
Abstract
Stroke recovery research involves distinct biological and clinical targets compared to the study of acute stroke. Guidelines are proposed for the pre-clinical modeling of stroke recovery and for the alignment of pre-clinical studies to clinical trials in stroke recovery.
Keywords
Introduction
Moving treatments from the preclinical to the clinical realms is notoriously difficult. For all diseases, only 10% of agents that enter phase 1 trials result in a clinically used drug.1,2 The success rate in stroke and traumatic brain injury is also low and well-documented.3–5 The translational failure in stroke has been attributed to the narrow therapeutic window and to mistakes such as very broad inclusion criteria, and imprecise, global outcome measures.3–5 On the preclinical side, depth and rigor of study design, analysis and interpretation have received special focus.
Stroke recovery involves distinct biological principles and a very different time window compared to stroke neuroprotection.6–8 Unlike acute stroke, post-stroke behavioral activity shapes recovery and can be manipulated to promote recovery, or to negatively interact with recovery.6,9 In addition, stroke recovery involves a unique biology of altered synaptic signaling, enhanced synaptic plasticity and changes in neuronal circuits that provide novel drug and cellular targets but also raise special considerations in clinical translation. The special considerations include: the animal stroke models, the tissue and behavioral outcome measures, imaging biomarkers and conceptual management of the full translational pipeline.
Recent conceptual and technological developments in neuroscience are bringing promising physical, pharmacological and cellular therapies to the field of neurorehabilitation and brain repair. This paper outlines a series of guidelines and recommendations specifically tailored to enhance the quality and rigor of preclinical stroke recovery research.
The task of the translational working group of the Stroke Recovery and Rehabilitation Roundtable (SRRR) 10 was to develop a set of guidelines and recommendations appropriate for preclinical stroke recovery research. Existing preclinical stroke research recommendation papers (e.g. STAIR, STEPS) focus chiefly on acute stroke.11,12 Although cognitive impairments and depression are common after stroke, 13 the SRRR working groups concluded that these topics require a subsequent roundtable discussion so the emphasis here is on preclinical sensorimotor recovery. The ultimate goal of the translational group was to align preclinical to clinical stroke recovery studies so as to avoid past mistakes and maximize clinical translation.
Methodology
An expert panel of basic and clinical scientists was assembled. Care was taken to include individuals at early, mid and late career stages with broad geographical representation. To facilitate the process, a questionnaire was sent to each team member asking them to answer a series of questions including: 1. What are the top research priorities in the stroke recovery field; 2. What key animal models should be employed; 3. What core tissue and behavioral analyses and outcome measures should be used to assess post-stroke recovery and 4. What flaws or mistakes in this field have impeded progress towards clinical trials or development of new therapies? The responses showed a high level of consensus and were summarized, recirculated, and subsequently formed the basis for discussion at the two-day SRRR meeting held in Philadelphia in May 2016. The ensuing consensus guidelines and specific recommendations described herein were achieved after extensive discussion including input from the other three SRRR working groups (Biomarkers, Interventions, Measurements).
Getting the Most Out of Preclinical Stroke Models
Research on stroke recovery is concerned with long-term outcome. The four most common rodent models in stroke recovery research are all ischemic stroke models: photothrombotic (PT) stroke, distal middle cerebral artery occlusion, transient occlusion of the proximal middle cerebral artery, and endothelin-1 (ET-1)-induced stroke (Table 1) have been recently reviewed.14,15 A major advantage of most rodent stroke models is that they result in a stroke of similar size to about 60% of all human strokes, can target cortical subdomains, and can be reliably used in aged animals and animals with comorbidities, such as obesity and diabetes. Human stroke is itself highly heterogeneous and thus there is no “gold standard” stroke model that is most relevant to human disease.
Common Rodent Stroke Models for Recovery Studies.
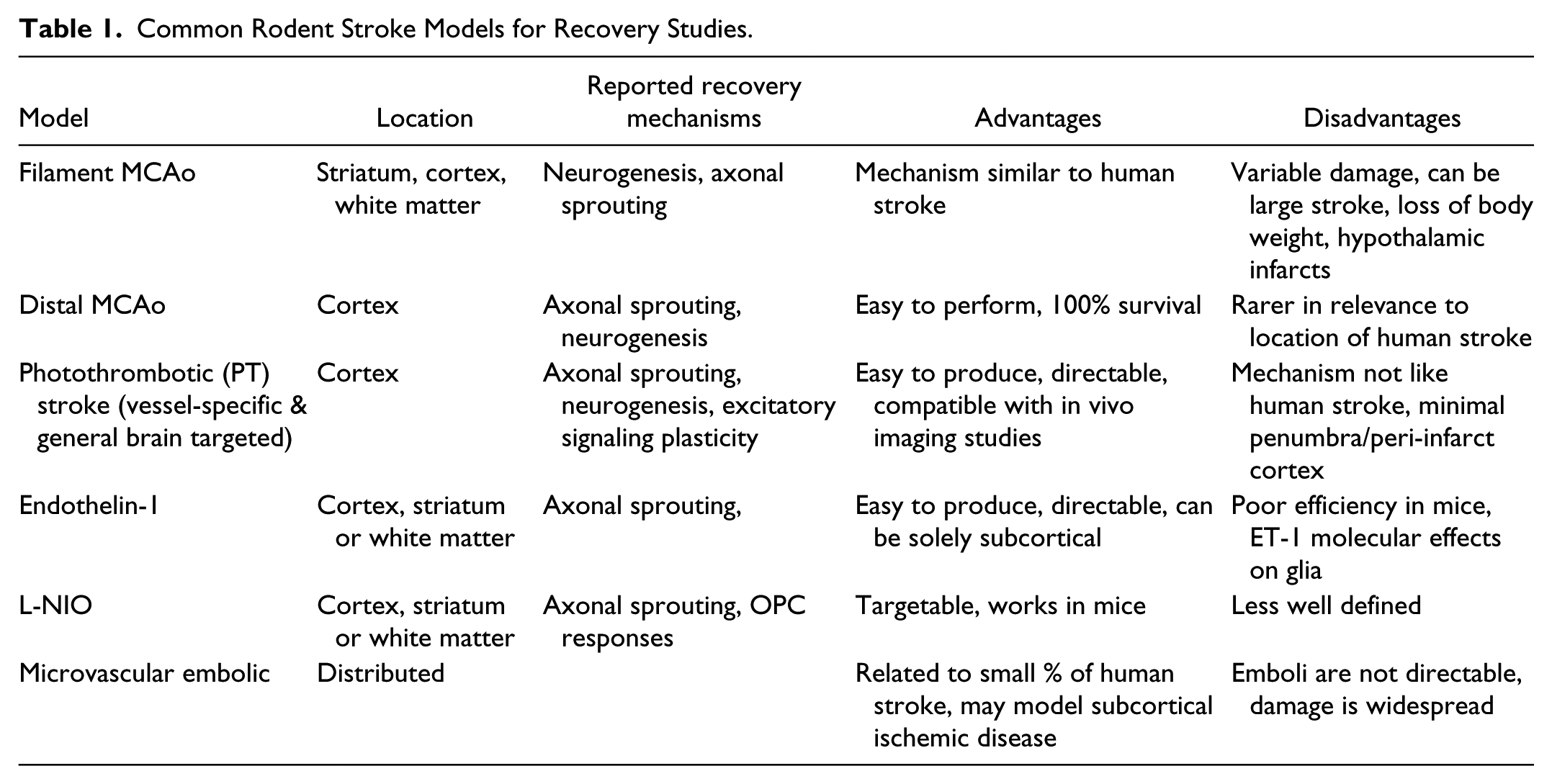
Photothrombotic stroke is reproducible, relatively non-invasive and technically simple. It is ideal for producing a stroke for in vivo optical studies in mice and for ablating a specific cortical region. Disadvantages include a confined small rim of partially damaged peri-infarct cortex, where many biological processes (e.g. angiogenesis and neurogenesis) associated with neural repair after stroke occur, hemorrhagic transformation of perilesional tissue 16 and that its ischemic mechanism (simultaneous occlusion of all vascular elements) and immediate and profound edema seen in ~50% of animals are not seen in human stroke. Also, in the absence of fiber optic implantation,17,18 it is not possible to target subcortical brain structures with photothrombosis. Distal middle cerebral artery occlusion produces a border zone of partial damage and robust angiogenesis, neurogenesis and axonal sprouting 6 mostly in the whisker/vibrissal cortex in rodents. Motor function is not greatly altered by distal middle cerebral artery stroke which is in essence a somatosensory stroke. 19 Transient filament occlusion of the middle cerebral artery produces a stroke with a pattern of damage (i.e. striatum and cortex) that is common in humans.20,21 This reperfusion model triggers tissue repair responses; however, damage is highly variable with infarcts that are often large resulting in significant morbidity and mortality. Comparably sized human strokes are not associated with recovery. 22 ET-1 is a vasoconstrictor that produces stroke after local injection into the brain parenchyma or adjacent to the middle cerebral artery.23,24 This approach, like photothrombotic stroke, is highly targetable and generates cortical strokes with excellent behavioral readouts. This approach is limited by the lack of reproducible effect of ET-1 in mice but can be enhanced by nitric oxide inhibition (L-NIO). There is some concern in activating the ET-1 signaling system in non-vascular (glial) cells. 25
Because of costs and ethical considerations, fewer studies on stroke recovery can be undertaken in non-human primates. When studying recovery of motor control, there are some distinct differences in the motor system of rodents in comparison to primates and humans. For example, while rats have corticospinal projections, 26 they do not have direct corticomotoneural connections.27,28 Primate studies can provide a valuable validating step between work in rodents and clinical trials. An example is the progression of the neuroprotective PSD-95 inhibitor 29 from rodents to monkeys and then to clinical trials.
Finally, the typical stroke patient presents with advanced age as well as cardiovascular and metabolic comorbidities. In contrast, most rodent stroke studies employ young, healthy animals of the same sex. To better mimic stroke patients, preclinical studies should use males and females, older animals, different strains, and animals with different comorbidities. These experiments would be undertaken after simpler, “proof of principle studies” in order to improve evaluation of a potential new therapy. 30
Outcome Measures
Sensorimotor Outcomes
Both mice and rats are widely used in stroke recovery studies. Since upper and lower limb impairments are common, clinically it is valuable to include tests that measure homologous impairments in rodents. Rats readily learn to reach for food pellets in either single pellet or staircase tests.31,32 These tests are quantifiable and reveal both initial and chronic upper limb impairments. They also lend themselves to kinematic analysis and other analyses of the quality of the movement. Ability to use the impaired upper limb in a reaching task does not necessarily guarantee that the limb will be used in other contexts since compensation in rodents33,34 like humans, is highly prevalent. Therefore, a test of spontaneous limb use, such as the cylinder test 35 can provide valuable information. Hindlimb impairments can be detected using tapered beam 36 and horizontal ladder 37 tasks. Ideally, a more detailed characterization of locomotor impairments could be achieved by examining quantitative parameters, using kinematics, over-ground walking and other behaviors. 38 Rotarod, neurological deficit score (NDS) test batteries and adhesive tape tests of somatosensory function do not have much sensitivity aside from identifying initial deficits after large strokes. 8 Mice are now widely used in stroke recovery studies but there needs to be greater test refinement in mice. The single pellet 17 and pasta 39 reaching tasks can reveal long-term impairment in mouse stroke models. Other sensitive outcome measures used in mice are grid and ladder walking 40 and adhesive tape tests of sensorimotor function 41 both of which detect chronic impairments in mice following photothrombotic or ET-1 stroke. Preclinical investigators should develop a test battery spanning a range of sensory-motor functions (Table 2) similar to those used in human stroke.
Behavioral Tests Used to Assess Sensorimotor Impairment After Experimental Stroke With the Time Window, Sensitivity and Validity.
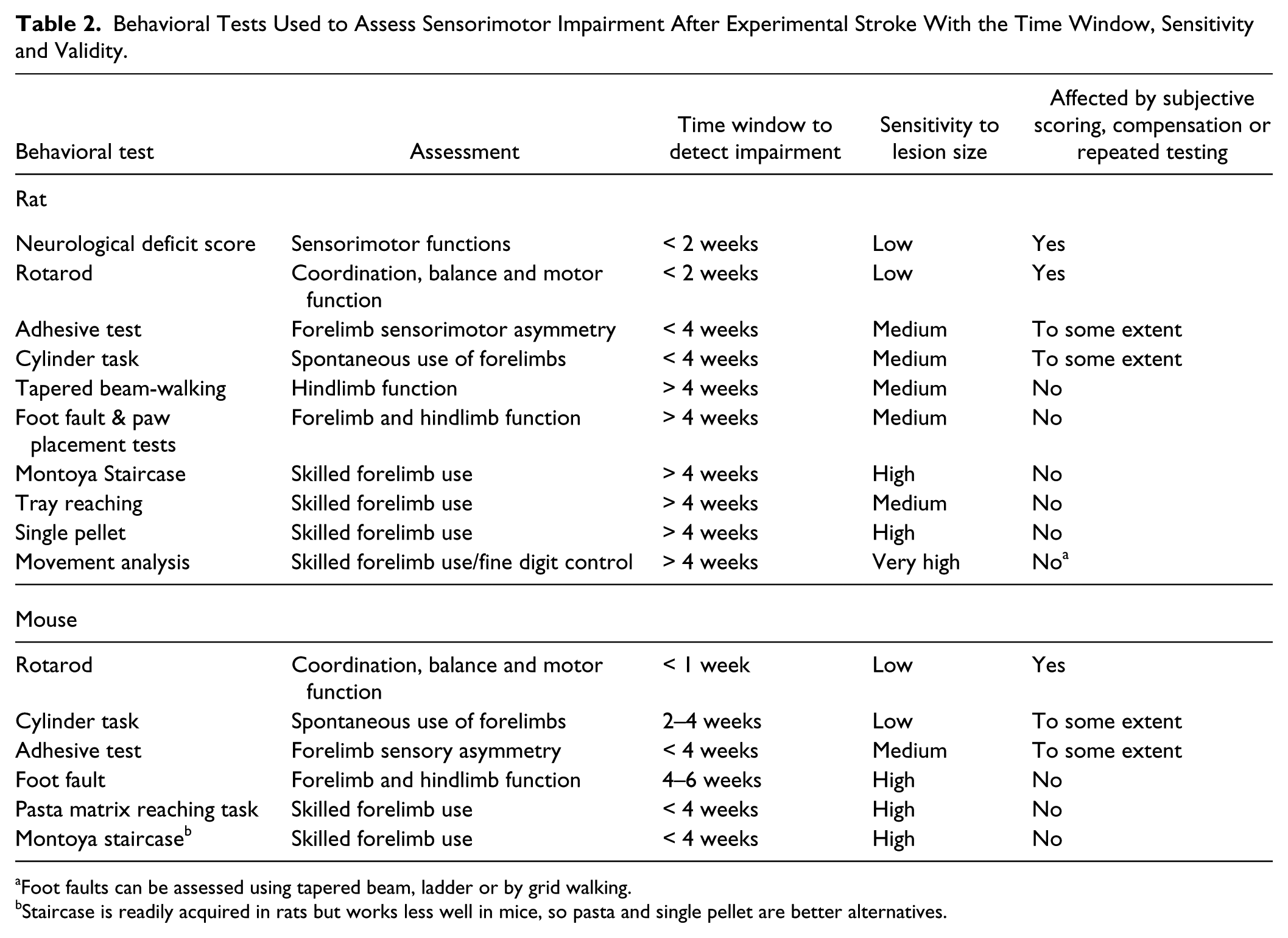
Foot faults can be assessed using tapered beam, ladder or by grid walking.
Staircase is readily acquired in rats but works less well in mice, so pasta and single pellet are better alternatives.
Another aspect of human stroke often not captured in preclinical studies is chronicity of impairment. Except in the case of small cortical strokes, nearly 50% of individuals report persistent loss of upper limb function several years after stroke.42,43 While the time course of recovery in rodent models is more rapid than in humans, many preclinical studies show that animals recover completely, returning to pre-stroke performance levels within days or a week or two. Animal stroke recovery studies need to demonstrate comparable behavioral recovery profiles to those of human stroke. This would mean an initial impairment that shows some degree of spontaneous recovery over several weeks but then plateaus significantly below pre-stroke performance levels as in human stroke.
Rodent stroke models are limited because there is no true measure of impairment equivalent to the Fugl-Meyer scale used in humans. The term “recovery” in rodent studies refers to improved performance on tasks that do not distinguish spontaneous – or treatment-induced recovery from compensation. 44 In humans, compensatory movement patterns or trajectories can be corrected and made more efficient by therapist or robot-provided feedback, whereas in animals this is difficult. High speed, high-resolution video recordings enable documentation but also unbiased quantification using computer algorithms. This permits automated kinematic analysis of rodent limb movements comparing pre-and post-stroke movement features in the same animals thereby increasing sensitivity of animal behavioral readouts. Automated rodent post-stroke training and assessment devices, 45 especially to reinforce more normal rather than compensatory movement strategies are in development.
Tissue Outcomes
Stroke recovery occurs as a result of changes in synaptic signaling in existing neuronal networks, formation of new neuronal networks through axonal sprouting and dendritic branch and spine growth, alterations in glial cells through glial progenitor responses, angiogenesis and neurogenesis.6,8,46 For rigorous translational studies in this field, these tissue repair processes should be quantified and directly related to behavioral recovery. The biological events in stroke recovery frequently involve small modification in neurons, glia and vasculature within a much larger network of cells that do not respond to stroke or mediate recovery. Tissue outcome studies in stroke recovery need to directly measure or visualize the proposed biological process, be manipulable to study gain and loss of function so that the relationship of a tissue repair process to recovery can be causally measured, and reproduced in a different lab or context. Common examples of failures for tissue outcome measures are in the use of immunohistochemical staining for a particular protein epitope as an indicator of biological response. Increased GAP-43 staining has been used as evidence for “axonal sprouting.” 47 However, GAP-43 is also present in astrocytes and oligodendrocyte precursors, in addition to neurons, is induced by stroke in these cells and marks plasticity in their adaptation to stroke or other insults.48–50 Further, immunohistochemistry is a non-linear process in which general reaction product does not necessarily correlate with a discrete increase in the underlying biological process, such as axonal growth cone number. The same critique applies to stains of axonal neurofilaments, which do not necessarily indicate increases in axonal connections.
Direct, quantifiable, manipulable, and reproducible techniques for studying tissue responses have been applied for years in learning and memory and in regeneration studies. Here direct measurements of dendritic spine number and response rate, axonal connections, sprouting and elongation as demonstrated by axonal tracing techniques or genetic markers have provided insights into the underlying biology of CNS structural plasticity.51,52 In stroke, direct measurements of axonal connections and direct quantification of vascular architecture and glial populations using appropriate controls have been performed. 52 Stroke recovery processes are dynamic, therefore combining the use of the above tissue outcome measures with new imaging techniques (below) to track these tissue responses over time may provide a means for identifying mechanisms of action in potential new therapies.
Brain Imaging and Biomarkers
Animal imaging should have parallels to human assessment
In preclinical stroke recovery, treatment regimes are typically not informed by prognostic use of imaging. 8 Clinical imaging has been used in a post hoc manner to provide mechanistic information to explain lasting deficits and in some cases therapeutic interventions.21,53,54 Connectivity studies offer the potential of future prognostic value. 55 An ideal scenario would be for diagnostic imaging to guide the practice of stroke recovery, perhaps informed by insights from animal connectivity work.52,56–60
A challenge is matching clinical imaging indices with those that are appropriate for animal experimentation. The choice of imaging modalities for research also depends on the questions to be addressed. The technology for identification of perfused versus infarcted tissue is very different from that for identification of tract integrity, which could be a predictor for recovery. Step one should be the identification of the relevant timescale and informative diagnostic indices in rodents that model those commonly used in humans.
Can Imaging Stratify Animals for Recovery?
Ideally, imaging would be used to identify animals that will benefit from recovery-inducing treatments. Imaging offers a non-invasive means for quantifying the functional and structural integrity of residual brain areas and pathways using techniques such as diffusion tensor imaging (DTI), resting state functional MRI (rsFMRI) and task-based functional MRI. For example, in human studies, combining clinical information with measures derived from multimodal imaging or electrophysiology can inform predictions of spontaneous recovery or response to treatment.61,62 There are numerous challenges in acquiring comparable DTI neuroimaging data in humans and rodents due to the smaller relative volume of white matter and smaller fiber tracts in the rodent brain. Despite these challenges, there has been some success in applying neuroimaging measures in preclinical models. For example, assessing structural and functional connectivity, via combining DTI and either rsFMRI, 63 or intracortical stimulation evoked FMRI, 64 provides insights into preserved response and reorganization of sensorimotor networks in relation to functional recovery after experimental stroke.
One challenge for the future is to combine neuroimaging measures that can be derived in humans, with more detailed assessments that would not be possible to achieve outside the laboratory. For example, optical imaging of neuronal activity allows for more precise functional connectivity measures than can be achieved with MRI-based estimates, but fails the principle of trying to align rodent and human imaging modalities. Future cross-modal studies using intrinsic or recombinant activity sensors could potentially bridge this resolution gap. Another future challenge is to exploit neuroimaging approaches to understand variability in recovery and treatment response. This is the primary goal for use of neuroimaging in humans but preclinical models have yet to deliver in this domain. Nevertheless, embracing structural and functional connectivity assessments in animals, with a goal to provide parallels between human and animal indices, help to pave the way for progress.
Stroke induces highly dynamic tissue remodeling processes with regionally specific and time-dependent effects. 65 There is growing evidence for a window of increased plastic potential 7 but also a vulnerable early phase in which forced activity might be harmful: This phase includes a period of increased GABA-mediated tonic inhibition 66 to limit ischemic damage as well as homeostatic plasticity mechanisms to ensure a balanced amount of synaptic input 8 to neurons. Thus, it becomes critical for all restorative intentions to define when the brain is most responsive to sensorimotor input or extrinsic plasticity modulating agents. Recent studies where different growth-promoting and rehabilitative approaches have been combined suggest that stroke therapy designs and their temporal pattern of administration are complex.52,67–69 It is still unclear how to translate the preclinical critical period of heightened neuroplasticity identified in rodents 7 to the human condition (i.e. when and for how long the window is open).
But how to define the right time point? Both pre-clinical and clinical studies would greatly benefit from the development and establishment of biomarkers—imaging markers such as white matter signals indicating the presence of specific intact tracts, or small molecules which are able to cross the blood-brain barrier to be detectable in blood samples. These plasticity biomarkers would indicate the “plastic status” of the brain, help to distinguish between animals that recover and those that do not and support decisions whether the amount or intensity of an intervention is sufficient to achieve recovery. Recent studies have found that the amount of ipsilesional white-matter disruption in the corticospinal tract is a good predictor of human motor impairments. 70
Injury profiles (i.e. relative size and location) should match heterogeneity of human stroke
Mouse: PT >> >> distal MCAo>>L-NIO
Rat: ET-1 > PT >> Distal MCAo
intraluminal filament MCAo model not recommended due to large infarcts associated with morbidity and poor recovery
Use of a test battery (two or more tests) highly recommended
Behavioral impairments need to show chronicity (weeks-months) with evidence of some spontaneous recovery and a final plateau below pre-stroke levels
Use kinematic analysis of limbs (reaching, gait) wherever possible to help distinguish between recovery and compensation and to identify persistent impairments.
Direct measurement of biological recovery process instead of indirect tissue staining.
For mechanism of action studies, gain and loss of function within biological process and direct association to behavioral recovery.
For clinical translation, reproducible finding of biological recovery process in an independent lab.
Align animal and human imaging techniques so that pre-clinical data will directly inform phase II clinical trials
Study pre-clinical imaging modalities for their ability to predict the neuroplasticity that underlies recovery.
How to Develop a More Effective Translational Pipeline
Basic scientists and clinicians need to agree on the most pressing problems in the field where two-way collaboration can advance knowledge and lead to new therapies. To date clinical trials have sought to demonstrate a difference from standard care without regard to mechanistic targets of these interventions. The problem with this approach is interpreting negative outcomes. Did the intervention actually cause any change beyond what occurs with spontaneous biological recovery? There is a great need to identify mechanistic targets in BOTH animal and human studies because preclinical targets may not be feasible in stroke patients. Once identified, these targets should be analyzed with respect to changes occurring during both spontaneous (more easily studied in animal models) and intervention-induced recovery.
Promising interventions need to go through a rigorous evaluation process before entering clinical trials. Replication(s) in the home lab to ensure robust effects are a must. Once confirmed, other translational labs would try to reproduce the original findings by following the same or very similar experimental protocols. Ultimately, this would involve replicating results across different stroke models, different species, both sexes, age and disease. Some successes of this type in preclinical studies have identified BDNF,40,71 NOGO A and its receptor NgR138,52 and extrasynaptic GABA receptors in post-stroke recovery.66,72 It is also imperative that preclinical, like clinical trials, use some agreed upon standardized outcome measures. 73
The typical drug discovery pipeline is a serial process that can take many years. To facilitate this process, labs need to divide the labor so that those best equipped to identify underlying mechanisms (e.g. sprouting, map reorganization) could conduct such experiments, while other labs with expertise in different stroke models or rehabilitation training could do studies in parallel. Much attention has focused on flaws of animal studies that do not always utilize or report randomization, blinding, power analysis, exclusion criteria and key methodological details. A preclinical equivalent of “best practice or “standard of care” also needs to be developed. Most experimental stroke studies employ no treatment, a worse case type of control group that predisposes researchers to obtain positive results. While a non-treated control is adequate for initial in-house testing of a novel therapeutic, the next step should be to use some form of clinically inspired best practice, such as training or enrichment. This approach should reduce the likelihood of identifying statistically significant effects that are of no real biological or therapeutic importance.
Collaboration is essential with regard to replication of key findings but other benefits can be derived from this approach. Unique tissue samples (e.g. from older or diabetic animals) from one lab could be used by others to address additional novel questions. Similarly, “omic” databases, imaging data, and complex behavioral data could be shared to identify new therapeutic targets, or blood biomarkers for predicting recovery. Large databases are common within clinical networks and should be reproduced at the preclinical level. Included here could be an on-line repository of negative findings to save precious time and funds pursuing dead end targets or using the information to develop better experiments. The bi-directional collaborative approach, between basic and clinical scientists, outlined above offers great promise for identifying the transformative interventions so urgently needed to improve post-stroke recovery.
Footnotes
Acknowledgements
We would like to acknowledge Prof Julie Bernhardt for convening this first Stroke Recovery and Rehabilitation Roundtable (SRRR), Ms Katie Lafferty for moderating discussions at SRRR and Dr Karen Borschmann for project management.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Florey Institute of Neuroscience and Mental Health was the coordinating center, for which we acknowledge support from the Victorian Government, in particular from the Operational Infrastructure Support Grant. Financial support was provided by NHMRC CRE Stroke Rehabilitation & Brain Recovery (Australia), Heart and Stroke Foundation of Canada, and Heart and Stroke Foundation Canadian Partnership for Stroke Recovery. An unrestricted educational grant was provided by Ipsen Pharma.