
Abstract
Background. It may be possible to use attention-based exercise to decrease demands associated with walking in Parkinson’s disease (PD), and thus improve dual task walking ability. For example, an external focus of attention (focusing on the effect of an action on the environment) may recruit automatic control processes degenerated in PD, whereas an internal focus (limb movement) may recruit conscious (nonautomatic) control processes. Thus, we aimed to investigate how externally and internally focused exercise influences dual task walking and symptom severity in PD. Methods. Forty-seven participants with PD were randomized to either an Externally (n = 24) or Internally (n = 23) focused group and completed 33 one-hour attention-based exercise sessions over 11 weeks. In addition, 16 participants were part of a control group. Before, after, and 8 weeks following the program (pre/post/washout), gait patterns were measured during single and dual task walking (digit-monitoring task, ie, walking while counting numbers announced by an audio-track), and symptom severity (UPDRS-III) was assessed ON and OFF dopamine replacement. Pairwise comparisons (95% confidence intervals [CIs]) and repeated-measures analyses of variance were conducted. Results. Pre to post: Dual task step time decreased in the external group (Δ = 0.02 seconds, CI 0.01-0.04). Dual task step length (Δ = 2.3 cm, CI 0.86-3.75) and velocity (Δ = 4.5 cm/s, CI 0.59-8.48) decreased (became worse) in the internal group. UPDRS-III scores (ON and OFF) decreased (improved) in only the External group. Pre to washout: Dual task step time (P = .005) and percentage in double support (P = .014) significantly decreased (improved) in both exercise groups, although only the internal group increased error on the secondary counting task (ie, more errors monitoring numbers). UPDRS-III scores in both exercise groups significantly decreased (P = .001). Conclusions. Since dual task walking improvements were found immediately, and 8 weeks after the cessation of an externally focused exercise program, we conclude that externally focused exercise may improve on functioning of automatic control networks in PD. Internally focused exercise hindered dual tasking ability. Overall, externally focused exercise led to greater rehabilitation benefits in dual tasking and motor symptoms compared with internally focused exercise.
Introduction
Walking, or gait, is believed to be a well-learned series of movements that can be accomplished with minimal conscious control or demand on attention in healthy individuals.1-4 Gait is facilitated by the basal ganglia, especially through motor loops of the dorsal striatum that link with the sensorimotor cortex.1-3,5-8 In individuals with Parkinson’s disease (PD), the dopamine producing cells of the basal ganglia degenerate, initially in dorsal areas of the striatum,6-8 causing dysfunction to automatic control processes. In compensation, individuals with PD shift to a more conscious control of walking,9-13 and as a result there is greater demand on attention resources to control gait (compared with healthy individuals).14-16 Thus, attempting to consciously control walking and complete a secondary task (dual tasking) has been found to overload conscious control resources, causing substantial deterioration to gait in individuals with PD (ie, decreased step length, increased step time, increased percentage of time spent in double support, and increased step-to-step variability).4,10,14-20 Decreased gait amplitude and increased gait variability inherently increase the risk of falling,21-25 injury,26,27 and hospitalization.28,29 Unfortunately, dopamine medications offer limited mitigation to gait impairments exacerbated when walking with and without a secondary task,30,31 suggesting that adjunct rehabilitation is necessary. To improve on the ability to dual task (and thus improve on functioning of one’s automatic control), one possibility may be goal-based exercise rehabilitation that strives to draw attention to impaired movements as they are being performed.
While performing a movement, individuals can direct their focus of attention toward the effect of an action on the environment (eg, toward the club head during a golf putt, 32 toward pushing water backward while swimming,33,34 or on the movement of tape attached to one’s chest during a gymnastics jump 35 ), or toward their limbs to ensure movement accuracy. Task performance is typically more successful in healthy individuals when focus of attention is directed toward the effect of an action on the environment (ie, external focus) compared with the completion of movements while attention is focused toward controlling one’s limbs (ie, an internal focus).36-41 It has been argued, and neural imaging has supported, that an external focus of attention naturally promotes recruitment of automatic processes (sensorimotor cortical areas) indicative of automatic movement control, providing benefits to performance.42,43 In contrast, it has been argued that an internal focus of attention promotes a more conscious control of movement (that recruits frontal areas) that can be detrimental to motor performance.42,43 However, one might expect then that since individuals with PD have dysfunctional automatic processes, adopting an internal focus of attention might prove beneficial to movement control. This is especially the case when instructing patients with PD to focus on taking larger steps (ie, an internal focus) positively influences gait.44-46 Interestingly, when individuals with PD were asked to control postural stability on an inflated disk placed over a force-plate (to increase task difficulty) while ON dopamine medication, significantly less postural sway (improved control) was found when participants were instructed to focus attention on minimizing movements of the platform (external focus) compared with minimizing movements of their feet (internal focus). 47 In a similar paradigm, it was uncovered that an external focus of attention was found to be detrimental to control of postural stability in PD compared with an internal focus while participants were OFF dopamine medications. 48 These findings may suggest that an external focus of attention recruits automatic processes that include the basal ganglia, and when individuals with PD are ON dopaminergic medication, they are able to effectively use their automatic processes to perform movements, and this proves beneficial for overall motor control.47,48 However, due to years of progressive basal ganglia degeneration and conscious compensation,6-8,49,50 individuals with PD either refrain from, or are unable to effectively use their automatic processes, regardless of whether the automatic networks function properly. Therefore, by combining a goal-based exercise program that trains specific aspects of walking with an external focus of attention, ability to dual task might be improved through enhanced automatic control.
Thus, the present study aimed to investigate if combining a goal-based exercise program with an external focus of attention might improve on dual task walking in individuals with PD. It was expected that if an external focus of attention does promote the use of automatic control networks while completing a goal-based exercise program, then improvements to dual task walking might be fostered in individuals with PD. In contrast, promoting an internal focus of attention during goal-based exercise might hinder dual task walking performance since this training may increase reliance on conscious control of movement. The present study further aimed to explore the influence of external and internal focus of attention exercise on motor symptom severity. Since automatic processes rely on basal ganglia function, it was expected that goal-based exercise combined with an external focus would lead to greater improvements to motor symptoms when compared with an internal focus, which it is argued promotes use of conscious control networks less influenced by the basal ganglia. Finally, if changes to neuronal connections took place after the present intervention to either automatic and/or conscious control networks, one might expect that changes to dual task walking behavior should persist for a given period of time after cessation of the exercise intervention.44,51-56 Therefore, we also sought to explore whether changes to gait and symptom severity as a result of a goal-based exercise program persist throughout an 8-week washout period.
Methods
Participants
Participants diagnosed with idiopathic PD by a neurologist (using the UK Parkinson’s Disease Society Brain Bank clinical diagnostic criteria 57 ) were randomly recruited from the Movement Disorders Research and Rehabilitation Centre (MDRC) exercise database at Wilfrid Laurier University, Waterloo, Canada. Participants of both genders were included in the present study if they possessed the ability to understand verbal instructions in English, were able to walk 10 m unassisted, and able to stand for 5 minutes unassisted. Exclusion criteria included a diagnosis of a neurological disease other than PD, peripheral neuropathy, diabetes, or a clinical diagnosis of dementia (as confirmed by their most recent Montreal Cognitive Assessment and/or the Modified Mini-Mental State score available from the MDRC database). Prior to any evaluation or participation in exercise, written informed consent was obtained from individuals interested in participation according to the Declaration of Helsinki. The Research Ethics Board at Wilfrid Laurier University granted full ethical approval of this research study. This study was registered with the U.S. National Institute of Health (ClinicalTrials.gov Identifier: NCT02476240). All individuals included in the rehabilitation program completed a Physical Activity Readiness Medical Examination signed by a physician prior to the rehabilitation program.
Study Design and Exercise Intervention
The present study was a parallel group, single blind (assessment evaluators were blinded to group allocation), randomized controlled trial. Individuals with PD interested in participating, and who fit the inclusion criteria, were asked to visit the MDRC one week prior to the exercise program for preassessment. Afterward, participants interested in the exercise program were randomized (via computerized randomization) to 1 of 2 groups:
External Focus of Attention Exercise (External)—Participants were consistently instructed to focus on the movement of colored labels attached to the posterior side of their hands (red label), medial epicondyle of the humerus (yellow label), superior aspect of the patella (green label), and dorsal aspect of the foot (blue label; Figure 1). An example of instruction given to this group during a knee raise movement was “focus on pushing the green label up in a slow, controlled manner.” Directing one’s focus toward labels attached to his or her body is an effective method of achieving an “external focus” thus leading to benefits in movement performance. 35
Internal Focus of Attention Exercise (Internal)—Participants were consistently instructed to focus on the movement of their limbs in physical space. An example of instruction given to this group during a knee raise movement was “focus on lifting your knee up in a slow, controlled manner.”
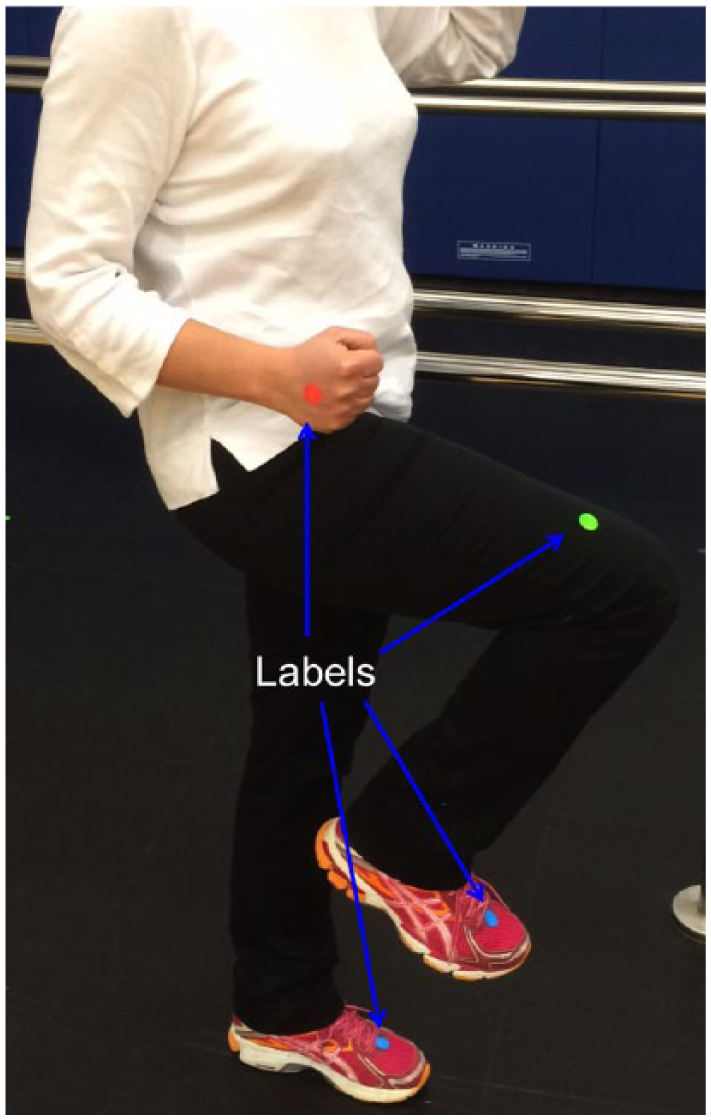
Participants randomized to the External focus of attention exercise group wore colored labels on the posterior side of their hands (red label), medial epicondyle of the humerus (yellow label), superior aspect of the patella (green label), and dorsal aspect of the foot (blue label). These individuals were consistently instructed to focus on the movement of the colored labels.
Individuals who did not believe they could meet the necessary time commitment for involvement in the program, but were interested in participating, were assigned to the:
Nonactive Control Group—Participants were asked to continue with their normal daily routine.
Participants were not randomized to the nonexercise control group for 3 reasons: (1) the purpose of this group was only to serve as an important reference point; (2) it was suggested to be unethical by the ethics board at Wilfrid Laurier University to randomize participants into a nontreatment group, as it could be seen as withholding a treatment to people who had registered to be involved in exercise studies when enrolling into the MDRC database of participants with Parkinson’s disease; and (3) previous exercise rehabilitation experiments have demonstrated that attrition rates/dropouts for people randomly assigned in the control group would leave this group with a very small number.
The exercise program commenced 1 week after preassessment and lasted 11 weeks. Participants in the exercise groups completed walking, balance, stretching, and coordination exercises each session, following the Parkinson’s disease Sensory Attention Focused Exercise (PD-SAFEx) program. 45 Both exercise groups completed the PD-SAFEx program identically (type of movements completed, number of sets, repetitions and sets completed). The only difference between exercise groups was the location (external vs internal) in which the trained exercise instructor directed participants’ attention toward with regard to their movements. Each exercise session duration was 60 minutes and was completed 3 times per week. Postassessment took place 1 week immediately after the cessation of the exercise program. A washout assessment took place 8 weeks after the cessation of the intervention, a period of time in which participants were asked to continue activities of daily living, but not asked to attend exercise sessions, or make adjustments to their medications. The control group did not participate in the washout evaluation since any changes that may have occurred over the intervention period would not be expected to differ over another subsequent 8 weeks. Participants completed all exercise sessions in the ON dopaminergic state. Figure 2 presents the participant recruitment, randomization, assessment time points, and withdraws.
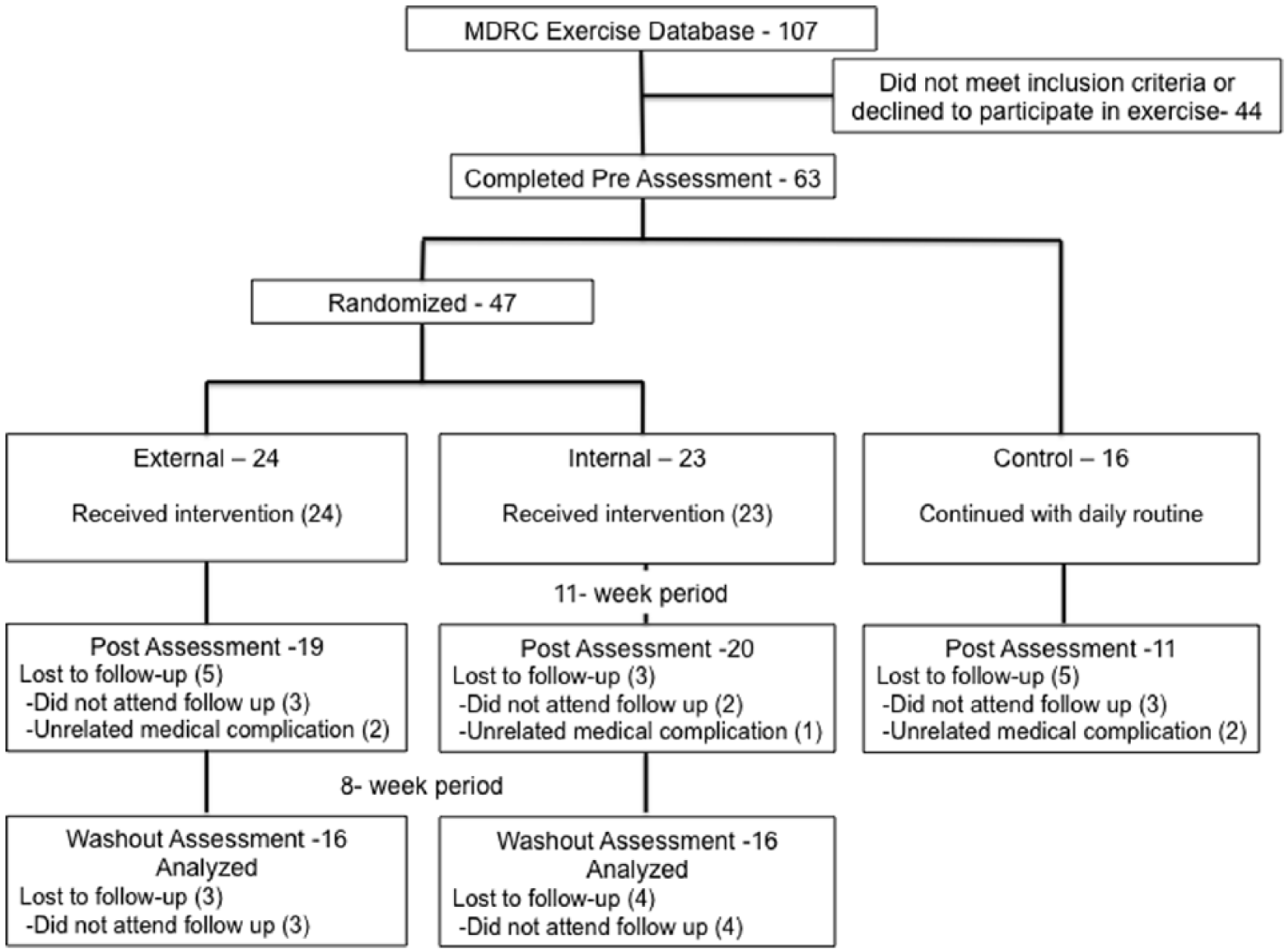
Profile flowchart for the present single-blind randomized controlled trial.
Outcome Measures
Primary Outcome Measures
Two primary outcome measures were used in the present randomized controlled trial, one instrumental and one clinical.
The degree to which gait was affected by a dual task served as the instrumental primary outcome measure. Before walking parameters could be tested, participants completed 3 seated trials of the secondary task to familiarize them with the protocol and to assess baseline ability. For a full description of the secondary task, see Beck et al. 20 In brief, participants listened to an audio track of numbers between 1 and 9. They were assigned 2 digits and asked to count (without manual aid) the number of times they heard the 2 assigned digits announced by the audio track, separately. When the trial ended, participants informed the researcher of the number of times they heard each digit. The difference between participants’ response and the actual number of digits that were announced by the audio track was calculated. Therefore, the degree to which participants prioritized the digit-monitoring task compared with walking could be quantified. During walking trials, participants were asked to walk across a 9.75 m long and 0.61 m wide electronic walkway carpet (Zeno Walkway—ProtoKinetics, Havertown, PA, USA) at a comfortable pace. Participants began walking 2 m before the start of the Zeno Walkway to avoid collecting acceleration, and to continue walking past the end of the Zeno Walkway to avoid collecting deceleration. Two walking tasks were assessed. Three single task, and 3 dual task (walking while simultaneously completing the digit-monitoring secondary task) walking trials were completed in random order after the seated baseline assessment of the secondary task performance.
The primary clinical outcome measure was motor symptom severity measured with the Unified Parkinson’s Disease Rating Scale Motor Section (UPDRS subsection III) in participants while they were both OFF (>12 hours withdrawal from dopaminergic medication) and ON (1 hour after taking their normal dopaminergic medication) their dopaminergic medication. The UPDRS-III assessment has been found to reflect the level of dopamine present in the basal ganglia. 58 Therefore, the purpose of assessing the UPDRS-III both OFF and ON dopaminergic medications was to investigate the effects of the exercise program on endogenous basal ganglia function without and with the influence of exogenous dopamine, respectively, that has been found to mask true UPDRS-III improvements after an exercise intervention. 59
Secondary Outcome Measures
To control for any patient characteristics that may influence the effect of the exercise program on the primary outcome measures, several secondary outcome measures were also collected. Since physical activity levels prior to participation in an exercise program can influence the degree of benefit the program provides, the Community Health Activities Model Program for Seniors questionnaire (CHAMPS) was used. The CHAMPS questionnaire is a validated self-report measure used to quantify how physically active one has been during the previous 4 weeks. 60 General cognitive status was also evaluated with the Montreal Cognitive Assessment (MoCA), and the participants’ perceived quality of life was quantified with the 39-item Parkinson’s disease Questionnaire (PDQ-39). Last, although participants were asked to refrain from changing any aspects of their Parkinsonian medication regime throughout the duration of the study, levodopa equivalent dose (LED) was calculated for each assessment time point. 61
Evaluation at Pre, Post, and Washout Assessments
During preassessment, postassessment, and washout evaluation time points, participants visited the centre while in the OFF medication state, unless they opted out of the OFF medications UPDRS-III assessment portion of the research study (External n = 2; Internal n = 2; Control n = 1). UPDRS-III assessment was completed immediately by a movement disorders specialist, whom at pre, post, and washout assessments was blinded to which group participants were randomized and to whom was allocated to the control group. Participants subsequently took their normal dopaminergic medications and completed the CHAMPS questionnaire while the medications were digested. After one hour ON medications,30,62 participants were re-assessed with the UPDRS-III assessment by the same (blinded) movement disorders specialist.
After the ON medication UPDRS-III assessment, the degree to which gait was affected by a dual task was evaluated following the protocol presented previously in the Outcome Measures subsection. After walking trials were completed, participants’ general cognitive status was evaluated with the MoCA, and the participants’ perceived quality of life was quantified with the PDQ-39 questionnaire.
Data and Statistical Analysis
Seven participants from the exercise groups, and all participants in the control group, did not complete the washout assessment. Since the purpose of the washout assessment was to determine whether gait measures and motor symptoms revert back to preassessment levels or persist, data from participants who withdrew after postassessment, and data from the control group, were not carried forward. Instead, statistical analysis was divided into 2 parts: part A included analysis of External, Internal, and Control participant assessments at pre- and postexercise, while part B included analysis of only those participants in the External and Internal groups who completed pre, post, and washout. Therefore, part A analysis allowed for comparison of both intervention groups with an important nonexercising reference point, to control for learning effects and natural disease progression. Part B allowed for a more controlled analysis between the External and Internal interventions without sample bias. Tukey’s post hoc and alpha level of P < .05 were used for all statistical analyses in this study.
Participant Demographics
Part A: Pairwise comparisons between the External, Internal, and Control group means were conducted (95% confidence intervals [CIs]) to determine whether age, number of years since diagnosis, body weight, or exercise program adherence ([No. of classes attended/33] × 100; only between External and Internal) were different among groups at preassessment.
Part B: Independent-samples t tests were used to identify preassessment differences between groups with respect to age, number of years since diagnosis, body mass, and percentage adherence.
Primary Outcome Measures
ProtoKinetics Movement Analysis Software (ProtoKinetics, Havertown, PA, USA) was used to analyze the primary instrumental outcome measure, spatiotemporal gait parameters. First and last footfalls were removed offline. Left and right footfalls were collapsed. The Zeno Walkway captured the following spatiotemporal gait characteristics that were used in the statistical analyses: (1) step length (cm), (2) step length variability (coefficient of variation [CV]), (3) step time (seconds), (4) step time variability (CV), (5) double support time percentage (DST%), (6) DST% variability (CV), and (7) velocity (cm/s). Statistical analysis in parts A and B were as follows:
Part A: Pairwise comparisons within (differences between pre- and postassessment; differences between single and dual task walking) and between the External, Internal and Control group means were conducted (95% CIs) with regard to each gait parameter. Error on the digit-monitoring task was calculated after both the baseline (seated) and the dual task walking conditions. The 3 baseline and dual task conditions were then averaged (separately), 20 and pairwise comparisons (95% CIs) within and between groups were conducted.
Part B: Four-factor mixed repeated-measures analysis of variance (ANOVA) (2 groups × 3 evaluation times × 2 tasks × 3 trials) assessed group differences and changes at each evaluation time point. Performance on the secondary task was assessed with a 3-factor mixed repeated-measures ANOVA (2 groups × 3 evaluation times × 2 tasks).
The primary clinical outcome measure, UPDRS-III score, was statistically analyzed as follows:
Part A: Pairwise comparisons within (differences between pre- and postassessment; differences between medication states) and between the External, Internal, and Control group means were conducted (95% CIs) with regard to UPDRS-III while participants were both ON and OFF dopaminergic medications.
Part B: Three-factor mixed repeated-measures ANOVA (2 groups × 3 evaluation times × 2 medication states).
Secondary Outcome Measures
Part A: Pairwise comparisons within (differences between pre- and postassessment) and between the External, Internal, and Control group means were conducted (95% CIs) with regard to LED, MoCA, CHAMPS, and PDQ-39.
Part B: Two-factor mixed repeated-measures ANOVA were used (2 groups × 3 evaluation times) to determine whether significant differences were present with regard to LED and CHAMPS.
Results
Figure 2 presents the participant recruitment, randomization, assessment time points, and withdraws from the study. Both exercise rehabilitation programs were well tolerated, and no adverse effects related to the PD SAFEx exercise programs were reported.
Participant Demographics
Part A: All participant demographics can be found in Table 1.
Part A Participant Demographics, Primary Clinical Outcome Measure (UPDRS-III Scores), and Secondary Measure Outcomes as Group Averages (Standard Deviation in Parentheses). a
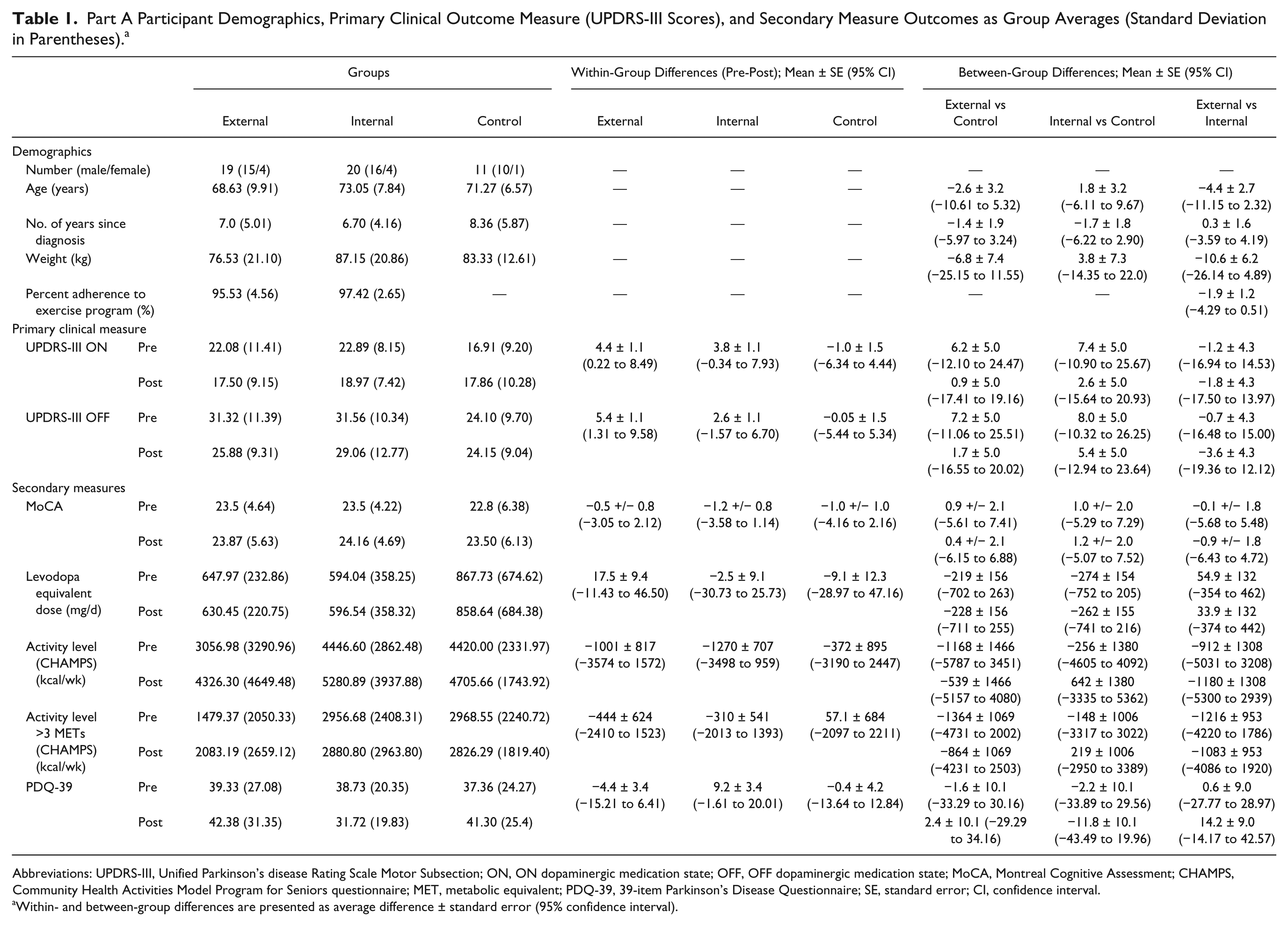
Abbreviations: UPDRS-III, Unified Parkinson’s disease Rating Scale Motor Subsection; ON, ON dopaminergic medication state; OFF, OFF dopaminergic medication state; MoCA, Montreal Cognitive Assessment; CHAMPS, Community Health Activities Model Program for Seniors questionnaire; MET, metabolic equivalent; PDQ-39, 39-item Parkinson’s Disease Questionnaire; SE, standard error; CI, confidence interval.
Within- and between-group differences are presented as average difference ± standard error (95% confidence interval).
Part B: Participant demographic effects can be found in Table 2. No significant effects were uncovered.
Part B Participant Demographics, Primary Clinical Outcome Measure (UPDRS-III Scores), and Secondary Measure Outcomes as Group Averages (Standard Deviation in Parentheses).
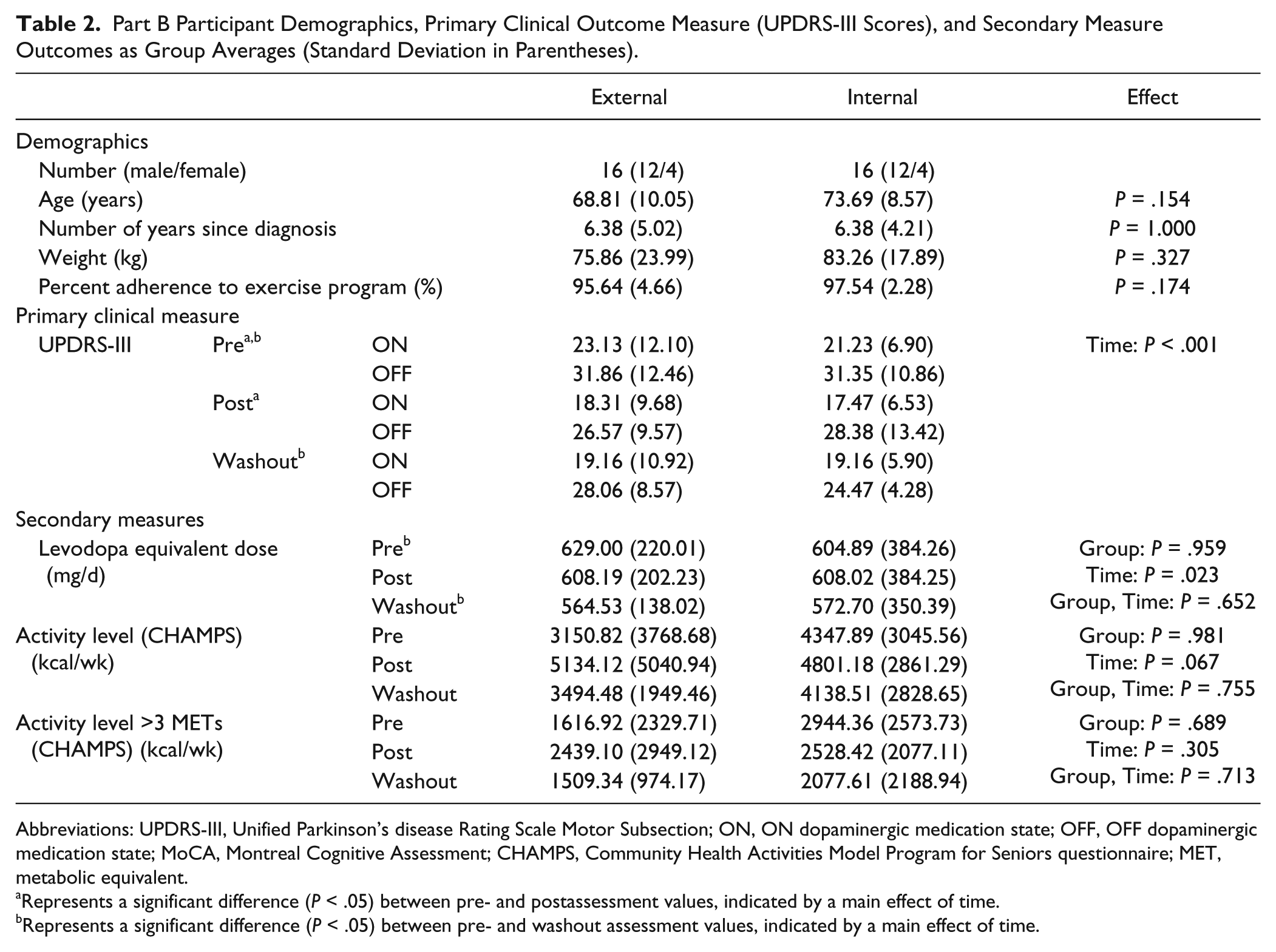
Abbreviations: UPDRS-III, Unified Parkinson’s disease Rating Scale Motor Subsection; ON, ON dopaminergic medication state; OFF, OFF dopaminergic medication state; MoCA, Montreal Cognitive Assessment; CHAMPS, Community Health Activities Model Program for Seniors questionnaire; MET, metabolic equivalent.
Represents a significant difference (P < .05) between pre- and postassessment values, indicated by a main effect of time.
Represents a significant difference (P < .05) between pre- and washout assessment values, indicated by a main effect of time.
Primary Outcome Measures
With regard to the primary instrumental outcome measure, gait parameters, the findings uncovered in parts A and B were as follows:
Part A
To confirm the effectiveness of the secondary task, pairwise comparisons demonstrated that all groups were influenced (as expected) by the addition of a secondary counting task. In particular, at pre and post assessment, participants walked with shorter step length (95% CI External pre = 0.97 to 3.85, post = 1.24 to 4.13; Internal pre = 2.15 to 5.04, post = 3.87 to 6.76; and Control pre = 1.74 to 5.50, post = 0.47 to 4.24), greater DST% (CI External pre = −2.89 to −1.16, post = −2.90 to −1.17; Internal pre = −2.80 to −1.07, post = −4.04 to −2.32; and Control pre = −3.10 to −0.84, post = −2.36 to −0.11), and slower velocity (CI External pre = 3.28 to 11.17, post = 4.32 to 12.22; Internal pre = 3.58 to 11.47, post = 8.25 to 16.15; and Control pre = 3.87 to 14.16, post = 1.55 to 11.84) while dual task walking compared with the single task walking.
Of most importance, single (CI 0.007 to 0.04) and dual tasking (CI 0.01 to 0.04) step time decreased from preassessment to post in the External group. In contrast, participants in the Internal group walked with a shorter step length (CI 0.86 to 3.75) and slower velocity (CI 0.59 to 8.48) while dual task walking at postassessment compared with pre. All within- and between-group pairwise comparisons, with regard to gait parameters, are presented in Table 3. The number of errors made on the secondary digit-monitoring task, while dual task walking, increased from preassessment to post by 9.82% (increase in absolute error by 0.20) in the External group, 1.28% (increase in absolute error by 0.04) in the Internal group, and 33.06% (increase in absolute error by 0.62) in the control group (Table 3).
Part A Gait Parameter and Absolute Error on the Secondary Digit-Monitoring Task Averages (Standard Deviations in Parentheses), Significant Main Effects, and Interactions. a
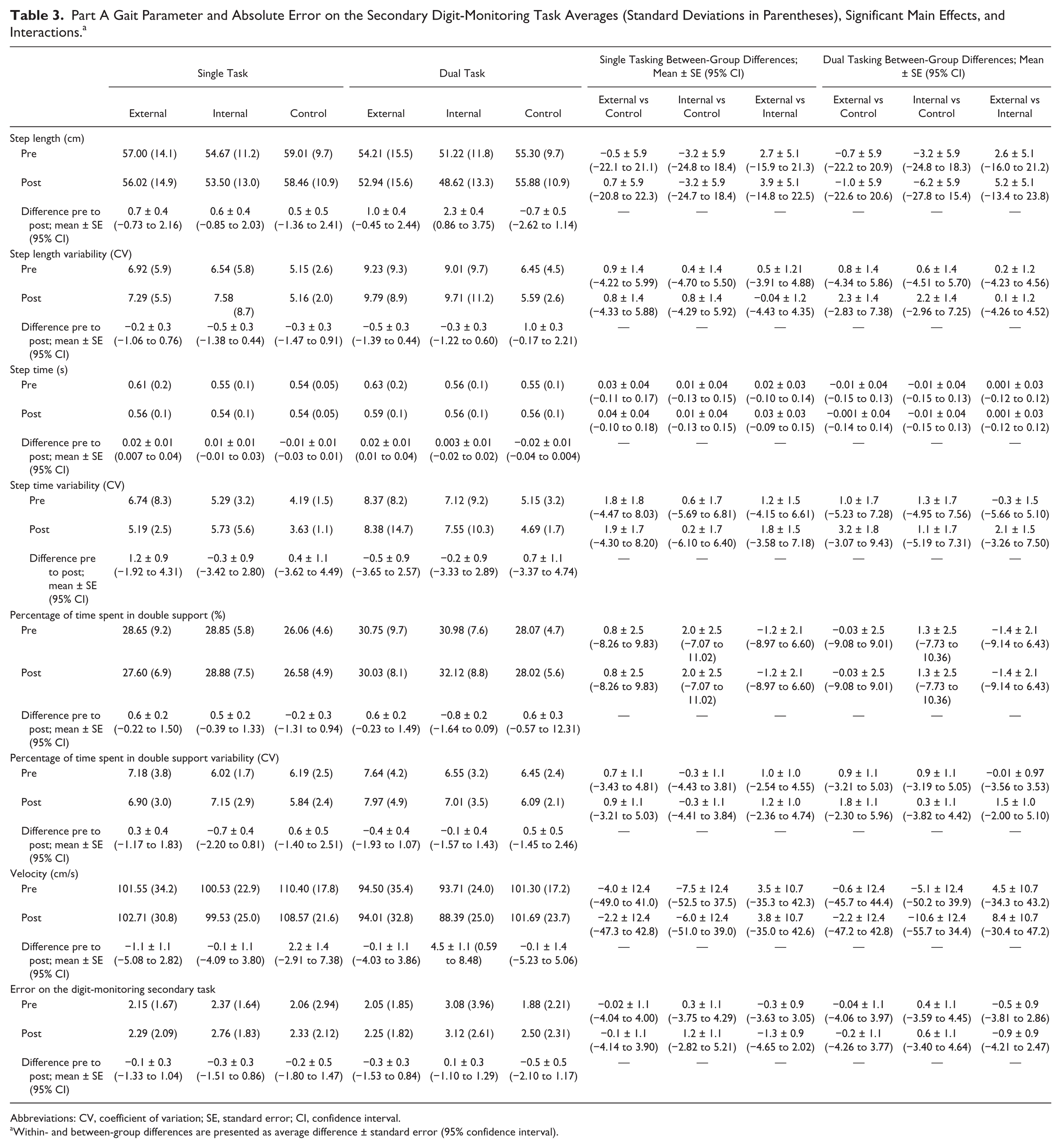
Abbreviations: CV, coefficient of variation; SE, standard error; CI, confidence interval.
Within- and between-group differences are presented as average difference ± standard error (95% confidence interval).
Part B
When we compared single with dual task walking, with regard to step length, a significant interaction between group and task was found, F(1, 23) = 4.56, P = .044, and post hoc revealed that both the External and Internal groups walked with a significantly shorter step length while dual task walking compared with single task walking (P < .02). Main effects of task were found, and demonstrated that participants walked with a significantly greater step length variability, F(1, 23) = 11.07, P = .003; step time, F(1, 23) = 7.60, P = .011; step time variability, F(1, 23) = 5.87, P = .023); DST%, F(1, 23) = 38.40, P < .001; and slower velocity, F(1, 23) = 39.15, P < .0001; while dual task walking compared with single task walking.
The most important finding from part B came from the significant main effects of evaluation time, with regard to step time, F(2, 46) = 5.43, P = .008 and DST%, F(2, 46) = 4.25, P = .02. The post hocs for these main effects of time demonstrated that both the External and Internal groups walked (both single and dual task walking) with shorter step time (P = .005) and DST% (P = .014) as washout assessment compared with pre. Table 4 presents all part B gait parameter main effects and interactions. No significant main effects or interactions were found for performance on the secondary digit-monitoring task employed during the dual task walking trials (Table 4). However, it is important to note that participants in the External group increased the number of errors on the secondary task while dual task walking by 6.44% (increase in absolute error by 0.14) from preassessment to post, 5.45% (increase in absolute error by 0.11) from preassessment to washout, and decreased error by 0.93% (decrease in absolute error by 0.02) from postassessment to washout. The Internal group decreased the number of errors on the secondary task while dual task walking by 0.33% (decrease in absolute error by 0.01) from preassessment to post, and increased number of errors on the secondary task while dual task walking by 41.56% (increase in absolute error by 1.39) from preassessment to washout, and 42.04% (increase in absolute error by 1.40) from postassessment to washout.
Part B Gait Parameter and Absolute Error on the Secondary Digit-Monitoring Task Averages (Standard Deviations in Parentheses), Significant Main Effects, and Interactions.
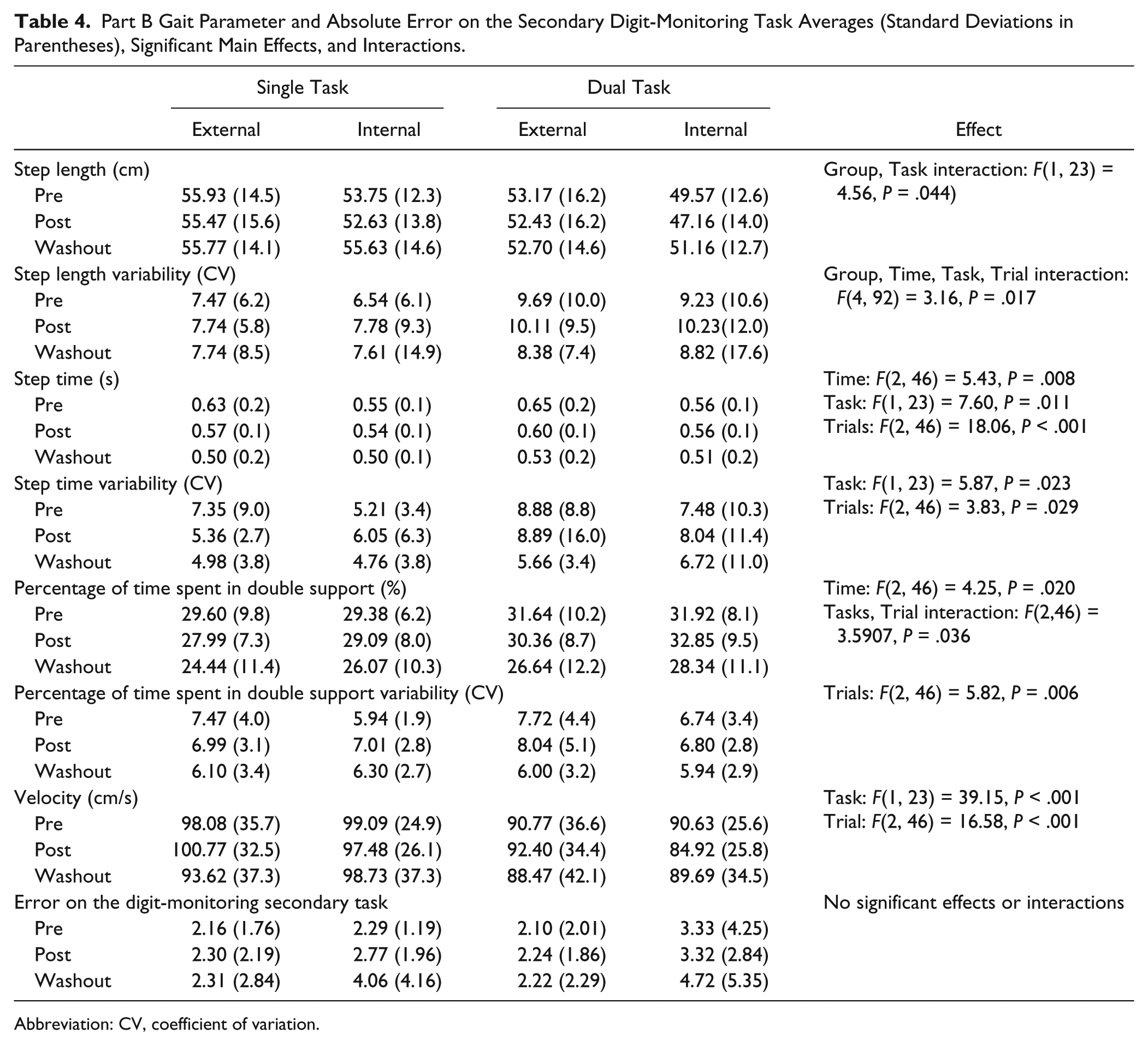
Abbreviation: CV, coefficient of variation.
With regard to the primary clinical outcome measure, UPDRS-III scores, the findings uncovered in Parts A and B were as follows:
Part A: Pairwise comparisons demonstrated that UPDRS-III scores were greater in the OFF medication state compared with the ON state, regardless of evaluation time (CI External pre = −14.08 to −5.81, post = −12.99 to −4.72; Internal pre = −13.61 to −5.34, post = −14.84 to −6.57; and Control pre = −14.29 to −3.51, post = −13.39 to −2.61). Both ON and OFF dopamine medication UPDRS-III scores decreased from preassessment to post in only the External group (CI ON = 0.22 to 8.49, OFF = 1.31 to 9.58) (see Table 1).
Part B: A significant main effect of evaluation time, F(2, 52) = 11.09, P < .001, was found for UPDRS-III, and Tukey’s post hoc revealed that both groups demonstrated significantly lower UPDRS-III scores at post and washout assessments compared to pre (see Table 2).
Secondary Outcome Measures
Part A: All secondary measures can be found in Table 1.
Part B: All secondary measures can be found in Table 2. The only significant difference was a main effect of evaluation time with regard to LED, F(2, 60) = 4.04, P = .023, and Tukey’s post hoc revealed that LED significantly decreased from pre assessment to washout (P = .026).
Discussion
This is the first single-blind randomized controlled trial investigating the effects of goal-based exercise with either an External or Internal focus of attention on dual task walking and motor symptom severity in individuals with PD. Findings from part A analysis demonstrated that one gait parameter, step time, improved (ie, decreased) while dual task walking from preassessment to post in the External group (Table 3). However, since findings from part B analysis did not demonstrate that gait during the dual task significantly improved from pre to post in the External group, our hypothesis that externally focused exercise might improve dual tasking in individuals with PD was not supported. These results might suggest that either the external focus of attention exercise did not improve on functioning of participants’ automatic control networks, that improvements to automatic processes did not translate to walking, or that improvements to the functioning of automatic processes began to emerge (improved dual tasking step time at post compared with pre) but a longer exercise program may be necessary to fully improve on the complex neuronal connections associated with dual task walking. It should be pointed out, however, that lack of improvements in dual task walking from preassessment to post cannot likely be attributed to the difficulty of the secondary task. If the digit-monitoring secondary task was not challenging enough, neither gait impairments nor error on the digit-monitoring task would be expected to precipitate while dual task walking. However, the digit-monitoring task resulted in significantly greater gait impairment compared with single task walking. This would suggest that the counting task was challenging enough to effectively load cognitive processes that are typically recruited while walking in individuals with PD. The low task absolute error (approximately 2-3 errors) indicates both that the participants were focusing attention on the task (as opposed to prioritizing walking), and that the task was not too difficult for participants to perform.
Interestingly, dual tasking step length and velocity decreased from preassessment to post in the Internal group (Table 3). These findings might suggest that an internal focus of attention during goal-based exercise increased reliance on a less damaged compensatory conscious control system, in that control of gait became more consciously demanding.6-11,51 This may have left participants more susceptible to deterioration in gait parameters when attentional focus was directed away from one’s own movements. To investigate further whether gait changes persisted throughout a washout period, and therefore whether changes to neuronal connections potentially took place after the present intervention to either automatic and/or conscious control networks, gait was measured 8-weeks after the exercise program ended.44,51-56
The results from part B of the present study illustrate that from preassessment to washout, both groups demonstrated significantly decreased step time and DST% while single and dual task walking. However, the External group demonstrated an increased secondary task error of only 5.45%, whereas the Internal group increased error on the secondary task by 41.56%. This suggests that at washout, the External group prioritized the secondary task and demonstrated significant improvements to dual task walking. In contrast, the internal group prioritized walking instead of the secondary task, which most likely reflects that improvement to step time and DST% were the result of consciously controlling gait, and not representing improved dual task ability. It should be noted that with regard to error on the secondary task, no significant interaction was found, only anecdotal differences illustrated in Figure 3. However, Yogev-Seligmann et al 44 have previously demonstrated that a nonsignificant change in secondary task performance of 13.87% reflects a change in explicit prioritization from the secondary task toward gait. Thus, these findings might suggest that improvements to dual task ability induced by external focus of attention exercise could have been subject to a delayed effect, in that the exercise program may have provided the training foundation necessary to enhance automatic processes (illustrated by improved step time at post compared with pre, part A analysis), but more time was needed to further establish an efficient use of this information (significant improvements in step time and DST% at washout compared with pre, part B analysis). To gain further understanding of the potential effects that the differing exercise instructions had on the underlying function of automatic and conscious control networks, we explored the influence of externally and internally focused exercise on UPDRS-III scores that reflect basal ganglia function, 58 central to automatic control.
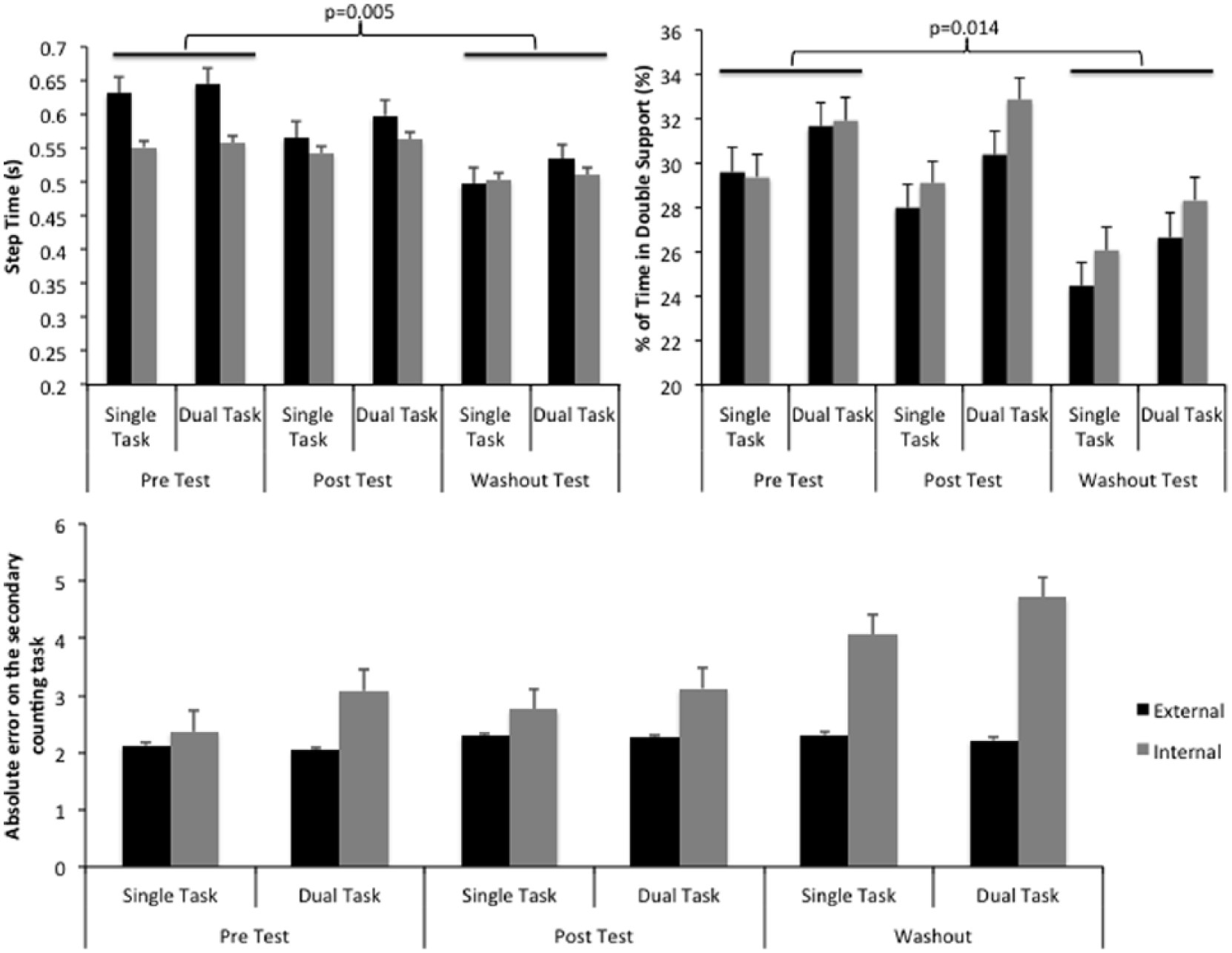
Graphical illustrations of significant gait parameter main effects of evaluation time (pre, post, and washout) with regard to step time (top left) and percentage of time in double support (top right). Absolute error (AE) on the secondary digit-motoring task can also be found in the bottom graph. Participants in the External group increased the number of errors on the secondary task while dual task walking by 6.44% (increase in AE by 0.14) from preassessment to post, 5.45% (increase in AE by 0.11) from preassessment to washout, and decreased error by 0.93% (decrease in AE by 0.02) from post assessment to washout. The Internal group decreased the number of errors on the secondary task while dual task walking by 0.33% (decrease in AE by 0.01) from preassessment to post, and increased number of errors on the secondary task while dual task walking by 41.56% (increase in absolute error by 1.39) from preassessment to washout, and 42.04% (increase in absolute error by 1.40) from postassessment to washout.
Part A analysis demonstrated that UPDRS-III scores, both ON and OFF dopaminergic medications, improved from preassessment to post in only the external focus of attention exercise group (UPDRS-III changes: External OFF = −5.40, ON = −4.58; Internal OFF = −2.56, ON = −3.92; Control OFF = +0.05, ON = +0.95). Importantly, the OFF medication improvement in UPDRS-III scores from pre to post assessment in the external group was the only change to reach minimal clinical importance (greater than a 5-point change). 63 Moreover, both ON and OFF UPDRS-III improvements in the external group surpassed the clinical important difference of 4.5 points defined by Shulman et al. 64 These results might suggest that since the UPDRS-III assessment reflects functionality of the basal ganglia (especially OFF medications in which dopamine replacement is not masking endogenous functioning), externally focused exercise may have improved basal ganglia function,65-68 whereas internally focused exercise did not to the same capacity. This potential benefit to basal ganglia functioning may have provided the foundation for improved dual task walking (improved automatic control processes) that were found at postassessment and washout.
The final important finding to report was a significant main effect of evaluation time, which demonstrated that UPDRS-III scores were significantly lower at postassessment compared with pre, and persisted at this level 8 weeks after the exercise program had ceased. What is most unique about these findings is that despite our instructions to participants to refrain from changing aspects of their dopaminergic medication regime, participants required significantly less dopaminergic medications consumed each day from preassessment to washout. Therefore, improved symptom severity persisted for 8 weeks after cessation of the exercise program despite decreased levels of dopamine consumed each day. Because of a realm of unpleasant side effects that may accompany medications, these findings are novel and carry great clinical importance. Since critical findings in the present study demonstrated a significant improvement in gait from preassessment to washout that paralleled a significant decrease in LED, one might contest that improvements to gait and LED were somehow linked. However, this is unlikely, and in fact one might predict that with decreased LED at washout, motor symptoms, including gait, should have worsened (also at washout). Our results show the exact opposite trend. Furthermore, as was stated in the introduction, many gait parameters do not respond to dopamine medications, and would therefore not be expected to change with a lower dose. If anything, this strengthens the likelihood that gait changes were due to the effects of the intervention and not the result of changes to medication.
A final point that may be important to consider is the lack of between group differences at post and washout assessment, in both parts A and B with respect to single or dual task gait parameters, error on the secondary digit-monitoring task, and ON/OFF UPDRS-III scores. While the current results do not suggest that Externally focused exercise improves dual tasking ability or motor symptoms compared with internally focused exercise, they do however, for the first time, provide evidence that externally focused exercise may improve on dual task walking ability with a greater improvement to symptom severity, when compared with internally focused exercise that actually hinders dual task walking with a lesser improvement to overall motor symptoms. The lack of significant between-group differences at post and washout may be due to the intensity and/or length of the exercise program; in that more exercise sessions or a longer program (>11 weeks) may be necessary to establish between-group differences. This highlights an important direction for future research, given the trends that were observed.
Limitations/Future Directions
A number of limitations were evident in this study, providing direction for future research. First, a suboptimal external focus of attention method may have been employed. Previous investigations have demonstrated that when participants are instructed to focus “externally” on the movement of a marker attached to a platform (participants stand on the platform and control its movement via postural stability), movement performance improves as the marker is placed further from the participant’s body. 69 Therefore, since the colored labels were situated on the patients’ limbs in the present study, we may not have utilized the most effective externally focused method, which may have impeded optimal rehabilitative benefits surmounting to no differences found between groups at post and washout, as discussed above. However, by using labels attached to participants’ limbs, we promoted a research-supported method of eliciting an external focus of attention 35 while ensuring parsimony and ecological validity. Second, the MoCA and PDQ-39 were not assessed at the washout in the present study. Since walking ability, symptom severity, cognitive status and quality of life are all closely related, 70 decrements to cognitive ability and/or perceived quality of life may have influenced improvements in dual task walking and symptom severity found at the washout assessment. By not measuring MoCA and PDQ-39 at washout, stronger conclusions could not be made. Third, data from a nonexercise control group was not collected at the washout assessment. Therefore, any significant changes revealed at washout may have been the result of a learning effect, although unlikely due to the amount of time between assessments (ie, 11 weeks from pre to post and 8 weeks from post to washout). Fourth, although it was a welcomed surprise to find significant decreases in LED from preassessment to washout, these changes paralleled improvements to gait found at washout compared to preassessment. Although we asked participants to not change any aspects of their medications throughout the study, it is an inherent limitation of exercise research that patients may make changes to medications despite our instructions. It is for this reason that we collected LED. Last, as mentioned in the methods, we did not randomize patients into the nonexercise control group, and acknowledge the bias associated with this decision. However, since a separate analysis was run that discarded the nonexercise control group, this bias was accounted for.
Conclusion
Dual task walking improvements were found immediately, and 8 weeks after the cessation of an externally focused exercise program. These findings suggest that external focus of attention exercise may improve on functioning of automatic control networks in Parkinson’s disease. Internal focus of attention exercise proved detrimental to dual task walking in individuals with Parkinson’s disease. Finally, although benefits to motor symptoms were found after both externally and internally focused exercise, focusing externally on the effect of an action on the environment while exercising provided greater improvements to UPDRS-III scores in Parkinson’s disease.
Footnotes
Acknowledgements
We would like to thank all of the individuals who participated in this study for their tireless effort and passion. We would also like to thank Professor Gabriele Wulf for her consultation and recommendations regarding the methodology of the present study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Canada Foundation for Innovation to Quincy J. Almeida (Grant No.: 20774).