
Abstract
Background. Unilateral spatial neglect (USN) is a highly prevalent and disabling poststroke impairment. USN is traditionally assessed with paper-and-pencil tests that lack ecological validity, generalization to real-life situations and are easily compensated for in chronic stages. Virtual reality (VR) can, however, counteract these limitations. Objective. We aimed to examine the feasibility of a novel assessment of USN symptoms in a functional shopping activity, the Ecological VR-based Evaluation of Neglect Symptoms (EVENS). Methods. EVENS is immersive and consists of simple and complex 3-dimensional scenes depicting grocery shopping shelves, where joystick-based object detection and navigation tasks are performed while seated. Effects of virtual scene complexity on navigational and detection abilities in patients with (USN+, n = 12) and without (USN−, n = 15) USN following a right hemisphere stroke and in age-matched healthy controls (HC, n = 9) were determined. Results. Longer detection times, larger mediolateral deviations from ideal paths and longer navigation times were found in USN+ versus USN− and HC groups, particularly in the complex scene. EVENS detected lateralized and nonlateralized USN-related deficits, performance alterations that were dependent or independent of USN severity, and performance alterations in 3 USN− subjects versus HC. Conclusion. EVENS’ environmental changing complexity, along with the functional tasks of far space detection and navigation can potentially be clinically relevant and warrant further empirical investigation. Findings are discussed in terms of attentional models, lateralized versus nonlateralized deficits in USN, and tasks-specific mechanisms.
Keywords
Background
Unilateral spatial neglect (USN) is a common and highly debilitating consequence of stroke, characterized by a deficit in directing attention to stimuli located in the contralesional hemispace. 1 USN is experienced by nearly 50% of individuals with a right hemisphere lesion 2 and while it can resolve spontaneously within the acute poststroke period, symptoms of USN and their dramatic impact on functional performance may persist in up to 75% of initially diagnosed cases. 2 Unfortunately, those numbers are expected to surge with the rise in the aging population, given that post-stroke USN is associated with increase in age. 3
USN is known to adversely affect patient-related outcomes such as functional independence, community reintegration, and quality of life, and the sensitive detection of USN symptoms and their effects on everyday functional tasks is crucial.4,5 Nevertheless, USN represents a real challenge for rehabilitation professionals to properly detect and to characterize its direct impact on functional performance given the lack of sensitivity and ecological validity of conventional assessment methods.2,6 This challenge could be accounted for by USN’s high heterogeneity, which is evident in ongoing debates amongst researchers with regard to its anatomical, physiological, and conceptual models. The variety in behavioral manifestations of neglect includes different modality categories (sensory vs premotor), 7 spatial representations (egocentric vs allocentric), 8 and range of space (personal, near- and far-extrapersonal).9,10 Other, “nonspatial” factors such as level of alertness,11,12 sustained attention, 13 increased cognitive load,14-17 and increased perceptual demands18-20 are known to affect the severity of USN’s spatial deficits.
It is therefore not surprising that conventional assessments do not grasp all the facets of USN’s multimodal and heterogeneous presentation. Despite an extensive body of research on USN standardized assessment tools, there is currently no gold standard. 21 Moreover, studies reported that participants with “recovered” USN based on conventional paper-and-pencil tests showed residual deficits when more complex, challenging, and/or functional tasks were employed.22-25 The commonly employed measures are not sufficiently sensitive to detect subtle but clinically important deficits, 23 to predict functional performance in daily life and are constrained to assessing USN within the near-extrapersonal space only, using static, 2-dimensional (2D) methods. This is of great concern given that these individuals are at risk of being discharged into the community to resume their pre-stroke life roles and activities (eg, community ambulation, instrumental activities of daily life, driving, parenting, etc) without proper diagnosis of the impact of USN or symptoms of USN on functional performance. Therefore, with current advancements in the use of technologies in rehabilitation, it is highly relevant and timely to further the development of USN assessment and rehabilitation techniques, by incorporating state of the art technologies like virtual reality (VR) that could address the aforementioned restrictions.
VR affords us the possibility to employ 3D images or stereovision, far space and dynamic targets, functional everyday tasks, and modifiable spatial and nonspatial factors. Different VR-based USN assessments have been proposed, and some were found to be more sensitive in detecting the presence of deficits in cases where conventional USN assessment was negative (reviewed in Ogourtsova et al 26 ). However, these studies have several limitations, including the use of nonfunctional tasks (eg, Broeren et al 27 and Kim et al 28 ) that do not easily translate into real functional performance in daily life; small sample sizes (eg, Katz et al 29 ); comparing performances of patients with USN with that of healthy control individuals, rather than to those with stroke but no USN (eg, Broeren et al 27 ); or using 2D displays23,29-31 that lack immersiveness and interactivity. 32 We believe that the latter limitation is of particular importance, given that USN is largely viewed as an attention-based deficit and the use of full immersion in its assessment can help limit possible attentional shifts to the physical world that could influence performance.
In addition, previous VR-based studies have not evaluated the impact of increased perceptual-attentional demands (eg, a more crowded, ecological scene with multiple objects) within an immersive VR scene on the functional performance of object-detection and space navigation patients with poststroke USN. Previously, detection time and the time to complete a task have both been found to be affected in USN+ patients, compared with either USN− patients or healthy controls,25,33,34 suggesting that such measures can be sensitive to the presence of USN. In addition, there is some indication that USN influences navigation abilities (eg, wheelchair navigation 35 ), as such tasks involve both the near and far space perception and adjustment, and can be performed toward changing directions and within different environments. Thus, examining target detection and goal-directed navigation in the far-extrapersonal space, while covering both the contra- and ipsilesional space and manipulating perceptual-attentional demands, is relevant and has the potential to complement previous findings and deepen our understanding of the poor functional recovery that so often accompanies USN. It is possible that a more complex/crowded virtual environment, as opposed to a simple/sparse environment, will result in more noticeable deficits in patients with poststroke neglect and thus, be more predictive of and generalizable to the real-life functional performance. A VR assessment that is performance-based thus has the potential to further inform clinicians managing stroke survivors with USN on their functional performance, while providing additional benefits in terms standardization, space, safety, objectivity and possibly sensitivity and responsiveness compared to simulated task observation in a real environment.
Accordingly, we have developed a novel tool, the Ecological VR-based Evaluation of Neglect Symptoms (EVENS) that is immersive and is in 3 dimensions. It consists of 2 ecological scenes with variable perceptual-attentional demands where functional tasks of object detection and goal-directed navigation are performed. To further assist its development and examine its feasibility, in this proof-of-concept study we aimed to investigate the effects of poststroke USN on functional tasks as performed in VR.
Methods
Study Design
A cross-sectional, observational study design was used.
Study Participants
Adult individuals with stroke were included based on the following inclusion criteria: presence of a first-time right hemisphere stroke, with or without left USN (as per one or more of the following tests: Line Bisection Test (LBT), 36 Star Cancellation Test (SCT), 37 and/or Apples Test (APT) 8 on testing, or history of USN as per medical chart); and right handedness. As a first step, it was deemed suitable to include individuals with left USN only (ie, right hemisphere stroke), the latter being more prevalent38-40 and known to have larger effects on functional outcomes such as detection time 33 than right USN following left hemisphere brain injury.
Individuals were excluded based on the following criteria: presence of primary visual impairment that impedes normal or corrected-to-normal visual acuity (score ≤20/25 on the Early Treatment Diabetic Retinopathy Study Chart 41 ); presence of moderate cognitive impairment (score ≤22 on the Montreal Cognitive Assessment 42 ); presence of apparent sensorimotor deficits of the right (ipsilesional/nonparetic) upper extremity that can interfere with the use of the joystick (as per observation); and presence of a visual field defect (as per medical chart, Goldmann perimetry, or computerized equivalent). In addition, age-matched (±5 years) healthy controls were recruited following the same inclusion/exclusion criteria where applicable.
Participants were recruited from 3 clinical sites of Centre de Recherche Interdisciplinaire en Réadaptation du Montreal Métropolitain (CRIR). The study was approved for ethics by the CRIR Institutional Review Board. All study participants reviewed and signed the informed consent before enrolling in the study.
Experimental Setup and Procedure
The process of data collection consisted of a clinical evaluation of USN, VR-based detection, and navigation tasks.
Evaluation of USN
Presence, severity, and type of USN were determined using the LBT, SCT, and the APT. All tests were chosen with care as to their psychometric properties.8,43,44
Apparatus and stimuli
A previously employed setup was used to assess near and far space USN.45,46 It was deemed relevant to assess far space USN, in addition to traditional near space evaluation, given that the VR-based task is performed in far space and one of the aims consisted of determining whether far and/or near space USN could explain the VR-based performance in far space. Participants were positioned 40 and 320 cm away from the screen for near and far USN testing, respectively. The LBT and SCT were displayed on a projector screen with the appropriate sizes (near space, 21 × 28 cm; far space, 168 × 224 cm) to keep the visual angle of each array and the retinal size image constant during both testing conditions. Each displayed test contained a middle point, with regard to which the participants’ sternum was aligned with a laser. A chin rest was used to minimize head movements and to ensure a constant viewing angle. Responses were provided by the participants using a handheld laser pointer. Responses were marked directly on the computerized test form by the investigator using a wireless mouse and the pencil in Microsoft Paint. The order of tasks and distance conditions was randomized across participants. The APT was presented on a sheet of paper on a steady table, aligned with the participant’s midline (ie, sternum) and fixed on the table with tape to prevent possible shifts.
Procedure
In the LBT, participants were asked to find the midline of each presented line, starting from the top line. In the SCT, participants were instructed to find all the small stars among the distractors. In the APT, participants were instructed to find all the complete-shaped apples. For the scoring of the LBT, the deviation from the center in each line was measured and averaged across all lines. An absolute mean deviation of more than 6.0 mm to the right is indicative of left near space USN on the near LBT test, 36 and 4.8 cm to the right is indicative of left far space USN on the far LBT test. An average percentage of deviation from midline was also computed for near and far space LBT to estimate the difference in severity between near and far space USN. For the scoring of the SCT, the number of small cancelled stars was divided by the total number of small stars to compute the laterality index score. Scores between 0 and 0.46 are indicative of left near space USN. 36 For the scoring of the APT, the total number of crossed out complete and incomplete shape apples was computed, and an asymmetry scores for egocentric and allocentric USN were calculated. 8 The overall cutoff of <42/50 is indicative of near space USN. Asymmetry cutoff score across the page of <−2 or >2 (difference between right- and left-sided targets cancelled) is indicative of egocentric near space USN. Asymmetry cutoff score across the cancelled distractors on the page with left- versus right-sided openings of <−1 or >1 is indicative of allocentric near space USN. All cancellation tests were timed.
In terms of neglect severity, it has been strongly suggested that a battery of tests is more sensitive to detect the presence of neglect than a single test. 47 However, no clear guidelines exist defining the overall USN severity rating when multiple tests are used. For instance, Lindell et al 47 defined mild versus moderate/severe USN as positive results on 1 to 3 tests versus 4 or more tests, respectively. In the present study, this proposed classification was further modified to separate moderate versus severe cases. Severity of USN was thus characterized by a positive result on 1 to 3, 4, and 5 or more clinical tests for mild, moderate, and severe USN, respectively.
Outcomes
Outcomes retained for analysis included (a) overall USN severity (mild, moderate, or severe), (b) USN range of space severity (near and/or far space), and (c) USN spatial representation type (allocentric vs egocentric) within one’s reaching distance (near space) and/or beyond reaching distance (far space). Participants were included in the group of individuals with USN (USN+) if they had USN on one or several of the aforementioned tests, or if they had a history of USN as per their medical chart.
Detection and Goal-Directed Navigation in Simple Versus Complex Virtual Scenes
Apparatus and stimuli
A simulation consisting of 2 virtual scenes was created in the Unity (Unity Technologies SF, CA) game engine: the complex and simple scenes (Figure 1). The viewing media was a helmet mounted display (HMD–NVisor, NVIS Inc, Reston, VA) with field of view of 60° diagonal, 30° vertical by 40° horizontal, extended graphics array resolution 1024 × 1280, frequency of 60 Hz, 1 kg in weight, and blocking all peripheral vision with only the virtual environment (VE) visible to the participant. Responses were provided with the dominant, nonparetic right hand using a stationary and fixed joystick (Attack3, Logitech, Newark, CA).

Simple and complex virtual scenes. In the detection task, the participant was asked to press the joystick button in response to the target (blue cereal box with “Pop Start” sign) appearing or refrain from clicking in its absence. In the navigation task, the participant was asked to navigate to the target in the most direct way possible using the joystick.
The scenes contained a symmetrical and richly textured room displaying a grocery shopping aisle with 3 shelves located in front and 3 m away from the participants. For the simple scene, the target of interest (blue cereal box “Pop Start”) appeared stand-alone on the middle/eye level shelf at one of the following 5 locations, ±40°, ±20°, and 0° in a random order. For the complex scene, the target of interest appeared at the same locations but among additional grocery items on the same shelf (eg, similar looking cereal boxes). Supplementary items on other shelves and grocery carts were also presented. A gradient in response to targets located centrally versus laterally (±30°) was previously reported in USN+ individuals. 34 For the current experiment, we intended to capture neglect’s gradient reported previously over a larger portion of the visual spectrum, while presenting maximal target eccentricities that can feasibly and comfortably be attained using eye in head horizontal shifts (ie, ± 20° and 40°). The scenes were viewer-centered, and the HMD was not head-tracked, allowing the scene to remain stable and centered despite head rotations and eliminating the need to stabilize the head during navigation and detection trials. This also allowed for standardization of VR tasks versus traditional tests, where a chin rest was employed to prevent head rotations. Navigation in the scene, when required, was possible using the joystick in the mediolateral (left/right) and anterior-posterior (front/back) planes using self-controlled speeds of displacement ranging from 0 m/s (ie, complete stop) to 1.2 m/s (maximum speed). Both experiments were performed while seated.
Procedure
Practice trials were provided prior to the actual experiment until the participant felt comfortable in executing the tasks. For the detection task, participants were instructed to press the joystick button with their index finger of the nonparetic (right) hand as soon as they detected the target. An auditory feedback (“beep” sound) was provided once the joystick button was pressed. Catch trials with no target appearing were also introduced to minimize response bias. Participants were instructed that in the absence of a target they should refrain from clicking the joystick button and wait for the next trial to appear. Five trials per condition (5 target locations + no target condition) were performed for a total of 30 responses each for the simple and complex scenes. In cases where the participant was not able to detect the target for more than 30 seconds, he or she was provided verbal encouragement from the examiner to continue visual scanning. In all trials except catch trials, the target remained on the screen until a response was provided by the participant.
For the navigation task, participants were instructed to navigate using the joystick in the mediolateral and anterior-posterior planes using self-controlled speed to reach the target in the most direct way possible. The navigation trials ended when the participant reached within 0.5 m (anterior direction) of the target, so as not to collide with the shelf. Five trials per target location were performed for a total of 25 responses for the simple and complex scenes.
Outcomes
The outcomes for the detection task was detection time (seconds), defined by the time at which the participant detected (ie, pressed the joystick button) the target in the detection task. Outcomes for the navigation task included (a) the maximal mediolateral deviation (mMLD) from an ideal navigation trajectory that is represented by the most direct route possible from the start position to the respective target in the navigation task and (b) the navigation time to target (seconds), defined as the time required by the participant to navigate to the target.
Data and Statistical Analysis
The simulation data were recorded at 120 Hz and stored for off-line analyses in Matlab. Participants’ responses on the USN tests and detection/navigation tasks were averaged across conditions, such that mean values could later be compared across groups and between conditions. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc, Cary, NC). Significance was accepted at P ≤ .05. Groups’ demographics and USN characteristics were analyzed using descriptive summary statistics and test of normality ad equality of error variance were performed on all study variables. Depending on data distribution, 1-way analysis of variance or the Kruskal-Wallis test were used to compare demographic characteristics between groups. Difference in USN severity (near vs far) was evaluated using the Wilcoxon signed rank sum test.
The effects of scene complexity and target location on detection time and goal-directed navigation performances were examined using a repeated-measure mixed model approach, with “Group [USN+ vs USN− vs HC]” as between-subject factor, as well as “Scene Complexity” [simple vs complex] and “Target Location” [±40°, ±20°, 0°] as within-subject factors. In the presence of significant effects, post-hoc comparisons of simple effects were elaborated on using previously identified relevant pairwise comparisons. The mixed model approach was selected given that it accounts for the large between-subject heterogeneity frequently present in individuals with poststroke USN, and is also tolerant to small and unequal sample sizes as used in the present study. Recently, the mixed model approach was highly recommended as the favorable type of statistical analysis over repeated-measures analysis of variance for post-stroke USN-related research. 48 The combined covariance structures (unstructured as the reference structure and compound symmetry structure) and a random coefficient structure were used. The final model was chosen using the Akaike’s information criterion, the Bayesian information criterion, and the restricted maximum likelihood ratio test. This chosen model was further ascertained by evaluating the fit of the data and deviations from model assumptions using residuals’ analysis.
To provide insight into EVENS’ concurrent validity, Kendall’s rank correlation coefficient was used to quantify the relationship of goal-directed navigation and detection abilities to the left eccentric (−40°) target in the complex scene with clinical assessments of neglect within near and far space. To gain a better understanding of how EVENS’ detection and navigation tasks evidence functional deficits in USN of different severities; and how sensitive EVENS is in detecting deficits otherwise not detected using traditional tests, single case analyses were used to compare the performance of each USN+ participant with regard to the average performance of the USN− group as well as to compare the performance of each USN− participant with regard to the average performance of the HC group. Precisely, the Crawford and Garthwaite 49 approach (Singlims.exe, University of Aberdeen, Aberdeen, UK), which implements classical methods for comparison of a single case’s score to scores obtained in a control sample, was used. The interval estimate of the effect size for the difference between each case and controls (as normative data) was obtained.
Results
Twelve individuals with poststroke USN (n = 12, USN+), 15 individuals poststroke without USN (n = 15, USN−), and 9 age-matched healthy control individuals (n = 9, HC) were recruited in the period between September 2015 and March 2016. Each participant successfully completed all experimental trials, without any missing data. No adverse effects such as dizziness, nausea, or any other discomfort were reported by study participants during testing. Table 1 outlines the demographic and clinical variables for the 3 groups. USN+ and USN− groups predominantly consisted of male participants, both statistically similar in stroke chronicity and age.
Descriptive Variables of Study Groups.
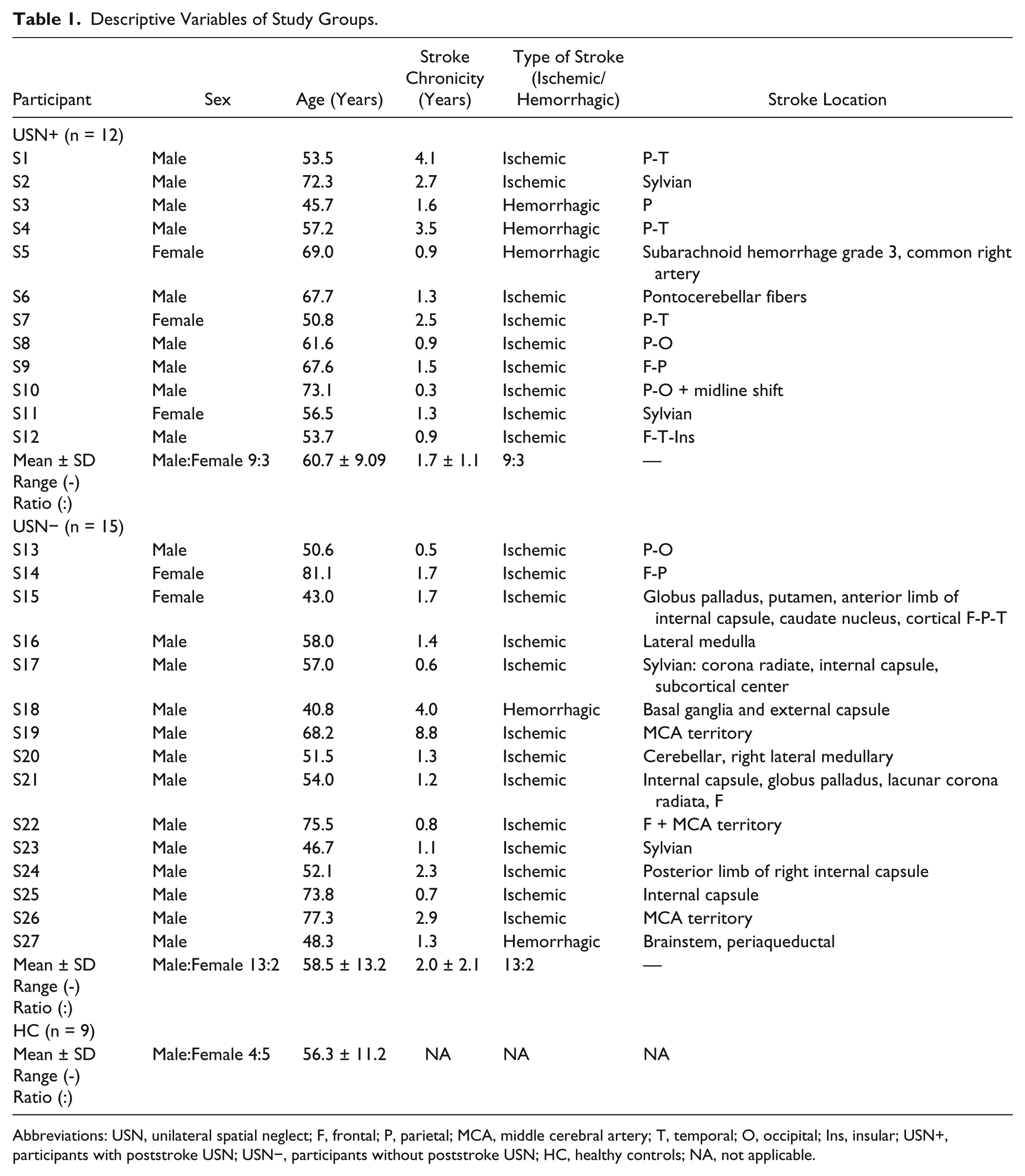
Abbreviations: USN, unilateral spatial neglect; F, frontal; P, parietal; MCA, middle cerebral artery; T, temporal; O, occipital; Ins, insular; USN+, participants with poststroke USN; USN−, participants without poststroke USN; HC, healthy controls; NA, not applicable.
USN Characteristics
USN+ group demonstrated significantly greater deficits than the USN− group on all USN-related measures in the near and far space (P ≤ .05) (Table 2). The USN+ group took longer to complete the APT and SCT in the near and far space (P ≤ 0.05) versus USN− group. Similarly, those with history of USN also took longer to complete the APT and SCT in the near space (P ≤ .05) versus USN− group. No other significantly greater deficits were found in those with history of USN versus USN− group. None of the USN− individuals scored positive in any of the USN assessments. No statistically significant difference was found for USN severity (near vs far space) within USN+ group (P = .90 for LBT; P = .54 for SCT).
Results of the USN Clinical Tests. a
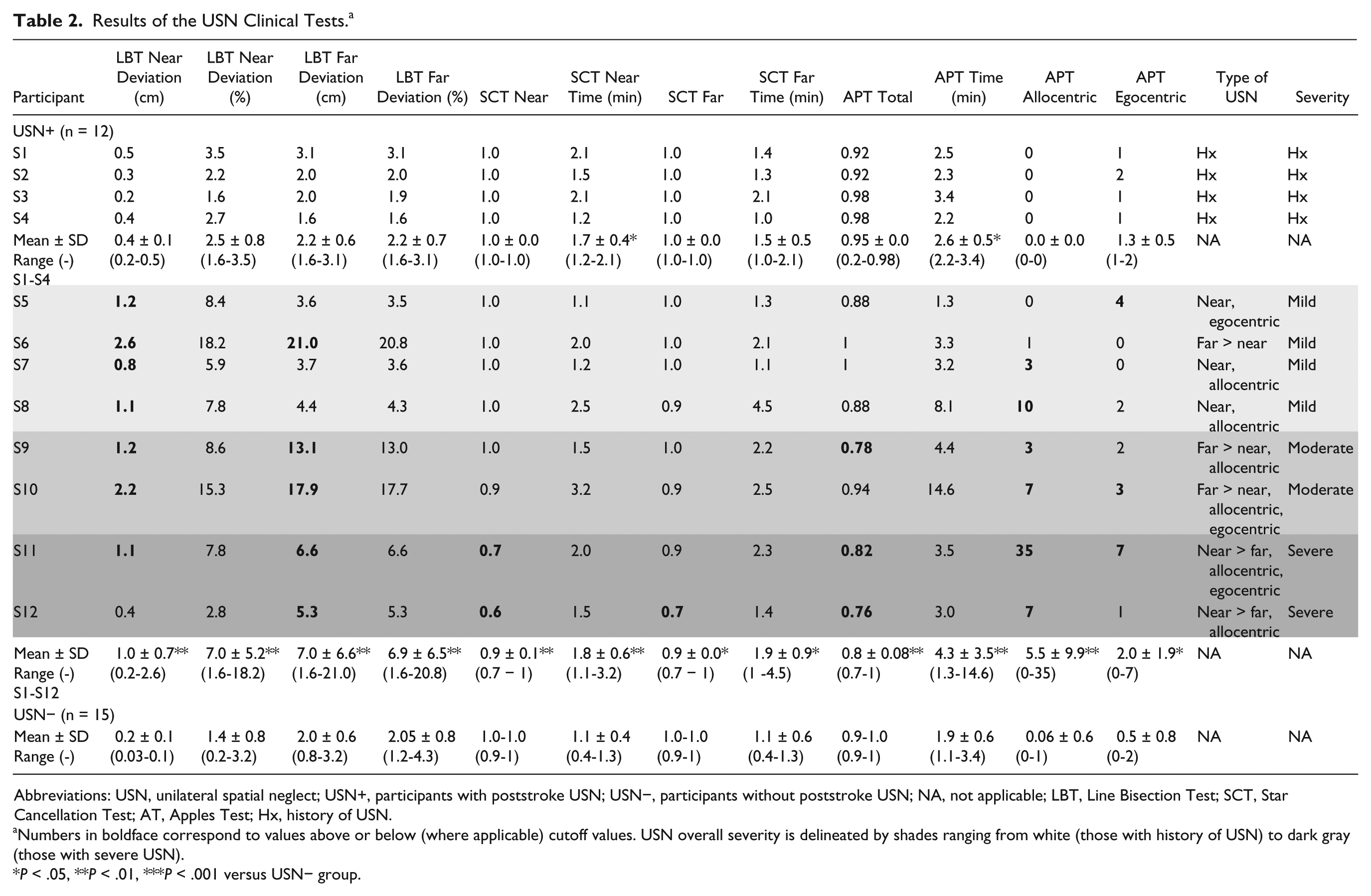
Abbreviations: USN, unilateral spatial neglect; USN+, participants with poststroke USN; USN−, participants without poststroke USN; NA, not applicable; LBT, Line Bisection Test; SCT, Star Cancellation Test; AT, Apples Test; Hx, history of USN.
Numbers in boldface correspond to values above or below (where applicable) cutoff values. USN overall severity is delineated by shades ranging from white (those with history of USN) to dark gray (those with severe USN).
P < .05, **P < .01, ***P < .001 versus USN− group.
Detection Task
For detection time (Figure 2), a 3-way interaction of Group × Scene Complexity × Target Location was found to be significant, F(18, 231) = 1.78, P = .0287. Within the USN+ group, significantly longer detection times were found all target locations in the complex (mean ± SD for targets at −40° to +40°: 4.06 ± 4.93, 4.05 ± 4.06, 2.62 ± 2.52, 2.04 ± 1.48, 2.40 ± 1.29 seconds) versus simple scene (mean ± SD for targets at −40° to +40°: 1.41 ± 1.78, 0.69 ± 0.29, 0.59 ± 0.26, 0.60 ± 0.24, 0.75 ± 0.43 seconds) (P < .05). Similarly, USN− and HC showed significantly longer detection times to all target locations in the complex versus simple scene (P < .05). Between-group analyses revealed that USN+ individuals showed longer detection times for left and middle targets at −40°, −20°, 0° (mean ± SD: 1.41 ± 1.78, 0.69 ± 0.29, 0.59 ± 0.26 seconds) in comparison with both USN− (mean ± SD: 1.67 ± 0.78, 1.13 ± 0.41, 1.14 ± 0.57 seconds) and HC groups (mean ± SD: 1.40 ± 0.69, 0.95 ± 0.20, 0.88 ± 0.16 seconds) in the complex scene only (P < .05). No significant detection time differences were found between USN− and HCs.
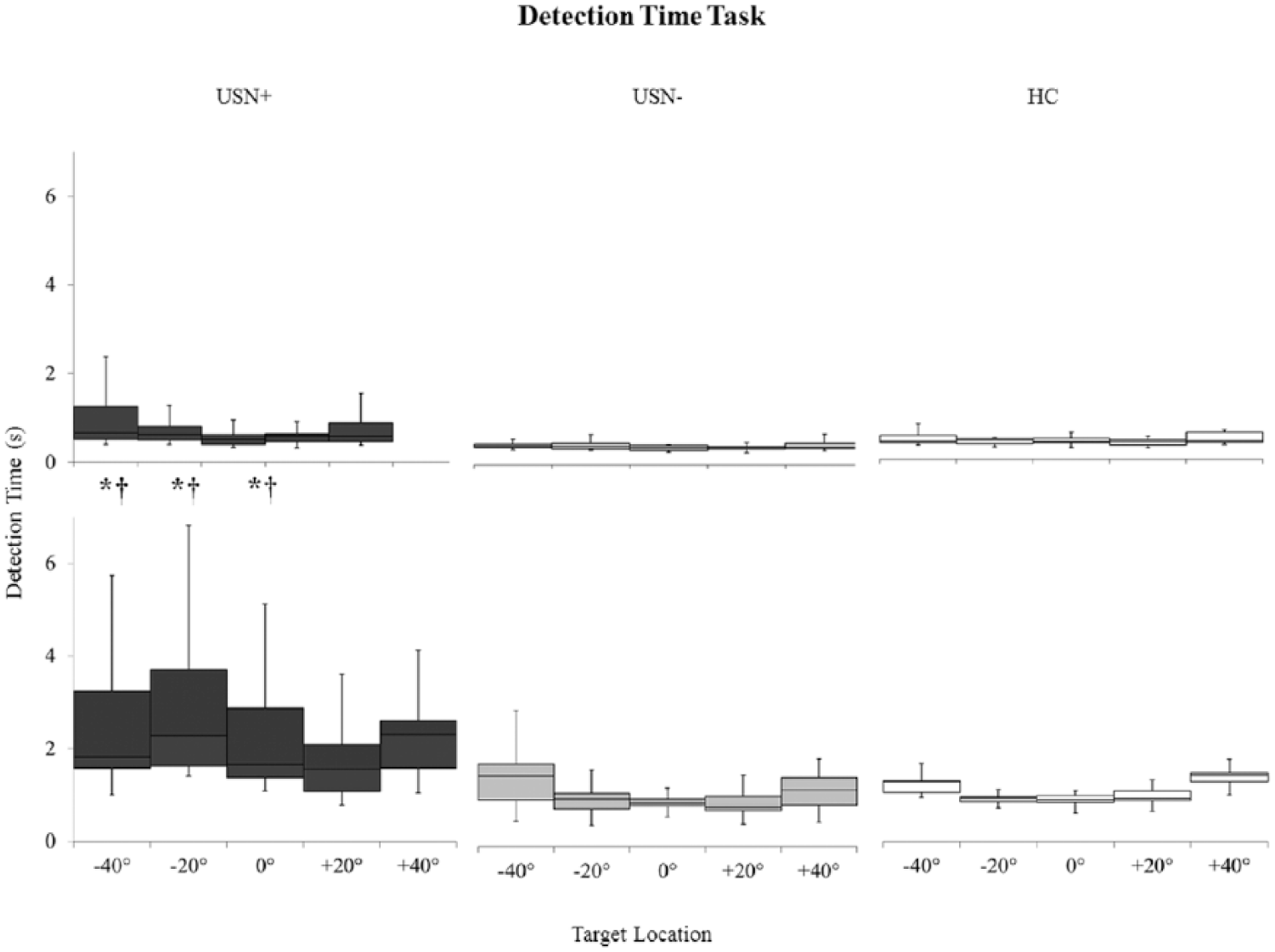
Detection time (seconds) for the simple (top) and complex (bottom) scenes and the 3 study groups. Black boxes and whiskers for USN+ group, gray for USN− group, white for HC group. Box and whiskers description: minimal and maximal values shown by the whiskers, the bottom and top of the box are the first and third quartiles, and the band inside the box is the second quartile (the median). Statistically significant differences between groups are indicated by: *for USN+ versus USN− groups; †for USN+ versus HC groups, at P ≤ .05 for specific target locations. USN+, participants with poststroke unilateral spatial neglect; USN−, participants without poststroke unilateral spatial neglect; HC, healthy controls.
Navigation Task
Figure 3 depicts the displacement traces of both a USN+ and USN− stroke participant in the simple and complex scenes. While the USN− mostly selected a heading direction from the start, and maintained a nearly linear goal-directed route, the USN+ participant demonstrated a “searching” strategy, where he or she first searched for the target (shown by larger deviations of trajectories at the beginning or early in the trial) and only then advanced toward it, making final mediolateral corrections at the end of the trial.
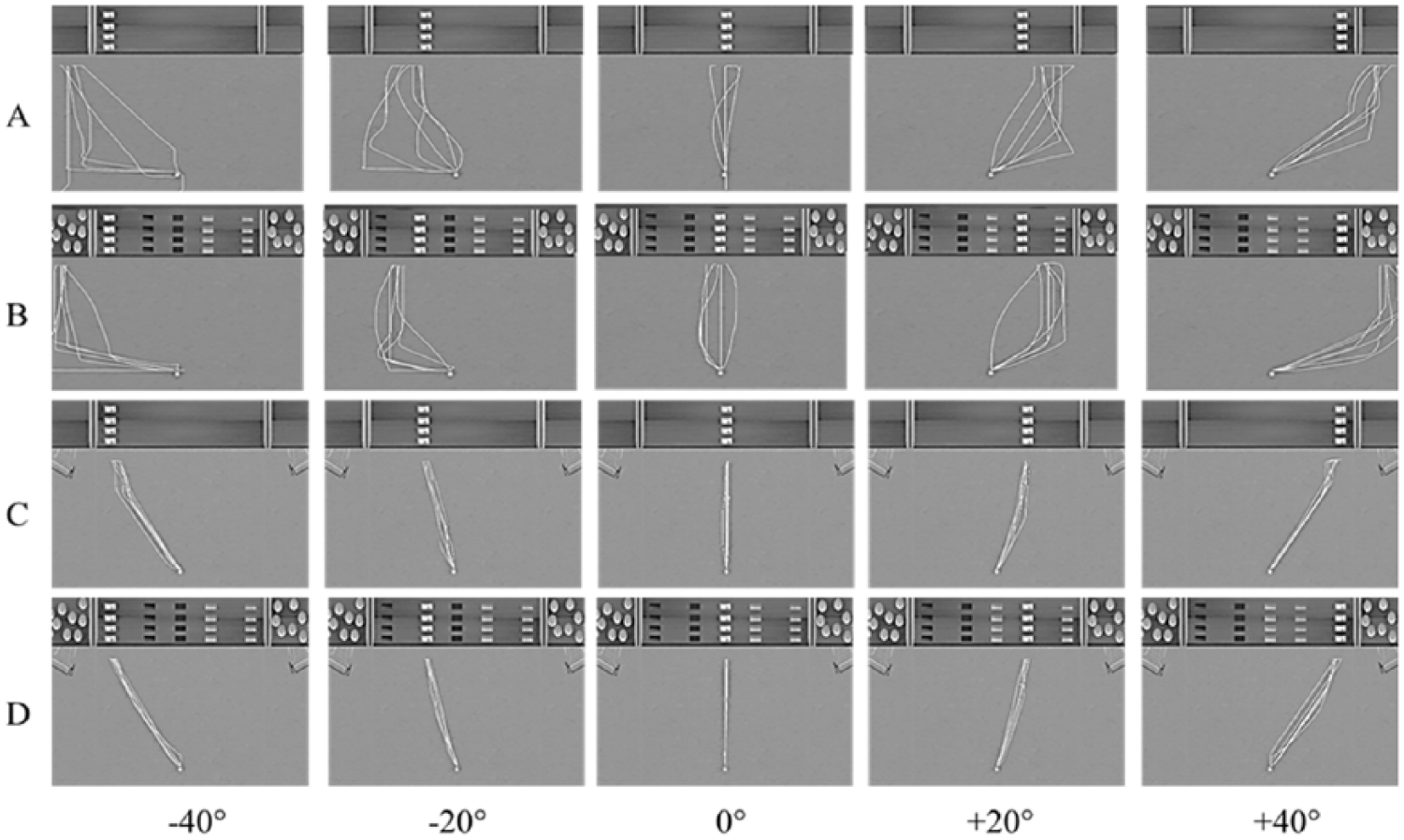
Bird’s eye view of the virtual environment and displacement traces (y = anteroposterior displacement; x = mediolateral displacement) during the navigation task toward targets of different eccentricities (from −40° to +40°). Performance for one individual with (USN+, A and B) and one individual without (USN−, C and D) USN is illustrated for the simple (A and C) and complex (B and D) virtual scenes. The scale in the X-axis refers to the mediolateral (left and right) space. The scale in the Y-axis refers to the anterior-posterior (front and back) space. The participant always starts at coordinate 0, 0 along both axes. USN+, participants with poststroke unilateral spatial neglect; USN−, participants without poststroke unilateral spatial neglect.
A significant 3-way interaction of Group × Scene Complexity × Target Location was observed for mMLD outcome, F(18, 122) = 2.28, P =.0043 (Figure 4). Within USN+ group, larger mMLDs were found for left and middle targets in the complex (mean ± SD for targets at −40°, −20°, 0°: 1.10 ± 0.70, 0.78 ± 0.64, 0.34 ± 0.33 m) versus simple scene (mean ± SD for targets at −40°, −20°, 0°: 0.89 ± 0.42, 0.64 ± 0.23, 0.31 ± 0.25 m) (P < .05). No within-group differences depending on the complexity of the scene were found among USN− and HCs. USN+ individuals displayed significantly larger mMLDs for the most eccentric targets (±40°) (mean ± SD: 1.10 ± 0.70, 0.84 ± 0.42 m) compared with USN− (mean ± SD: 0.82 ± 0.44, 0.52 ± 0.36 m) individuals under the complex VR scene condition only (P < .05). The mMLDs of USN+ individuals across the different target locations were generally larger compared with those of HCs under both the simple and complex scene conditions (P < .05). No significant mMLD differences were found between USN− and HCs.
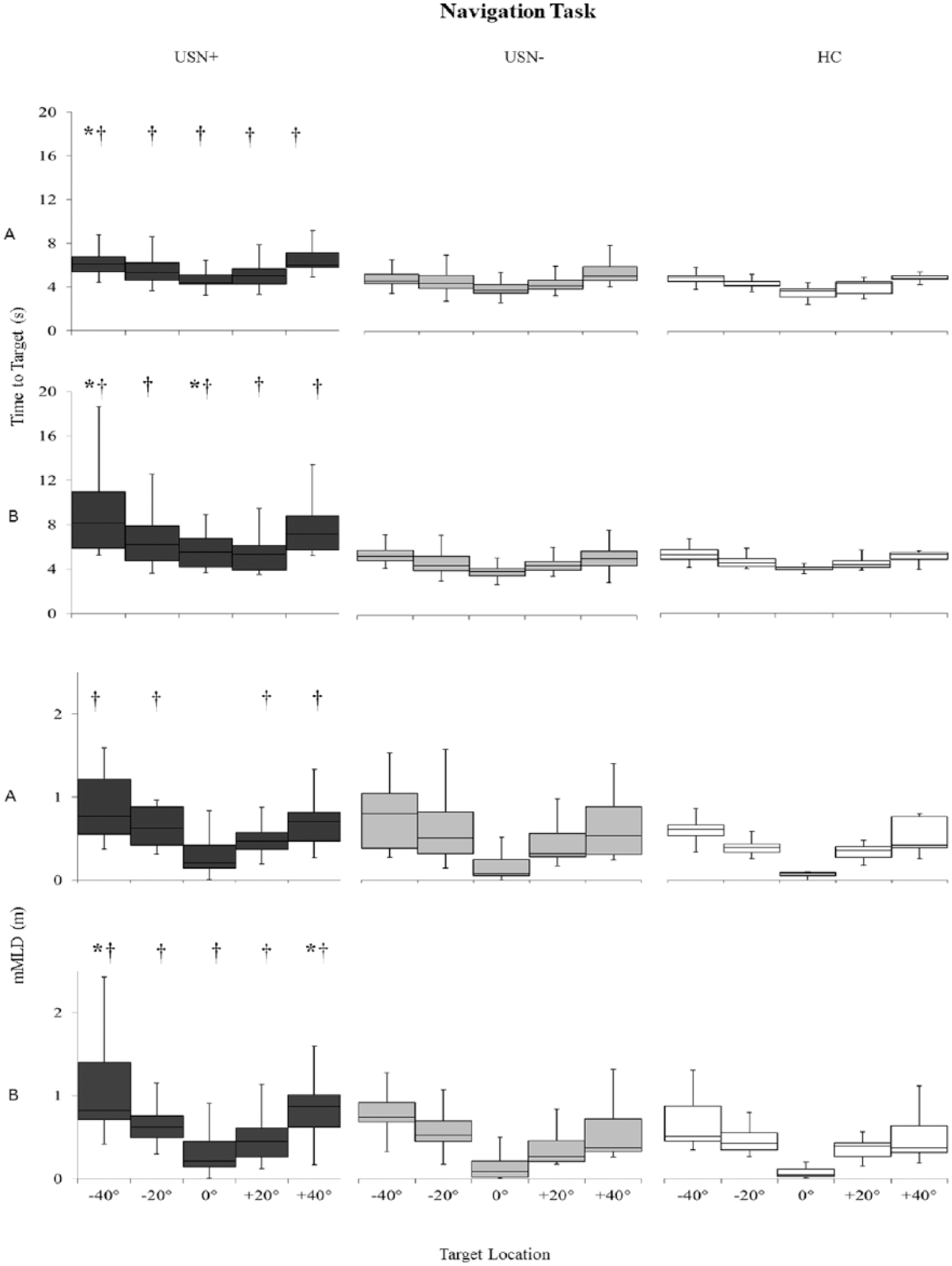
Navigation time to target (seconds) and maximal mediolateral deviations from the ideal path (mMLD, m) for the simple (A) and complex (B) scenes and the 3 study. Black boxes and whiskers for USN+ group, gray for USN− group, white for HC group. Box and whiskers description: minimal and maximal values shown by the whiskers, the bottom and top of the box are the first and third quartiles, and the band inside the box is the second quartile (the median). Statistically significant differences between groups are indicated by: *for USN+ versus USN− groups; †for USN+ versus HC groups, at P ≤ .05 for specific target locations. USN+, participants with poststroke unilateral spatial neglect; USN−, participants without poststroke unilateral spatial neglect; HC, healthy controls.
Time to target results (Figure 4) also showed a significant 3-way interaction of Group × Scene Complexity × Target Location, F(18, 122) = 3.57, P < .0001). Within the USN+ group, longer lasting navigations were observed for the most eccentric left target at −40° in the complex (mean ± SD: 9.53±5.21 seconds) versus simple scene (mean ± SD: 6.61 ± 1.84 seconds) (P < .05). No within-group differences depending on the complexity of the scene were found among USN− and HCs. USN+ individuals displayed significantly longer lasting navigations for the most eccentric left target at −40° and middle target at 0° under the complex scene (mean ± SD: 9.53 ± 5.21, 5.71 ± 1.74 seconds) in comparison with the USN− group (mean ± SD: 5.65 ± 1.32, 4.25 ± 1.38 seconds) (P < .05). The times to target of USN+ individuals across the different target locations were generally larger compared with those of HCs under both the simple and complex scene conditions (P < .05). No significant time to target differences were found between USN− and HCs.
Severity of USN and EVENS’ Sensitivity
The outcomes of the detection (detection time) and navigation tasks (time to target, mMLD) to the left eccentric target (−40°) in the complex virtual scenes were used to examine how these outcomes vary as a function of USN severity. It was deemed suitable to select these outcomes as responses to that target location in the complex virtual scene were found to be consistently worse in USN+ versus USN− and HC participants. Table 3 outlines the single case analyses of single USN+ participant versus the USN− group, as well as single USN− participant versus the HC group. The time to target outcome (navigation task) and to a lesser extent the detection time outcome (detection time task), but not the mMLD outcome (navigation task) appear to be responsive to USN severity, where performances worsen with increase in neglect severity (as per the effect size values). None of the participants, with the exception of S25, presented with deficits solely in the detection task. In other words, most USN+ participants who showed an altered object detection performance also showed deficits in navigation, but participants could show an altered navigation performance with a preserved object detection ability.
Single-case Analysis of Single USN+ Participants Versus USN− Group (as Control Data) and Single USN− Participants Versus HC Group (as Control Data) on the Performance of the Detection Time and Navigation Tasks for the Outcomes Related to Responses to Leftmost Target (−40°) in the Complex Scene. a
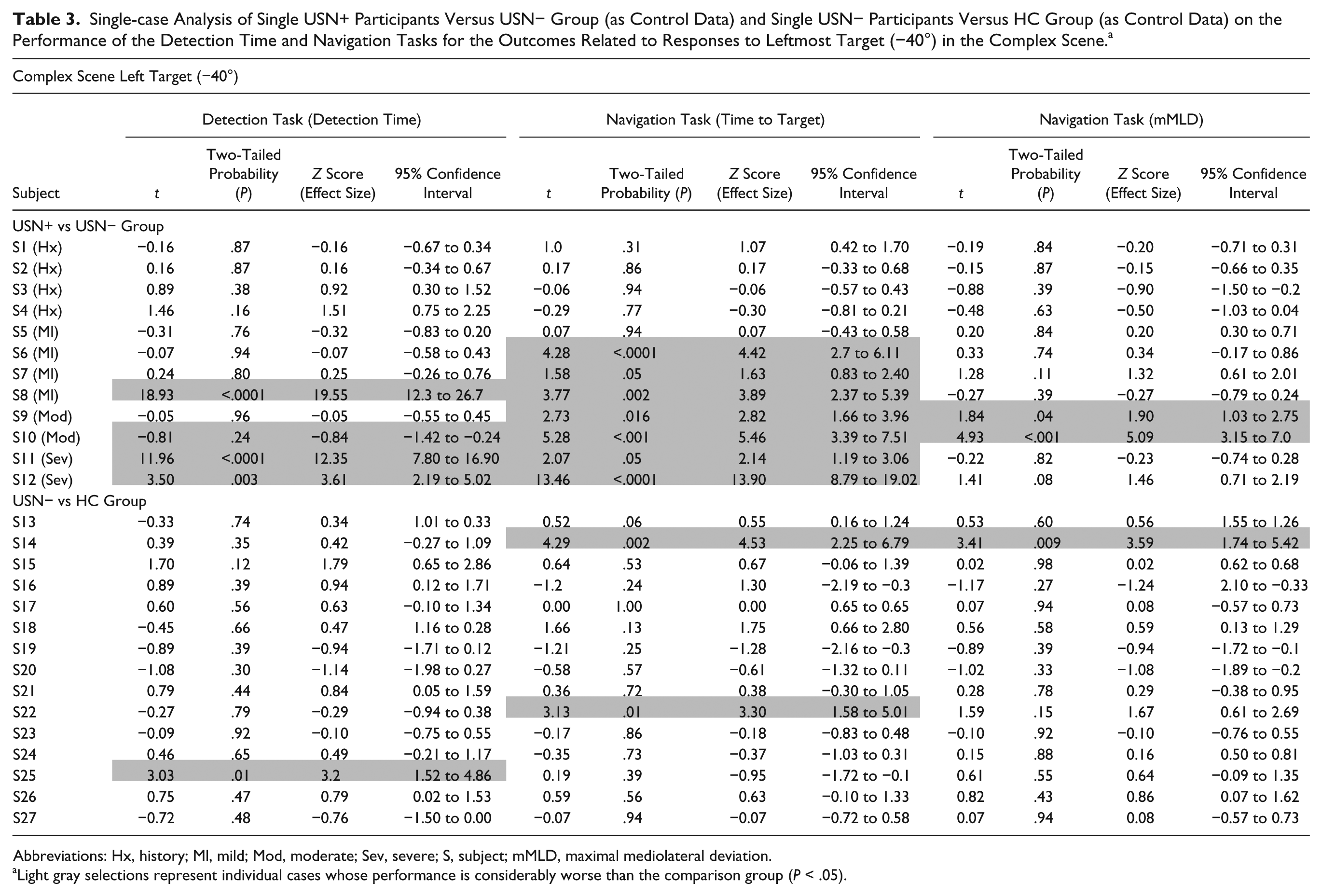
Abbreviations: Hx, history; Ml, mild; Mod, moderate; Sev, severe; S, subject; mMLD, maximal mediolateral deviation.
Light gray selections represent individual cases whose performance is considerably worse than the comparison group (P < .05).
Moreover, 3 individuals from the USN− group (S14 [both navigation task outcomes], S22 [time to target, navigation task], S25 [detection time outcome, detection time task]) were found to have significantly worse performance on EVENS in comparison with the HC group as the control normative sample (P < .05).
Correlations
A supplementary table shows the correlation coefficients between USN clinical test and detection/goal-directed navigation to left eccentric target (−40°) performances in the complex scene. None of the USN tests showed correlation with the time taken to detect the targeted object. Significant (P < .05) but low-magnitude (0.38-0.49) correlations were found, however, between most USN clinical measures and the navigation time to target outcome, indicating that a poor performance on USN tests was somewhat associated with a poor performance on the navigation task.
Discussion
This study investigated, for the first time, the effect of poststroke USN on object-detection and goal-directed navigation in the far space while using a newly developed, immersive VR-based USN assessment, EVENS, which allows to systematically assess participants’ performance in an environment of changing complexity. Key findings include the presence of altered performances on both, the detection and navigation tasks, in the USN+ individuals compared with individuals without USN; presence of deficits that varied as a function of environment complexity and which could present either unilaterally (lateralized) or bilaterally (non-lateralized); and unveiled deficits that were otherwise left undetected using traditional clinical measures. The following paragraphs discuss the implications of present findings, possible mechanisms for the observed findings, as well as benefits of further studying EVENS for the assessment of poststroke USN.
Environment Complexity Influences USN-Related Deficits
The present study found that while USN negatively affects perceptual and navigational abilities to targets located predominantly on the neglected side, deficits significantly worsen when exposed to a complex environment with an increased perceptual load. We propose that such an environment imposes greater demands on the perceptual-attentional resources compared with the uncluttered environment. Our findings may explain the difficulties individuals with chronic USN experience on daily basis in real-world situations where cluttered environments are encountered, such as mobility within the community that requires goal-directed locomotion,35,50 obstacle avoidance, 24 wheelchair navigation skills, 23 street crossing, 51 or performing instrumental activities of daily living. 52 These tasks may not only be lengthier to perform for those with poststroke USN but also more demanding, tiring, and possibly leading to difficultly in maintaining a given level of performance over an extended period of time. This could also explain the behavior of busy environment avoidance so often present in individuals with poststroke neglect in chronic stages. 53 Our results are also consistent with the view that the quantity and allocation of attentional resources available alter performance such that true deficits can be revealed when one can no longer effectively allocate his or her attentional resources in instances of increased perceptual or cognitive demands of the task. 16 Specifically, multiple studies found that increased task demands negatively affect the performance and result in the emergence of signs and symptoms of neglect in chronic stages that were otherwise not detected using conventional methods.24,54-56
Spatially Lateralized and Nonlateralized USN-Related Deficits
Findings of this study further revealed the presence of lateralized and nonlateralized deficits in individuals with USN, notably in detection time and time to target outcomes on the detection time and navigation tasks, and in maximal mediolateral deviation from the ideal path outcome on the navigation task. These findings may be explained by attentional mechanisms underlying USN. First, time-related performances (detection time, navigation time to target) of USN+ versus USN− group, in general, were worsened in a “gradient manner” from the ipsilesional/right (+20°) to contralesional/left periphery (−40°). This demonstrates that time-related outcomes can identify spatially-lateralized loss of attentional capacity. These findings are in accordance with two models of USN attentional theory: the hemispheric imbalance model, namely its opponent processor; and the disengagement deficit/attention shift model. The opponent processor hypothesis stipulates that there are 2 opponent processors (in the left/right hemispheres) that control attention toward the contralateral portion of the visual hemispace and inhibit one another via collasal connections. 57 Neglect is viewed as the result of the hypoactive ipsilesional hemisphere and hyperactive contralesional hemisphere following a stroke. This interhemispherical imbalance causes a decrease from center to periphery of the left/contralesional visual hemispace attention gradient, and an increase of the right/ipsilesional visual hemispace attention gradient. 57 Similar to the results obtained using EVENS, a previous study on the gradient of attention deployment evidenced that all patients with right hemisphere stroke and USN showed reduced response accuracy and increased reaction times to contralateral versus ipsilateral targets in comparison to individuals with left hemisphere stroke and healthy controls. 58
The disengagement deficit/attentional shift model is viewed as a sequence of three internal mental operations including disengagement of attention from current stimulus; moving attention toward a new stimulus; and engagement of attention on the new stimulus. Previously, USN+ individuals with right hemisphere parietal lesions were found to have a deficit in disengagement of attention from ipsilesional targets in response to contralesional targets.59-61 Similarly, our results could be associated with a deficit in moving attention from ipsilesional to contralesional targets in an activity reflecting real-world attentional demands. In addition, a related meta-analysis deduced that the disengagement deficit is in fact larger in individuals with USN+ individuals a right hemisphere lesion (especially with parietal lobe damage) than in USN− individuals with a left hemisphere stroke. 62 Nearly 60% of our sample of USN+ individuals presented with lesion to the right parietal lobe, supporting the evidence for possible disengagement difficulties.
Second, current findings, however, also revealed the presence of nonlateralized deficits, as demonstrated by the outcome of maximum mediolateral deviation from an ideal path in the navigation experiment which was found to be altered both for the left/“neglected” and right/“nonneglected” visual hemispaces in USN+ individuals. Such bilateral deficit in USN+ individuals was also recently observed by our team in the context of goal-directed walking (T. Ogourtsova, July 2017, unpublished data). Goal-directed navigation and locomotion both require space computation and re-adjustments of self with regard to target location 63 and perceived optic flow direction, 64 which are processes that involve a complex brain network that transforms perception into goal-directed action and which includes the parietal area.65,66 The latter area, which is largely involved in poststroke USN, is also known to have nonlateralized functions, 67 which may explain the presence of nonlateralized deficits observed in this study during goal-directed navigation. Findings are further consistent with the growing evidence that the persistence of neglect into chronic stages of stroke recovery is likely to be accompanied by widespread nonlateralized attentional deficits, unconfined to one region of space, in addition to the unilateral imbalance of attention to the contralesional space (reviewed in Robertson 68 and Husain and Rorden 69 ). Collectively, present findings suggest that behavioral performance in poststroke USN cannot be solely explained by lateralized deficits, but rather by combination of spatially lateralized and nonlateralized impairments.
The initial search and endpoint adjustments noted among individuals with USN in the present study is analogous to those found by Berti et al, 46 where the walking trajectories to a far space target were not corrected as the patient was approaching the target that was becoming a near versus a far space one. The patients thus followed a path that was related to the first computation of space carried out at the starting point and failed to remap and readjust the heading direction. Accordingly, present findings could indicate nonlateralized deficits in online control and heading in individuals with neglect poststroke.
Severity of USN and EVENS’ Sensitivity
The navigation task outcome “time to target,” and to a lesser extent the detection task outcome “detection time” in the complex scene evidenced a gradient of responses according to USN severity. Thereby, individuals showed worsened performance with an increase in USN severity, as assessed with clinical tests ranging from mild USN to severe USN. The nature of the navigation task, requiring space computation and readjustments of self with regard to target location 63 and perceived optic flow direction 64 to transform perception into action, could account for these findings. In addition, it emerges that time-related outcomes in both tasks are more predictive of USN severity. However, the single-case analyses revealed that the navigation performance does not seem to be dependent on the ability to detect the object, further supporting the usefulness and advantages of EVENS versus traditional and existing VR-based methods. Indeed, 5 participants (3 USN+, 2 USN−) demonstrated worsened time to target performance (navigation task), despite a normal object detection time (detection task). Several current VR-based USN evaluations employ solely a visual search/object-detection paradigm.25,27,28,70,71 Our results suggest that a performance-based component of navigation is potentially beneficial for a comprehensive and sensitive assessment. In line with this, EVENS demonstrated promising preliminary sensitivity, as it identified considerably worse performance in 3 USN− individuals versus HCs (2/3 on the navigation task only), that were otherwise left undetected using traditional tests. Nonetheless, it should also be mentioned that it failed short in identifying performance alterations in those with history of USN versus USN+ group. Therefore, additional research, including patients with different USN severities, is required to make more concrete inferences as to its usefulness and clinical applicability.
Benefits of a VR-Based Assessment Such as EVENS
In this study, a VR-based assessment revealed the presence of deficits (a) that varied depending on the nature of task to be performed (detection vs navigation), (b) that were modulated according to target location and environment complexity, (c) that could be either lateralized or nonlateralized, and (d) that become apparent despite normal performance on traditional USN tests. Together, these findings support EVENS’s usefulness in detecting USN-related deficits in object detection and goal-directed navigation. These findings further emphasize that the nature of the tasks (detection vs. navigation) and the environmental complexity are crucial factors to consider when designing assessment and treatment tools for poststroke neglect. These factors, as well as other aspects such as target location and the inclusion of a static and dynamic environments, are difficult to control in a real-world setting and not accounted for in currently employed clinical assessments for USN. We further propose that perhaps, in comparison to traditional USN cancelation tests with distractors (paper-and-pencil test [eg, Bells’ Test 72 ] or computerized tests [eg, Star Cancellation Test 27 ]), EVENS imposes greater demands on attentional resources as it displays a setting in which we aim to mirror a real grocery shopping aisle. Considering this, further empirical research is needed to determine its relevance and clinical usefulness for evaluating and predicting the impact of USN on real-life functional performance.
Additionally, the significant correlations between USN clinical tests and VR task performance refer to the adequate concurrent criterion validity of EVENS. However, the low-magnitude correlations may indicate that the functionality of the VR task, the realism and complexity of the VR scene and EVENS’ immersiveness is likely more sensitive in detecting deficits experienced by individuals with post-stroke USN on daily basis. In addition, EVENS’ applicability and suitability for busy rehabilitation settings are supported by the current study, as the setup, running, and scoring of the entire evaluation took less than 30 minutes; in comparison with the administration and scoring of all clinical tests, which took 40 to 60 minutes.
Limitations
It is acknowledged that only participants with left USN (ie, right hemisphere stroke) were included, limiting the generalizability of results to the left hemisphere stroke population. In addition, EVENS incorporates navigation tasks that did not include a locomotor component. While the performance could worsen during actual locomotion, EVENS presents with the advantage of minimizing the contribution of gait and balance impairments while allowing the examination of attentional-perceptual deficits. Moreover, the motor function of the nonparetic upper extremity used in EVENS was not objectively evaluated in the present study using standardized measures. Thus, one could argue that poststroke, subtle but documented changes in the nonparetic upper extremity function explain the results observed in our group of USN individuals. All participants of this study, however, were able to hold and successfully use a pencil with their right nonparetic hand in cancellation tests and in writing/drawing (eg, consent form, Clock Drawing/Trail Making/Spatial Construction subtests of the Montreal Cognitive Assessment [MoCA]) and presented with no apparent deficits in the nonparetic upper extremity that would prevent them from using the joystick correctly. Most important, the performance of the poststroke USN individuals in this study was significantly altered compared with that of the poststroke individuals without USN who also performed the task with the nonparetic upper extremity. Furthermore, no significant differences in performance were observed between our group of USN− individuals and healthy controls, a finding that is consistent with previous studies where the nonparetic hand was employed for similar tasks (eg, target detection 25 and obstacle avoidance 73 ), and which shows that potential sensorimotor poststroke deficits in the upper extremity did not affect the responses provided with the joystick.
General Conclusion and Future Directions
There are important advantages of the VR design developed in the present study. EVENS offers the potential to assess more functional and complex tasks in individuals with neglect; thus, addressing crucial limitations of the currently available traditional methods and responding to the needs of clinicians for diagnosis, treatment planning, and rehabilitation purposes. Future studies could focus on incorporating an assessment of the feeling of presence, adverse effects, and satisfaction. Furthermore, we aim to bring additional adjustments to EVENS using knowledge translation approach where clinicians and experts in the field were interviewed 74 and an in-depth assessment of its psychometric properties (eg, predictive validity and reliability).
Footnotes
Acknowledgements
We extend our deepest thanks to all study participants, Gevorg Chilingaryan (JRH) for the assistance with statistical analysis and Deian Ivanov for the assistance of Matlab scripts development for analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TO was supported by the Richard & Edith Strauss Fellowship in Rehabilitation Sciences and the Fonds de Recherche du Québec–Santé (FRQS). AL and PA are supported by Salary Awards from FRQS. This project is funded by the Canadian Institute of Health Research (MOP–77548).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.