
Abstract
Background. Constraint-induced aphasia therapy (CIAT) has proven effective in patients with subacute and chronic forms of aphasia. It has remained unclear, however, whether intensity of therapy or constraint is the relevant factor. Data about intensive speech and language therapy (SLT) are conflicting. Objective. To identify the effective component of CIAT and assess the feasibility of SLT in the acute stage after stroke. Method. A total of 60 patients with aphasia (68.2 ± 11.7 years) were enrolled 18.9 days after first-ever stroke. They were randomly distributed into 3 groups: (1) CIAT group receiving therapy for 3 hours per day (10 workdays, total 30 hours); (2) conventional communication treatment group, with same intensity without constraints; and (3) control group receiving individual therapy twice a day as well as group therapy (total 14 hours). Patients were assessed pretreatment and posttreatment using the Aachener Aphasia Test (primary end point: token test) and the Communicative Activity Log (CAL). Results. Pretreatment, there were no between-group differences. Posttreatment, all groups showed significant improvements without between-group differences. Conclusion. It was found that 14 hours of aphasia therapy administered within 2 weeks as individual therapy, focusing on individual deficits, combined with group sessions has proven to be most efficient. This approach yielded the same outcome as 30 hours of group therapy, either in the form of CIAT or group therapy without constraints. SLT in an intensive treatment schedule is feasible and was well tolerated in the acute stage after stroke.
Introduction
Stroke is one of the most frequently occurring diseases in modern industrial countries, often leading to severe disabilities in its victims. As a result of stroke, patients suffer not only from impaired motor functions but also a wide range of other impairments, making them somewhat or completely reliant on caregivers. Aphasia, an acquired impairment affecting some or all language modalities, including the production and comprehension of speech, reading, and writing, is a particularly devastating condition commonly witnessed in stroke patients. As a result of a reduction in the ability to communicate, patients encounter myriad problems, ultimately resulting in a stark loss of independence and decline in social behavior. Although there is clear evidence that aphasia therapy is effective,1,2 questions remain as to the intensity of administered therapy, the preferred therapeutic approach, and its initiation with regard to stroke onset.
In regard to the intensity of administered aphasia therapy, Bhogal et al 3 found a considerable difference in intensities between effective and ineffective therapy schedules. Studies demonstrating effective therapeutic approaches provided a mean of 8.8 hours of therapy per week over a span of 11.2 weeks. Ineffective therapies, on the other hand, provided only 2 hours per week over a span of 22.9 weeks. Bhogal et al, therefore, concluded that intense therapy conducted over a short time period can improve the outcome of aphasia therapy in stroke patients, whereas lower-intensity therapy provided over a longer time period failed to show a significant therapeutic effect.
In a randomized controlled study conducted with acute aphasic stroke patients by Bakheit et al, 4 no differences between a standard speech and language therapy (SLT; 2 h/wk) and an intensive SLT (5 h/wk) could be established. It is important to note, however, that no patients from the intensive SLT group received the full amount of therapy because it could not be tolerated. Furthermore, the Cochrane Review of Brady et al 5 found a significant benefit of SLT compared with no SLT but could not identify any significant differences between the conventional and more intensive forms. The authors concluded that the higher drop-out rate from intensive SLT confounded potential benefits.
Cherney et al 6 conducted a review of both acute and chronic aphasic patients, ultimately finding no clearly identifiable differences between intensive and nonintensive therapies at the language impairment and communication activity/participation level. It must be taken into consideration that the reviewed studies were heterogeneous in treatment type, intensity and patient characteristics.
In 2001, Pulvermüller et al 7 described a new therapeutic approach (constraint-induced aphasia therapy [CIAT]) based on the principles of constraint-induced movement therapy (CIMT): constraint, shaping, and massed practice.8,9 The basis of the development of CIMT was the observation of a learned nonuse of affected limbs. 10 Learned nonuse can also be observed in aphasic patients, who often use nonverbal communication such as gesticulating or pantomiming, as compensatory strategies for their acquired language impairment.
CIAT is a form of group therapy that hinges on a card game, comparable to Quartets. To play, patients have to communicate solely in spoken words or sentences. Compensatory strategies, such as nonverbal communication, are not allowed during game play. Depending on the individual initial deficit and recovery progress, patients were encouraged to improve their communicative abilities through shaping; by switching from 1-word to 2- or 3-word sentences, they were able to achieve their respective goals. 7
The initial study by Pulvermüller et al 7 did not address the impact of treatment intensity versus treatment type. It consisted of 2 groups receiving the same therapy time of 30 to 35 hours, spread out, however, over varying time intervals: the CIAT group as massed practice over 10 days and the conventional therapy group over a time span of roughly 4 weeks.
Considering that 2 potentially significant factors were altered simultaneously—the treatment intensity and the therapeutic approach—the question remained as to which had the most impact on the results. Evidence indicated that intensity was indeed the crucial factor when administering effective aphasia therapy, as confirmed by Barthel et al 11 when comparing treatment outcomes in chronic aphasia patients using both CIAT and model-oriented aphasia therapy with identical intensity.
Modern medical infrastructure enables rehabilitation centers to admit stroke patients swiftly, with most patients starting therapy within 2 weeks. Although CIAT has proven effective in both chronic7,12,13 and subacute14,15 cases of aphasia, there exist discrepancies as to when administering any type of speech therapy should begin, thanks to the clinical definition of a subacute patient. The subacute stage of aphasia—when caused by vascular injury—begins 6 weeks after stroke with relatively stable clinical symptoms, 16 but the question remains as to what should be done with patients currently in the acute stage. Whereas it is ethically unjustifiable in many cases, withholding an adequate SLT from patients in the acute stage could be indicated when there are constraints in feasibility on the patient’s part to successfully participate in intensive therapies.4,5
The present study aims to answer the following questions:
Is the effective factor of CIAT the intensive therapy or the therapeutic approach (constraint)?
Is an intensive group SLT more effective than a less-intensive clinic-typical therapy combining individual and group therapy, and is it feasible early on after stroke?
Following the growing evidence in motor rehabilitation that massed practice and shaping rather than constraint are the key factors in therapy,17,18 we hypothesize that the crucial factor for a successful aphasia therapy is the therapeutic intensity rather than the therapeutic approach. The primary end point was the token subtest of the Aachener Aphasia Test (AAT) as a measure of the severity of aphasia. Secondary outcomes were the other AAT subtests (repetition, written language, naming, comprehension), the profile level of the AAT (weighted mean of subtest measure, taking into account reliability of the individual subtest), and the Communicative Activity Log (CAL).
Method
Participants
A total of 86 patients with aphasia were screened to be eligible for study inclusion (Figure 1). The screening was done using the AAT subtest focusing on spontaneous speech (value range = 0-5). Patients had to attain values between 1 and 4. Exclusion criteria were severe cognitive or attentional impairments, severe depression, left-handedness, severe dysarthria, apraxia of speech, severe deafness, and additional neurological diseases affecting speech (eg, Parkinson’s disease).
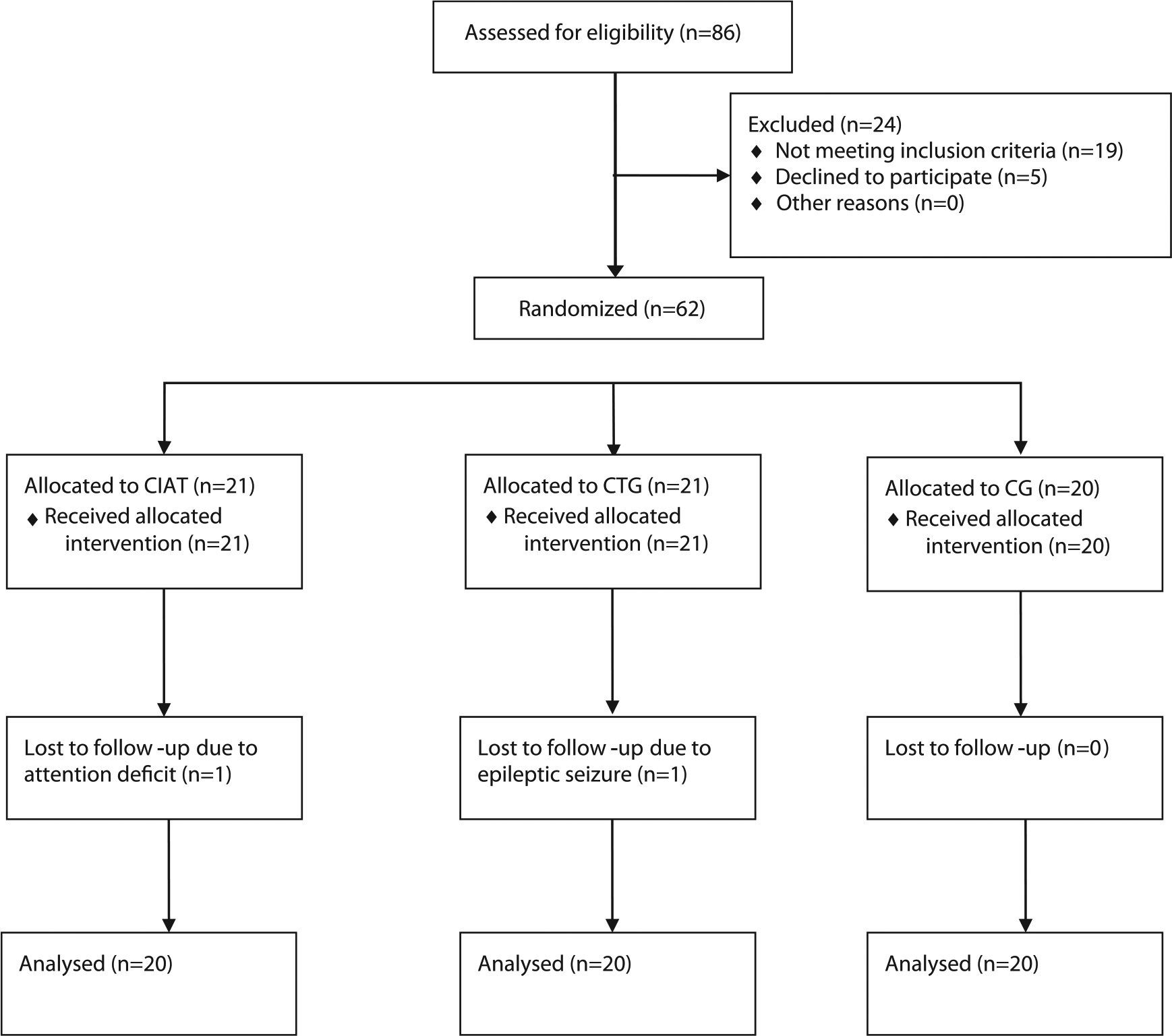
CONSORT 2010 flow diagram.
In all, 62 patients were included in the study, with 2 patients dropping out as a result of epileptic seizure and an attention deficit, respectively. Finally, 60 patients (38 female, 22 male) with a mean age of 68.2 ± 11.6 years fulfilled the study protocol and, thus, could be analyzed (for details, refer to Table 1). All patients were recruited from our rehabilitation center (Neurologisches Rehabilitationszentrum Leipzig), suffering from a first-ever stroke in the left hemisphere confirmed by cranial computed tomography or magnetic resonance imaging. Of these, 47 patients had an infarct of the middle cerebral artery and 13 a hemorrhagic stroke. The average time difference between stroke and inclusion in the study amounted to 18.9 days. All patients were native German speakers and had to be able to understand the rules of the card game played in the CIAT group, which was ensured by playing a test game. Written informed consent was given by all patients and/or their caregivers, and the study protocol was approved by the ethics committee of Leipzig University.
Patient Characteristics.
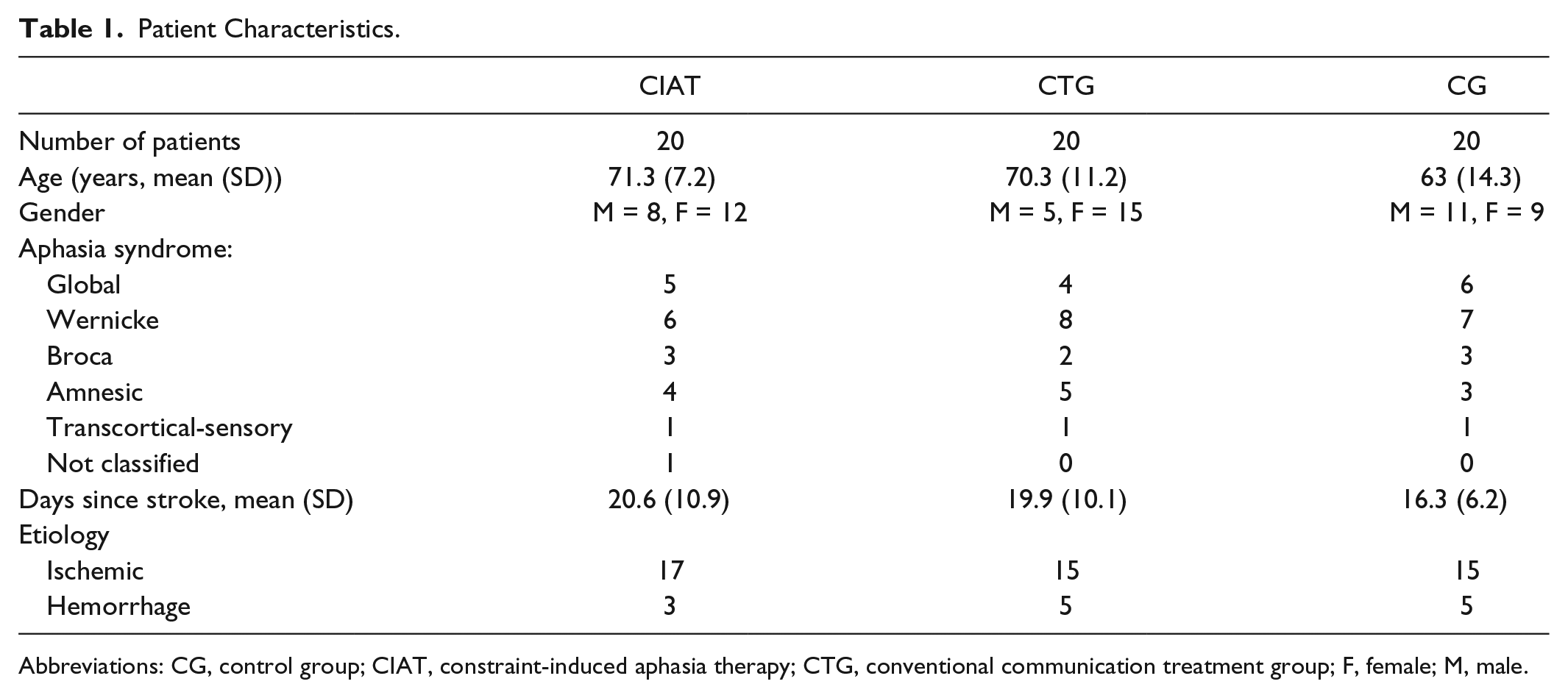
Abbreviations: CG, control group; CIAT, constraint-induced aphasia therapy; CTG, conventional communication treatment group; F, female; M, male.
Assessments
The type of aphasia, its severity, and the individual deficits of the patients were assessed by the AAT, which is the standard neurolinguistic German aphasia test battery. 19 Further assessment was done by the CAL, which was also used by Pulvermüller et al 7 and Barthel et al. 11 The CAL was adapted from the Motor Activity Log, a commonly used assessment tool in studies involving CIMT, 7 which is a 2-part questionnaire rating the amount and the quality of daily communication on a 6-point scale (0 = never, 5 = unimpaired). Assessments were completed 1 day prior to the onset of therapy as well as 1 workday after the completion of therapy and were administered by trained therapists. In an effort to keep results objective, CAL was performed twice on each assessment day by a therapist and trained nurse independently. The mean value of both CAL assessments was then analyzed by parties involved in neither randomization nor therapeutic efforts. These assessors were also blinded to the allocation of the patient and to the initial AAT or CAL assessment in its entirety.
Experimental Protocol
A single-blind, randomized controlled study with 3 arms was conducted. Randomization was achieved by using a computer-generated randomization code to 1 of the 3 arms. Codes were kept in sealed, opaque envelopes, which were then drawn by chance to allocate the patient. The respective syndrome of aphasia was not a criterion for randomization.
Patients in the CIAT arm of the study received 3 hours of CIAT therapy per day over a span of 10 workdays (30 training hours total) as group therapy. The CIAT therapy group consisted of 2 to 3 patients and 2 speech therapists who engaged with one another using the following card game: A deck of 15 to 20 identical card pairs containing pictures of everyday items, situations, or people was distributed randomly among the patients, all the while ensuring that each patient held only 1 card of the available pair. With patients visually isolated from one another by a wooden barrier, the participants were then prompted to engage with their fellow players through spoken communication only, the ultimate goal being to obtain the corresponding card of the pair from the other player(s). Whereas one therapist joined the patients in playing the game, the other observed the group, ensuring that rules were abided by, no compensatory communication mechanisms were being used, and cueing patients when necessary. Shaping elements were introduced into game play by forcing patients to include increasingly complex verbal structures into their respective interactions with one another, including but not limited to the names of the other players, polite phrases, and so on. In addition to the standard CIAT shaping mechanisms mentioned above, additional shaping elements were introduced by using playing cards with increasingly complex pictures, which were, for example, distinguishable solely by color, number of identical items, and so on.
The second arm of the study included patients who were in a conventional communication treatment group (CTG), a therapeutic approach vastly different from that of CIAT. Although the intensity of the therapy remained the same (3 h/d over a span of 10 workdays, totaling 30 training hours), several key aspects contributed to a different therapeutic approach. CTG consisted of 3 to 4 patients and 1 speech therapist, interacting with one another in such a way as to allow all types of communication, including mutual support and other forms of aid, without constraint. This type of therapy was individualized to each patient’s particular deficit, all the while keeping the principle of shaping in mind. The content of CTG was varied, with possible topics encompassing sentence completion, listening and repeating, conversation about current events, following instructions, written language training (phoneme-grapheme conversion), and word retrieval.
The control group (CG) received a clinic-typical therapeutic approach, which includes evidence-based SLT and is commonly used and widely accepted in neurological rehabilitation centers. Although it has only been evaluated empirically and never in a controlled study, its use in the third arm of this study was mainly of importance in controlling therapeutic intensity. Therapy in the CG consisted of 30 minutes of individual therapy twice a day over a span of 10 workdays (10 hours) and 1 hour of group therapy 4 times within a time span of 2 weeks (a total of 14 training hours). Whereas the content of the individual therapy was adapted to fit each patient’s unique needs in a deficit-focused manner, group therapy was administered in the same way as described above for CTG. Both forms of therapy, individual and group, addressed all communication modalities under the strict consideration of the shaping principle.
When compared with the data presented in Bhogal et al, 3 participants in this study who were in either the CIAT or CTG arms underwent 1.7 times the amount of hours of therapy per week previously described to be effective, whereas the CG arm performed 1.8 fewer hours. No patient included in this study received any additional speech or language training during the duration of the training period but participated in occupational therapy and physiotherapy regularly.
Data Analysis
Biographical data among the 3 groups was compared using 1-way analysis of variance on ranks (Kruskal-Wallis) because of the fact that the normality test (Kolmogorov-Smirnov) and the equal variance test (Brown-Forsythe) both failed. Within-group performance in AAT and CAL was tested by paired t-tests. The primary analysis of efficacy end points is based on a linear analysis of covariance model, modeling posttherapy values depending on the pretherapy value of the respective patient and type of treatment. The treatment contrasts are chosen such that CG is regarded as standard (CTG vs CG and CIAT vs CTG). For the primary end point (token test), a difference of greater than 4 (t-transformed raw values) was expected to reject the hypothesis that there are no between-group differences (null hypothesis or H0). 19 The level of significance was set to .05, and the effect size was calculated as Cohen’s d. Tests were calculated with SigmaPlot (version 13, Systat Software Inc), and the linear regression model with R (version 3.2.3).
Results
Pretreatment and posttreatment data for a total of 60 patients, 20 from each arm of the study, could be analyzed. No between-group differences concerning age, gender, time since stroke, etiology, or aphasia syndromes could be identified. Prior to treatment, neither the CAL (quantitative and qualitative) nor the AAT subtests or profile level showed any between-group differences.
The AAT failed to show any between-group differences posttreatment. According to the model, the posttreatment token test (primary end point) is predicted as follows:
6.8 + 0.94 × Pretreatment token test for CG;
6.8 + 0.94 × Pretreatment token test −1.3 for CTG; and
6.8 + 0.94 × Pretreatment token test −0.1 for CIAT.
Estimates of treatment effects (−1.3 and −0.1, respectively) are negligibly small compared with the group means. The same holds true for repetition (3.7 and 1.8), written language (0.6 and −0.2), naming (1.6 and 1.6), comprehension (−0.6 and −0.04), and profile level (1.9 and 0.9). As for the quality of communication (CAL qualitative), a significantly better performance in the CIAT arm as compared with the CTG arm was observed (15.2 + 0.9 × Pretreatment CAL qualitative −6.8, P = .049). No between-group differences in the quantity of communication were identified. Thus, the quality of communication was the only measure showing an advantage of the CIAT compared with the other therapeutic approaches, even with a weak significance.
On the within-group analysis, the CG was the only arm of the study to show highly significant improvements, with moderate effect size in all AAT subtests and subsequent profile level. Both CIAT and CTG failed to reach significance in AAT repetition, with CIAT also failing in regard to profile level (Table 2). As for the CAL, CTG was the only arm of the study that failed to show significant improvements in communication quality posttreatment. This lack of improvement in quality is contrasted by a marked increase in the amount of communication observed. In the pre-post comparisons for both CIAT and CG, highly significant improvements were identified (Table 3).
Pretest Values and Performance (as the Difference Posttest − Pretest) on the AAT (t-Transformed Raw Values) for the CIAT, CTG, and CG.
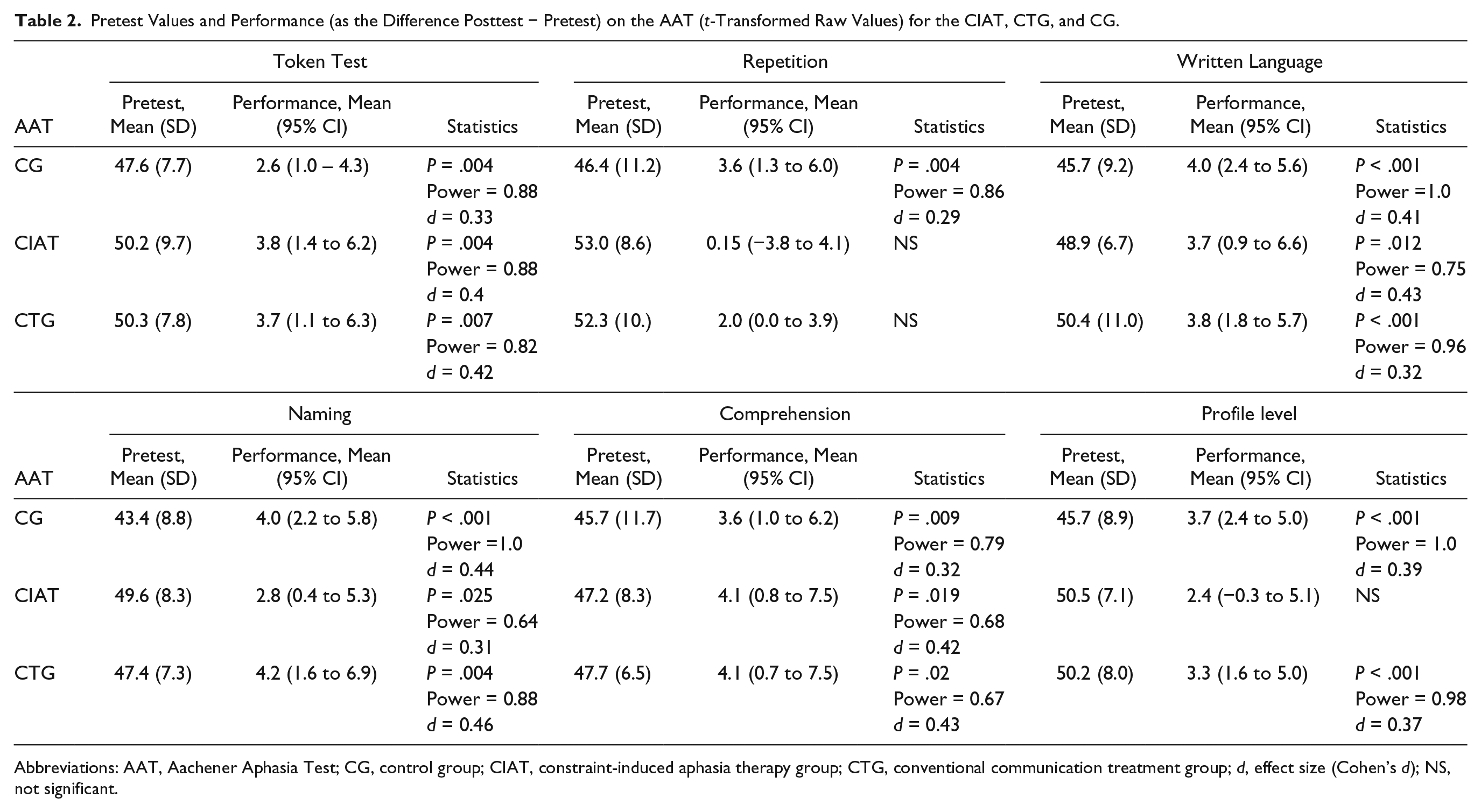
Abbreviations: AAT, Aachener Aphasia Test; CG, control group; CIAT, constraint-induced aphasia therapy group; CTG, conventional communication treatment group; d, effect size (Cohen’s d); NS, not significant.
Pretest Values and Performance (as the Difference Posttest − Pretest) on the CAL for the CIAT, CTG, and CG.
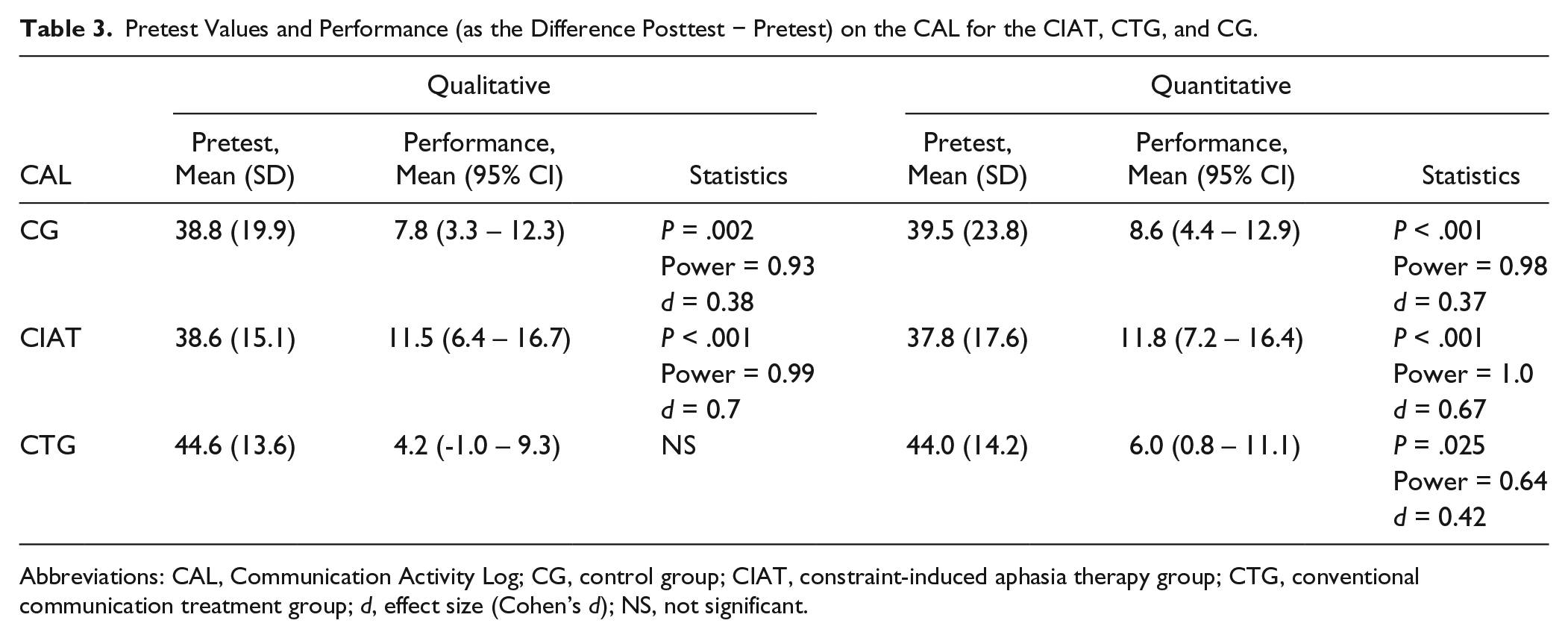
Abbreviations: CAL, Communication Activity Log; CG, control group; CIAT, constraint-induced aphasia therapy group; CTG, conventional communication treatment group; d, effect size (Cohen’s d); NS, not significant.
Discussion
The main goal driving this study was to clarify which aspect of poststroke speech therapy was most crucial in achieving significant improvement among aphasia patients: therapeutic intensity or therapeutic approach. Whereas CIAT was the first type of aphasia therapy to be adapted from principles that had long led the way in motor rehabilitation through CIMT, questions remained as to what made this approach superior. With its 3 guiding principles—intensive therapy, constraint, and shaping—there is no doubt that CIMT is a well-researched, highly effective approach.20,21
In this study, 2 of the 3 arms—CIAT and the conventional communication therapy group (CTG)—received equal amounts of SLT. The only difference between these 2 groups was the fact that the CIAT group’s therapy included constraints prohibiting the use of nonverbal communication as an aid while playing the designated card game; demographically and medically, there was no significant difference between the groups. The data clearly show significant posttherapy improvements for both groups while failing to show between-group differences in the AAT. The CIAT group, however, showed a measurably better posttherapy performance in the secondary end point—quality of communication in the CAL. The therapeutic approach of introducing constraints into a game-type setting with CIAT, although enjoyable and motivating for patients, seemingly did not have an impact on therapy outcome. Keeping these results in mind, it can, therefore, be suggested that both groups, CIAT and CTG, profited mostly from the therapeutic intensity. These conclusions are in line with the growing amount of evidence that patients generally profit from an intensive training schedule, whether that be in conjunction with motor skills, language, or other acquired impairments.11,14,22 It is interesting to note that the CG, who received a clinic-typical therapy comprising both individual and group sessions totaling 14 hours over a span of 10 days, showed results comparable to those of the CIAT and CTG arms of the study. The CG’s results were reached with less than half of the total therapy time used in either of the other 2 arms of the study. This leads to the conclusion that the combination of one-on-one therapy with a speech therapist and therapy in a group setting makes for the approach with the highest efficacy.
The starting conditions of all 3 arms of the study were the same with respect to biographical data, group composition of aphasia syndromes, and AAT and CAL score, with the CG showing a slight tendency toward a lower age in years and more acute medical conditions.
Although the CG also showed lower scores in other relevant subtests, these did not reach statistical significance and can, therefore, be neglected. Nevertheless, it cannot be fully discounted in terms of a sampling bias that the CG included more severely affected, younger patients than either CIAT or CTG. Because of the fact that the AAT is an age-corrected method and Sickert et al 14 have shown that neither age nor sex influence the degree of improvement measured by the AAT, the influence of the patient’s age on his or her results has been deemed negligible. In terms of severity, however, it has been shown by Meinzer et al 13 that more severely affected patients may profit more greatly from an intensive therapy than moderately or mildly affected patients. This was documented in a study using CIAT that ultimately showed that severely aphasic patients benefited more and scored higher on posttherapy tests, especially in the naming and repetition subtest of the AAT. However, given that therapy results of either CIAT or CTG are far removed from the normal range, it cannot be expected to witness anything resembling a ceiling effect among these patients. In this vein, the conclusion that the existing group differences may have had an impact on results is not convincing.
Therapeutic intensity is not sufficiently defined as the number of therapy hours multiplied by the total number of sessions because of the fact that the concept of dosing is not incorporated. The dose is defined as “the number of times an active ingredient or a teaching episode containing a unique combination of active ingredients occurs per session” (p. 402). 23 To compare intervention groups on this level, information such as recordings of therapy sessions is necessary, which was not done here. Keeping this in mind, the speculation that the dose per patient in an individual therapy session is higher than that of a group session was accepted. As it applies to this study in particular, the difference between the CG and the group therapies (CIAT and CTG) in therapeutic intensity per patient may be lower than expressed by therapy hours alone.
The question remains, however, as to why an intensive group therapy with 15 hours per week is less efficient than a nonintensive therapy combining both individual and group sessions with 7 hours per week. One possible explanation for this is the saturation effect, in which positive returns reach a maximum despite increased dosage. Because of the fact that stroke is a complex disease that affects several different aspects of cerebral functioning and language skills are influenced by nonlanguage capabilities such as attention capacity and memory, this is a compound issue. In stroke patients, a combination of aphasia and deficits in both attention and working memory can be identified 24 as well as the phenomenon that the explicit training of attention and memory can improve aphasic symptoms. 25 Studies concerning the cognitive predictors of aphasia therapy in the acute stage after stroke are not available.
Poeck et al 26 presented the first piece of evidence supporting a positive correlation between premorbid nonverbal intelligence and the outcome of aphasia therapy in the acute stage after stroke. Administering SLT for at least 1 h/d requires considerable attention and cognitive resourcefulness on behalf of the patient, and it could be speculated that more than 7 hours of this per week may overtax the cognitive capacities of stroke patients in the acute stage. In fact, some studies indicate that a highly intensive therapy schedule is associated with a higher drop-out rate.4,5 One of the 2 patients who dropped out of this study did so as a result of an attentional deficit that made it impossible to follow the therapy’s intensive schedule.
Another factor that contributes to the efficacy of a combination of individual and group therapy in treating aphasic patients is the fact that individual SLT meets the needs of each unique patient. Given the heterogeneous nature of aphasic patients in general and, in particular, of the patients in this study, the chance to focus on individual deficits may very well be a vital aspect in the overall success of SLT.
A definite drawback of investigating aphasic patients in the acute stage is the fact that spontaneous recovery cannot be ruled out. Considering the fact that this may be the reason for the nearly equal improvement in all groups (CIAT, CTG, and CG), it would in fact be of interest to rule out this particular factor. This cannot be done for ethical reasons, however, because the only way to accomplish this would be to test results against a CG that received no SLT. Therefore, the data presented here provide no evidence as to the effectiveness of the administered therapeutic approaches. It can only be stated that the patients improved considerably without between-group differences.
In the planning stages of this study, previously published aphasia studies were of small sample size (10 or fewer per group) and failed to provide sufficient data for a sustainable sample size calculation. This study is therefore limited by the lack of an a priori sample size calculation and the small sample size of each group. The lack of significant improvement in qualitative CAL analysis as seen in the CTG group, for instance, may be a sampling bias. It was planned to obtain long-term follow-up data, but the responder rate and the quality of data were too low for a worthwhile analysis.
In summary, aphasia therapy administered in an intensive treatment schedule is feasible and well tolerated in the acute stage after stroke, albeit not necessarily efficient; a simple increase in SLT is not always the solution. It was found that 14 hours of aphasia therapy administered within a 2-week time span combining both individual and group therapy yielded the same outcome as 30 hours of group therapy, either in the form of CIAT or group therapy without constraints. In light of the limited resources within health care systems, this is an important development that may help restructure therapeutic offerings with respect to the allocation of therapeutic resources. Although collecting such data is ambitious and not without its complications, doing so is fundamentally important to establish optimal treatment intensities of SLT for those affected.23,27
Footnotes
Acknowledgements
We are grateful to Dr Dirk Hasenclever from the Institute for Medical Informatics, Statistics and Epidemiology from the Medical Faculty of Leipzig University and Klaus Willmes from the Department of Neurology and Neuropsychology at the University Hospital RWTH Aachen, statistician and one of the authors of the AAT, for statistical advice. Our thanks are due to Tiffany Schaumburg and Christopher Maslowski for language editing. This trial has been registered on ![]() , identifier: NCT02804412.
, identifier: NCT02804412.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.