
Abstract
Background. Persons with anterior cruciate ligament reconstruction (ACLR) show deficits in gait and neuromuscular control following rehabilitation. This altered behavior extends to locomotor adaptation and learning, however the contributing factors to this observed behavior have yet to be investigated. Objective. The purpose of this study was to assess differences in locomotor adaptation and learning between ACLR and controls, and identify underlying contributors to motor adaptation in these individuals. Methods. Twenty ACLR individuals and 20 healthy controls (CON) agreed to participate in this study. Participants performed four cognitive and dexterity tasks (local version of Trail Making Test, reaction time test, electronic pursuit rotor test, and the Purdue pegboard). Three-dimensional kinematics were also collected while participants walked on a split-belt treadmill. Results. ACLR individuals completed the local versions of Trails A and Trails B significantly faster than CON. During split-belt walking, ACLR individuals demonstrated smaller step length asymmetry during EARLY and LATE adaptation, smaller double support asymmetry during MID adaptation, and larger stance time asymmetry during DE-ADAPT compared with CON. Conclusions. ACLR individuals performed better during tasks that required visual attention and task switching and were less perturbed during split-belt walking compared to controls. Persons with ACLR may use different strategies than controls, cognitive or otherwise, to adapt locomotor patterns.
Introduction
Anterior cruciate ligament (ACL) injury is a devastating yet unfortunately common injury amongst competitive and recreational athletes. As many as 200 000 ACL injuries occur each year in the United States, affecting roughly every 1 in 3500 individuals.1-4 Fifty percent of those individuals seek surgical reconstruction of their torn ligament in hopes of making a full recovery and returning to the same level of competitive performance. 5 Indeed, surgical repair coupled with extensive rehabilitation is the gold standard treatment in active populations to help individuals regain stability and return to previous activity levels. Unfortunately, impairments in gait may persist even after ACL reconstruction (ACLR) surgery and extensive physical rehabilitation.6-8 For example, ACLR individuals examined on return to sport clearance still showed altered gait kinematics and kinetics compared to healthy age-matched controls,7,9 indicative of potential neuromuscular control changes due to injury. Furthermore, these altered biomechanics have been observed up to a year and a half after ACLR 6 and may contribute to secondary complications, such as progression of early onset knee osteoarthritis or increased risk of reinjury.7,10,11
Much research has been conducted to help identify underlying mechanisms contributing to these persistent deficits, reinjury rates, and disabilities. ACL injury leads to subsequent neurologic and neuromuscular sequela that likely contribute to these performance differences.12-17 For example, during a force reproduction task, persons with ACLR exhibited increased frontal lobe activation compared to healthy adults suggesting these individuals may require more cognitive resources related to working memory and attention to perform the task. 12 Grooms et al 14 also reported cortical activation differences in ACLR individuals, specifically, increased activation in the secondary somatosensory area and lingual gyrus. These areas are responsible for complex integration of multiple sensory inputs, visual and sensory processing, attention, and memory. With this newfound focus on neurologic changes, such as visuomotor and attentional processing, cognitive faculties have emerged as another potential contributor to injury risk and subsequent altered locomotor control.
Many athletic and daily activities place a high demand on cognitive functions. In an athletic setting, individuals must control ball movement, track opponents, and make decisions, all while controlling their body movement. The balance between biomechanics and cognition is delicate and the tipping of prioritization toward cognition and away from biomechanics may be a contributor to many noncontact ACL injuries.18-21 When 2 attention demanding tasks are introduced, such as a motor and cognitive task, one is often prioritized over the other. In an athletic situation, when external factors (eg, opponent tracking, etc) require attention, biomechanics and motor control become more automated.22,23 Individuals may not be able to maintain appropriate balance between cognition and biomechanical functions, lending to injury and reinjury risk. Persons who later went on to injure their ACL showed slower reaction times and processing speeds prior to injury. 24 Following ACLR, Negahban et al 25 found participants exhibit impaired postural control during a single leg balance task that is further exacerbated when presented with a dual motor/cognitive task. This finding suggests when cognitive demands increase, persons with ACLR may not be able to maintain motor performance. Cognitive performance was similar between groups, 25 suggesting individuals with ACLR may either prioritize cognition or may be using cognitive faculties to aid in motor performance. Taken together these studies suggest cognitive-motor interplay may be altered in this population.
During activities of daily living and sporting performance, individuals must adapt their locomotor pattern to appropriately respond to variable environmental constraints. A popular means to investigate locomotor adaptation in the laboratory is the use of split-belt treadmills. This unique treadmill has 2 belts that can decouple and operate at different speeds, creating a novel asymmetry individuals must adapt to. Adaptation of gait parameters on the split-belt has typically been categorized as either fast (ie, limb excursion, stance time) or slow (ie, step length, double support time) adapting. 26 The split-belt treadmill has been used to assess motor adaptation and learning in a variety of populations27-29 and more recently has been applied to the ACLR population. 30 During these split-belt paradigms ACLR individuals exhibited altered motor adaptation and learning compared to healthy adults. 30 However potential contributing factors to this observed behavior have not been investigated. In light of evidence for the effect of cognition on motor control, differences in adaptation may in part be due to differences in cognitive performance between these populations. By investigating motor adaptation in combination with cognitive faculties that are most often used in sporting scenarios, such as executive function, 31 attention,31-33 reaction time, 24 and working memory,24,34 a clearer association between the 2 can be formed. Understanding this relationship may have important ramifications for ACLR rehabilitation and therefore subsequent reinjury risk. Furthermore, to account for the fact that locomotor adaptation is primarily a lower extremity adaptation task, assessment of upper extremity adaptation and motor control tasks would help discern whether this is a global phenomenon or isolated to the disrupted lower extremity. The purpose of this study was to assess differences in motor adaptation and learning between ACLR individuals and healthy adults, as well as identify underlying cognitive contributors to motor adaptation.
Methods
Subjects
Twenty persons with ACLR (12 females) and 20 age- and sex-matched controls (CON) (12 females) naïve to the split-belt were recruited to participate (Table 1). Injury and graft information for ACLR individuals is presented in Table 2. At the time of recruitment, all subjects were physically active as defined by participation in at least 30 minutes of moderate-intensity physical activity at least 2 times per week. Participants were excluded if they had an injury within the past 6 months to their back or lower extremity that limited physical activity for more than 3 days. Additionally, participants were excluded if they had any medical or neurological disorders. CON participants were excluded if they had surgery to their back or lower extremity. ACLR individuals were excluded if they had more than one ACL injury. ACLR individuals who had additional injury to their knee such as meniscus, medial cruciate ligament, or posterior cruciate ligament damage were excluded if they had multiple correction surgeries.
Demographic Results of CON and ACLR Individuals.
Abbreviations: ACLR, anterior cruciate ligament reconstruction; CON, control group.
Number of ACLR Individuals With Specific Injuries and Grafts.
Abbreviations: ACL, anterior cruciate ligament; MCL, medial cruciate ligament.
Procedures
All procedures were explained and written consent was obtained as approved by the University of Florida Institutional Review Board. Participants began by performing 4 cognitive and dexterity tasks: a local version of the Trail Making Test, a reaction time test, an electronic pursuit rotor test, and the Purdue pegboard. During Trails A and B, participants were instructed to complete the task as fast as possible without lifting their pen off the page. No verbal comments were made to the participant if they made an error (ie, skipped a number or letter). Following the Trails tests, participants completed a card-flip test to assess reaction time (CogState Ltd, Melbourne, Victoria, Australia). During the test, a deck of cards was face down on a computer screen; participants were instructed to hit a key on the keyboard as soon as the top card flipped over. Next, participants performed an electronic pursuit rotor task where they tracked a dot, or “target”, around a circle (PEBL 0.14). 35 All participants used their nonmouse hand, which was also their nondominant hand. Participants performed a total of 8 pursuit rotor adaptation trials; after split-belt walking, participants performed a total of 3 pursuit rotor retention trials. The speed of the target was adjusted for each participant so their initial time-on-target accuracy was 25% to 35%. Finally, participants performed the Purdue pegboard protocol (Lafayette Instrument Company, Lafayette, IN, USA): placing pegs with their dominant hand, nondominant hand, both hands, and creating assemblies. 36
Passive reflective markers were then placed on the participant in accordance with the Vicon Plug-In Gait full body model. Kinematic data were collected using an 8-camera, 3-dimensional motion analysis system (Vicon Motion Systems, Centennial, CO, USA) at a sampling frequency of 120 Hz. After a 10-minute treadmill accommodation period, participants walked for 5 minutes at 0.5 m/s (BASELINE). The belts then decoupled and participants walked for 15 minutes at a 3:1 split (1.5 m/s, 0.5 m/s) with their injured (ACLR) or nondominant (CON) leg on the fast belt (ADAPT). Following the split condition, participants walked with both belts moving at 0.5 m/s for 10 minutes (DE-ADAPT) and then returned to the same 3:1 split condition for 10 minutes (RE-ADAPT). Participants were asked to place their hands on the handrails while walking and look at an X on the wall directly in front of them.
Data Analysis
Gait events were automatically detected using custom-written MATLAB software (Mathworks, Natick, MA, USA) and then visually confirmed. Heel strikes were first identified relative to when the heel marker velocity switched from positive to negative in the path of progression and toe-offs were identified relative to when the toe marker velocity switched from negative to positive in the path of progression as defined by the laboratory coordinate system. Four gait cycle parameters were used to characterize kinematics: limb excursion, stance time, step length, and double support time. Limb excursion was defined as the anterior-posterior distance traveled by the ankle marker from heel-strike to toe-off.37,38 Stance time was defined as the percentage of the gait cycle between heel-strike and subsequent toe-off of the same limb. Step length was defined as the anterior-posterior distance between the ankle markers at heel-strike. Double limb support (DLS) time was defined as the time between heel-strike and subsequent toe-off of the opposite limb. Asymmetry was defined for each gait parameter using the following asymmetry index 27 :

To compare magnitude of asymmetry, gait parameter asymmetries were averaged over the last 5 strides of the BASELINE condition, the first 5 strides of the ADAPT condition (EARLY), the first 5 strides at the 7.5-minute mark of the ADAPT condition (MID), the last 5 strides of the ADAPT condition (LATE), and the first 5 strides of the DE-ADAPT and RE-ADAPT conditions. As there were no significant differences between groups at BASELINE for limb excursion, stance time, step length, or double support time asymmetries (P = .87, .40, .20, and .09, respectively), BASELINE asymmetry was removed from all subsequent conditions. This process allowed us to obtain a true magnitude of change induced by the decoupling of belts during adaptation for each participant.
Rates of adaptation for step length and double support time asymmetry were quantified as previously described by Malone et al 39 with the exception that baseline symmetry was defined as the mean±standard deviation of the last 30 strides of the BASELINE condition (not the ADAPT condition) (Figure 1). BASELINE asymmetry was included to calculate rate of adaptation. Asymmetry curves were smoothed using a moving average and binned by 3 steps. The rate of adaptation was defined as the number of steps needed to achieve 5 consecutive steps within the baseline symmetry range.
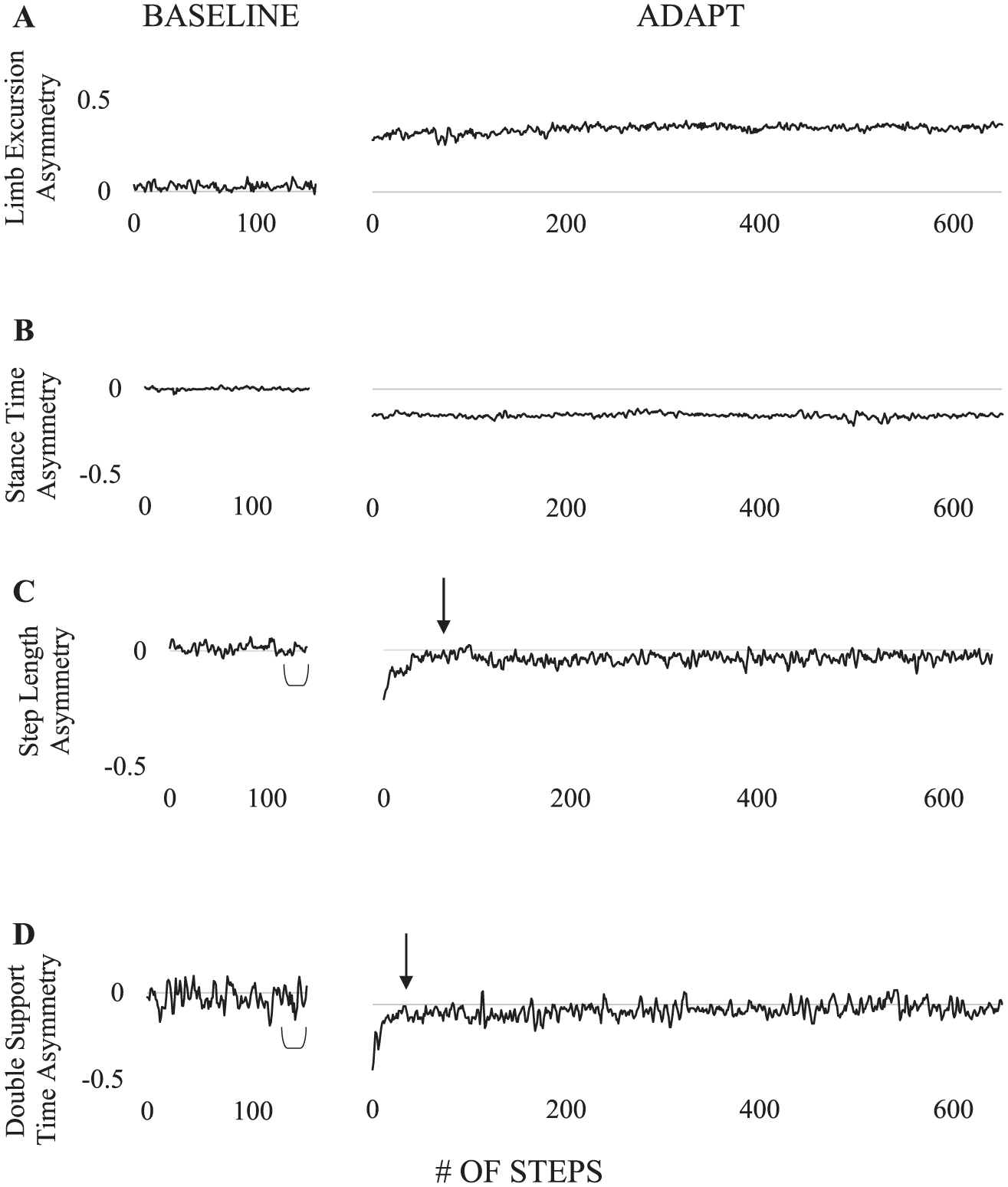
Gait parameter asymmetry values from a representative participant plotted across BASELINE and ADAPT for limb excursion (A), stance time (B), step length (C), and double support time (D). Number of steps to adapt were calculated for step length (C) and double support time (D) asymmetry. Baseline symmetry conditions were determined using the last 30 strides of the BASELINE condition (bracket). Individuals were considered adapted when they had five consecutive strides within the baseline range (arrow). For example, step length asymmetry was adapted by step 70 and double support time asymmetry was adapted by step 40 for the representative participant.
Statistical Analysis
Because participants were not asked to correct their errors during the Trail Making Test, a multivariate analysis of covariance was used to determine if differences in Trails A and B times existed between groups with number of uncorrected errors as a covariate. Four variables were used in the multivariate analysis of covarianc: Trails A time, Trails B time, Trails B time minus Trails A time, and Trails B time divided by Trails A time. An independent-samples t test was used to detect differences in reaction time between ACLR individuals and CON. A 2 × 2 (Group × Condition) repeated-measures analysis of variance was used to assess differences in pursuit rotor time-on-target during adaptation and retention. A multivariate analysis of variance was performed to analyze differences in Purdue pegboard performance across the 4 conditions (dominant hand, nondominant hand, both hands, and assembly).
A 2 × 5 (Group × Condition) repeated-measures multivariate analysis of variance was performed to analyze differences in magnitude of asymmetry for all gait parameters between the 2 groups (ACLR and CON) and the 5 conditions (EARLY, MID, LATE, DE-ADAPT, RE-ADAPT). Planned comparisons were used to examine the interaction between injury group and condition and evaluate how ACLR individuals behave differently compared with controls across conditions. Three ACLR subjects and 4 CON subjects did not return to baseline step length symmetry and thus did not have a value for rate of adaptation. One ACLR subject did not return to baseline double support time asymmetry. Therefore, 2 t tests were performed to assess differences in rate of step length and double support time asymmetry adaptation between groups. Pearson correlations were used to assess the relationship between cognitive and gait parameters. After performing statistical analyses on the dependent measures from locomotor adaptation, variables with significant differences between groups were evaluated to examine relationships between locomotor performance and cognitive and motor control faculties: Trails A and B, reaction time, and pursuit rotor adaptation and retention. CON and ACLR groups were analyzed separately for all correlations and only variables with Pearson correlation coefficients greater than or equal to 0.5 were considered. This cutoff criterion ensured only relationships with a large effect and variance greater than 25% were interpreted. 40 SPSS was used for all analyses (P ≤ .05, SPSS 24, IBM Corp, Armonk, NY, USA). Cohen’s d was calculated to determine effect size for t tests with ranges of 0.2 to 0.5 as small, 0.5 to 0.8 as medium, and greater than 0.8 as large. 41 Cohen’s f was calculated to determine effect size for analyses of variance with ranges of 0.1 to 0.25 as small, 0.25 to 0.4 as medium, and greater than 0.4 as large. 41
Results
Descriptive statistics for age, mass, height, and physical activity level were recorded (Table 1) and independent-samples t tests revealed no significant differences between groups (age, P = .80; mass, P = .32; height, P = .58; physical activity, P = .07).
Cognitive and Dexterity Tasks
There was a significant effect of group on Trail Making Test performance after controlling for number of uncorrected errors, F(3, 35) = 3.26, P = .033, Wilk’s Λ = 0.78, f2 = .28. Follow-up univariate tests revealed persons with ACLR completed the local versions of Trails A and B significantly faster than CON, F(1, 37) = 5.61, P = .023, d = 0.69 and F(1, 37) = 6.27, P = .017, d = 0.68, respectively. The CON group completed Trails A in 22.0 ± 5.6 seconds while ACLR individuals completed the test in 18.6 ± 4.2 seconds (Figure 2A). Statistically significant differences were not detected for B minus A, F(1, 37) = 1.52, P = .99, d = 0.33, or B divided by A, F(1, 37) < 0.001, P = .23, d < 0.01. Neither group had uncorrected errors during Trails A. During Trails B, ACLR individuals had 6 uncorrected errors and CON had 3 uncorrected errors which yielded no statistical significance, t(38) = −0.89, P = .38, d = 0.28. CON completed Trails B in 42.8 ± 11.0 seconds and the ACLR group completed the test in 36.3 ± 7.7 seconds. No group differences were found in reaction time during the electronic card flip, t(38) = 0.92, P = .36, d = 0.29 (Figure 2B). Furthermore, no group main effect, F(1, 38) = 0.77, P = .39, f = 0.11, or interaction, F(1, 38) = 0.17, P = .69, Wilk’s Λ = 0.99, f < 0.01, was detected for pursuit rotor (Figure 2C) and there was no significant effect of group on Purdue pegboard performance, F(4, 35) = 0.60, P = .66 Wilk’s Λ = 0.94, f2 = 0.07 (Figure 2D).
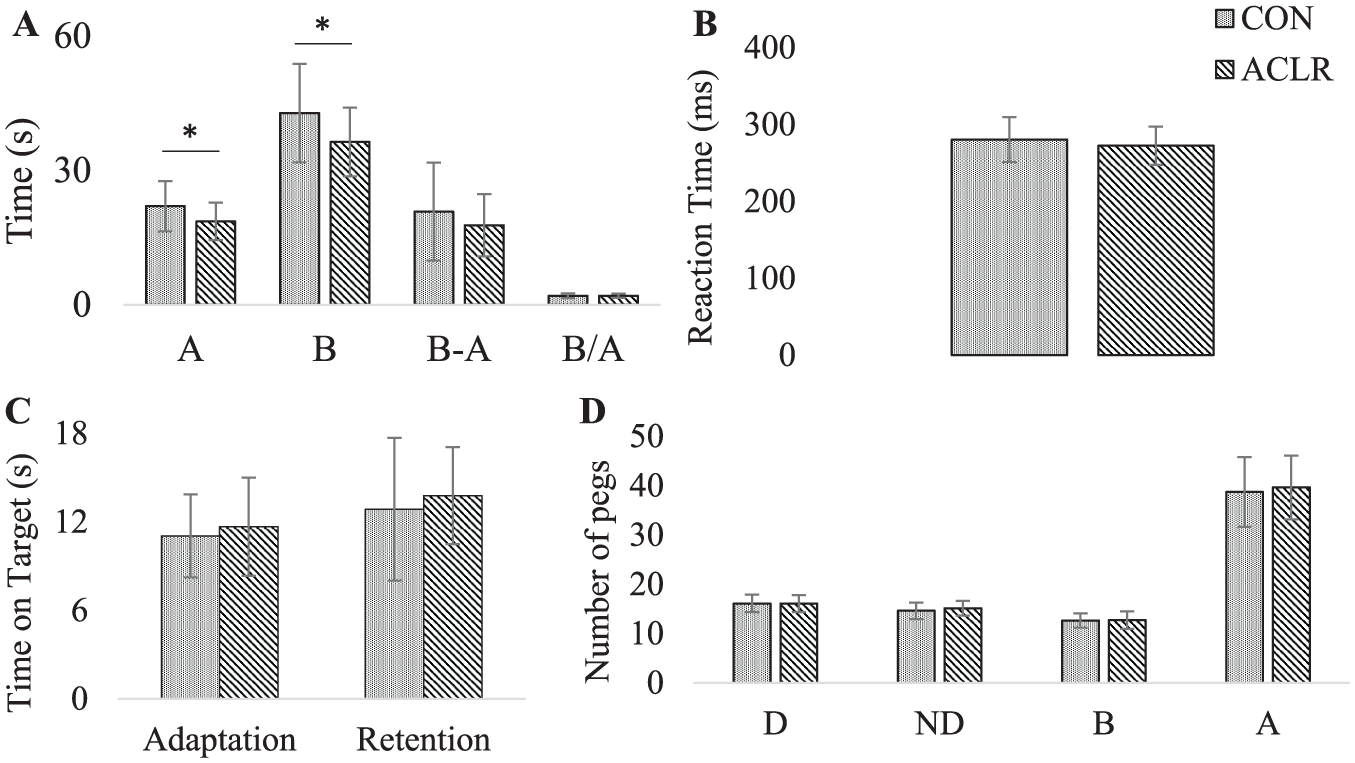
Cognitive test results for CON (presented as dots) and ACLR individuals (presented as stripes). (A) Trails A and B times in seconds, Trails B minus A, and Trails B over A. (B) Reaction time in milliseconds. (C) Pursuit rotor performance presented as average time-on-target in seconds for the adaptation and retention trials. (D) Purdue pegboard performance separated into four tests: placing pegs with dominant hand (D), non-dominant hand (ND), both hands (B), and creating assemblies (A). Asterisks indicate significance at P≤0.05 between groups.
Locomotor Adaptation
A statistically significance interaction was not detected at the multivariate level, F(16, 23) = 0.78, P = .69, Wilk’s Λ = 0.65, f2 = 0.54 or univariate level for limb excursion, F(1.83, 69.94) = 0.53, P = .57, f < .01; stance time, F(2.31, 87.76) = 1.20, P = .31, f = 0.01; step length, F(2.05, 78.04) = 1.21, P = .31, f = 0.01; or double support time asymmetry, F(2.51, 95.30) = 1.22, P = .31, f = 0.01. Although the omnibus test was nonsignificant, with an a priori hypothesis that ACLR individuals would behave differently than CON based on the condition, the interaction between group and condition was examined. When compared with CON, ACLR individuals demonstrated significantly smaller step length asymmetry in EARLY (CON: −0.24 ± 0.09, ACLR: −0.18 ± 0.09, P = .042), MID (CON: −0.09 ± 0.06, ACLR: −0.05 ± 0.07, P = .043), and LATE (CON: −0.07 ± 0.06, ACLR: −0.02 ± 0.08, P = .019) compared with CON (Figure 3C). Furthermore, ACLR individuals displayed smaller double support asymmetry during MID (CON: −0.12 ± 0.11, ACLR: −0.01 ± 0.14, P = .009) (Figure 3D) and larger stance time asymmetry during DE-ADAPT (CON: 0.01 ± 0.03, ACLR: 0.04 ± 0.05, P = .048) (Figure 3B). Though ACLR individuals and CON exhibited distinctly different patterns during ADAPT and DE-ADAPT, no group differences were present during RE-ADAPT (limb excursion: P = .43; stance time: P = .12, f = 0.013; step length: P = .90; double support time: P = .72). Finally, statistical analysis detected no differences in limb excursion asymmetry between groups during any of the conditions (Figure 3A).
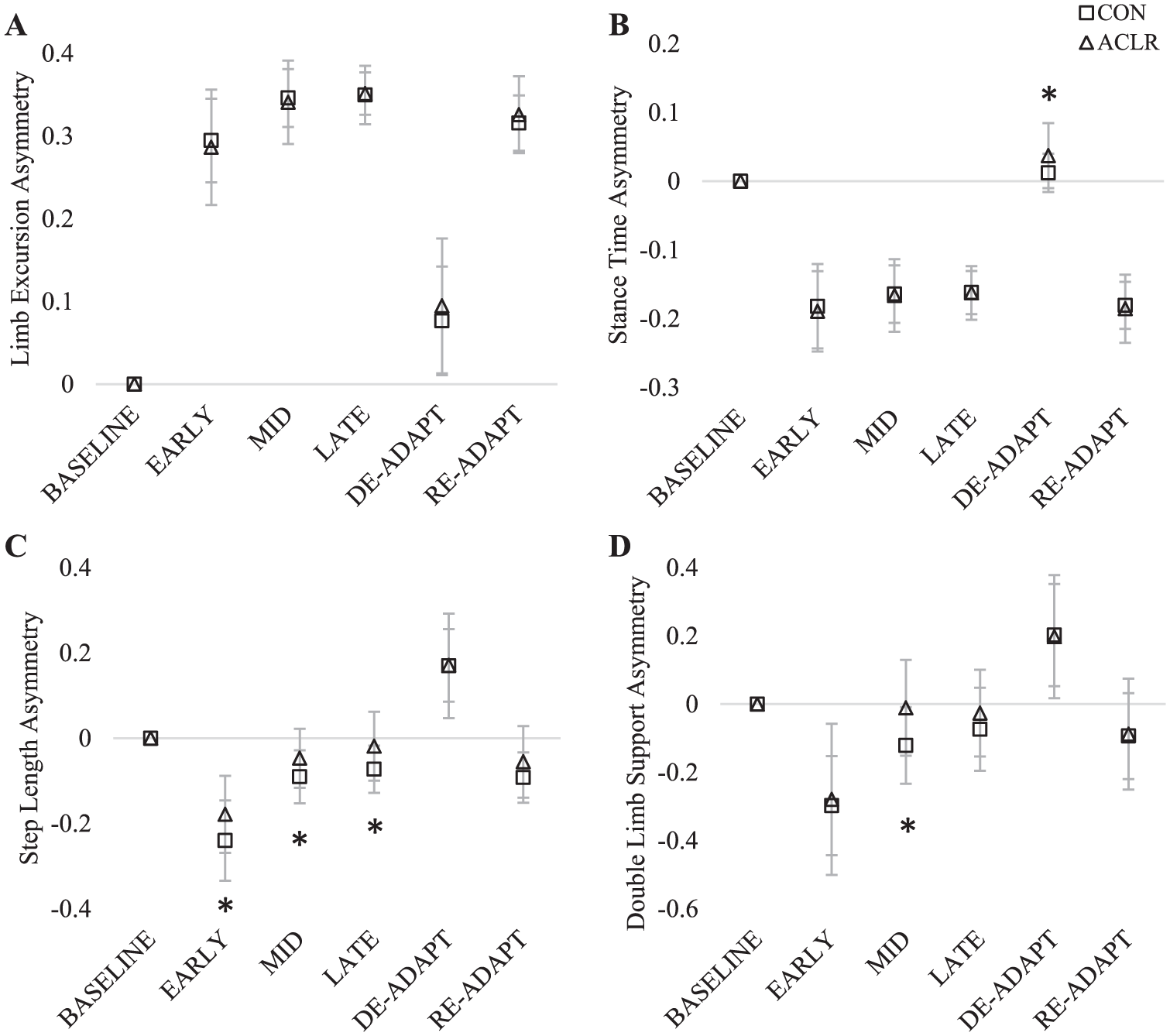
Gait parameter asymmetry scores for limb excursion (A), stance time (B), step length (C), and double support time (D) averaged over the first five strides of adaptation (EARLY), the first five strides at the seven-and-a-half-minute mark of adaptation (MID), the last five strides of adaptation (LATE), and the first five strides of the DE-ADAPT and RE-ADAPT conditions. A BASELINE asymmetry value of zero is provided for reference since BASELINE asymmetry was removed from all conditions. CON are presented as squares and ACLR individuals are presented as triangles. Asterisks indicate significance at P≤0.05 between groups.
Statistically significant differences were not detected in rate of step length asymmetry adaptation between ACLR individuals and CON during ADAPT, t(31) = −0.17, P = .87, d = 0.06; DE-ADAPT, t(36) = 1.46, P = .15, d = 0.48; or RE-ADAPT, t(31) = 0.2, P = .84, d = 0.07. No group differences were found in rate of double support time asymmetry adaptation during ADAPT, t(37) = 1.49, P = .15, d = 0.47; DE-ADAPT, t(38) = 0.36, P = .72, d = 0.11; or RE-ADAPT, t(36) = 0.28, P = .78, d = 0.09.
Relationship Between Cognition and Locomotor Adaptation
All correlation results are presented in Table 3. Step length asymmetry during EARLY was negatively correlated with reaction time and DLS asymmetry during MID was negatively correlated with pursuit rotor adaptation performance in the CON group. No locomotor adaptation parameters were correlated with cognitive performance in the ACLR group.
Correlation Results for Locomotor Adaptation and Cognitive Tests. a
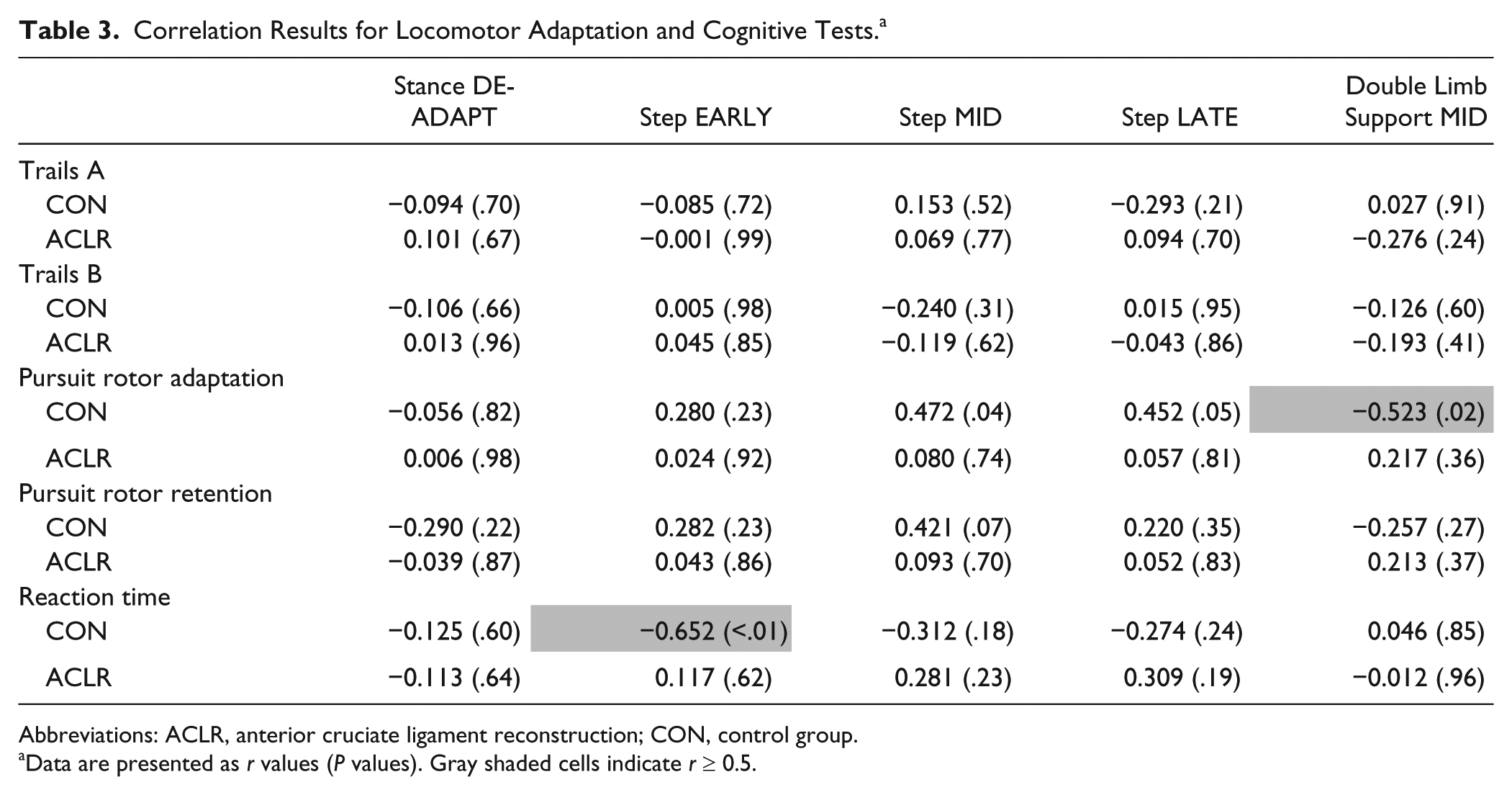
Abbreviations: ACLR, anterior cruciate ligament reconstruction; CON, control group.
Data are presented as r values (P values). Gray shaded cells indicate r ≥ 0.5.
Discussion
The primary objective of this study was to understand motor adaptation and cognitive performance differences between ACLR individuals and healthy controls, as well as the relationship between adaptation performance and cognition. Individuals with ACLR displayed improved cognitive performance during the Trail Making Test compared with CON and showed altered performance in both slow and fast adapting parameters during the locomotor task. Finally, CON and ACLR individuals exhibited different relationships between locomotor performance and cognition.
Cognition
ACLR individuals exhibited either comparable or improved cognitive performance compared with CON; individuals in the ACLR group demonstrated significantly faster Trails A and B times, indicative of better visuomotor scanning, but showed no differences in B minus A or B over A, suggesting no group susceptibility to task switching. Previous research suggests these individuals may rely more heavily on visual sensory input. During a simple knee movement task, ACLR individuals displayed increased activation of attentional and task complexity regions, 42 as well as increased activation of the lingual gyrus, an area involved in visual processing, specifically selective visual attention.13,43 If persons with an ACLR are hypervisual, they may excel in visual attention tasks by utilizing an increased amount of visual processing compared to CON. During a dual task, ACLR individuals appear to display cognitive prioritization. Persons with ACLR maintained similar cognitive performance (digit span backward) at the expense of motor performance, represented by diminished postural control when compared with healthy controls. 25 During a more challenging dual task, ACLR individuals had impaired postural control, but conversely displayed longer reaction times and more errors during an auditory Stroop test, indicative of poorer cognitive performance. 44 These 2 studies assessed different postural tests (dynamic balance versus static balance) and cognitive domains (working memory vs reaction time) which may lend to their dissimilar findings. Taken together, these results suggest ACLR individuals may be using a combination of increased visual and cognitive processing to perform the Trail Making Tests faster than CON. ACLR individuals may be able to better use visual information, such as visual inputs during balance or visual tracking of the relative belt speeds, to not only adapt but also overcome potentially reduced proprioceptive sensory input compared to CON.
Locomotor Adaptation
ACLR individuals display altered adaptive performance compared to controls, evident via altered fast and slow adapting parameters. While previous literature also observed alterations in spatiotemporal measures of locomotor adaptation, they observed differences between ACLR and CON groups at different time points and in additional spatiotemporal measures. 30 Roper et al 30 reported ACLR individuals displayed increased limb excursion asymmetry during LATE and DE-ADAPT and decreased double support time asymmetry during DE-ADAPT compared with controls, behaviors generally considered evident of worse performance in the locomotor adaptation literature. Conversely, current findings indicate ACLR individuals showed no differences in limb excursion asymmetry between groups in any condition and no differences in double support time asymmetry during DE-ADAPT. Furthermore, the present study found ACLR individuals displayed increased stance time asymmetry during DE-ADAPT, reduced step length asymmetry during the entire ADAPT condition, and reduced double support time during MID adaptation. These discrepancies in observed findings may be explained by differences in methodology and design and the aforementioned enhanced visually relevant cognitive performance of the ACLR group.
The largest contrast between the 2 studies is the use of dribble goggles. The current study did not inhibit vision in any way, while the previous study instructed participants to wear dribble goggles, which blocked visual input from their lower extremity and the treadmill belts. Without peripheral visual information, ACLR individuals in the previous study may not have been able to utilize superior visual processing to compensate and overcome their altered proprioceptive sensory input. A previous study has investigated the influence of complete visual feedback removal on locomotor adaptation; however, the impact partial occlusion may have is unknown. Future investigations are warranted to elucidate the role of visual feedback on locomotor adaptation. A secondary difference between the previous and current studies was the ratio at which the belts were decoupled. The current study used a belt speed ratio of 3:1, while the previous study used a belt speed ratio of 2:1. A belt speed ratio of 3:1 was selected as Roper et al 30 observed subtle differences in adaptation parameters and we wanted to create a larger perturbation to further challenge the locomotor control system. Reisman et al 26 have previously demonstrated that when walking at higher speed ratios with the belts decoupled, participants walked with greater asymmetries in both slow and fast adapting parameters. In sum, using a higher belt speed ratio in this study challenged the system such that different locomotor adaptation control strategies were observed in persons with ACLR compared to the previous study. Step length asymmetry was immediately reduced in the ACLR group and these individuals were able to maintain this reduced asymmetry throughout the entire ADAPT condition. While statements cannot be definitively made based on the current study, factors potentially contributing to this observation are increased use of other proprioceptive inputs (eg, hip proprioceptors) or utilization of enhanced visual feedback processing.
Relationship Between Cognition and Locomotor Adaptation
Previous literature has shown a strong relationship between cognition and adaptation. Specifically, working memory has been shown to be highly related to rate of adaptation34,45 and persons with higher working memory capacity exhibited faster rates of adaptation. 46 Additionally, response speed and decision making were shown to be related to adaptation. 47 In the current study, we related gait parameters that were significantly different between groups to cognitive tasks to investigate if (a) any parameters were related and (b) CON and ACLR groups showed different patterns of relationships. ACLR and CON groups displayed differing relationships between cognition and adaptation. CON participants had a negative correlation between reaction time and step length asymmetry during EARLY adaptation, meaning individuals with a faster reaction time tended to walk with greater step length asymmetry during initial adaptation. This result is surprising given reaction time was previously found to be directly related to adaptation. 47 CON participants also showed a negative correlation between pursuit rotor adaptation and DLS asymmetry during MID adaptation, indicating a higher time-on-target was associated with a smaller DLS asymmetry. In many respects, both pursuit rotor and split-belt adaptation are largely measures of motor learning processes used to alter spatiotemporal elements of task performance. Other correlations relating pursuit rotor performance and locomotor adaptation had r values just less than 0.5 and thus were not considered for statistical analysis. These findings suggest a potential relationship between upper and lower extremity motor adaptation and learning, though additional investigations should be performed in a larger population to elucidate this relationship. The ACLR group showed no relationships between cognitive and adaptive parameters. These results indicate ACLR individuals may use other components of cognition not herein investigated to adapt on the split-belt treadmill.
Limitations
The present study is not without limitations. The current investigation did not limit time since injury or surgery, only that ACLR participants needed to be cleared for full unrestricted activity. Additionally, no limitations on graft type were enforced. Though all these demographics were recorded and reported, there were not enough ACLR participants in subgroups to warrant further decomposition. However, previous research has shown no consistent relationship between graft type and occurrence of reinjury, knee pain, or osteoarthritis.48-50
Conclusions
This is the first study to report both lower and upper extremity adaptation and motor control tasks, as well as assess the relationship between adaptation and cognition, in individuals with ACLR. Three findings emerged from this study: (a) ACLR individuals perform better during tasks that require visual attention and task switching compared with CON; (b) during EARLY, MID, and LATE adaptation, slow adapting parameters are less perturbed in the ACLR group when walking at a 3:1 ratio; and (c) ACLR individuals use different strategies than CON, cognitive or otherwise, to adapt locomotor patterns.
Footnotes
Acknowledgements
The authors would like to thank Matthew Terza for his expertise and assistance with programming. The authors would also like to thank all laboratory students for their help with data processing and compilation and all volunteers for their participation in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: During the duration of this project, Dr Daniel Herman was supported by the National Institutes of Health Rehabilitation Medical Scientist Training Program under award number 5K12HD001097-17.