading paretic UL Shoulder Abduction and Finger Extension (SAFE) strength at day 3 poststroke using the Medical Research Council grades (Figure 1). If the sum of these grades is ≥5/10, the patient’s age (<80 or ≥80 years) is taken into account to predict either an Excellent or Good UL functional outcome at 3 months. For patients with a SAFE score <5, ipsilesional corticospinal system function is evaluated with transcranial magnetic stimulation. Patients with motor evoked potentials (MEP+) in the first dorsal interosseus or extensor carpi radialis muscles of the paretic UL are predicted to achieve a Good UL functional outcome, regardless of the initial motor impairment. Patients without MEPs (MEP−) are predicted to achieve a Limited or Poor functional UL outcome, depending on overall stroke severity measured at day 3 poststroke with the National Institute of Health Stroke Scale. At 3 months poststroke, PREP2 predictions are correct for 75% of patients, with predictions too optimistic for most of the remaining 25%. 4
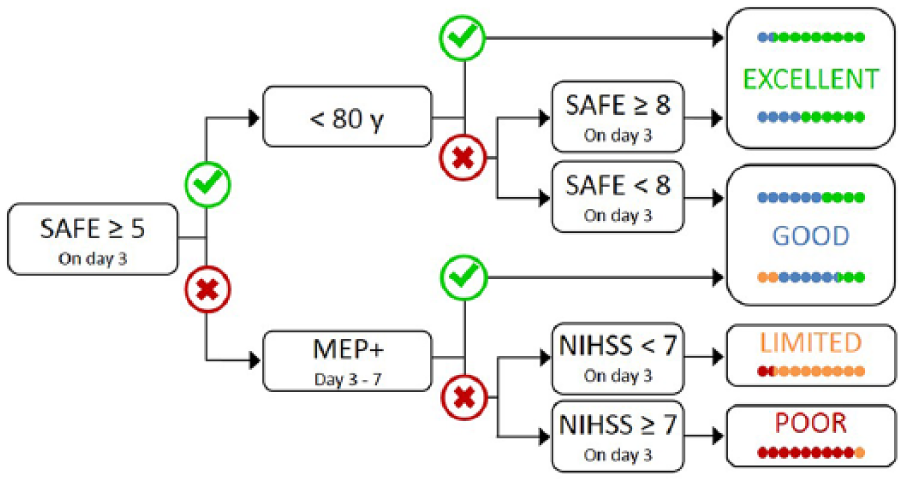
The PREP2 algorithm. The SAFE score is the sum of the Medical Research Council grades for Shoulder Abduction and Finger Extension, out of 5, for a total SAFE score out of 10. MEP+ means that MEPs can be elicited from the paretic extensor carpi radialis and/or first dorsal interosseous muscles of the paretic upper limb (UL) using transcranial magnetic stimulation. The algorithm predicts 1 of 4 possible UL functional outcomes at 3 months poststroke. Each prediction category is associated with rehabilitation goals that can be used to tailor UL therapy. 2 The colored dots represent, proportionally, PREP2 algorithm accuracy. The dots are color coded based on the outcome category actually achieved 3 months poststroke (green, Excellent; blue, Good; orange, Limited; red, Poor).
Most motor recovery after stroke occurs within the first 3 months.6-12 However, a plateau in motor performance might not occur until 5 to 6 months poststroke for some patients with more severe initial impairment.13,14 To the best of our knowledge, no longitudinal studies have tracked UL performance from early after stroke for more than 6 months. This means that little is known about what happens to UL impairment, function, and use once a patient reaches plateau and moves into the early chronic phase of stroke. Learned nonuse may contribute to deterioration in UL motor function from the peak motor performance achieved at plateau, particularly for patients with more severe UL impairment.14,15 This could make it difficult to discern whether the benefits of UL therapy reported in studies with patients at the chronic stage are a result of improvements over and above participants’ previous maximal function or a result of participants being boosted back up to their previous best after deterioration since the subacute stage.
The aim of this study was to determine whether PREP2 predictions made within a few days poststroke were correct 2 years after stroke and determine whether UL performance improves, deteriorates, or remains stable between 3 months and 2 years after stroke. We hypothesized that PREP2 predictions made at baseline would be correct at 2 years poststroke and PREP2 outcome category and UL motor performance would remain stable between 3 months and 2 years after stroke.
Methods
This is a follow-up study of the 192 patients recruited within 3 days of stroke to participate in the PREP2 algorithm validation study, which was previously reported. 2 Patients were eligible for participation in the PREP2 validation study if they were aged at least 18 years and had experienced an ischemic stroke or intracerebral hemorrhage producing unilateral UL weakness within the previous 72 hours. Previous stroke and acute reperfusion therapies were allowed. Patients were excluded if they had cerebellar stroke, had cognitive or communication impairments precluding informed consent, or lived out of the study area precluding follow-up. The PREP2 algorithm (Figure 1) was used to predict UL functional outcome within days of stroke for all participants in the validation study. 4
Of the original 192 participants in the PREP2 validation study, 157 (82%) completed follow-up assessments at 3 months poststroke. At 2 years poststroke, attempts were made to contact all participants who had completed 3-month assessments in the PREP2 validation study (n = 157) to determine eligibility for participation in the present 2-year follow-up study. All 157 participants were considered eligible unless they had moved out of the study area (not available for in-person assessments), they were unable to be contacted, or their medical status, cognition, or communication had declined to the point that they were no longer able to provide informed consent or were too unwell to participate. The 2-year time point was chosen to maximize the time since stroke while minimizing the expected natural attrition over time as patients experience medical deterioration or death. 16 The study was approved by the regional ethics committee, and written informed consent was obtained from each participant.
Follow-up assessments at 2 years poststroke were completed by trained clinical assessors who were blinded to the participants’ original PREP2 prediction. The assessments included the following: ARAT to determine PREP2 outcome category at 2 years, upper extremity Fugl-Meyer Assessment (FM-UE) to measure motor impairment, and the Motor Activity Log (MAL) for self-reported use of the paretic UL. Baseline clinical and demographic data, baseline PREP2 prediction, 3-month PREP2 outcome category, and 3-month FM-UE, ARAT, and MAL scores for each participant were retrieved from the PREP2 validation study data set.
Nonparametric tests were used for analyses because of the nonnormal distributions of data. Pearson χ2 tests were used to compare categorical baseline characteristics of participants included in this study (n = 86) with those who were not available for follow-up at 2 years (n = 71). The percentage of patients in this follow-up study who achieved their predicted UL outcome at 2 years was calculated. The percentage of patients who changed PREP2 outcome category between 3 months and 2 years poststroke was also calculated separately for patients whose category improved or worsened. Clinical scores (ARAT, FM-UE, MAL) were compared between 3 months and 2 years poststroke using related-samples Wilcoxon signed rank tests. Differences of 6 points in the FM-UE and ARAT scores were considered clinically meaningful.17,18 All tests were 2-sided, with α =.05 and are reported with 95% CIs.
Results
Of the 157 PREP2 validation study patients who completed a 3-month poststroke assessment, 86 participated in the present follow-up study at 2 years poststroke (33 [38%] women, mean [SD] age 72 [13] years; Figure 2, Table 2). These 86 participants had a lower median age, a lower incidence of atrial fibrillation, and fewer comorbidities, and there was a lower proportion of women compared with the 71 patients who were not available for follow-up at 2 years (Table 2). The reasons for being unavailable for follow-up assessment at 2 years are reported in Figure 2: deceased (19), unable to be contacted (19), medically unwell (8), cognitive deterioration (3), moved out of the study area (9), and declined to participate (13).
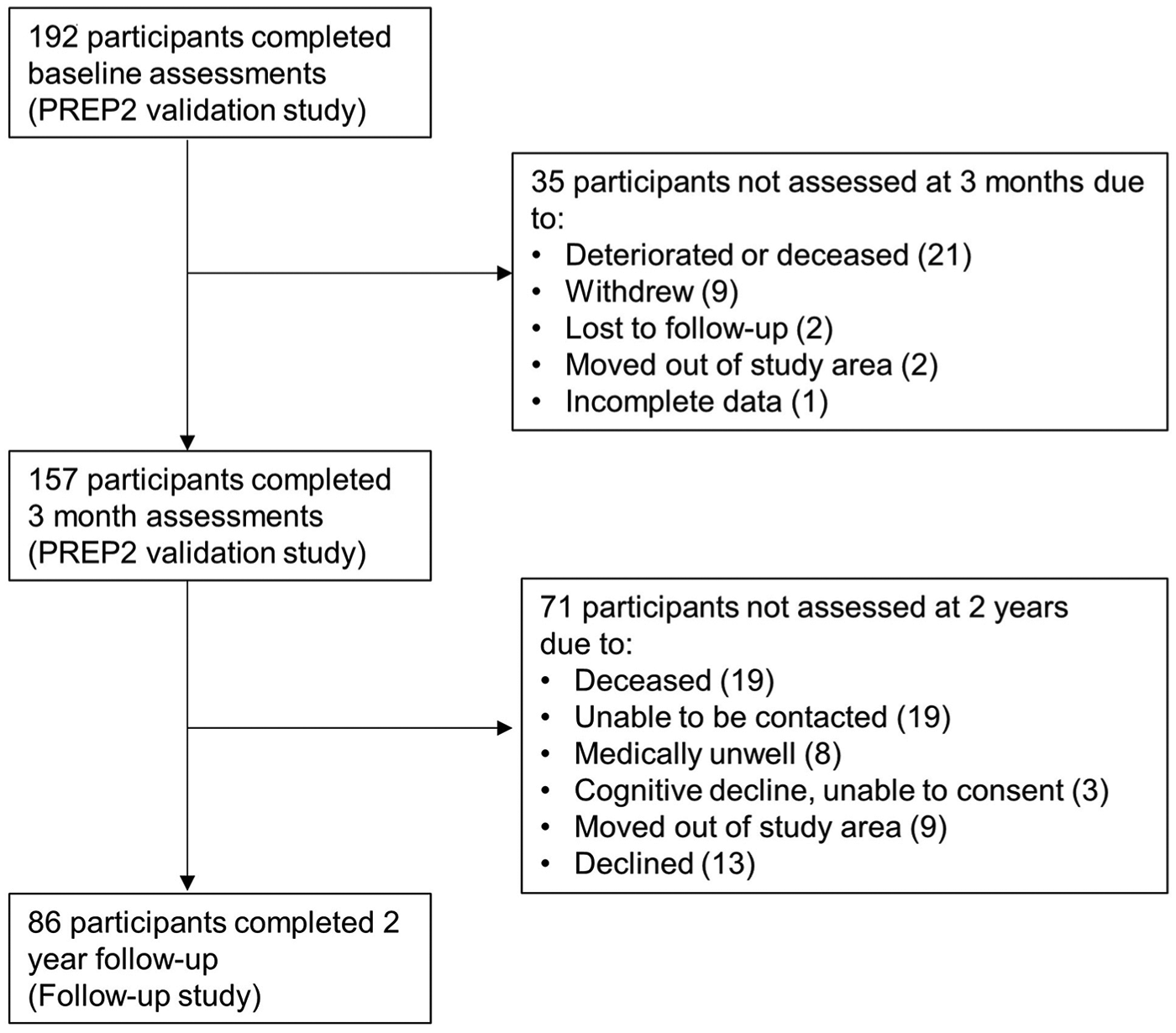
Study flowchart.
Baseline Data Obtained Within 7 Days Poststroke.
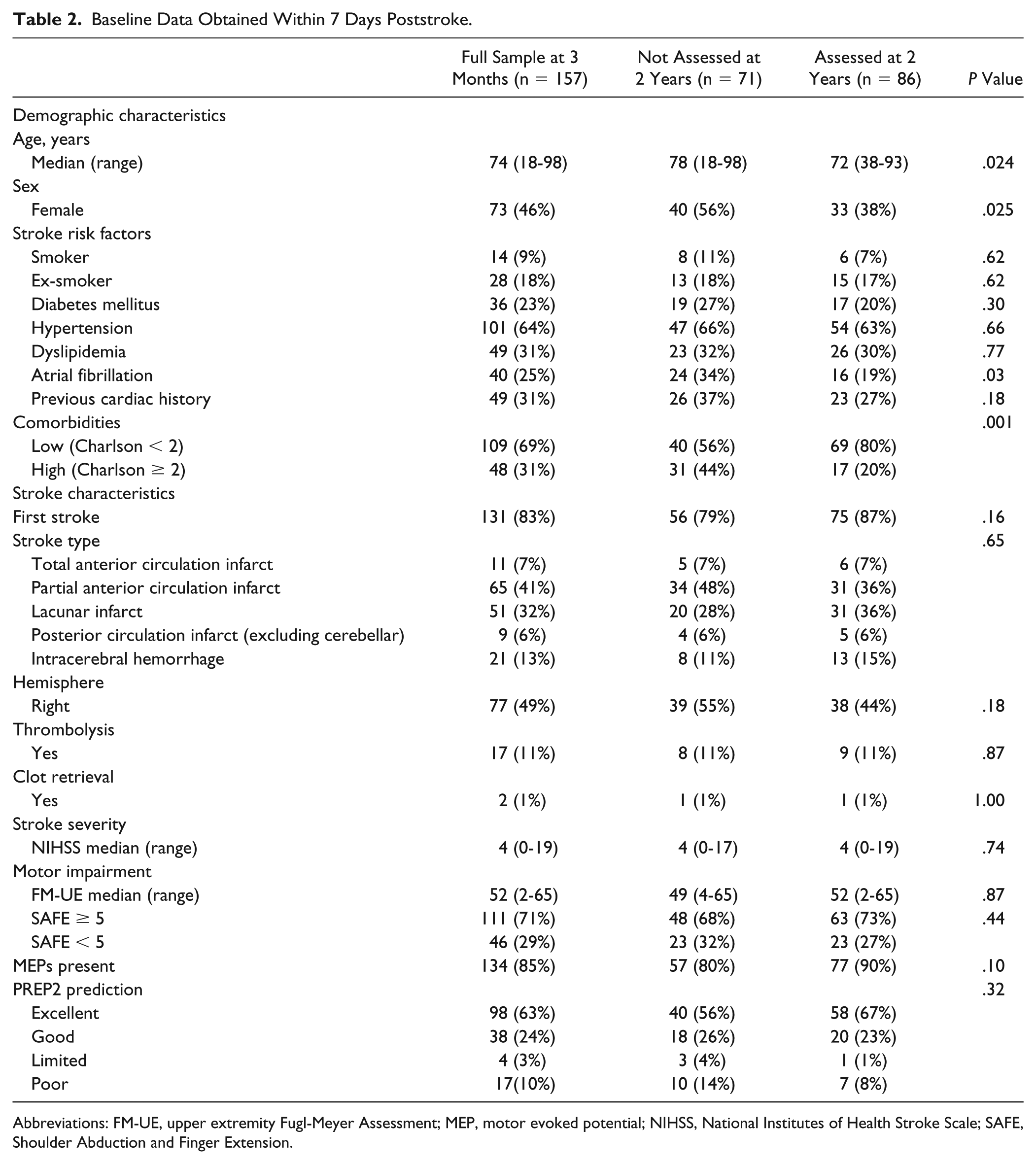
Abbreviations: FM-UE, upper extremity Fugl-Meyer Assessment; MEP, motor evoked potential; NIHSS, National Institutes of Health Stroke Scale; SAFE, Shoulder Abduction and Finger Extension.
PREP2 predictions made at baseline were correct for 69/86 participants (80%) 2 years poststroke (Table 3). Of the remaining 17 participants, PREP2 category was better than predicted for 9 (11%) and worse than predicted for 8 (9%) participants at 2 years poststroke.
Follow-up Assessments for Participants Who Completed Both 3-Month and 2-Year Assessments Poststroke.
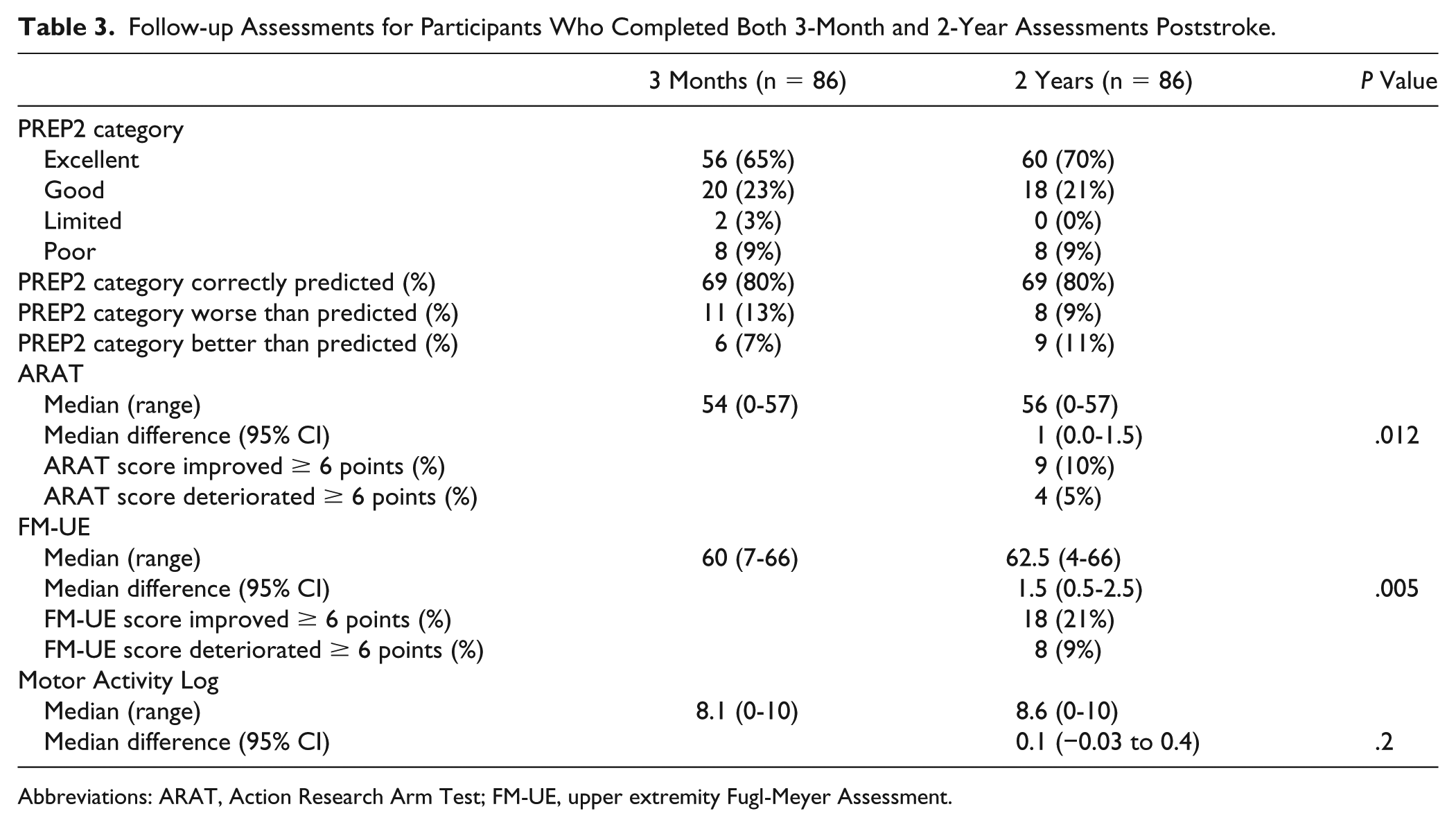
Abbreviations: ARAT, Action Research Arm Test; FM-UE, upper extremity Fugl-Meyer Assessment.
Most participants (71/86, 83%) remained in the same PREP2 UL outcome category between 3 months and 2 years poststroke. Of the 15 participants who changed category, 10 improved, 5 deteriorated, and all were predicted to achieve either a Good or Excellent UL outcome (Figure 3). Six of the 10 participants who improved had not achieved their predicted Excellent outcome category by 3 months but achieved it by 2 years. Two of the 10 participants who improved had achieved their predicted Good outcome by 3 months but exceeded their prediction, achieving an Excellent UL outcome by 2 years. The remaining 2 participants who improved had been predicted to achieve a Good outcome by 3 months but had only achieved a Limited outcome by this time. Between 3 months and 2 years, one of these participants improved to achieve the predicted Good outcome, and the other exceeded the predicted Good outcome to achieve an Excellent outcome. None of the participants predicted to achieve a Limited or Poor outcome changed categories between 3 months and 2 years poststroke. There were no differences in age, stroke severity, or comorbidities among participants whose UL outcome category remained stable, improved, or worsened (all P > .1).
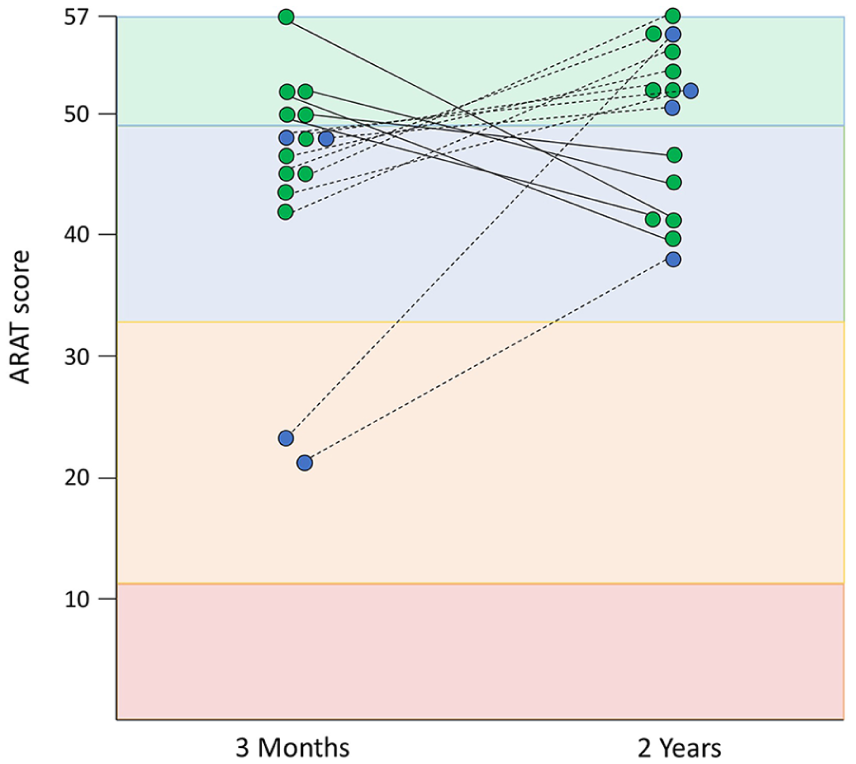
A total of 15 participants changed PREP2 category between 3 months and 2 years, based on the Action Research Arm Test (ARAT) score (maximum = 57). The 71 participants who did not change category are not depicted. Each dot represents a participant and is color coded based on their original PREP2 prediction (green, Excellent; blue, Good). The colored zone indicates the PREP2 outcome category actually achieved. Dots that do not match the color of their zone indicate that the participant either under- or overachieved their prediction at that time point. For example, 6 participants predicted to achieve an Excellent UL outcome (green dot) by 3 months only achieved a Good UL outcome (blue zone) at this time point. They improved to achieve their Excellent UL outcome by 2 years.
ARAT, FM-UE, and MAL scores could change between 3 months and 2 years without resulting in a change in PREP2 outcome category. Therefore, the differences in these UL scores between 3 months and 2 years were also examined. At the group level, the median difference between ARAT scores at 3 months and 2 years was 1 point (95% CI = 0-1.5; P = .012) and for FM-UE scores was 1.5 points (95% CI = 0.5-2.5; P = .005). These differences are statistically significant but not clinically meaningful6,7 (Table 3). However, some individual participants exhibited clinically meaningful increases and decreases in ARAT (n = 13, 15%) and FM-UE (n = 26, 30%) scores (Table 3), without necessarily changing outcome category. Of the 18 (21%) participants who increased FM-UE scores by 6 points or more, 6 participants also exhibited clinically meaningful increases in the ARAT score, and 5 of these improved PREP2 outcome category. Four of the 8 participants who decreased FM score also decreased ARAT score and dropped to a lower PREP2 UL outcome category. Three participants (3%) meaningfully improved ARAT score without a corresponding increase in FM score. The median difference between MAL scores at 3 months and 2 years was 0.1 (−0.03 to 0.4), which was neither statistically nor clinically significant.
Discussion
PREP2 algorithm predictions about UL functional outcome made within days of stroke are correct for 80% of patients at 2 years poststroke. Most participants (83%) remained in the same PREP2 category between 3 months and 2 years, and median scores for motor function (ARAT), motor impairment (FM-UE), and use of the paretic hand and arm (MAL) did not meaningfully change between these time points. These results indicate that functional limitations seen in patients at the chronic stage are predictable and likely to have been fairly stable since 3 months poststroke. Of the 10 participants whose UL outcome category improved between 3 months and 2 years, only 3 exceeded their original prediction, whereas the remaining 7 took longer than 3 months to achieve their original predicted UL function, achieving this by 2 years poststroke. Five participants deteriorated to a lower category between 3 months and 2 years. None of the participants predicted to achieve a Limited or Poor outcome changed categories between 3 months and 2 years poststroke. There was no difference in age, stroke severity, or comorbidities among those whose category remained stable, improved, or deteriorated. Further investigation would be useful to identify factors that predict which patients take longer than 3 months to achieve their predicted UL function and which patients are at risk of deteriorating after 3 months.
Although median ARAT and FM-UE scores did not meaningfully change between 3 months and 2 years after stroke for this group of participants, some individuals did exhibit a meaningful increase or decrease in these scores. However, only a third of the 18 participants who experienced a meaningful increase in FM-UE scores also experienced a meaningful increase in UL hand and arm function (ARAT score), and only half of those who had decreased FM-UE scores (n = 8) also had a decreased ARAT score. Despite a clinically meaningful change in UL function on the ARAT score for these participants, self-reported use of the UL did not change. This reflects the high threshold required for patients to translate changes in UL impairment into UL function and use of the UL in daily life. 19
Spontaneous biological recovery processes drive improvements in motor control and impairment during the initial weeks after stroke, with most motor recovery occurring within the first 3 months poststroke.6-11 However, studies at the chronic stage also report improvements in UL function after therapeutic interventions. The findings of this study shed some light on whether these improvements at the chronic stage are over and above previous best performance or whether the benefit from UL therapy at the chronic stage is a result of reconditioning or boosting the patients back up to previous best function. Although the ARAT score meaningfully increased for 9 (10%) and decreased for 4 (5%) participants between 3 months and 2 years poststroke, overall UL performance (UL impairment, function, and self-reported use) remained fairly stable during this time for the majority of participants. This stability in UL performance between 3 months and 2 years poststroke suggests that improvements at the group level, reported after an intervention at the chronic stage, are likely to be true improvements over and above previous performance. At the chronic stage, improvements in motor performance may be achieved by learning to compensate for residual impairments because motor learning is unimpaired after stroke.20,21
Of the 157 PREP2 validation study participants assessed at 3 months, only 86 (55%) were available to participate in this follow-up study 2 years after stroke. These participants were younger, there were a lower proportion of women among them, and they had fewer comorbidities compared with those who were unavailable. Stroke type, location, and severity did not distinguish between patients available for follow-up and those who were unavailable. The unavailability of nearly half of the PREP2 validation study participants limited the sample size for this follow-up study. However, this was largely unavoidable because most were unavailable as a result of illness, death, or moving out of the study area. This attrition rate is similar to other longitudinal studies poststroke. 16 Other limitations of this study include a lack of measures between 3 months and 2 years poststroke and no record of any UL rehabilitation undertaken in this time.
In conclusion, using the PREP2 algorithm, it is possible to predict UL functional outcomes within a few days of stroke, and these predictions are correct for most patients at both 3 months and 2 years. Most UL motor recovery occurs within the first 3 months after stroke; therefore, 3 months is an appropriate time point for UL predictions. Further investigation may be useful to improve the overall accuracy of the algorithm and identify which patients are likely to improve, remain stable, or deteriorate between 3 months and 2 years.
Footnotes
Acknowledgements
We thank Christine Mangold, Alison Elston, and Jenelle Preece for assistance with data collection. We thank the Neurological Foundation of New Zealand, Health Research Council of New Zealand, and the Julius Brendel Trust for funding support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Neurological Foundation of New Zealand, Health Research Council of New Zealand, and the Julius Brendel Trust.