
Abstract
Background. Visuospatial neglect is a disabling syndrome with serious consequences for activities in daily life. This study investigated the effect of adaptive cueing during a reading task as a possible treatment for neglect by including (1) a task relevant for the patient’s daily life, (2) a fading out procedure to stimulate independent orientation to the left by self-cueing, and (3) a clear definition of neglect severity for the adaptive treatment protocol. Methods. A randomized controlled crossover design was used, including 26 patients from an early rehabilitation unit with left-sided visuospatial neglect after stroke or hemorrhage. They were examined twice at baseline (T1, T2), after 15 daily sessions in 1 condition (T3), and again after 15 daily sessions in the other condition (T4). The intervention condition included a daily reading task combined with endogenous and exogenous cues provided by a therapist, which were continuously reduced after a patient had reached a defined level of performance. The control condition consisted of a neuropsychological treatment of the same length, not targeting visuospatial attention. Results. Significant improvements were shown after intervention on scores for reading (word and text reading), daily life activities (Catherine Bergego Scale), Line Bisection, and the Clock Drawing Task. Conclusion. This study shows that adaptive cueing in a reading task can improve neglect symptoms by using an intensive intervention lasting 3 weeks.
Introduction
Patients with visuospatial neglect typically fail to detect stimuli on the left side of space and show specific reading impairments because of right hemispheric brain damage.1-3 The symptoms are accompanied by prolongation of inpatient rehabilitation and larger impairments in activities of daily living (ADL) when compared with stroke patients without neglect, whereas pathology and severity of motor impairment do not seem to differ. 4 An effective treatment of neglect during stroke rehabilitation is, therefore, of particular importance.
Nowadays, many studies focus on neglect treatment methods, which aim to improve bottom-up attentional processes such as prism adaptation,5,6 neck vibration,7,8 vestibular stimulation,9,10 transcranial direct current stimulation, 11 or optokinetic stimulation2,12 (see Kerkhoff and Schenk 13 for an overview). Such methods aim to manipulate sensory processing of the environment to overcome the rightward bias of neglect patients without requiring a patient’s awareness of this bias. 14
In 2013, the Cochrane Review analyzed existing methods, including top-down and bottom-up procedures, regarding efficacy for the rehabilitation of neglect. 15 Apparently, there is only limited evidence for an immediate beneficial effect of cognitive rehabilitation of neglect symptoms with current methods. The main reason for this conclusion was the paucity of studies with an appropriate methodological design. 15 Another review criticized the single use of paper-and-pencil tasks and the application of too general functional outcome measures, such as the Barthel Index, to validate the effect of a treatment method. 14
Experimental studies show that neglect patients can attend to the left if they are specifically cued or instructed to attend to the left.16,17 Cues could be exogenous (stimulus driven, bottom up) or endogenous (intrinsic, top down; see Bartolomeo and Chokron 18 for detailed definition). Initial neglect rehabilitation methods focused on procedures using left-sided visual cues, which require bottom-up and top-down attentional processes.19-22 For instance, Weinberg et al 22 developed a cueing procedure for a reading task using verbal instructions, an anchoring line, and sequentially numbered lines. The intervention group received daily training for 1 hour over a period of 4 weeks in which the extent of cueing was reduced when reading performance increased. The intervention produced a significant improvement on, among others, reading, copying, and cancellation tasks.
To develop or optimize a treatment method for neglect, in our opinion, the following points should be taken into account: First, treatment should be combined with an important task in daily life and assessed double blinded with measurements concerning ADL difficulties caused by neglect. Second, treatment should be “faded out” to stimulate an independent orientation to the left side. Third, explicit criteria for levels of neglect severity should be predefined and should structure the treatment with respect to task difficulty and adaptive cueing procedures. To our knowledge, no previous study on neglect rehabilitation included all these features.
The following study investigated the effect of adaptive cueing as a treatment for neglect by taking the considerations mentioned above into account and using a blinded, randomized controlled crossover design. Cues requiring bottom-up and top-down attentional processing were presented in a reading task. It was hypothesized that neglect will be reduced after an intervention compared with a control condition, which will be shown in reduced word omissions in word and text reading. In addition, the effect on ADL, drawing, and a bisection task was evaluated.
Materials and Methods
The data that support the findings of this study are available from the corresponding author on reasonable request. The study was registered before data acquisition at clinicaltrials.gov (identifier: NCT02945592). Patients gave written consent, and the study was approved by the Bremen Medical Board’s Ethics Committee.
Design and Procedure
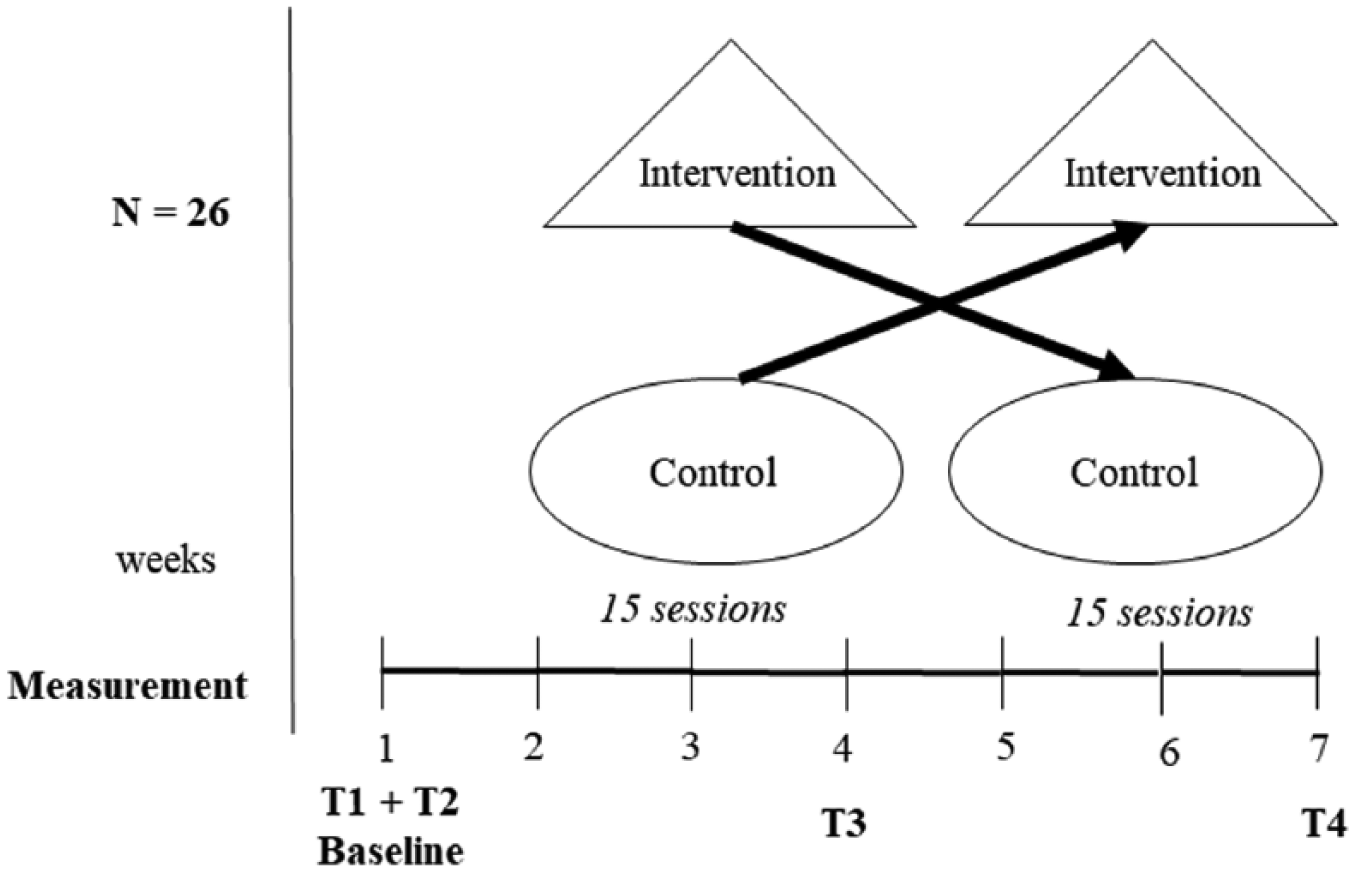
A crossover design was used: 14 patients received first the intervention condition, followed by the control condition (INTF); the order was reversed for the other 12 patients (CONF). Patients were examined twice at baseline (T1, T2), with a gap of 3 days between T1 and T2 to control for retest effects. After 15 daily sessions in 3 weeks, the evaluation of the first condition was performed immediately after the last therapy session (T3). Again 15 daily sessions in 3 weeks were performed and ended with the evaluation of the second condition (T4; see Figure 1 for an overview).
Study design.
Proper concealment was ensured by allocating patients after baseline measurement (T2) using numbered envelopes containing a patient’s assignment, which had been prepared previous to enrollment by a person external to the project. The control condition consisted of a neuropsychological treatment not specifically assessing visuospatial deficits but focusing on other deficits concerning, for example, working memory or executive functions. During the intervention and control condition, physiotherapeutic, occupational, computer-based neuropsychological, and nursing interventions were also offered to all patients, which, among other things, targeted neglect symptoms. This functional treatment is regularly presented to patients in a German rehabilitation clinic for 5 hours per day.
Outcome measures were all single blinded for patients; measurements, which were based on subjective evaluation (sitting position, Clock Drawing Test, ADL measurements), were double-blinded, including the assessor.
Treatment
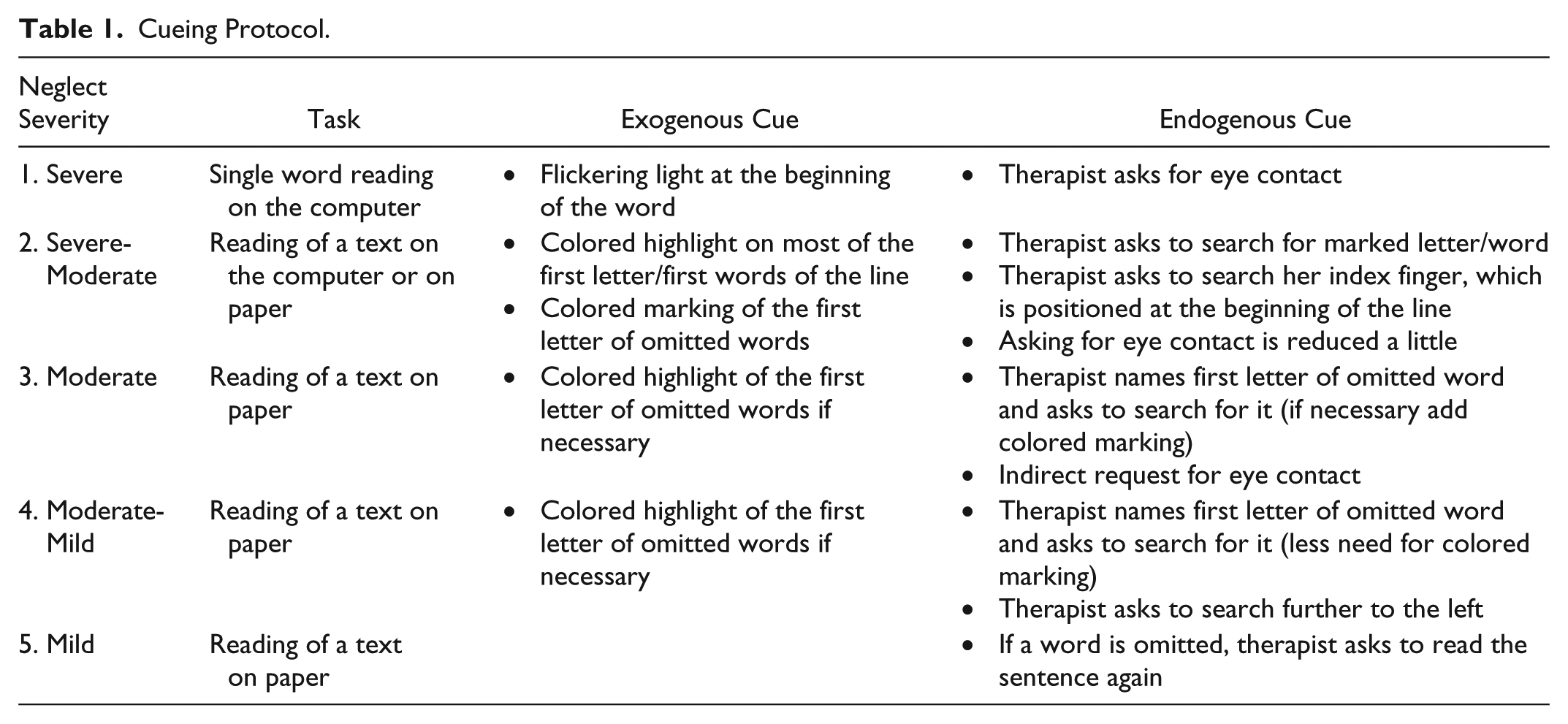
The daily treatment for the intervention group consisted of a reading task with adaptive cueing for at least 20 minutes and a maximum of 45 minutes. During this time, the therapist always sat on the left side of the patient because the therapist also functioned as a cue. Cueing consisted of visual highlights (exogenous) and verbal instructions, which require intrinsic actions (endogenous). Exogenous cues ranged from a flickering light on a dark screen to highlighted letters. Endogenous cues ranged from the instruction to create eye contact with the therapist to the instruction to read a sentence once more because of an omission. Cueing followed a predefined protocol, which provided a classification of neglect into 5 categories of severity (see Table 1 for the detailed procedure). Patients were categorized based on their reading performance and the independent implementation of the cues.
Cueing Protocol.
In the course of the therapy sessions, patients were asked to repeat and implement the verbal instructions. The instructions were continuously repeated by the therapist if the patient showed difficulties. In case of implementation, therapist-induced cues were continuously reduced.
The font type of the text was standardized to Courier New, which is characterized by consistent letter spacing (also used by Daini et al 23 ). When reading performance improved, font size and line spacing were adapted fitting the criteria of the next level of severity of the neglect. Reading material was chosen in line with a patient’s preference to keep him or her motivated during the 3 weeks. To avoid confounding by fatigue, visuospatial tasks with adaptive cueing were performed only after the reading task. The visuospatial task consisted of the arrangement of wooden pieces to a presented figure. The therapist was sitting, meanwhile, on the patient’s left side and offered, in case of omissions, the same cues as in the reading task (eg, eye contact, highlighting missing figure parts).
Measurement
Primary Outcome Measures
Reading performance was evaluated at T1 to T4 using 1 of 4 texts of 58 to 62 words, taken from the German version of the Rivermead Behavioral Memory Test (RBMT). 24 The order of the 4 texts was random. The therapist was sitting on the right side and did not use any cues during the measurement. All omissions were counted and included in the analysis. Reading errors with substituting letters without omissions were not seen as a primary neglect symptom and were not further analyzed.
In addition, the patient had to perform a word reading task. On a standard sheet of paper, the patient had to read from left to right 13 compound words, which were presented in 3 columns. Again, all word omissions were counted.
Secondary Outcome Measures
To evaluate neglect severity, a series of tests was used. The evaluation of body posture included the spontaneous sitting position in the wheelchair and the sitting position after a patient was cued by 3 questions from the left side (“How are you? How did you sleep tonight? Do you remember, what we were doing the last time?”). Spontaneous and cued body orientation were scored as follows: normal position = 0 points; modest ipsilesional deviation = 1 point; and strong ipsilesional deviation = 2 points (maximum score = 6). Both evaluations were double blinded.
The line bisection task consisted of 3 lines, each 21 cm long, 1 horizontal and 2 with a slightly different angle, and starting at slightly different directions. Patients were asked to mark the center of each line using their unaffected hand. Deviation of the true center of each line was measured in centimeters, and the mean over the 3 lines was calculated.
The Apples Cancellation Task consisted of 50 apples with either no holes, or left- or right-sided holes, presented on an A4 sheet of paper. 25 The patient was instructed to cancel out full apples and to ignore apples with left- or right-sided holes, having 5 minutes to finish the task. Omissions and false-positive reactions, separate for left- and right-sided holes, were counted.
The Clock Drawing Test is part of the Behavioral Inattention Test, in which the patient had to write the numbers 1 to 12 clockwise in an empty circle. 26 The evaluation of the drawings was blinded, and scoring was done as follows: 0 = normal, 0.5 = partially distorted, 1.0 = strongly distorted, 1.5 = left side with number omissions, 2.0 = no numbers on the left side.
All outcome measures conform to the German neurological guidelines for deficits in spatial cognition. 27 To evaluate neglect-related impairment in ADL, we obtained scores on the German version of Catherine Bergego Scale. 28 The German versions of The Functional Independence Measure as well as the Early Rehabilitation and Barthel Index were included as general measurements for ADL.29,30
All ADL measurements were assessed by the hospital staff, blinded to patient’s allocation in the study. Following a suggestion by Azouvi et al, 14 the Barthel Index Score as well as the subscores for eating and PEG supply, urinary continence, and fecal continence were removed from the analysis because they were seen as irrelevant for neglect improvement.
Descriptive Measures
Spatial working memory was evaluated at T1. Patients had to point to the direction of a pen that had been shown before by the therapist. Scoring was done as follows: 0 = no impairment or 1 = impairment. The presence of hemianopia was evaluated using the Test of Attentional Performance for Visual Field Deficit 31 and scored with 0 = no hemianopia and 1 = hemianopia.
Statistical Analysis
We used descriptive statistics to summarize data and obtain CI. To evaluate the treatment effect, we performed an analysis of covariance (ANCOVA) for repeated measurements for primary and secondary outcome measures, using Evaluation (PRE vs POST) as the within-subject and Condition (control, intervention) as the between-subject variable. Order (INTF vs CONF) was used as a covariate.
In the case of CONF, PRE consisted of measurements of T2 and POST of T3 for the control condition; for the intervention condition, PRE included all measurements of T3 and POST of T4. For INTF, PRE was T2 and POST was T3 for the condition intervention; for condition control, PRE was T3 and POST T4. Because of this procedure, the same participants were included in both conditions.
We calculated the impairment reduction for main outcome measures, which included primary outcome measures and possible significant ADL measurements. For post hoc analyses, we performed nonparametrical intragroup and intergroup testing (Wilcoxon signed-rank test, Mann-Whitney U test) correcting the P value threshold for text and word reading as well as the Catherine Bergego Scale, for P =.016. For all other outcome parameters, we followed the same line of post hoc analysis without correcting for the number of statistical tests.
A number-needed-to-treat analysis (NNT) 32 was conducted for primary outcome measures to evaluate how many patients had to be treated to ensure that at least 1 patient improves performance for at least 1 SD. Multiple regression analysis was used to test whether age, lesion size, evaluation prior to condition (PRE), or condition significantly predicted an impairment reduction for primary outcome measures.
We performed all statistical analyses using SPSS software, version 23. Based on the results of former studies from our group,6,11 we aimed for a target sample size of at least 24 patients to achieve a P ⩽.05 and a power of 0.80.
Results
Patients
A total of 26 patients with severe left-sided visuospatial neglect, recruited from the early rehabilitation unit of the hospital Bremen-Ost during the period from October 2016 until November 2017, were included in the study. Visual spatial neglect was diagnosed in a patient on the basis of a deviation of the line bisection test of at least 3 mm and omission of at least 5 apples in the Apples Cancellation Task. Only patients suffering from a cerebrovascular disease were included. The majority had a stroke of the middle and/or posterior cerebral artery. Five patients had a hemorrhage in the frontal, parietal-temporal, or basal ganglia areas. Two patients suffered from an aneurysm of the internal carotid artery or middle cerebral artery. Lesion overlapping analysis indicated that the majority of 20 patients showed lesions in the right frontoparietal areas and white matter (see Figure 2). 33

Lesion overlay: lesion overlapping using MriCron. 33 In total, 25 magnetic resonance imaging or computed tomography scans were available. Using the ch2.nii.gz template, lesion drawing was made on every sixth slide starting at Z = 46 till Z = 136. The histogram displays the number of patients with the same lesion from black (no overlay) till white (20).
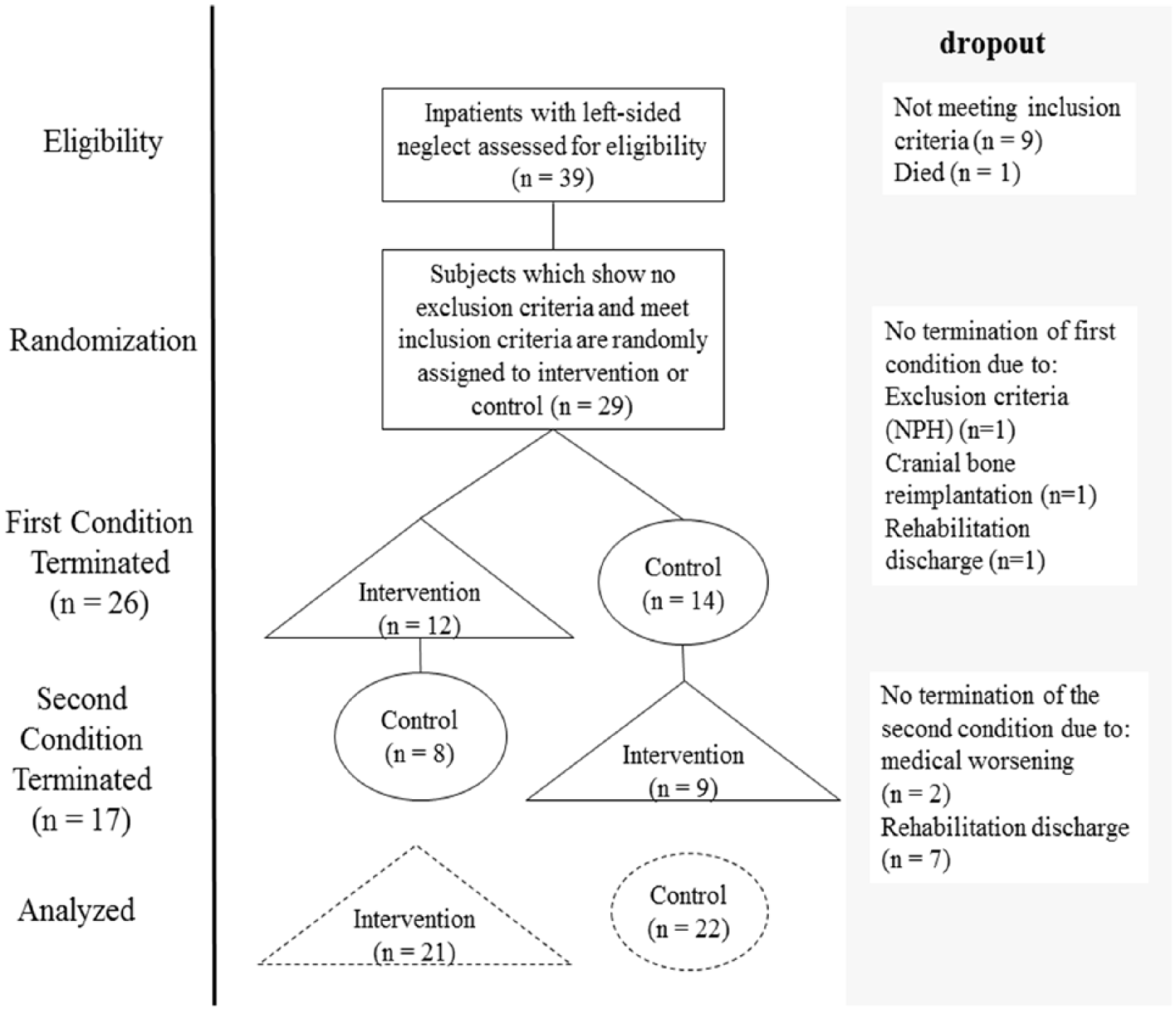
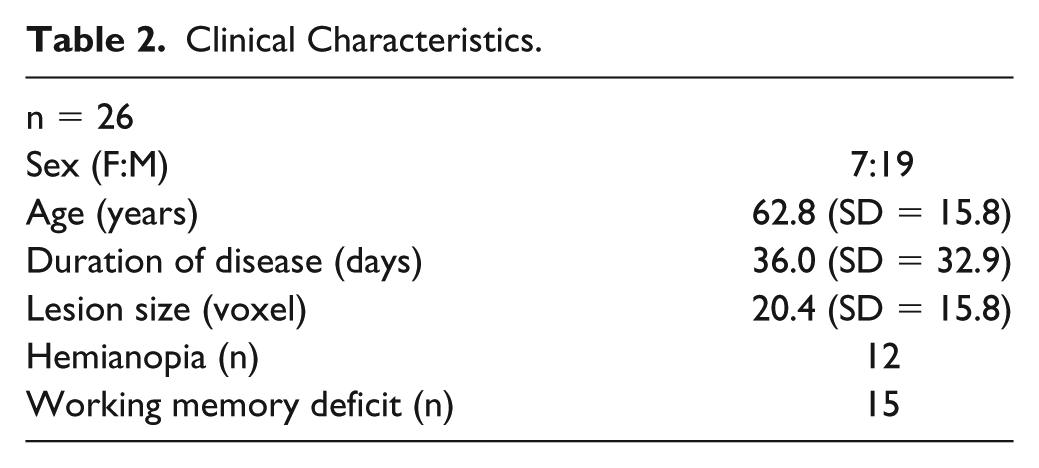
Further inclusion criteria were as follows: presence of left-sided neglect, capacity to be mobilized to the wheelchair for at least 30 minutes, and the ability to read German texts. Exclusion criteria were as follows: previously established dementia, the development of normal pressure hydrocephalus, or deterioration of the patient’s general medical condition. The exclusion criterion for data analysis was participation in less than 10 sessions of the intervention or control condition (see Figure 3 for an overview of dropouts). Time since brain lesion was not used as an inclusion or exclusion criterion. The score of the Catherine Bergego Scale (range 0-30) showed substantial ADL impairments for the neglect patients (Median = 16.4; SE = 1.6). Further demographic information is given in Table 2.
Flow diagram: 29 patients were randomized, and 3 patients did not fulfill the first condition; 7 patients did not fulfill the second condition because of rehabilitation discharge (4 started first with control).
Clinical Characteristics.
Description of Characteristics
The mean age of patients in the CONF group (9 men, 5 women) was 64.4 years (SD = 16.7) and of patients in the INTF group (10 men, 2 women) was 60.8 years (SD = 15.1). For the CONF group, the average number of days between brain lesion and admission to the study starting with control condition was 42.0 (SD = 37.0) and between brain lesion and start of intervention 60.1 (SD = 36.8). For the INTF, the average number of days between brain lesion and admission to the study was 21.5 (SD = 11.3). For the CONF group, 8 patients were diagnosed with hemianopia, and 6 showed spatial working memory deficit. For the INTF, 3 patients had additional hemianopia and 9 spatial working memory deficit. A significant difference between the days between brain lesion and beginning of the intervention condition was found (t = −3.49; CI = −61.5 to 15.8; P = .002). No effect of gender (χ2 = 0.36; P = .69), age (t = −0.60; CI = −16.1 to 8.8; P = .56), lesion size (t = −0.317; CI = −15.4 to 11.34; P = .75), days since brain lesion till admission (t = −1.57; CI = −44.1 to 5.88; P = .13), hemianopia (χ2 = 1.44; P = .28), or spatial working memory deficit (χ2 = 1.90; P = .25) was found. Furthermore, CONF and INTF did not differ in neuropsychological testing, in ADL measurements prior to condition, and with respect to their drop-out rate.
Using the Wilcoxon Test, no differences were found for the primary outcome measures of T1 and T2. For the secondary outcome measures, there was only a significant effect for the mean of the line bisection task: Z = −2.57; asymptotic significance P = .010. Small differences were to be expected because of a possible test repetition effect, and that was the reason why we included 2 time points as baseline measures. We still can assume that the time point prior to condition is reliable.
Treatment Effect
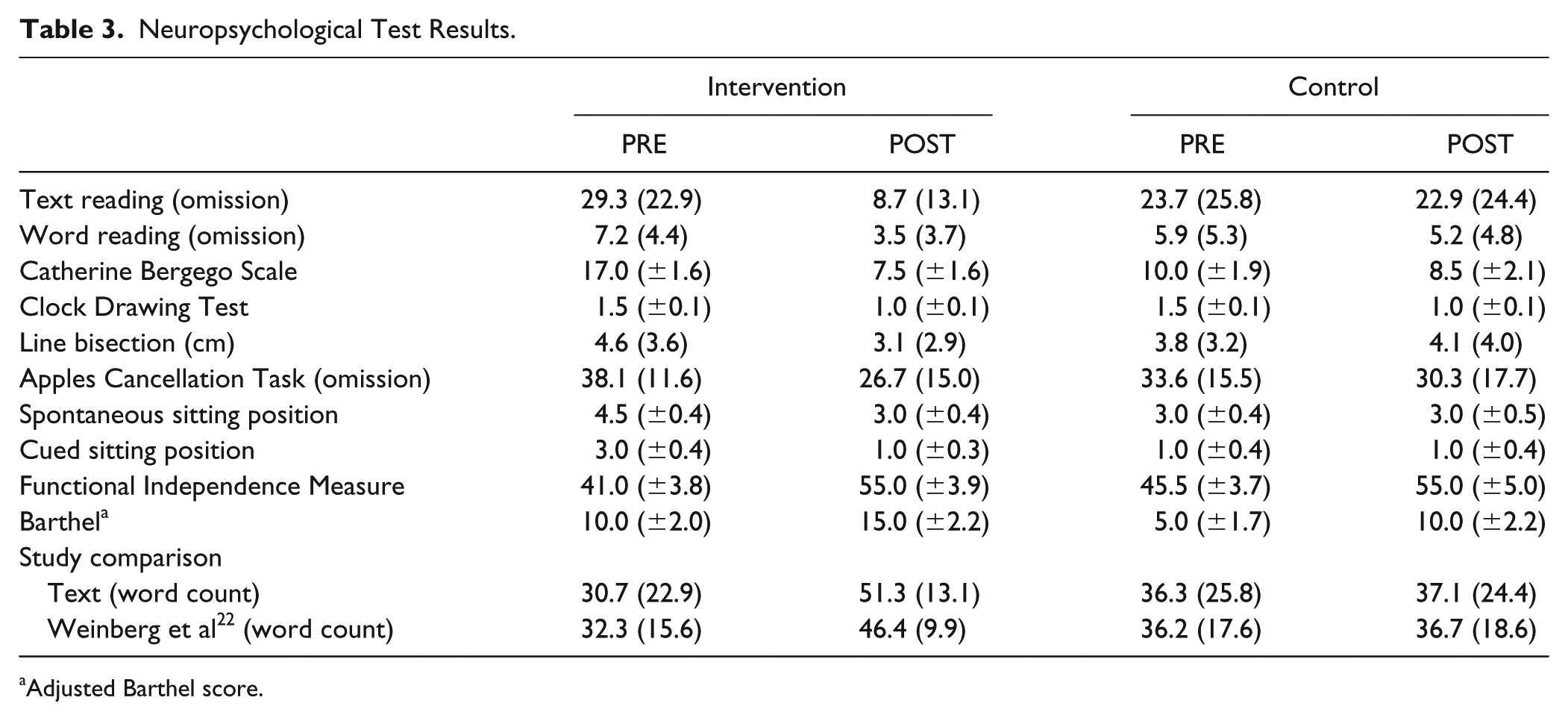
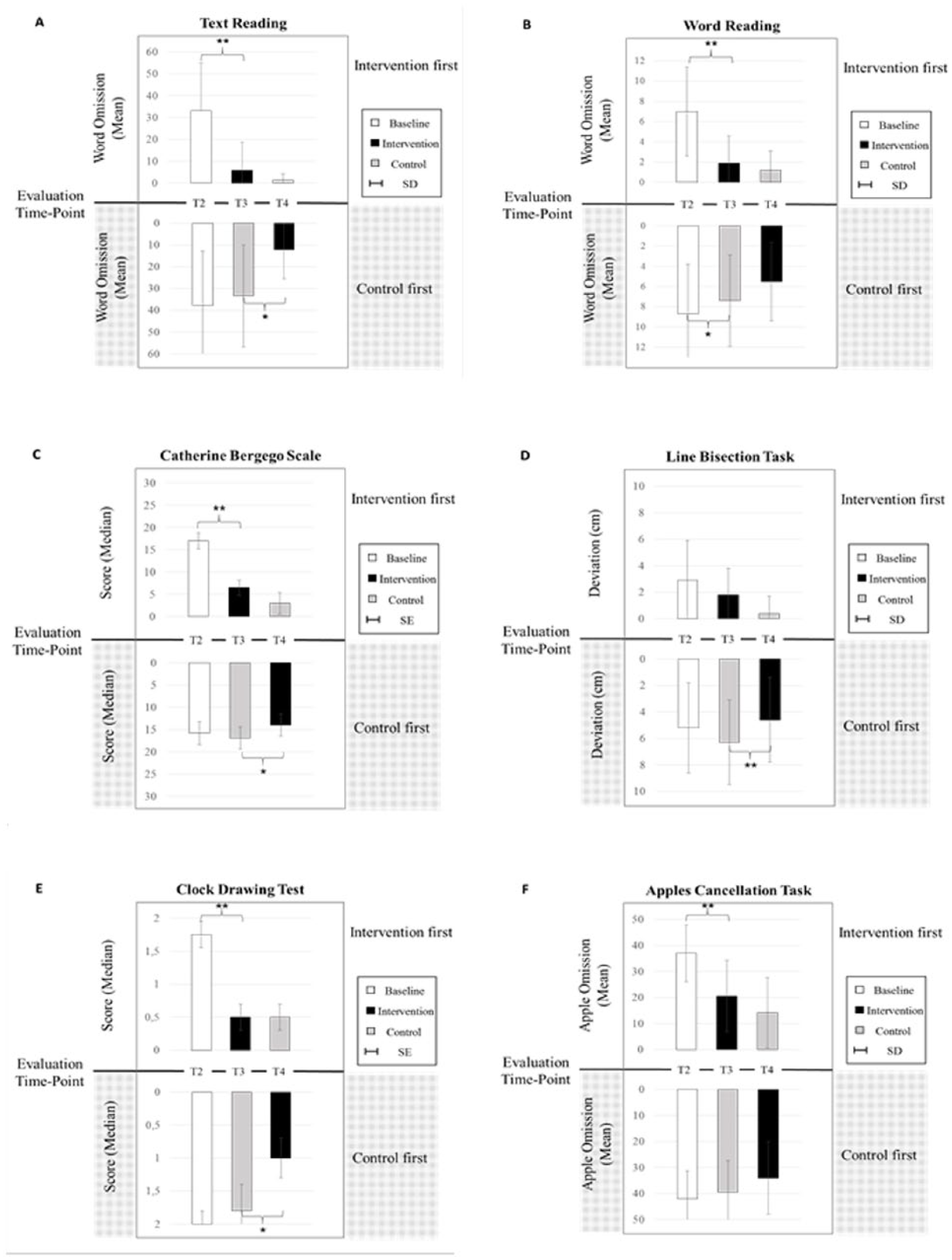
The ANCOVA yielded significant effects for the Evaluation × Condition interaction for primary outcome measures in word [F(1, 39) = 6.66; P = .014] and text reading [F(1, 39) = 9.58; P = .004]. A significant Evaluation × Condition interaction effect was observed for the mean of the Catherine Bergego Scale [F(1, 39) = 11.04; P = .002], line bisection task [F(1, 38) = 4.28; P = .045], and the Clock Drawing Test [F(1, 37) = 10.04; P = .003]. An Evaluation × Order interaction was found for the Apples Cancellation Task [F(1, 39) = 6.22; P = .017]; for an overview of all means see Table 3. Figure 4D displays the reduction in omissions in the Apples Cancellation Task. In the case of the intervention condition, the reduction is higher when the intervention is presented first (−14.9, SD = 10.0) compared with after the control condition (−5.3, SD = 6.9). Concerning the control condition, the impairment reduction was similar when control was conducted first (−4.6, SD = 9.3) or after intervention (−7.1, SD = 9.1).
Neuropsychological Test Results.
Adjusted Barthel score.
Neuropsychological test results.
Post hoc Results
The prior to control condition (PRE) includes T2 for the CONF group and T3 for the INTF group. Because at T3 patients already had intervention and start the control, PRE is on average lower in the control condition than in intervention, albeit not significantly (see Table 3).
Intergroup Comparison
For the primary outcome parameters, post hoc comparisons revealed significantly greater improvements during the intervention condition for word (T3: U = −2.90, P = .004; T4: U = −2.60, P = .008) and text reading (T3: U = −3.04; P = .002) and the Catherine Bergego Scale (T3: U = −2.56; P = .009). For the secondary outcome parameters, the Clock Drawing Test (T3: U = 2.8; P = .005), mean of deviation in the Line Bisection Task (T3: U = −3.35, P ⩽ .001; T4: U = −2.70, P = .005), and omissions of the Apples Cancellation Task (T3: U = −2.99, P = .002) showed significant differences between both conditions, pointing to a better performance of the intervention group.
Intragroup Comparison
Intervention first
Post hoc comparisons of our primary outcome parameter showed significant improvements for patients in omissions of word (Z = −2.94; P = .003) and text reading (Z = −3.06; P = .002) as well as the Catherine Bergego Scale (Z = −2.85; P = .004). As regards our secondary outcome parameter, the analysis revealed a significant improvement in spontaneous (Z = −2.9; P = .017) and cued body orientation (Z = −2.36; P = .018), the Clock Drawing Test (Z = −2.55; P = .011), and for omissions in the Apples Cancellation Task (Z = −3.06; P = .002).
Intervention second
Patients improved on our primary outcome parameter in the Catherine Bergego Scale (Z = −3.34; P = .001). Text reading was slightly above the significance threshold after correction for multiple testing (Z = −2.35; P = .019). With respect to our secondary outcome parameters, patients improved in spontaneous body orientation (Z = −2.56; P = .011), the Clock Drawing Test (Z = −2.25; P = .024), the Line Bisection Task (Z = −2.92; P = .003), and in omissions on the Apples Cancellation Task (Z = −2.94; P = .003).
Control first or control second
For patients receiving the control condition first, no significant intragroup improvements for primary and secondary outcome measures were found compared with baseline. Moreover, no significant results were obtained when control was conducted after intervention.
NNT analysis
Impairment reduction and NNT analysis were conducted for word reading (control: M = −1.3, SD = 2.7; intervention: M = −4.0, SD = 3.6; NNT = 2.5), text reading (control: M = −4.7, SD = 13.3; intervention: M = −19.2, SD = 17.8; NNT = 4.0), and the Catherine Bergego Scale (control: Median = −0.7, SE = 0.9; intervention: Median = −9.1, SE = 1.7; NNT = 3.7), showing higher impairment reduction for the intervention condition.
Multiple Regression Analysis
Multiple regression analysis was used to test if age, lesion size, Evaluation prior to condition (PRE) or Condition (intervention, control) significantly predicted the impairment reduction of word and text reading as well as of the Catherine Bergego Score. The analysis indicated that 2 predictors explained 35.8% of the corrected variance for word reading [R2 = 0.42; F(4, 41) = 6.72; P = .00] 43.9% for text reading [R2 = 0.50; F(4, 41) = 8.83; P = .00], and 35.0% for the CBS [R2 = 0.41; F(4, 42) = 6.67; P = .00]. It was found that Condition significantly predicted the impairment reduction in word reading (β = 0.36; T = 2.85; CI = 0.70 to 4.17; P = .007), text reading (β = −0.57; T = 3.64; CI = 6.56 to 23.03; P = .000), and the Catherine Bergego Scale (β = 0.44; T = 3.50; CI = 2.7 to 10.0; P = .001) as did Evaluation prior to condition (PRE; text: β = −0.57; T = −4.28; CI = −0.59 to −0.21; P = .000; Catherine Bergego Scale: β = −0.39; CI = −0.53 to −0.10; T = −0.97; P = .005).
Discussion
Based on the approximately 40-year-old publication of Weinberg et al, 22 the present study evaluated a therapy method involving a systematic cueing procedure adapted to neglect severity, using sensory bottom-up and cognitive top-down cues. The results indicate a significant reduction on all primary outcome measures, including word and text reading and even on the Catherine Bergego Scale for daily life activities, compared with the control treatment. In the intervention condition, patients improved on average 9 points on the Catherine Bergego Scale, which corresponds to almost one-third of the total score. We, therefore, found not only improvement in a task that was trained during intervention, but also far transfer effects on ADL. Improvement on the primary outcome measures and the Catherine Bergego Scale cannot be explained by factors such as age or lesion size. The Functional Independence Measure and the Early Rehabilitation Barthel Index seem to be insensitive to improvements in neglect symptoms, as previously reported by Azouvi et al. 14
Our results concerning the improvement in reading stand in line with that of Weinberg et al. 22 Their neglect patients had to read a paragraph containing 51 words, and that task is therefore comparable with the texts from the RBMT, which contain between 58 and 62 words. In the lower part of Table 3, we display the results of Weinberg et al 22 for severe neglect patients in paragraph reading along with the results of the present study in text reading. The results are very similar; reading improved after intervention using cueing, and the control groups showed no effect. However, our study also showed clear improvements in ADL as measured by the Catherine Bergego Scale, which had not been evaluated by Weinberg et al. 22 Furthermore, we presented the intervention for 3 weeks instead of 4 weeks, a reduction of 25% with at least the same efficacy, which is an economical advantage and a progress in the development of neglect treatment.
Concerning the other measurements, significant improvements for the intervention condition were observed for the line bisection task and the Clock Drawing Test (see Table 3). However, the Apples Cancellation Task showed no interaction with condition, but there was an Evaluation × Order interaction. The intervention, therefore, seems to produce an improvement in the Apples Cancellation Task, when conducted first. Figures 4A to 4C display a similar pattern for the other measurements, indicating that the intervention might be more beneficial when conducted first. This raises the question as to what might explain the difference in effectiveness of the intervention in patients who received intervention first or later after control. Because the intervention effect is smaller in the group receiving the control condition first, it is not likely that this difference in intervention effect between the arms can be explained by a transfer effect.
Dropouts resulting from rehabilitation discharge may have had an influence on the intervention effect of the patients receiving CONF because patients with a good outcome may not have been included in the intervention condition. But dropping out (n = 4) of patients as a result of rehabilitation discharge in the CONF group did not differ much from the remaining patients in this group, and therefore, it is unlikely that dropouts can explain the smaller intervention effect.
In our study, the evaluation of the days between brain lesion and inclusion in the study shows no significant difference between CONF and INTF groups. However, on average, the INTF group started around 40 days earlier with the intervention, which might have had an effect on the results. Previous studies have shown that the general rehabilitation outcome is better for patients who receive specific rehabilitation within the first 20 days after stroke compared with patients receiving specific treatment after 1 month.34,35 A review of animal studies investigating enriched environment for memory function also indicates that the moment of onset of treatment may play a role with respect to the efficacy of the treatment. 36 Therefore, the difference in time since lesion might explain the difference in treatment effect for CONF and INTF. Still, no definite answer can be given with our results. To that end, one should be able to differentiate patients according to etiology, severity, and time postonset, which would require a much larger sample.
During the control condition patients received treatment from all therapy groups assessing, among other things, visual spatial neglect. In Figure 4, we see a tendency for improvement also for the control condition. Patients show a significant improvement in word reading when control is provided first. We assume that this result is a consequence of treatment during control condition in combination with spontaneous recovery. We assume that for the control condition, more sessions would be needed to reach significant effects also in other neuropsychological tests.
As reported in previous studies, sensory and cognitive therapies may have a differential impact on different neglect symptoms.13,23 Gossmann et al 6 combined prism adaptation with a motor task. The patients improved on a test measuring egocentric symptoms, whereas there was no effect on allocentric symptoms. Similar results were found in a study combining tDCS and an optokinetic drift task, which mainly improved egocentric symptoms in left-sided neglect patients. 11 No effect was found in Volkening et al, 37 investigating only bipolar galvanic vestibular stimulation and in combination with a visual search training conducted over 2 weeks. In the present study, we combined endogenous and exogenous cues, adapted to neglect severity. Importantly, we reduced the level of cueing continuously based on the reading performance. Our results indicate that improvements are shown in a wide range of neglect aspects with relevance for a patient’s ADL capacities as assessed by the Catherine Bergego Scale. The effect of this new treatment on egocentric and allocentric neglect symptoms was not the main focus of this study. However, the results indicate that both might be affected by this intervention. Patients showed reduced omissions of text and word reading, which require both egocentric and allocentric attentional processes. Moreover, the mean deviation of the line bisection task (egocentric) and the Clock Drawing Test (allocentric) improved significantly. Because the present study shows a beneficial effect of the newly developed cueing paradigm, future studies may investigate more in detail the impact of such a treatment differentiating between egocentric and allocentric neglect symptoms.
Gialanella et al 38 showed that anosognosia may worsen prognosis of the effect of rehabilitation on neglect. Unfortunately, we did not evaluate anosognosia and, consequently, cannot assess its relevance to the rehabilitation outcome. Future studies may investigate whether anosognosia can be reduced by adaptive cueing in combination with an important task in daily life because it might lead to an increase of a patient’s awareness for his or her problem.
Furthermore, a detailed lesion analysis could be linked to neglect severity and provide information as to which patients would profit the most from the presented cueing paradigm. Because the data are available, this question will be assessed in a separate study.
Limitations of this study concern the small size of the sample. A complete double-blinded assessment for all time points was not possible because of limitations of the hospital (staff, evaluation rooms). However, 2 out of 3 double-blinded tests showed significant improvement in neglect after intervention compared with control. Our design involved 7 weeks of patient participation, which is often the maximum of inpatient stay in an early rehabilitation unit in Germany. An evaluation of long-term effects can only be accomplished outside the clinic in current rehabilitation units, in care facilities, or at home. These places provide different amounts of therapy and are, therefore, not comparable.
One may argue that in the intervention, patients practiced reading, and it may, therefore, not be surprising and that important that this function improved. We do not think that this line of reasoning is correct. First, reading is an important ADL capacity and, therefore, a significant outcome parameter in itself. Moreover, our treatment also produced far transfer effect on ADL functions (Catherine Bergego Scale), on visual search (Apples Cancellation Test), and on visuoconstruction (Clock Drawing Test). Therefore, our treatment of cueing and systematically increasing the task load achieved both major goals: an improvement on an ADL-relevant task and far transfer effects to other functions, including an ADL questionnaire.
The development of new therapy methods to treat neglect is important and should, in our opinion, not only focus on sensory manipulation, but also include cognitive strategies, which are individually adapted to the patient. Halligan et al 39 formulated it adequately, saying “redirecting” attention in a sustained fashion after right hemisphere damage is a daunting challenge for both patient and therapist. We think that the treatment of neglect is indeed a challenge but possible, if certain factors are taken into account: a combination of exogenous and endogenous cues to assess bottom-up and top-down processes, adaptation to patient’s neglect severity in a standardized procedure, continuous reduction of cues to enable independent orientation to the left as a result of self-cueing, and combination with a motivating ADL-relevant task to enable transfer, conducted in an intensive fashion as early as possible.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hans Böckler Foundation.