
Abstract
Background. Language disorders may occur in patients with disorders of consciousness (DoCs), and they could interfere with the behavioral assessment of consciousness and responsiveness. Objective. In this study, we retrospectively explored whether ERP N400 was eventually associated with the presence of aphasia diagnosed in those patients who had evolved into Exit-Minimally Conscious State (E-MCS) at the clinical follow-up. Methods. In this retrospective cohort study, the ERPs elicited by an auditory sentences task were retrospectively examined in a sample of 15 DoC patients diagnosed according to the Coma Recovery Scale–Revised (CRS-R). All these 15 DoC patients underwent a (at least) 1-year clinical follow-up, which included a neuropsychological evaluation to assess language function among other cognitive functions. Ten healthy individuals also underwent the same paradigm to investigate the variability of ERPs characteristics. Results. The N400 ERP component with centroparietal topography was found in 9 of 10 healthy controls in response to the ill-formed sentences. Analysis of patients’ data revealed that (1) a significant N400 component could be detected in 64% (9 of 14 patients) of the DoC patients regardless of the type of DoC; (2) no significant N400 ERP component was retrospectively detected in those E-MCS patients who showed aphasia at the follow-up; and (3) the presence/absence of the N400-ERP component was consistent with the brain lesion side and significantly predict the recovery. Conclusion. These preliminary findings indicate that the absence of N400 was significantly associated with the presence of aphasia diagnosed at the clinical follow-up in E-MCS patients.
Keywords
Introduction
Severe acquired brain injury might often result in disorders of consciousness (DoCs) that can be acute and reversible or chronic and (partially or definitively) irreversible. Some patients with DoC might recover wakefulness without signs of consciousness (only showing reflex motor responses—that is, vegetative state/unresponsive wakefulness syndrome, VS/UWS), whereas others might show nonreflex motor responses with some interaction with the environment without functional communication (ie, minimally consciousness state [MCS]).1-3 The recent advancements in the development of neuroimaging and electrophysiological paradigms that do not require overt behavioral responses have opened new perspectives in the detection of residual cognitive functions and even signs of awareness in DoC patients otherwise unresponsive.4-8 In this context, brain event-related potentials (ERPs) have been receiving much attention as a valuable tool to assess residual information processing in DoC patients.9,10
Language disorders might also occur in DoC patients because of severe acquired brain injury (especially in those cases with prevalent left cerebral lesions). The covert presence of a language disorder such as aphasia might interfere with the assessment of consciousness level by means of the gold standard Coma Recovery Scale–Revised (CRS-R),11,12 which is essentially based on language comprehension and command following items.
The ERP component N400 is a centroparietal negativity that is assumed to encode for semantic language integration processing. 13 The so-called N400 effect consists in a larger negative deflection occurring around 400 ms after the presentation of a word, which is incongruent with the sentence context with respect to a congruent word.14,15 The stability/reliability of N400 semantic priming effects in healthy individuals was reported to be as high as r =0.85, with possible variations of this value related to the timing of the repeated observations. 16 More recently, the probability of detecting statistically significant N400 responses to different auditory linguistic paradigms has been further investigated at the single- (healthy) subject level. 15 The probability for N400 detection was reported to be influenced mainly by stimuli as well as task demand manipulation factors, and thus, its sensitivity can vary as a function of linguistic/semantic paradigm features. Demographic factors such as age would not have significant influence on the scalp N400 latency and amplitude. 17
Currently, only few studies focusing on the characteristics of N400 and reporting evidence for a preserved semantic processing in DoC patients are available.18-22 N400 paradigms were also included in hierarchical auditory batteries administered to investigate auditory processing in DoC patients as a whole (auditory, perceptual, semantic processing). 23 Among these studies, only 2 investigated the potential value of N400-ERP detection as a prognostic indicator of consciousness recovery in DoC patients.19,20
The main goal of the present study was to test whether the presence/absence of the N400 ERP—as an index of semantic language processing—could be indicative of a covert language disorder in patients with DoC. The novelty of the present research resided in focusing on a selected sample of DoC patients who were clinically followed up to at least 1 year from the neurophysiological assessment (see below) and screened for language disorders. To better capture the evidence for a potential diagnostic role of N400 ERP in unmasking covert language disorders otherwise evident only at the clinical follow-up, we focused on patients who recovered consciousness and evolved into Exit-MCS (E-MCS). Finally, the presence of N400 was also investigated in relation to the side of brain lesions as derived from the available imaging data. We expected (1) the presence of N400 only in those patients with no language disorders at the follow-up (E-MCS) and (2) a relationship between side of lesion and N400 presence/absence.
Methods
Retrospective Cohort Study
The original cohort included 20 patients, consecutively admitted to the Post-Coma Unit of the Neurorehabilitation Hospital “Fondazione Santa Lucia” (Rome, Italy) for rehabilitation purposes. All DoC patients are routinely subjected, at admission, to a neurophysiological (electroencephalography [EEG]) screening, which includes the delivery of an auditory paradigm eliciting the N200, P300 and whenever possible the N400 (depending on the clinical status some patients cannot comply with the length of the paradigm administration).
For the present study, we selected 15 patients among those who had completed the entire auditory paradigm, thus, including the N400-eliciting stimuli and those whose clinical follow-up (1 year later) was available. Three patients of the original cohort were, in fact, excluded because they did not execute the N400 paradigm for lack of collaboration and 2 because they were lost at the 1-year clinical follow-up (see Supplementary Figure S1).
Participants
A total of 15 patients with the diagnosis of DoC, according to CRS-R, caused by severe acquired brain injury (ie, Glasgow Coma Scale ≤ 8 in the acute phase24,25; 10 men; mean age 50 ± 16.4 years; all right-handed from the anamnestic record) and 10 healthy volunteers (6 men; mean age =26.5 ± 6.2 years; all right-handed from anamnestic record; no history of neurological/psychiatric disorders, alcohol/drug abuse) were entered in the analysis of the present study. The group of healthy individuals was included to verify the reliability of the proposed auditory paradigm in eliciting the N400-ERP component.
The present study protocol was approved by the local (Fondazione Santa Lucia) Ethics committee (Prot. CE/AG4/PROG.328-56). Written informed consent was obtained by both healthy volunteers and the patient’s legal surrogates.
Clinical and demographic characteristics of patients are reported in Table 1. Diagnosis of DoCs (VS/UWS, n = 7; MCS, n=8 patients) was based on the CRS-R. 26 All patients had at least 1 available brain magnetic resonance imaging (MRI) or computed tomography (CT) scan (details are illustrated in Table 2). The 3T MRI images (Allegra scanner; Siemens Medical Solutions, Erlangen, Germany) consisted of whole-brain T1- and T2-weighted images and T2* with FLAIR sequences. Particular care was taken to center the patients in the head coil and to restrain their movements with cushions and adhesive medical tape. In some patients, MRI could not be acquired (eg, contraindications to MRI and/or presence of motion artifacts), and they underwent a brain CT scan (GE LightSpeed VCT).
Patients’ overview: Demographic, Clinical (Assessment and Follow-up), and Neurophysiological (N400) data of the patients enrolled in the study.
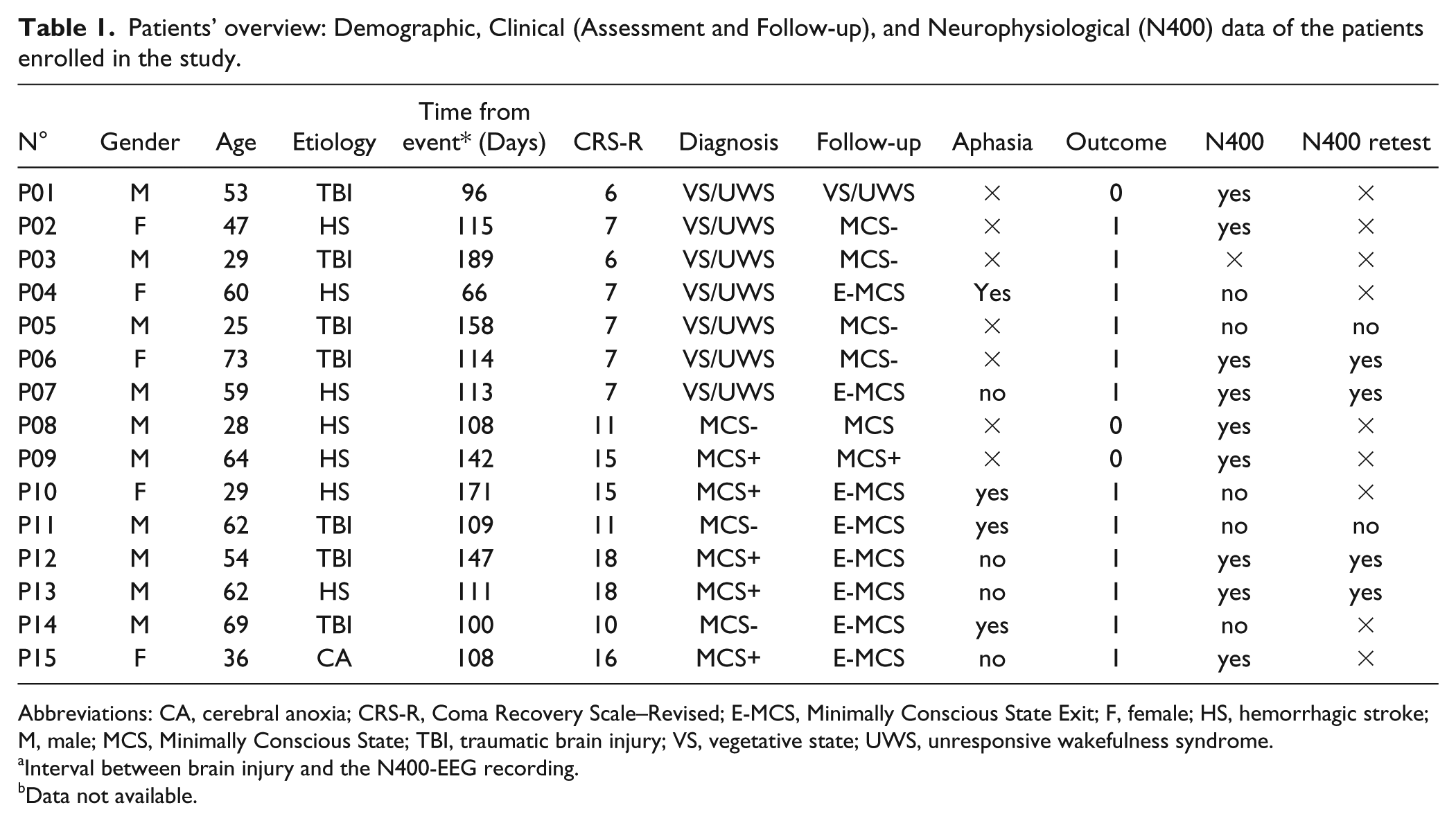
Abbreviations: CA, cerebral anoxia; CRS-R, Coma Recovery Scale–Revised; E-MCS, Minimally Conscious State Exit; F, female; HS, hemorrhagic stroke; M, male; MCS, Minimally Conscious State; TBI, traumatic brain injury; VS, vegetative state; UWS, unresponsive wakefulness syndrome.
Interval between brain injury and the N400-EEG recording.
Data not available.
Neuroimaging Data.
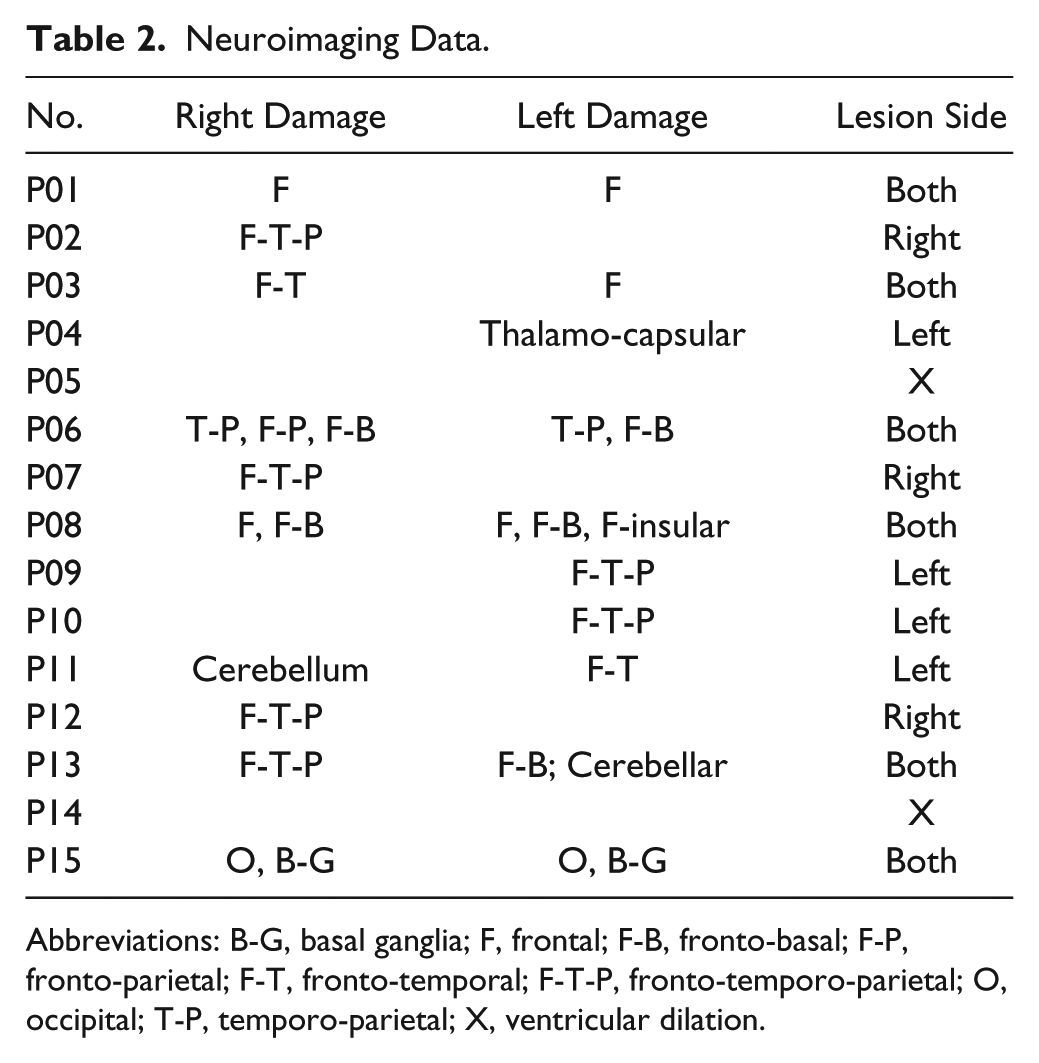
Abbreviations: B-G, basal ganglia; F, frontal; F-B, fronto-basal; F-P, fronto-parietal; F-T, fronto-temporal; F-T-P, fronto-temporo-parietal; O, occipital; T-P, temporo-parietal; X, ventricular dilation.
The brainstem auditory-evoked responses recorded on admission were preserved in all patients included in the present analysis. The CRS-R was administered prior to all EEG recording sessions, and no changes of drugs with effects on the central nervous system were performed within the last 2 weeks preceding the EEG recordings.
All patients were clinically followed up at least 1 year from the neurophysiological recording (range = 12-15 months). The follow-up included a neuropsychological evaluation for aphasia. 27 Specifically, we administered a standardized language test.27-29 The test included a picture description task, oral and written noun- and verb-naming tasks (n = 20 for noun naming—ie, topo [mouse]; n = 10 for verb naming—ie, correre [to run], dormire [to sleep]), word repetition, and reading and writing under dictation (n = 20—ie, letto [bed], tavolo [table]). The test also comprised an auditory picture-word matching task (n = 20 pictures) and a simple commands comprehension task (n = 20—ie, alzi la mano sinistra [raise your left hand], apra il libro [open the book]).27,29
Auditory Semantic Paradigm
A sentences task (implemented in and delivered by means of the Cubase Essential Software; Steinberg Media Technologies GmbH, 2008) was adopted. 18 It consisted of 100 sentences in which the last word was highly expected within the context and, thus, semantically congruent (eg, “the eel is a fish” or “a dress can be sewed”) and 100 sentences in which the last word was semantically incongruent (eg, “the eel is a bird” or “a dress can be driven”). All correct end words also appeared as incorrect end words. Congruent and incongruent sentences were presented in a pseudo-randomized order. Sentences had an average length of 1.92 (±0.38) s. Interstimulus interval between sentences was 900 ms. All stimuli were spoken by a young female Italian native speaker with a clear voice free of any dialect inflexion. All sounds in the semantic paradigms had a sampling rate of 44.1 kHz, a resolution of 32 bits, and were presented at a sound level of 70 dB. The participants were asked to just listen to the auditory stimuli that were delivered binaurally through sound isolating earphones (Shure SE-115 CL, sensitivity of 105 dB, impedance of 16Ω, and frequency range of 22 Hz to 17.5 kHz) equipped with soft flex sleeves.
EEG Data Acquisition and Data Analysis
Scalp potentials were recorded from 27 active electrodes (FP1, FP2, F7, F3, Fz, F4, F8, FC5, FCz, FC6, T7, C3, Cz, C4, T8, CP5, CP1, CP2, CP6, P7, P3, Pz, P4, P8, O1, O2, right mastoids) placed according to an extension of the 10-20 International System (GAMMAsys active electrode; Guger Technology OG, Graz, Austria). Data were online referenced to the left mastoid. Four additional electrodes were placed above and below the right eye and on the outer canthi of the 2 eyes to capture eye movements (EOG). The EEG signals were amplified (g.USBAmp; Guger Technology, Graz, Austria) band-pass filtered (0.5-70 Hz), digitized (sampling rate 512 Hz), and stored for off-line analysis (Brain Vision Analyzer suite Version 1.05.0005; Brain Products GmbH, Germany, and Matlab 2016, StatSoft Inc). All the patients included in the study underwent 1 EEG session; in 6 of them, we could perform a second retest recording session within the 24 hours immediately after the first.
Data were band-pass filtered in the range 2 to 15 Hz (IIR phase shift-free Butterworth filters with a slope of 48 dB/oct) and then segmented into [−200; 1000] ms windows according to the stimulus (last word) onset separately for congruent and incongruent sentences. A baseline correction was applied by using the signal mean value within 200 ms before stimulus onset. Artifacts were removed by means of an automatic threshold criterion (ie, signal segments exceeding 80 µV in absolute value were excluded from the analysis). Congruent and incongruent conditions were averaged according to the stimulus onset across trials for each channel and each participant. The difference waves between incongruent and congruent responses were computed for each channel. The ERP components were visually inspected by 2 independent EEG experts. The presence of N400 was judged according to the following criteria: (1) presence of a negative deflection in the time window comprised between 300 and 600 ms from the stimulus onset, with a larger negativity for incongruent versus congruent condition, preceded by ERP components such as N100, N200, and P300; (2) N400 scalp distribution mainly located over parieto-occipital areas; and (3) N400 peak value higher than the maximum value reached by the scalp potential in the prestimulus period. 30 All the 3 criteria had to be satisfied. The visual inspection was then validated by statistical assessment (for details, see Statistical Analysis).
Patient P03 in Table 1 (VS/UWS) was excluded from the following analysis because of muscular artifacts, which obscured the EEG traces. Grand average waveforms were obtained for the following different groups: healthy controls (CTRL), patients with left lesions (LEFT), patients with right lesions (RIGHT), patients with bilateral lesions (BOTH), and patients who showed aphasia (APHASIA) or did not (NOT APHASIA) at the emergence from MCS (E-MCS), during the follow-up, independent of the lesion side.
Statistical Analysis
Differences between incongruent and congruent EEG traces were statistically assessed by means of the cluster-mass procedure previously described by Maris and Oostenveld 31 in 2007, 15 both at individual and group levels. In brief, a nonparametric permutation test was used to establish the existence of a significant difference between the 2 conditions for each independent time sample, and then, a secondary nonparametric cluster method was applied to consider type I errors. As for the permutation test, the data sets relative to incongruent/congruent condition were pooled together as belonging to the same data set, then randomly partitioned several times (n = 100) in the 2 classes (incongruent/congruent) of interest without respecting the real data labels. For each random partition, the corresponding t-value was computed. Iterating the process led to the construction of a nonparametric distribution of the t-test statistic on which the t-value threshold for a significance level of .05 was extracted. Such a threshold was compared with the t-value obtained from the comparison of real incongruent/congruent conditions. If the actual t-value was higher than the threshold, it was concluded that a difference between the 2 conditions was found.
The Mann-Whitney U test (2-tailed) was used to assess the between-group (CTRL and DoC patients) differences in N400 amplitude and latency. A χ2 test was applied to test any relation between the presence/absence of the N400 waveform and the diagnosis of aphasia at the clinical follow-up. A χ2 test was also applied to test any relation between the presence of the N400 waveform and the clinical outcome (1-positive = for patients who recovered from VS/UWS to MCS or from MCS to E-MCS; 0-negative = no recovery).
The statistical analyses were conducted with the use of SPSS 16.0.1 and Matlab 2016 (StatSoft Inc).
Results
Clinical Follow-up
According to the CRS-R administered at clinical follow-up (Table 1), 3 patients (1 VS/UWS and 2 MCS) maintained the same diagnosis, 4 patients evolved from VS/UWS to MCS minus (MCS−), whereas 8 patients recovered functional communication (E-MCS). Four of these 8 patients showed some comprehension and language production deficits (ie, aphasia), as revealed by the neuropsychological testing for aphasia performed at the clinical follow-up (see Table 1). Patients diagnosed with aphasia presented an impaired verbal production characterized by anomia, circumlocutions (eg, “it makes din don, rather than bell”), verbal paraphasia (eg, pen instead of glass), neologisms (eg, “troso” instead of “topo”), and object naming deficits, whereas we found only mild comprehension deficits for complex order and long sentences. Repetition of single words was also possible in all patients.
N400 Waveforms
Grand average (GA) waveform depicted at Pz in healthy controls (CTRL) is reported in Figure 1. As expected, with regard to the reliability of the auditory paradigm, a negative deflection was found around 400 ms, which resulted in significant difference between incongruent and congruent conditions, and it was characterized by the typical centro-parietal topography (Figure 1; topographical map). The N400 peak was preceded by significant typical ERP components such as N100, N200, and P300.
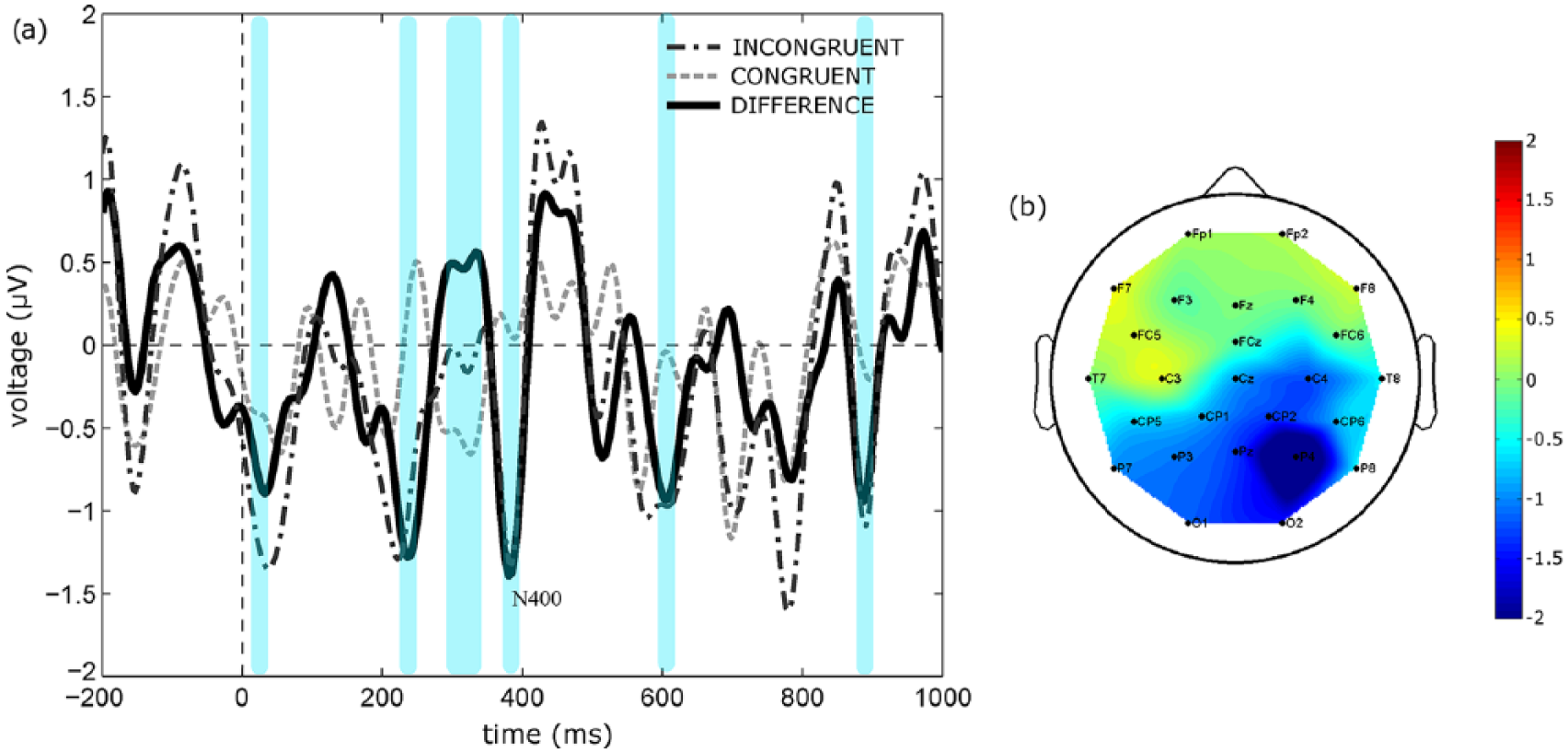
N400 in healthy controls. Panel A: Grand average of the incongruent/congruent difference waves computed at Pz (n = 10 individuals). Temporal windows in which we found a significant difference between incongruent and congruent conditions (non-parametric test, P < .05) are highlighted in light blue. Panel B: Topographical map of averaged scalp potential at N400 latency. Bar color codes for the amplitude of scalp potentials in all figures, unless otherwise specified.
Additionally, the N400 was present, as assessed by the statistical analysis, in 9 of 10 healthy controls and in 9 (4 VS/UWS and 5 MCS) of 14 patients (64%). The N400 amplitude and latency did not differ significantly between patients and controls at Pz location (Mann-Whitney U test: amplitude P = .352, latency P = .503; see Tables S1 and S2 in supplementary material). Similar results were found for Fz and Cz locations.
As illustrated in Figure 2, the E-MCS patients diagnosed with aphasia at the 1-year clinical follow-up did not display any recognizable and significant N400 during the DoC phase (Figure 2, panel A). Furthermore, a recognizable N400 in each single DoC patient with aphasia was not found (see Table 1). On the contrary, a N400 was detectable and significant in those E-MCS patients with no aphasia at the clinical follow-up (Figure 2, panel B). The N400 was located over parieto-occipital areas (topographical map in panel B in Figure 2).
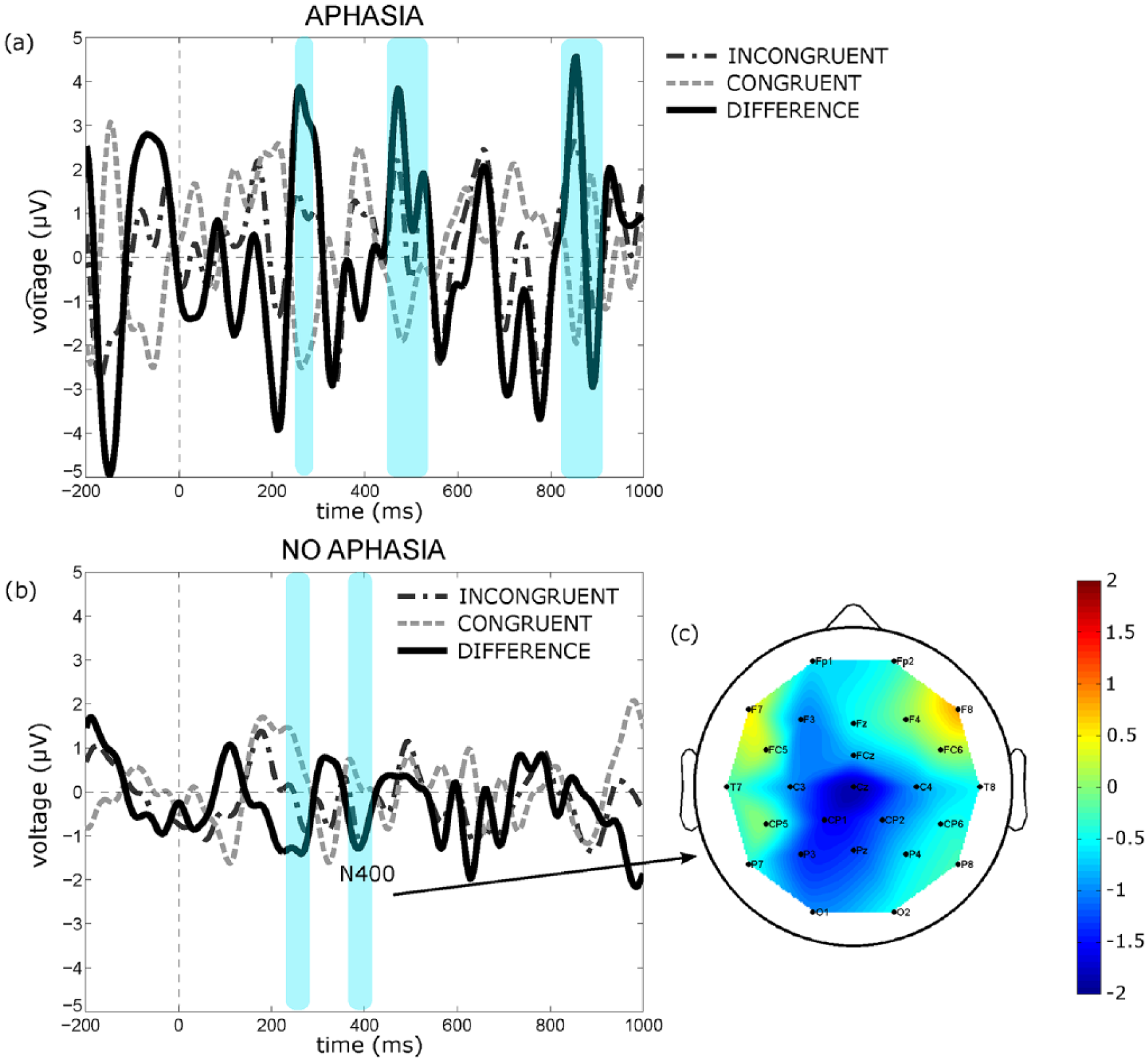
N400 in DoC patients. GA of the incongruent and congruent difference waves computed at Pz in DoC patients grouped according to the presence (panel A, Aphasia; n = 4) or not (panel B, No Aphasia; n = 4) of aphasia. Temporal windows in which we found a significant difference between incongruent and congruent conditions (nonparametric test, P < .05) are highlighted in light blue. Topographical map of averaged scalp potential at N400 latency in the No Aphasia patient group (panel C).
N400 Waveforms and Anatomical Lesions
The anatomical data in our patient sample are reported in Table 2. The GA waveforms (Pz) obtained from all DoC patients (n = 12 patients) grouped according to the lesion side (left, right, both) are illustrated in Figure 3. It can be noted that only patients with right (n = 3 patients) or bilateral (n = 5 patients) lesions (panels B and C; Right and Both) showed a significant N400 mainly located over parieto-occipital areas, and it was preceded by significant N200 and P300 components. The N400 was present in each single patient with right or bilateral lesions. In contrast, no significant N400 was found in patients with left lesions (panel A; n = 4 patients). All these patients showed significant P100 and N200 components.
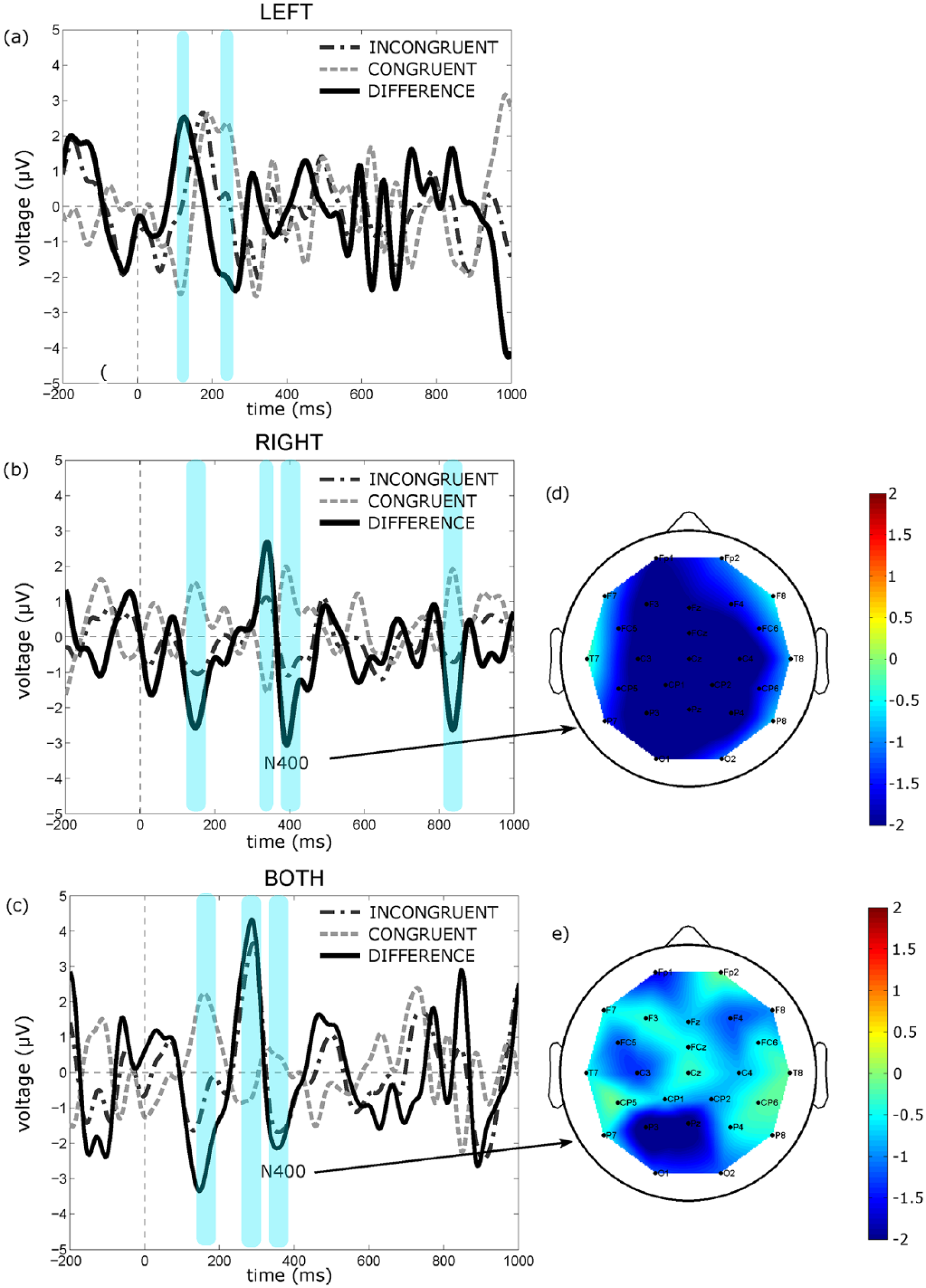
N400 in DoC patients as grouped according to the lesion side. GA of the incongruent and congruent difference waves computed at Pz: Left (panel A; n = 4), Right (panel B; n = 3) and Both (panel C; n = 5). Temporal windows in which we found a significant difference between incongruent and congruent conditions (nonparametric test, P < .05) are highlighted in light blue. Topographical map of averaged scalp potential at N400 latency in the Right and Both groups.
N400 Waveforms and Clinical Outcome at Follow-up
A significant relation between the presence/absence of N400 and the diagnosis of aphasia at the clinical follow-up was found [χ2 (df = 1) = 8.182; P = .0042]. A significant relation between the presence/absence of N400 and the recovery of consciousness and functional communication, according to the CRS-R was also found [χ2 (df =1) = 8.182; P = .0042].
Discussion
In the present study, we aimed at further defining the role of N400 ERP as a proxy for the existence of language disorders in DoC patients, otherwise detectable only on transition of DoC to a conscious communicative state. The neurophysiological assessment to unmask covert semantic language processing disorders may offer information not only to improve the reliability of the behaviorally based diagnosis of DoC, but also to address accurate rehabilitative interventions as early as possible.
To fulfill our aim, we combined information derived from the neuropsychological evaluation (focused on semantic language processing) and radiological assessment (ie, lesion side) and the presence/absence of N400 ERPs. The administration of the auditory semantic paradigm to the group of healthy individuals revealed the high reliability of such a paradigm in eliciting N400 response because the ERP was found in 90% of the enrolled individuals.
Focusing on the experimental group, we found that a significant N400 component could be detected in 64% of the DoC patients included in the study irrespective of DoC diagnosis (ie, VS/UWS, MCS). This finding is in line with previous findings, and thus, it further indicates that ERPs can be a valuable tool for an early assessment of semantic language processing in DoCs.18,19,21,22 Moreover, in our sample of DoC patients, the presence of N400 was also significantly related to the recovery of consciousness and functional communication according to CRS-R. In line with what was already found by Steppacher et al, 20 N400 presence could be indicative of a positive outcome for DoC patients—that is, consciousness recovery.
We exploratively compared healthy individuals and DoC patients in terms of N400 features. The characteristics of N400 in terms of amplitude and latency did not differ significantly between controls and DoC patients although they were not completely age matched (see supplementary Tables S1 and S2). Current available studies on N400 that investigated differences between healthy and DoC patients returned conflicting results,19,32 may be as a result of a nonhomogeneity of the experimental semantic paradigms to elicit N400.
Indeed, to our knowledge, this is the first study that correlated the presence/lack of N400 in DoC patients, diagnosed with aphasia at a long-term clinical follow-up, with recovery of consciousness and functional communication according to CRS-R.
When exploring the N400 in E-MCS patients at the clinical follow-up, it was found that those patients with a diagnosis of aphasia (as revealed by the neuropsychological assessment) did not show any recognizable and significant N400 response to the semantic paradigm at enrolment (during DoC) as compared with those with no language disorders (no aphasia; Figure 2; Table 1). This finding is further supported by the evidence of a statistical association (χ2 test) between E-MCS patients with aphasia and the absence of the N400 waveform.
Previous studies on stroke have shown robust evidence of a relationship between N400 alterations (ie, reduced amplitude, latency increase, changes in topographic distribution) and aphasia.33-35 Furthermore, when the aphasia was associated with severe comprehension deficits, patients did not show the N400 response to incongruent semantic stimuli. 36 Although preliminary, our findings in E-MCS indicate a similar relationship between language disorders (ie, aphasia) and the N400-ERP characteristics, thus providing further ground to introduce N400 evaluation in the neurophysiological screening (the so-called paraclinical tests) of DoC patients.
Interestingly, we also found that lesion side was significantly related to N400 presence (or absence) that is, no significant N400 waveform was elicited in response to a semantic paradigm in patients (all right-handed) with focal lesions exclusively in the left hemisphere (Figure 3). Several MRI studies have linked brain lesions side/site with different types of aphasia and have highlighted how aphasia is a common consequence of a brain lesion in the left hemisphere. 37 Our findings on the presence of N400 in patients showing bilateral lesions might be incongruent with the association between aphasia and lesions in the left hemisphere. Nevertheless, the neuropsychological evaluation conducted at the clinical follow-up revealed aphasia in none of the patients with bilateral lesions, thus suggesting that left hemisphere lesions in our “bilateral” patients did not involve brain areas related to the semantic language processing. The MRI imaging should be flanked by the assessment of N400 response to semantic stimuli in order to provide information on the functionality of lesional and perilesional areas and their residual ability to support processing of language stimuli.
Study Limitations
Although our findings on a long-term clinical follow-up contribute to address the challenging issue of aphasia in DoC patients, they should be treated with caution because of the small sample size of patients enrolled and the limited EEG acquisition of data (ie, only 1-2 recording sessions for each patient). This holds true also in light of the variability of N400 response to language-related stimuli at the level of the single subject reported in healthy individuals. 15
Additionally, the group of healthy individuals was not age and gender matched, although existing literature seems to exclude age, but not gender, as an interfering factor on the N400 reliability. 17 However, the healthy control group was included in our study only to confirm the reliability of the auditory paradigm utilized. Any comparison with the experimental group of patients was out of the scope of the study; we did it just exploratively.
Finally, sensibility and selectivity of the N400 ERP component to detect language disorders in DoC still needs to be assessed in large prospective longitudinal studies, including one with long-duration EEG monitoring to reliably retrieve semantic N400 features at the single-patient level.
Conclusion
Our preliminary EEG and clinical findings indicate that the N400 component could be elicited in 64% of DoC patients, and its presence was significantly associated with the recovery of consciousness and functional communication according to CRS-R. As seen at the long-term clinical follow-up, the presence of aphasia was paralleled by the absence of N400 in the DoC phase, whereas the N400 ERP was present in those DoC patients (E-MCS) who recovered functional communication with no language deficits. Overall, the side of hemispheric lesion was consistent with presence/absence of N400 and the diagnosis of aphasia.
An early detection of N400 ERP by means of bedside EEG monitoring (sequential recordings) could be instrumental in improving the accuracy of DoC diagnosis by disentangling the lack of responsiveness from the concomitance of semantic language processing disorders that may be present in DoC patients because of severe acquired brain injury. Moreover, disorder of language in DoC should be ruled out as contributing or leading factors in preventing the re-establishment of even a binary communication ability by means of novel technology, such as a brain-computer interface, which may be useful especially in patients with partially preserved language comprehension functions. Indeed, experimented functional communication paradigms in DoC patients 5 might be possible only in persons with intact semantic language processing.
Supplemental Material
figureS1 – Supplemental material for Language-Related Brain Potentials in Patients With Disorders of Consciousness
Supplemental material, figureS1 for Language-Related Brain Potentials in Patients With Disorders of Consciousness by Rita Formisano, Jlenia Toppi, Monica Risetti, Marta Aloisi, Marianna Contrada, Paola M. Ciurli, Chiara Falletta Caravasso, Giacomo Luccichenti, Laura Astolfi, Febo Cincotti and Donatella Mattia in Neurorehabilitation and Neural Repair
Supplemental Material
FORMISANO_supplementaryMaterials – Supplemental material for Language-Related Brain Potentials in Patients With Disorders of Consciousness
Supplemental material, FORMISANO_supplementaryMaterials for Language-Related Brain Potentials in Patients With Disorders of Consciousness by Rita Formisano, Jlenia Toppi, Monica Risetti, Marta Aloisi, Marianna Contrada, Paola M. Ciurli, Chiara Falletta Caravasso, Giacomo Luccichenti, Laura Astolfi, Febo Cincotti and Donatella Mattia in Neurorehabilitation and Neural Repair
Footnotes
Authors’ Note
Rita Formisano and Jlenia Toppi contributed equally to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie Grant Agreement No. 778234 (DOCMA), FIRB 2013—RBFR136E24, by Sapienza University of Rome–Progetto di Ateneo 2017 (EMBRACING), RM11715C82606455, Promobilia Foundation—2018-H1, by Ministry of Health GR-2013-02359341. This article only reflects the authors’ view, and funding agencies are not liable for any use that may be made of the information contained herein.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.