
Abstract
Background. Although rehabilitation therapy is commonly provided after stroke, many patients do not derive maximal benefit because of access, cost, and compliance. A telerehabilitation-based program may overcome these barriers. We designed, then evaluated a home-based telerehabilitation system in patients with chronic hemiparetic stroke. Methods. Patients were 3 to 24 months poststroke with stable arm motor deficits. Each received 28 days of telerehabilitation using a system delivered to their home. Each day consisted of 1 structured hour focused on individualized exercises and games, stroke education, and an hour of free play. Results. Enrollees (n = 12) had baseline Fugl-Meyer (FM) scores of 39 ± 12 (mean ± SD). Compliance was excellent: participants engaged in therapy on 329/336 (97.9%) assigned days. Arm repetitions across the 28 days averaged 24,607 ± 9934 per participant. Arm motor status showed significant gains (FM change 4.8 ± 3.8 points, P = .0015), with half of the participants exceeding the minimal clinically important difference. Although scores on tests of computer literacy declined with age (r = −0.92; P < .0001), neither the motor gains nor the amount of system use varied with computer literacy. Daily stroke education via the telerehabilitation system was associated with a 39% increase in stroke prevention knowledge (P = .0007). Depression scores obtained in person correlated with scores obtained via the telerehabilitation system 16 days later (r = 0.88; P = .0001). In-person blood pressure values closely matched those obtained via this system (r = 0.99; P < .0001). Conclusions. This home-based system was effective in providing telerehabilitation, education, and secondary stroke prevention to participants. Use of a computer-based interface offers many opportunities to monitor and improve the health of patients after stroke.
Introduction
Rehabilitation therapy is provided to most patients after discharge following acute stroke admission. 1 However, patients may not derive maximal benefits from rehabilitation therapy because of factors such as limited access to appropriate providers, increasing costs that reduce the amount of care provided, difficulty traveling to appointments, and poor patient compliance. Furthermore, even when a patient engages in rehabilitation therapy, doses provided can be strikingly low and fail to approximate those corresponding to favorable preclinical stroke studies.2 -4
Evidence supports the use of telehealth in the delivery of acute stroke care, but the utility of telehealth in the postacute treatment of patients with stroke is less clear.5,6 Telerehabilitation has been defined as “the delivery of rehabilitation services via information and communication technologies” 7 (p. 31) and, therefore, can include a broad range of services. This is consistent with the holistic framework outlined by Demiris et al, 8 who suggested that home-based poststroke telerehabilitation should include support that spans an array of medical, mental health, and other services and also addresses many of the specific priorities outlined by the Canadian Stroke Network Consensus Conference on Stroke Rehabilitation and Research. 9 Our long-term goal is to improve patient outcomes after stroke by incorporating telerehabilitation methods that use these priorities. The short-term goal, addressed in this report, was to develop a telerehabilitation system that provides home-based rehabilitation therapy, focused here on the upper extremity, which builds on standard-of-care physical/occupational therapy, embeds principles of learning and plasticity, uses a game-based approach, and includes regular videoconference contact between the treatment team and the patient at home.
The current report describes this system and its performance in a pilot study. The main goals of this study were to assess (1) feasibility, measured as patient compliance with assigned sessions, and (2) arm motor gains, measured as the change in arm motor Fugl-Meyer (FM) score from baseline to 1 month posttherapy, with this home-based telerehabilitation system. Secondary goals included determining whether compliance and arm motor gains could be achieved independent of the participant’s computer literacy. In addition, as part of the holistic framework, other issues relevant to the long-term care of patients with stroke were examined using this telerehabilitation system, including assessment of risk factors via blood pressure recordings, secondary stroke complications via depression screening, and stroke knowledge via daily education.
Methods
Overview of the Study and Telerehabilitation System
After providing written, informed consent, participants received 28 days of home-based telerehabilitation, organized as two 14-day blocks of daily telerehabilitation separated by a 1- to 3-week break; 14 days was selected based on the success of the EXCITE trial of constraint-induced therapy, 10 which showed benefits when making daily demands of patients for a 14-day period. Entry criteria required age >18 years, stroke (ischemic or intracerebral hemorrhage) with onset 3 to 24 months prior, arm FM scores of 22 to 55, either grip or pinch strength >1 kg, and visual acuity of at least 20/40; motor deficits could not be unstable, defined as FM score changes of >3 points from visit 1 to visit 2, which had to be at least 1 week apart; and participants could not have deficits in language (National Institutes of Health Stroke Scale [NIHSS] Q9 must be <2) or attention (NIHSS Q11 must be <2) that interfered with study participation.
Participants made 6 in-person visits to the lab for behavioral assessments, from baseline to 1 month posttherapy. At visit 2, a behavioral contract
10
was signed that included patient goals, duties, and the dates/times of home-based therapy, after which the telerehabilitation system was introduced and then delivered by a team member to the patient’s home, where it was assembled. Participants were given an instruction manual that covered all devices and their use, and all games/exercises and their rules, and were encouraged to phone the study team for technical support if needed. In addition, patients took a pill each day 1 hour prior to therapy, in a double-blind manner, organized as 14 consecutive days of
Design of the telerehabilitation system emphasized patient convenience; ease of use; simple, large-font instructions with clear options and easy navigation; feedback; regular interaction with a clinician; and patient autonomy in choosing some therapy details. 12 The approach was built on established principles of learning and plasticity: training was challenging, repeated many times, motivating, interesting, and intensive.12 -18 Game design started with therapists outlining movements to be performed by patients, then USB-based devices were selected to transduce these movements, and finally, the device signals were used to drive game play. All telerehabilitation communications between the study team and the patient’s home were HIPAA compliant and used Polycom Converged Management Application client software on both the therapist (in the lab) and patient (in the home) computers.
Participant Treatment
Each of the 28 days of therapy consisted of 1 required hour of activities selected by the therapist and 1 optional hour of games selected by the patient. A licensed occupational or physical therapist in the lab reviewed the patient’s baseline exam, then used a Therapist Control Panel program designed for use with this telerehabilitation system to generate the initial content for the required hour of therapy, and then uploaded it to the home-based telerehabilitation system. The patient saw the day’s 1-hour itinerary and used large buttons and arrows on the mat (Figure 1A) to move through itinerary items. The telerehabilitation computer software was locked such that patients could only run the telerehabilitation program, and the system would not operate beyond the permitted number of minutes.
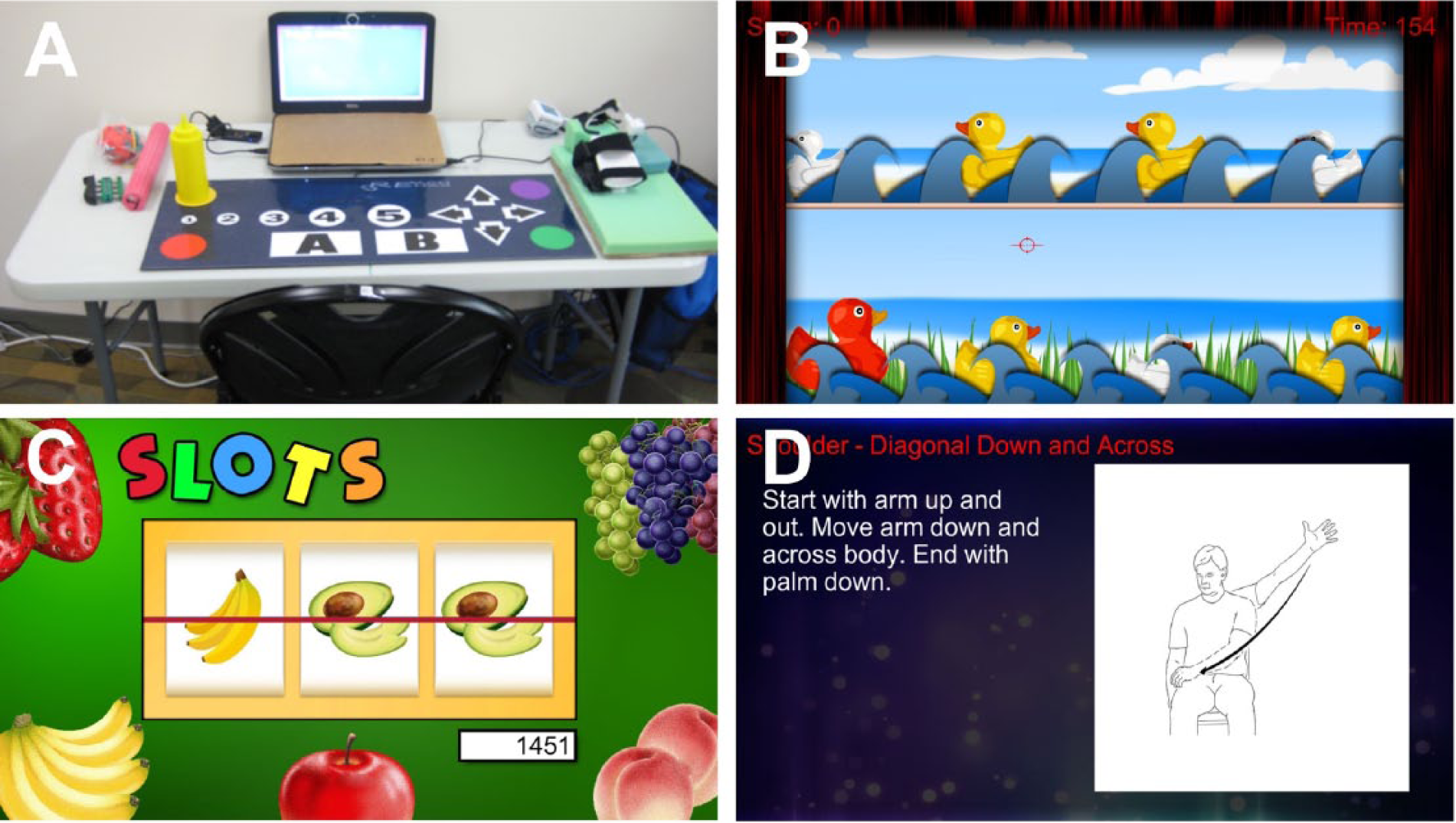
A. Hardware for the telerehabilitation system included a standard table, chair, laptop with keyboard covered, Verizon wireless modem, mat used for game play and moving through the day’s itinerary (via the buttons and arrows), standard rehabilitation equipment, and multiple USB-based input devices to drive game play. B. Carnival shooting, a game in which the patient performed supination/pronation movements to move the red cursor then squeezed a trigger using a lateral pinch movement to shoot at the yellow, but not red, ducks. C. Slot machine, a game in which the patient had to perform shoulder extension movements to stop each of the 3 reels from spinning at the correct time to match all 3 symbols. D. Shoulder abduction/adduction, 1 of the 67 available exercises.
During the required hour, patients proceeded through activities that included the following:
Games focused on arm motor therapy. A total of 18 games were available. Therapists could adjust game duration, difficulty, and input device used to drive game play. Games emphasized control of range, speed, timing, and accuracy of arm movements and spanned categories that included casino, arcade, music, and memory games.
Therapeutic arm exercises. A total of 67 upper-extremity exercises were also available.
Stroke education for 5 min/d. Patients were presented 5 of the practiced questions from the stroke knowledge quiz, in pseudo-random order; asked to select the correct answer from 4 choices; and then provided with the correct answer and a brief explanation.
Videoconferences 3 times/wk. There were 3 videoconferences per week between the patient at home and a study team member in the lab (1 per week by a licensed therapist and 2 per week by a research assistant). During their videoconference with the patient at home, the therapist reviewed the prior week’s activities with the participant, including scores, preferences, and issues in an open-ended manner. This was followed by a structured interview that included specific inquiries related to pain, adverse events, and telerehabilitation system performance. The therapist documented the interaction using standard clinic notes. Game scores and data on telerehabilitation system use were recorded and transmitted to the lab in real time. Therapists reviewed those data, along with patient responses from questionnaires and patient input during videoconferences, to modify choice, duration, and/or difficulty level of telerehabilitation games/exercises and then create and upload (silently, at any time of day) revised itineraries for future days. During videoconferences, therapists worked with patients to adjust the challenge level presented during telerehabilitation sessions as appropriate, providing feedback and encouragement to drive motivation, according to standard of care practice.
Participant Testing
Most testing was done live, in the lab. Baseline assessments (visits 1 and 2) included vital signs, magnetic resonance imaging, FM Scale, 19 Box and Blocks (B&B), NIHSS, Barthel Index, Geriatric Depression Scale (GDS) 15 question form, Mini-Mental Status Exam (MMSE), Optimization in Primary and Secondary Control Scale (adapted from Mackay et al 20 ), The Medical Outcomes Study Social Support Survey, 21 Mental Adjustment to Stroke Scale (Fighting Spirit subscore), 22 Stroke-Specific Quality of Life Scale, 23 modified functional reach forward displacement, shoulder pain using a visual analog scale from 1 to 10, gait velocity from 10-m walk test, and an adaptation of the subjective and objective Computer-Email-Web Fluency Scale tests of computer literacy. 24 The FM was scored at all 6 visits. At visit 2, patients also took a stroke knowledge quiz with 40 multiple-choice questions (4 choices per question) focused on knowledge about stroke symptoms and risk factors. Of these 40 questions, 20 were subsequently practiced during the 5 minutes of daily telerehabilitation stroke education over the next 14 days, and 20 were not practiced. At visit 3, 2 weeks later, the same 40-question quiz was administered. This entire process was repeated across visits 4 and 5 using a novel 40-question stroke knowledge quiz. Thus, from visit 2 to visit 5, patients were serially tested on a total of 40 practiced and 40 unpracticed questions.
Other testing was done remotely, via the telerehabilitation system. One set of telerehabilitation-based assessments was used to assess validity. After one therapist assessed depression in person in the lab during visit 2 using the GDS, as above, a second therapist assessed depression via the videoconference that occurred on the first day of telerehabilitation, using the patient health questionnaire (PHQ)-9 and PHQ-2 scales. Also, during visit 2, a therapist measured the patient’s systolic (SBP)/diastolic (DBP) blood pressure and pulse using a USB-based wrist blood pressure cuff (ION Health) in person. The patient then measured the same vital signs at the start of each day of telerehabilitation at home using the same cuff. A second set of telerehabilitation-based assessments was used to characterize participants at baseline. Two measures were obtained in this group, the Stroke Impact Scale (hand subsection), which measures difficulty of hand use, 25 and the Stroke Self-Efficacy Questionnaire. 26 A third set of remote assessments was used to assess patient status on a daily level. There were 4 such assessments: daily blood pressure, Target Bopping game, Wrist Targeting game, and Help The Postman game.
Hardware
The core telerehabilitation system consisted of a 24″ × 48″ table, bridge chair, Dell Latitude E5420 laptop (with 14″ display, internal webcam, and added fisheye lens), Verizon wireless USB modem, USB-based wrist blood pressure cuff, and custom-made USB-based mat that used contact-sensitive switches (Figure 1A). Other input devices, connected via USB and prescribed per therapist judgment, included a wrist splint with a sensor on its hinge to record the wrist flexion/extension position, an accelerometer with a trigger added that was used to move the screen cursor and trigger events, and a Music Glove. 27 The laptop keyboard was covered, and in fact, no keyboard was used. Instead, patients pressed buttons and arrows on the mat to move through the steps of telerehabilitation assignment. Standard nonelectronic exercise equipment, such as a weighted dowel and digit exerciser, was also provided.
Data Analysis
The number of repetitions performed by participants was assessed by either exact digital recordings or review of scores; this was done for a convenience sample of 12 different sessions (2 separate treatment days, for each of 6 different patients).
Parametric statistical methods were used for measures for which the normality assumption was valid, using raw or transformed values; otherwise, nonparametric methods were used. All analyses were 2 tailed with α = .05 and were performed using JMP-8 software. The primary outcome measure was the change in FM score from baseline (mean of visits 1 and 2) to 1 month posttherapy (visit 6). For the secondary analyses, Bonferroni correction for multiple comparisons was performed as follows: there were 3 secondary motor outcomes (B&B, FM proximal subscore, and FM distal subscore), and so P <.0167 was used to define significance. Each test of computer literacy was compared with 4 measures (age, usage, change in FM score, and change in education scores), and so P <.0125 defined significance. There were 2 tests of validation of telehealth methods for depression screening (PHQ-2 and PHQ-9), and so here, P <.025 was used. There were 3 tests of validation of telehealth vital signs measurement (pulse, DBP, and SBP), and so P <.0167 defined significance.
Results
Participants
A total of 12 patients were enrolled, with no participant dropout. Enrollees were 54 ± 17 years of age (mean ± SD) and had moderate-severe motor deficits at baseline, with FM score = 39 ± 12, range = 23 to 55 (Table 1). All but one lived with a caregiver relative. Verizon wireless reception, used to connect the telerehabilitation system to the internet, was present in all patients’ homes. Table S1 (supplement) considers problems, solutions, and lessons learned.
Baseline Participant Characteristics. a
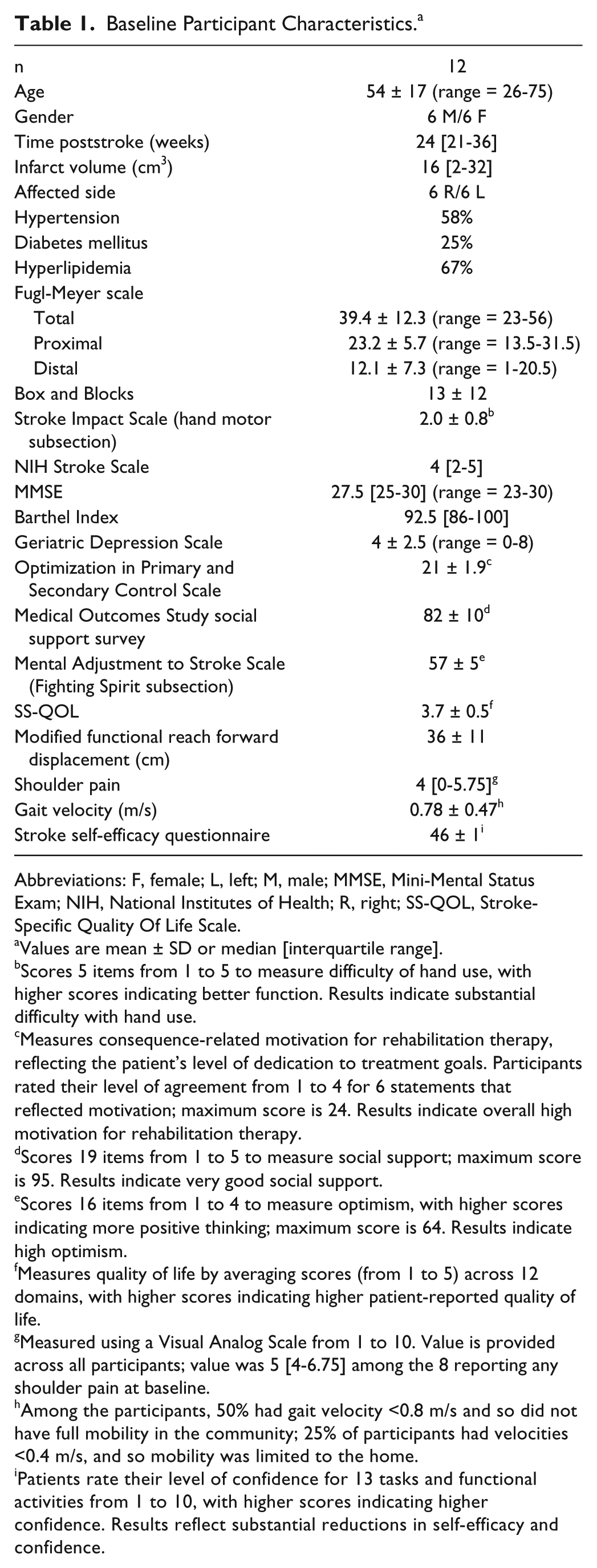
Abbreviations: F, female; L, left; M, male; MMSE, Mini-Mental Status Exam; NIH, National Institutes of Health; R, right; SS-QOL, Stroke-Specific Quality Of Life Scale.
Values are mean ± SD or median [interquartile range].
Scores 5 items from 1 to 5 to measure difficulty of hand use, with higher scores indicating better function. Results indicate substantial difficulty with hand use.
Measures consequence-related motivation for rehabilitation therapy, reflecting the patient’s level of dedication to treatment goals. Participants rated their level of agreement from 1 to 4 for 6 statements that reflected motivation; maximum score is 24. Results indicate overall high motivation for rehabilitation therapy.
Scores 19 items from 1 to 5 to measure social support; maximum score is 95. Results indicate very good social support.
Scores 16 items from 1 to 4 to measure optimism, with higher scores indicating more positive thinking; maximum score is 64. Results indicate high optimism.
Measures quality of life by averaging scores (from 1 to 5) across 12 domains, with higher scores indicating higher patient-reported quality of life.
Measured using a Visual Analog Scale from 1 to 10. Value is provided across all participants; value was 5 [4-6.75] among the 8 reporting any shoulder pain at baseline.
Among the participants, 50% had gait velocity <0.8 m/s and so did not have full mobility in the community; 25% of participants had velocities <0.4 m/s, and so mobility was limited to the home.
Patients rate their level of confidence for 13 tasks and functional activities from 1 to 10, with higher scores indicating higher confidence. Results reflect substantial reductions in self-efficacy and confidence.
Patient Experience
Compliance was exceptionally good, with participants engaging in therapy for at least 30 of the required 60 minutes on 329 of 336 (97.9%) assigned days. One patient, with the lowest motor status (FM score = 23) did not complete at least 30 minutes for 4 sessions because of fatigue; another patient did not complete at least 30 minutes because of hardware malfunction; and 1 patient missed 2 complete sessions because of conflict with other medical appointments. On 94 (28.6%) of the 336 days, the treatment team was contacted by phone for assistance, a rate that decreased over time for each patient across their 28 days of therapy (reflecting patient familiarity with the system; Supplement Figure S1A) and decreased over the 7 months during which this study was conducted (reflecting improved performance by the study team; Supplement Figure S1B). Nonelectronic devices were used only during a minority of the exercises, accounting for only a very small portion of treatment content, approximately 2 to 4 min/d on average.
Patients completed a questionnaire (Supplement, Table S2) regarding their telerehabilitation experience at the end of all study procedures, 1 month after end of treatment, rating the experience very favorably. When asked, “What did you think of the treatment overall?” using a 5-level Likert scale (5 being most favorable), the mean score was 4.4. When asked, “Would you recommend this type of treatment to someone with a similar condition after stroke?” the mean score was 4.8. In terms of system components, the lowest rating pertained to some of the hardware that was difficult to use, and the highest rating was for the appointment reminder system. Other patient ratings appear in Supplement Table S4.
In terms of specific patient preferences, memory games (eg, Simon) were not preferred. Patients did not express concerns with the exercise assignments. The most popular specific free-play choices were casino (slot machine, pachinko) and arcade (carnival shooting, duck hunt) games (Figures 1B and 1C), but preferences varied widely. Overall, the percentage of free-play time spent on music games was 7.0% ± 6.7%; on carnival games, 15.2% ± 7.6%; on arcade games, 24.4% ± 19.8%; on puzzle games, 24.6% ± 23.4%; and on casino games, 28.8% ± 30.5%. The percentage of free-play time spent in each free-play category was not related to participant’s self-reported interests in these respective categories according to a survey performed at baseline.
Patients underwent daily motor assessments. Each day at home, patients played the Target Bopping game (Supplement, Table S3.14), whereby patients grasped a cylinder to press on different input mat targets according to on-screen instructions. Average scores increased significantly over time (r = 0.65, P = .0002; Pearson’s correlation coefficient, Figure 2), by 122% across the 28 days of play of this 3-minute game, from 46 targets successfully bopped during play on day 1 at home to 102 targets on day 28 at home. Day-to-day variability was common. Scores on day 1 correlated significantly with baseline FM scores (r = 0.78, P < .003; Pearson’s correlation coefficient); however, the slope of game scores over the 28 days of home play was not related to the change in FM score over the same time interval (P > .5). For 2 other games played daily at home, Wrist Targeting and Help the Postman, reliable data could not be obtained over time because these 2 relied on the wrist splint, which proved difficult to don and calibrate consistently.
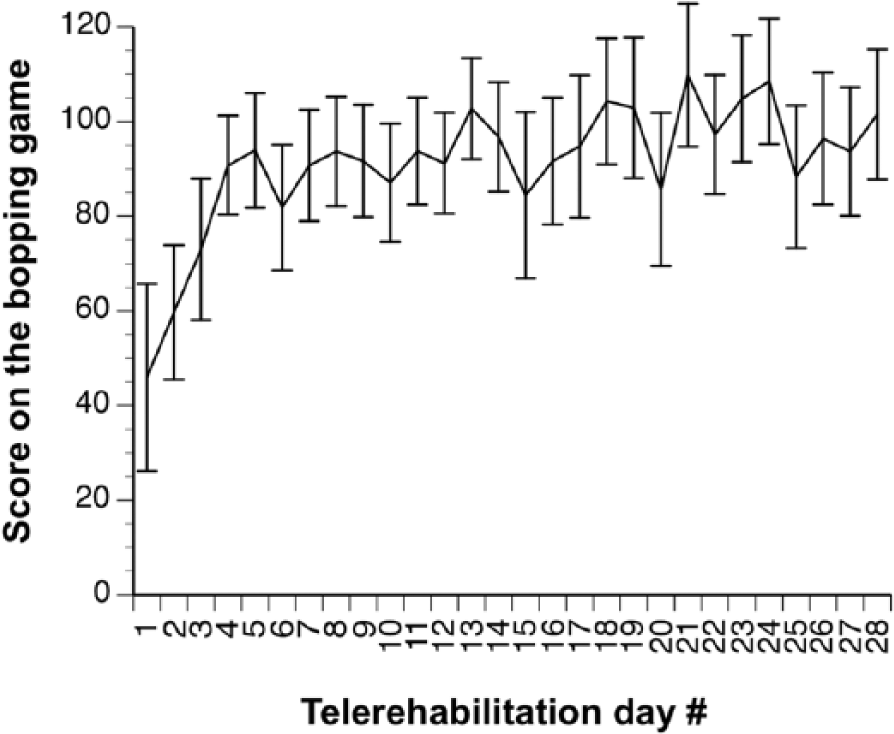
Mean ± standard error of the mean scores on the bopping game, during which participants had to use a cylinder held in the stroke-affected hand to bop the tabletop mat target that was indicated on the computer screen. Scores increased significantly across the 28 days of therapy (r = 0.65; P = .0002); note that this increase in scores over time remained significant if values from the first 3 days were removed.
Active time (time during which games and exercises were performed) averaged 60 ± 10 min/d, including an average of 22 ± 24 min/d of free play. Total time (active time plus education questions, measuring blood pressure, reading game instructions, donning devices, and taking breaks between tasks) averaged 182 ± 61 min/d. The average number of arm repetitions per day was 879 ± 355, and thus, the average number of repetitions per participant across the entire 28 days was 24,607 ± 9934.
Therapist Experience
Therapists were able to create an initial treatment plan, send it to the telerehabilitation system in the patient’s home, review patient scores and performance remotely, and then upload revised therapy settings to the telerehabilitation system in the patient’s home without difficulty, at any time of day. Videoconferences were performed as planned, without incident. Of the 48 planned weekly videoconferences with a therapist across all 12 patients, 46 were attended as planned. During these videoconferences, the therapist helped the patient adjust to assigned games, exercises, and equipment, or modified assignments. Common issues that arose were the need to reduce elbow extension, reduce pronation/supination, increase arm elevation, and refer to the instruction manual provided by study personnel. Also, patients were asked if any activities were associated with shoulder pain. Responses varied widely across patients and across weeks, with no trend for worsening over time, and included pain from the daily target bopping target game, the Simon game, various exercises, and reaching for the furthest targets on the input mat.
Arm Motor Gains
FM scores were stable at baseline, changing an average of 0.1 points (P > .9) from visit 1 to visit 2, which were 15 ± 3 days apart. Regarding the primary outcome measure, arm FM score increased from baseline to 1 month posttherapy by 4.8 ± 3.8 points (P = .0015, paired t-test, Figure 3A), with the gain in 6 participants exceeding the minimal clinically important difference (MCID) of 4.25 points. 28 Gains in proximal and distal FM score subsections are described in the supplement (Figure S2). None of the measures in Table 1 was significantly correlated with this FM score increase, whether assessed with or without correction for multiple comparisons. Gains in FM were not uniformly distributed across the 33 components comprising the FM score. For example, there were no questions where at least 10 of 12 enrollees showed a change of at least 1 point; there were 6 questions where at least 4 people showed an improvement of at least 1 point (shoulder external rotation, hand to lumbar spine, wrist flex/extend with elbow extended, wrist circumduction, palmar prehension, and movement with normal speed); and there were 4 questions where anyone showed a change of 2 points (triceps reflex, hand to lumbar spine, wrist circumduction, and palmar prehension).
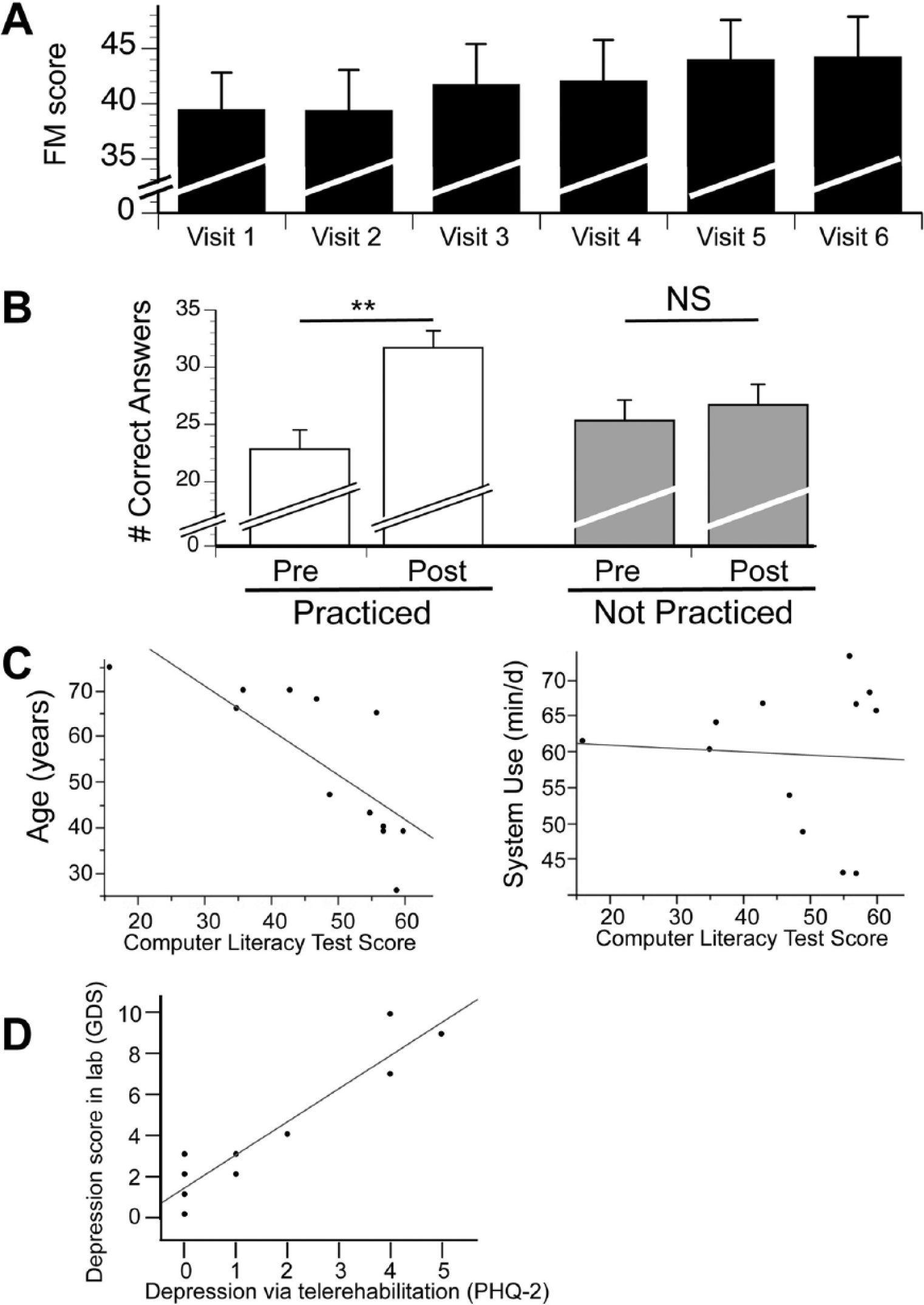
A. Arm motor deficits (mean ± SEM) were moderate-severe at baseline and increased 1 month posttherapy by 4.8 points (P = .0015), with gains in 6/12 participants exceeding the minimal clinically important difference. B. Stroke education using the home-based telerehabilitation system improved scores on tests of stroke prevention knowledge. White bars: For the 40 questions that were practiced as part of 28 days of daily stroke education, correct answers increased 39%, from 22.8 to 31.7 (P = .0007). Gray bars: As a control, 40 questions were not practiced but were also serially tested, and these scores did not change significantly (P = .17). C. Computer literacy was inversely related to age (r = −0.92, P < .0001; left panel) but not system use (average amount of time participants spent each day using the telerehabilitation system, P > .5, right panel). D. Depression score in the lab at visit 1 using the Geriatric Depression Scale (GDS) correlated significantly (r = 0.88; P = .0001) with the depression score obtained an average of 16 days later in the home on the telerehabilitation system using the Patient Health Questionnaire (PHQ)-2.
The B&B score, a measure of arm function assessed from baseline to end of therapy, also increased significantly, from 13 to 16 blocks transferred over 60 s (P = .01, paired t-test). Assuming an MCID of 6 blocks, 29 gains in 4 participants achieved the MCID for this functional measure.
Stroke Education
Patients showed significant gains in stroke prevention knowledge that were specific to facts reinforced in daily quizzes (Figure 3B). For the 40 quiz questions that were practiced on the telerehabilitation system, the number of correct answers increased by 39%, from 22.8 to 31.7 (P = .0007, paired t-test). For the 40 quiz questions that were not practiced, scores changed from 25.3 to 26.7 out of 40, a nonsignificant 5% change (P = .17, paired t-test).
Findings Not Dependent on Computer Skills
Computer literacy scores declined with age, as expected (ρ = −0.92 and −0.90, P < .0001, Spearman’s rank correlation coefficient, for the subjective and objective portions of the Computer-Email-Web Fluency Scale respectively, Figure 3C left panel). However, neither computer literacy score was significantly related to amount of system use (Figure 3C right panel), arm motor gains (change in FM score), or stroke education gains (P > .05, Spearman’s rank correlation coefficient).
Validity of Depression Screening Using Telehealth Methods After Stroke
The PHQ-2 and PHQ-9 were successfully scored in all participants during the first telerehabilitation videoconference, as planned. GDS scores obtained in person at visit 1 correlated significantly with these telerehabilitation-derived PHQ-2 scores (ρ = 0.88, P = .0001, Spearman’s rank correlation coefficient, Figure 3D) and showed a trend with respect to PHQ-9 scores (ρ = 0.57, P = .05, Spearman’s rank correlation coefficient). At visit 1, 3 patients had GDS scores of 5 to 10 (suggestive of depression), and all 3 had a PHQ-2 score >3 (also suggestive of depression) during the first telerehabilitation session 16 ± 3 days later; each was referred for further evaluation.
Validity of BP Measurement Using the Telerehabilitation System
The participants recorded their BP and pulse at home using the telerehabilitation system, and the results were then automatically transmitted to the lab, on 329 of 336 (97.9%) assigned days. SBP (130 ± 20 vs 130 ± 20 mm Hg), DBP (83 ± 16 vs 84 ± 16 mm Hg), and pulse (78 ± 11 vs 77 ± 11) recorded by a therapist in the lab at visit 2 closely matched values obtained by the patient using the same cuff at home during the first telerehabilitation session, which was 1 to 2 days later (all r = 0.99, P < .0001, Pearson’s correlation coefficient).
Discussion
We designed a home-based telerehabilitation program that provided arm motor therapy while addressing other issues important to the outcome of patients with stroke, such as secondary prevention and screening for complications. We found that (1) patients were highly compliant (97.9% of assigned days) and rated the system favorably; (2) therapists were readily able to review patient performance and revise therapy; (3) videoconferences supported regular communication between the patient and treatment team; (4) arm motor status improved significantly overall and exceeded the MCID in half of the participants; (5) daily education increased stroke prevention knowledge by 39%; (6) screening for depression was accurate; (7) BP measurement was very accurate; and (8) all these findings were unrelated to participants’ computer skills. These findings support the feasibility and potential utility of this home-based program for improving outcomes after stroke.
The best treatment program is of little help to patients if they do not adhere to it, and so the telerehabilitation system was designed to maximize compliance. One key feature in this regard was the use of games to drive treatment, an approach known to increase desirability and accessibility and to promote patient participation.30 -33 In addition, patients were asked to sign a behavioral contract, 10 which increases adherence, engagement, and accountability. 34 Our contract listed daily times of therapy, increasing organization, facilitating videoconference planning, and enabling system alerts to begin each day’s session on time. Another feature promoting compliance was that patients could pause the system as needed between assigned tasks. Also, in contrast with some commercial systems aiming to drive rehabilitation therapy in the home, our system emphasized variety, with the different modules (therapy, assessment, education, prevention, videoconferencing), numerous games and exercises, and a range of different hardware input devices incorporated into individual treatment plans. In addition, patients could phone the lab if a technical question arose, a feature mainly used during participant’s initial days of telerehabilitation (Supplement Figure S1A). Also, system design focused on ease of use, including simple, large-font instructions. A key finding in this regard was that computer literacy, although inversely related to age, was not related to treatment gains (Figure 3C), indicating that effective system use did not require computer skills. Patients could only use the telerehabilitation system for the itinerary assigned by the therapist, and in fact, the keyboard was inaccessible, making this system more like an appliance than a computer. In general, patient compliance with home-based physical therapy ranges from 23% to 64%, 35 and after stroke, 65.3% of patients report adhering to at least part of a home exercise program. 36 The above-described features likely underlie the superior compliance (97.9%) observed with the current telerehabilitation program.
The primary outcome measure was arm motor gains, assessed by the change in FM score from baseline to 1 month posttherapy. Findings were significant (Figure 3A), with 6 of 12 participants achieving the MCID. The FM is a measure of body structure/function limitation, so it is worth noting that results using the B&B, a measure of activities limitation, were also significant. The current findings are based on a small cohort in a noncontrolled study and so must be viewed with caution; for example, the limited sample size might have increased the risk for ascertainment bias. However, each of the 12 patients was assessed over 28 separate days, for a total of 336 telerehabilitation study days. In addition, a strength of the system that supports the validity of the current findings is the implementation of principles of neuroplasticity in game design, including the use of stimuli that are challenging, repeated many times, intense, fun, and adjustable.12 -18 As part of the research design, the current study limited therapy to 2 hours of therapy per day for 28 days, but greater gains may be possible with a longer duration of intensive therapy,37,38 which may be pursued in future studies. An important finding is that participants performed an average of 24,607 repetitions over 28 days, based on 879 arm repetitions each day, a value similar to the 466 movements per hour recorded in a prior study of one of the current input devices. 27
Stroke is a complex chronic disease associated with many risk factors and complications. Using a computer-based interface in the home offers opportunities to address several aspects of patient health in parallel. This type of holistic approach has been advocated8,9 and was incorporated into the design of the current program in 3 major ways. First, major depression is a common complication after stroke, 1 and it remains significantly underdiagnosed and poorly treated. 39 The current study validated a home-based telerehabilitation system for measuring depressive symptoms because PHQ-2 (P = .0001, Figure 3D) scores obtained using the telerehabilitation system in the home were significantly related to GDS scores obtained in person, independently, 16 days prior. Second, many patients with stroke have limited knowledge about the causes and effects of this disease; for example, in studies of patients admitted for stroke, 39% could not name 1 sign or symptom of stroke, 40 whereas 40% could not identify a single stroke risk factor. 41 Stroke education delivered by the telerehabilitation system increased participants’ knowledge of stroke symptoms and risk factors, with correct scores increasing from 23 out of 40 questions at baseline (58% correct) to 32 out of 40 questions correct at the end of therapy (80% correct), a relative increase of 39% (P = .0007). Third, many stroke survivors do not achieve good risk factor control. For example, among 1252 US survivors of stroke or myocardial infarction, long-term BP control was present in only 53%. 42 Using the current telerehabilitation system, patients recorded their blood pressure at home on 97.9% of the 336 assigned days, and these values closely matched those obtained independently by a therapist in the lab (r = 0.99; P < .0001). Such findings support the idea that a home-based telehealth system could be used to improve blood pressure control in patients with chronic stroke. Together, these findings suggest that, in addition to driving motor rehabilitation, a home-based telerehabilitation system can assess patients for poststroke complications, educate patients about stroke, and assess risk factor control. Future studies can build on these results to examine how such measures may be used to improve outcomes.
There are a number of strengths to the current study. A holistic framework was implemented, within the convenience of the home, with several different features, and with no dependence on computer skills. Effective therapist-facing software is as important as the patient-facing program 43 and performed well in this pilot study. Video-based techniques may be a key component to effective telerehabilitation 44 and were a central feature of the system under study. Although the sample size in this pilot study was modest, good compliance with therapy was found in patients with gait velocity <0.4 m/s (ie, mobility limited to the home) or MMSE score as low as 23 (Table 1). There are also important weaknesses to the current study. The sample size was limited. There was no control group, making it difficult to attribute specific outcomes to particular aspects of treatment content. Patients needed substantial support, at least during the initial days at home (Figure S1A). It is hoped that the lessons learned during study performance (Supplement, Table S1) will inform approaches that reduce the need for assistance in future telerehabilitation studies. At baseline (Table 1), patients had high consequence-related motivation for rehabilitation therapy, very good social support, and overall high optimism. It will be important to evaluate compliance with home-based telerehabilitation therapy among participants with less motivation, social support, and optimism to better understand the extent to which current results generalize across the entire spectrum of stroke survivors. Much of the telerehabilitation was based on tabletop activities, although there were some 3-dimensional components to the games and exercises, and future telerehabilitation-based therapies may wish to expand the amount of time devoted to 3-dimensional functional tasks. A separate control group was not enrolled; however, patients were enrolled after the time when arm motor recovery is generally considered to be at a plateau, 45 and confirmation of stable deficits at baseline increased confidence that observed gains in motor status were the direct result of the telerehabilitation intervention. Finally, this was a pilot study with a limited sample size, unblinded assessors, and no control group; however, results are promising for extension of the current approach to a larger clinical trial.
Conclusions
The burden of poststroke disability remains large. Telehealth methods may be useful to improve outcomes, particularly given decreasing lengths of stay for inpatient stroke care,46,47 and moderate evidence exists for equivalence to conventional rehabilitation. 44 The current study supports the feasibility and utility of a home-based system to effectively deliver telerehabilitation, improve patient education, screen for complications of stroke, and provide patients at home with a means for interaction with medical personnel.
Footnotes
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website at along with the online version of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was provided by NIH (K24-HD074722 and UL1-TR000153) and the UC Irvine Dean’s Triumvirate Award. Dr Cramer has served as a consultant for Dart Neuroscience, RAND Corporation, Toyama, MicroTransponder, and Roche, and is cofounder of personalRN.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.