
Abstract
Background. Brain-derived neurotrophic factor (BDNF) is assumed to play a role in mediating neuroplasticity after stroke. Carriers of the function-limiting Val66Met (rs6265) single nucleotide polymorphism (SNP) may have a downregulation in BDNF secretion, which may lead to a poorer prognosis after stroke compared to noncarriers in motor learning and motor function recovery. The present study investigates whether this polymorphism may also affect the recovery of poststroke aphasia (ie, language impairment). Objective. To study the influence of the BDNF Val66Met polymorphism on the recovery of poststroke aphasia. Methods. We included 53 patients with poststroke aphasia, all participating in an inpatient rehabilitation program with speech and language therapy. All patients were genotyped for the Val66Met SNP and subdivided into carriers (at least one Met allele) and noncarriers (no Met allele). Primary outcome measures included the improvement over rehabilitation time on the Amsterdam-Nijmegen Everyday Language Test (ANELT) and the Boston Naming Test (BNT). Results. The outcome measures showed a large variability in the improvement scores on both the ANELT and BNT. There was no significant difference between noncarriers and carriers in the primary outcome measures. Conclusion. This study investigated the effect of the BDNF Val66Met polymorphism on clinical recovery of poststroke aphasia. In contrast to earlier studies describing a reducing effect of this polymorphism on motor function recovery after stroke, the present study does not support a reduction in language recovery for carriers compared to noncarriers with poststroke aphasia.
Introduction
Stroke is a leading cause of adult disability. About one third of stroke patients will develop any form of aphasia, a deficit of language processing1,2 in one or more language modalities, that is, speaking, writing, auditory comprehension, and written comprehension. 3 Many patients show incomplete recovery and aphasia has a disruptive effect on social participation. Many report to feel isolated and experience distress due to communication impairments. 4 In the first weeks to months, people with aphasia may recover as a result of spontaneous recovery. 5 There is evidence that speech and language therapy (SLT) has a beneficial effect on functional communication, with therapy intensity, dose, and duration as important determinants. 3
Recovery of language after stroke is mediated by neuroplasticity processes. Brain-derived neurotrophic factor (BDNF) is a neurotrophin that plays an important role in these processes.6-8 BDNF levels would increase after stroke that would promote neuronal survival by, for example, attenuating glutamate toxicity 9 and therefore it plays an important role in spontaneous recovery after stroke. Furthermore, animal studies have shown that BDNF promotes long-term potentiation (LTP) through TrkB signaling,10-12 which is thought to be crucial for episodic memory processing in the hippocampus.13,14 Studies have shown a downregulation of LTP by activated BDNF-TrkB signaling in the hippocampal synapses of BDNF-knock-out mice,15-17 and poorer LTP in mice with a genetically modified gene coding for BDNF15,18 corresponding to reduced learning performance.19-22 Therefore, these animal studies show that BDNF is involved in LTP processes that may underlie learning.
The BDNF Val66Met polymorphism is a gene variation, where at least one Met allele is present. In humans, 30% of the general Caucasian population are carriers of a Met allele, with up to 70% in the Asian population. 23 In mice, carriers of a Met allele show a deficiency in activity-dependent release of BDNF, leading to a downregulation of LTP. In humans, this decrease in LTP in carriers was related to a reduced hippocampal volume and downregulated episodic memory storage.14,24,25 Carriers of a Met allele show a smaller hippocampal volume and more deficits in motor learning and skill acquisition.6,14,17,26-28 However, whether a reduced capacity to memorize and learn language skill also translates to recovery from aphasia after stroke has not yet been investigated
In the context of stroke recovery, some studies have shown that the Val66Met polymorphism is associated with slower or reduced (behavioral) recovery after stroke, based on general stroke outcomes or motor skill learning.29-31 Studies on general outcomes after stroke show a large variety of populations in terms of ethnicity, age, and time poststroke.31-34 So far, many studies on stroke survivors have focused on motor skill learning and motor function recovery.31,33-38 whereas, to our knowledge, literature on the role of the BDNF polymorphism in language recovery after stroke is scarce. 36 As aphasia has a great impact on the life of stroke patients, and aphasia training requires sufficient adaptive learning skills, it would be interesting to understand the role of the BDNF Val66Met polymorphism in language recovery after stroke and its potential effect on the variability in outcome among stroke patients with aphasia.
The aim of the present study is to investigate the role of the BDNF Val66Met polymorphism in recovery of aphasia after stroke. 14 We hypothesize that carriers of at least one Met allele show a reduced improvement of language recovery compared to noncarriers. This hypothesis is based on 2 assumptions. First, the BDNF Val66Met polymorphism may decrease the release of BDNF and therefore might interact with spontaneous recovery processes poststroke. Second, BDNF would promote LTP; it influences activity-dependent plasticity and would contribute to learning processes based on behavioral experience (ie, SLT). Therefore, the decreased BDNF release in the polymorphism may lead to less behavioral recovery following SLT. We studied the impact of the polymorphism in a group of stroke patients with aphasia, who received regular aphasia rehabilitation in the subacute phase after stroke, by comparing treatment outcomes between noncarriers (no Met allele) and carriers (at least one Met allele).
Methods
Participants
From July 2014 to June 2016, stroke patients were recruited from 3 stroke rehabilitation centers in the Netherlands: Rijndam Rehabilitation, Libra Rehabilitation and Audiology, and Revant Rehabilitation Center. Inclusion criteria were aphasia after stroke, enrolment in an inpatient stroke rehabilitation program including SLT, native speaker of Dutch, time post onset less than 3 months, and age 18 to 80 years at the time of stroke. Exclusion criteria were prior stroke resulting in aphasia, excessive use of alcohol or drugs, premorbid (suspected) dementia, and premorbid psychiatric disease affecting communication.
The presence of aphasia was diagnosed at admission to the rehabilitation institute, where patients are first seen by a medical specialist in Physical Medicine and Rehabilitation, who refers all patients with problems in language and communication to experienced language and speech therapists (SLTs). SLTs perform a standard set of standardized Dutch aphasia tests, to diagnose the presence of aphasia. This standard set includes at least the ScreeLing,39,40 72 items (cutoff score: 66), and an expert rating of the Aphasia Severity Rating Scale (ASRS) from the Akense Aphasia Test (AAT).41,42 Premorbid aphasia was excluded based on medical records.
During the first week of admission to the rehabilitation center, patients were asked to consider participation in the study. All patients provided written informed consent before inclusion. The study was approved by the Medical Ethics Committee of the Erasmus MC, University Medical Center Rotterdam.
Design
For this study, we used a prospective follow-up study design. Language functioning was routinely tested by SLTs at admission and at discharge from the rehabilitation clinic. We compared 2 groups of stroke patients with aphasia based on the Val66Met polymorphism: noncarriers (genotypes with 2 Val alleles) and carriers (genotypes with at least 1 Met allele).
Intervention
As part of their inpatient stroke rehabilitation program, all patients received SLT, 2 to 5 hours per week. Regular SLT for inpatients includes a detailed assessment of language functioning and verbal communicative abilities at intake, prior to formulating an individually tailored therapy program, which is designed to meet individual needs and capacities. In the first weeks to months, the focus will be on cognitive-linguistic therapy, that is, disorder-oriented therapy to optimize language processing at the affected linguistic levels (semantics, phonology, syntax). Later in the rehabilitation process, when language recovery is reaching a plateau, the focus of therapy shifts to communicative strategies.
Measures
Outcome measures were the improvement on the Amsterdam Nijmegen Everyday Language Test (ANELT) measuring communication in daily life situations 43 and on the Boston Naming Test, a picture naming task to measure word finding. 44 ANELT scores range from 10 to 50, and the BNT scores range from 0 to 60. 45 Relevant documented information of the stroke were date of onset and type of stroke (ischemic or hemorrhagic). Demographic data included age, gender, handedness (Edinburgh Handedness Inventory), presence of a partner, and educational level (ISCED classification 2011).
Genetics
We took saliva samples (Oragene Discover OGR-500, DNA Genotek Inc, Ottawa, Ontario, Canada) from each patient to determine the presence of the BDNF Val66Met single nucleotide polymorphism (SNP). There are 3 variants: homozygotes with either 2 Val66 alleles or 2 Met66 alleles, and heterozygotes with both a Val66 and a Met66 allele. Patients without a Met allele were classified as noncarriers (Val group), patients with at least one Met allele as carriers (Met group).
The BDNF Val66Met SNP (rs6265) was genotyped with TaqMan Allelic Discrimination using the Assay-On-Demand service of Life Technologies. Reactions were performed in a 384-wells format in a total volume of 2 µL containing 2 ng DNA, 1× TaqMan assay, and 1× genotyping master mix (Thermo Scientific, Thermo Fisher Scientific, Waltham, MA). Polymerase chain reaction cycling consisted of initial denaturation for 15 minutes at 95°C, and 40 cycles with denaturation of 15 seconds at 96°C and annealing and extension for 60 seconds at 60.0°C. Signals were read with the TaqMan 7900HT (Life Technologies, Thermo Fisher Scientific, Waltham, MA) and analyzed using the sequence detection system 2.4 software (Life Technologies, Thermo Fisher Scientific, Waltham, MA).
Sample Size Calculation
For the sample size calculation we used routinely collected data on outcomes of regular language training in the rehabilitation clinic. Based on these data we aimed to detect a minimal difference between noncarriers and carriers of 10-point improvement on the BNT, with a standard deviation of 12, leading to an estimated effect size of 0.833. Using an α of .05, a power of 0.80, and taking into account that 30% of the patients are carrier of at least one Met allele, we estimated that a total sample size of 54 patients was required.
Data Analysis
Differences in demographic characteristics between the 2 groups were analyzed with an independent t test for continuous variables, a Mann-Whitney U test for variables on an ordinal scale, and the χ2 test for categorical variables. We performed a Kolmogorov-Smirnov test to test whether the distribution of the delta scores of the ANELT and BNT was significantly different from a normal distribution. Results reveal that both the ANELT delta scores (D[48] = 0.149, P = .010) and the BNT delta scores (D[48] = 0.137, P = .024) differed significantly from a normal distribution, probably caused by a substantial number of patients without improvement (delta score = 0) on both tests.
Change over time within each group and differences between the 2 groups in improvement on the language tests (T0 − T1) were analyzed with generalized estimating equations (GEE), which takes into account that multiple measurements within patients are correlated. GEE is a semiparametric method that does not depend largely on the specification of the underlying distribution of the outcomes. It is also flexible in handling missing data. The outcomes on the language tests at T0 and T1 were the dependent variables in the GEE models, in which the measurement time (T0 vs T1) and group membership (carriers vs noncarriers) were entered as fixed variables. To study differences in improvement between the groups the interaction between group and time was added to the models. The effect of potential confounders was analyzed if significant differences were found between the groups at baseline. The level of significance (P) was .05 in all analyses. IBM SPSS 21 Statistics software was used for all statistical tests.
Results
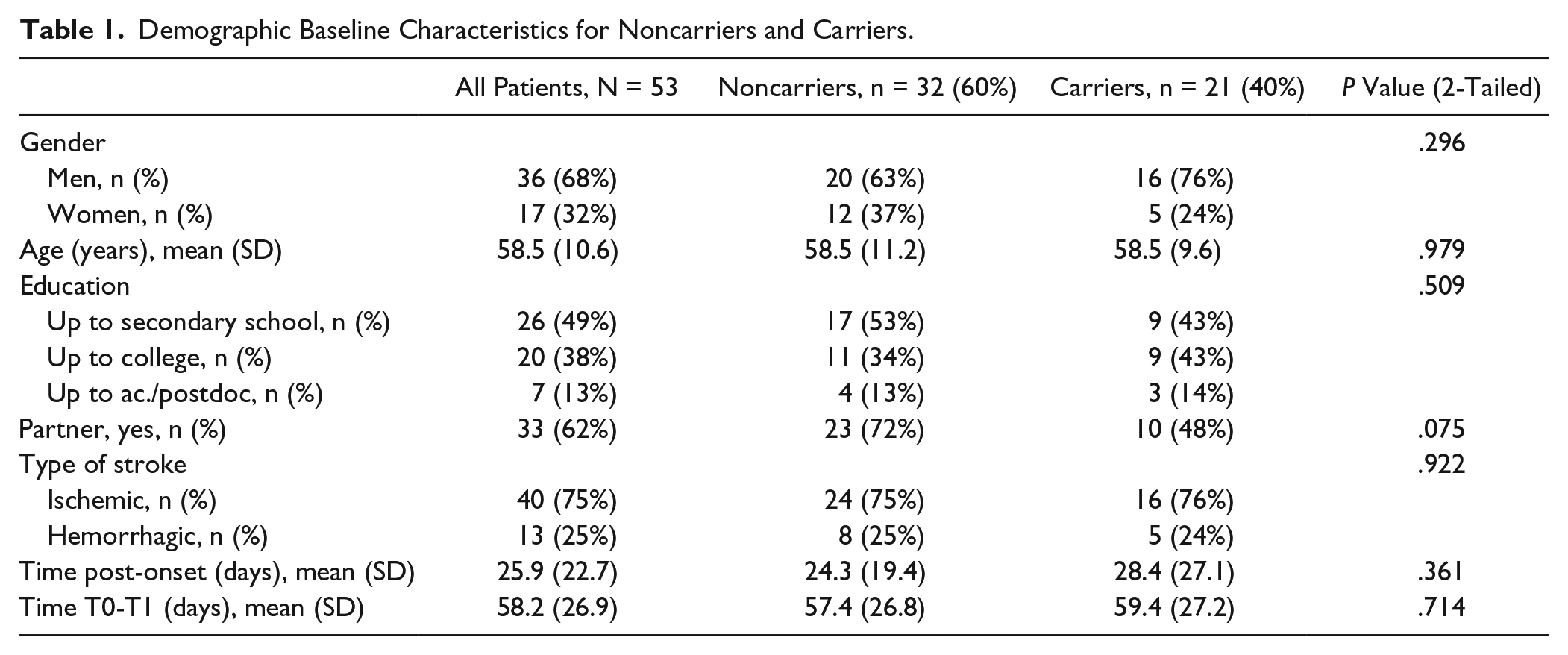
We included 60 patients during an inclusion period of 2 years (data are available on request from the corresponding author). We were able to collect BDNF data of 53 patients, as 7 patients were unable to fill up the saliva samples due to oral apraxia. For some participants scores on either T0 or T1 were missing, namely, 3% of the BNT scores and 5% of the ANELT scores were missing. For baseline characteristics, see Table 1. The Val group consisted of 32 patients (60%), and the Met group consisted of 21 patients (40%), including 2 patients with 2 Met alleles. At baseline, there were no significant differences between the groups. However, there was a trend for having a partner, such that noncarriers more often had a partner compared to the carriers, χ2(1, N = 53) = 3.18, P = .075. The Met group contained more men than women (76% men), although this was not significantly different from the gender distribution in the Val group (63% men; χ2(1, N = 53) = 1.09, P = .296).
Demographic Baseline Characteristics for Noncarriers and Carriers.
On both language tests there was a large variability in baseline scores in both groups and there was also considerable variability in improvement on both language tests, as shown in Figure 1 (ANELT) and Figure 2 (BNT). Within each group the improvement over time was significant for both tests (Table 2). The Val group improved significantly on the ANELT (estimated mean difference = 10.15, P < .001) and on the BNT (estimated mean difference = 13.39, P < .001). The Met group improved significantly on the ANELT (estimated mean difference = 10.20, P < .001) and on the BNT (estimated mean difference = 14.46, P < .001). Differences in improvement between the 2 groups were not significant, neither on the ANELT (estimated mean difference = 0.05, P = .984) nor on the BNT (estimated mean difference = 1.07, P = .770). Subgroup analyses for having a partner did not show any evidence for a significant difference in improvement between the Val and Met groups.
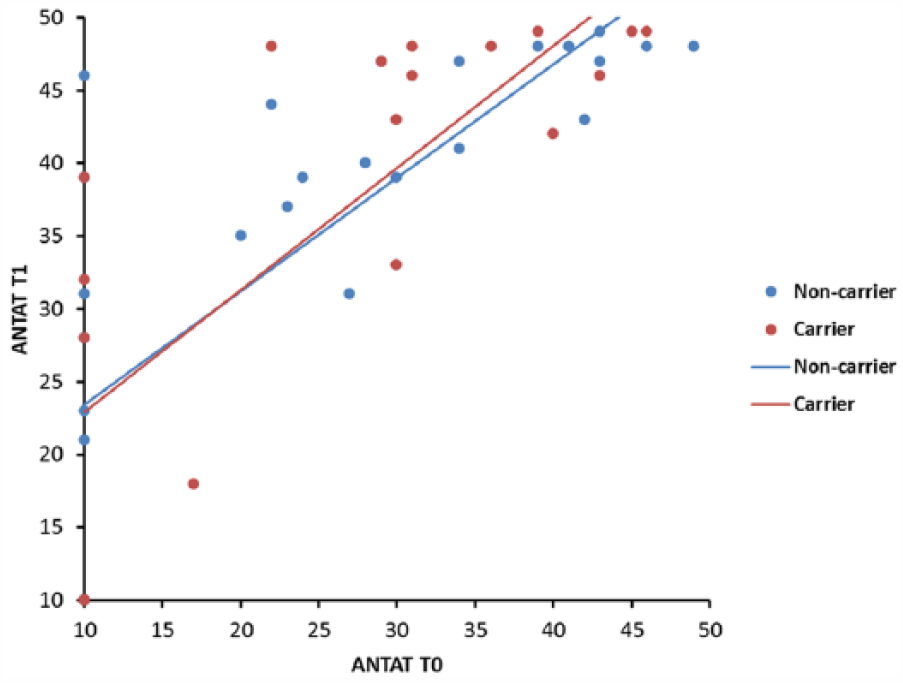
Individual scores on the ANELT (Amsterdam-Nijmegen Everyday Language Test) at admission and discharge with regression lines for the Val group (blue) and the Met group (red).
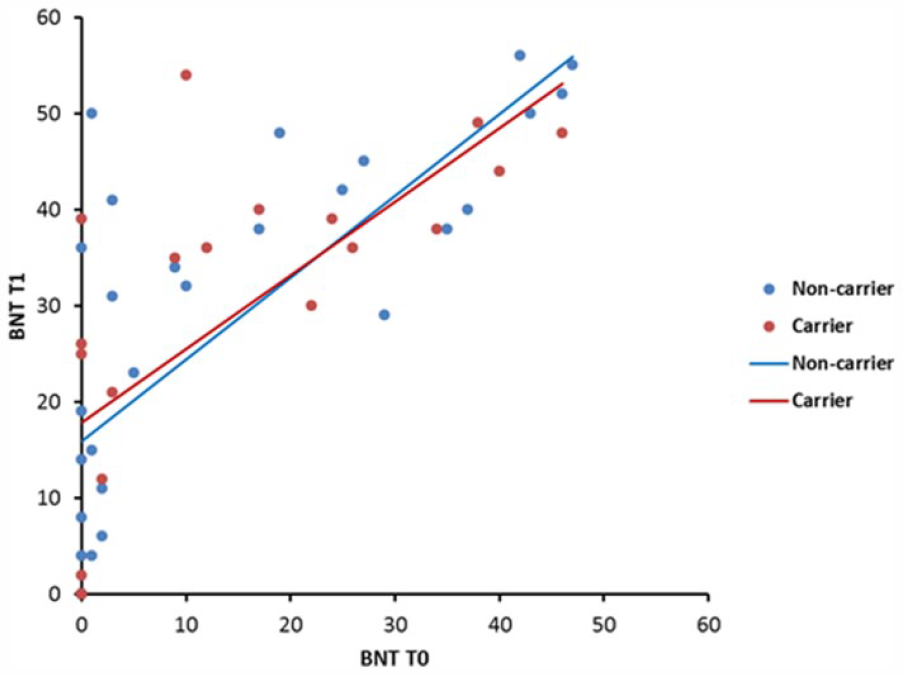
Individual scores on the BNT (Boston Naming Test) at admission and discharge with regression lines for the Val group (blue) and the Met group (red).
Estimated Means, Improvement Scores, and Mean Differences in Language Outcomes Between Carriers and Noncarriers.
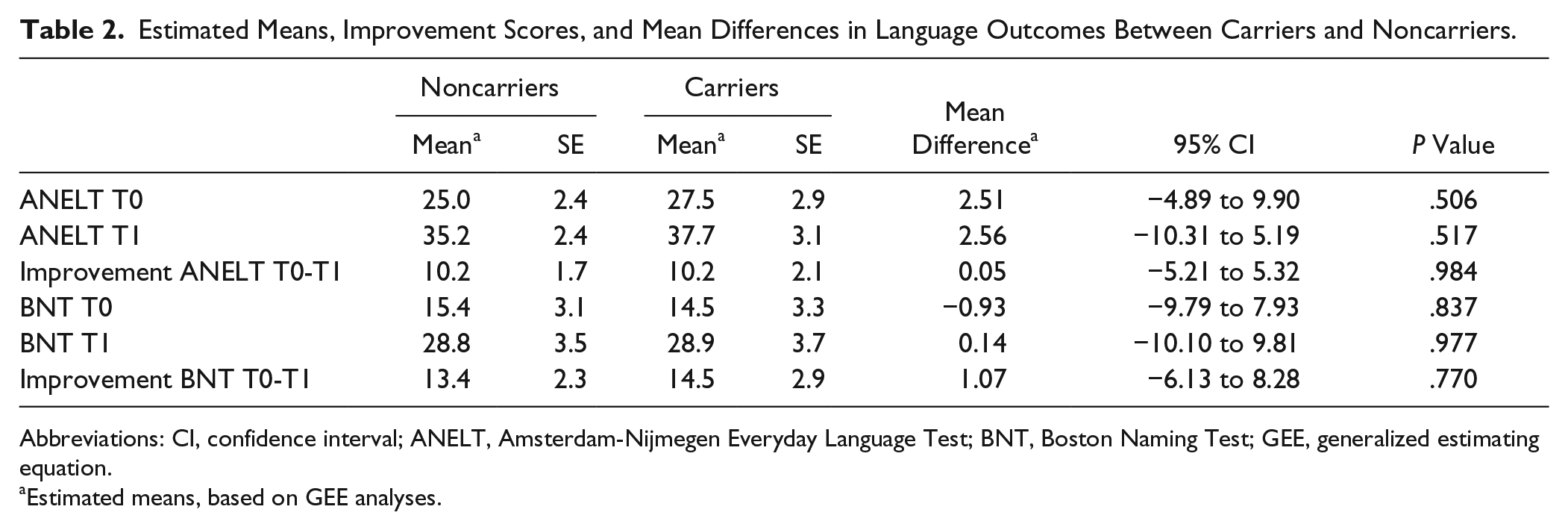
Abbreviations: CI, confidence interval; ANELT, Amsterdam-Nijmegen Everyday Language Test; BNT, Boston Naming Test; GEE, generalized estimating equation.
Estimated means, based on GEE analyses.
Discussion
The aim of our study was to investigate the influence of the BDNF Val66Met polymorphism on language recovery in patients with poststroke aphasia. In a prospective follow-up study, the BDNF Val66Met polymorphism was determined in a group of 53 stroke patients with aphasia, who received regular aphasia rehabilitation in the subacute phase after stroke. Thirty-two were noncarriers of a Met allele and 21 were carriers (at least one Met allele). Language recovery in each group was quantified by assessing the ANELT and BNT at admission and discharge at the clinic. The results showed no significant differences between the carriers and noncarriers in the level of improvement on either the ANELT or BNT, in contrast to our expectations.
The results of our study are in line with one previous study, 36 although this study differed from our study in several ways. The authors focused on brain stimulation and therapy consisted of repetitive transcranial magnetic stimulation or sham stimulation together with language therapy. Furthermore, they used other outcome measures (Aphasia Severity Rating Scale) and included only ischemic stroke patients. Despite these differences, the results also suggest that the BDNF polymorphism does not influence aphasia recovery after stroke.
In our study, the Met group contained relatively more men (76%) compared to the Val group (63% men); however, this difference did not reach significance. In other studies on the relation between the BDNF Val66Met polymorphism and neuroplasticity after stroke no gender differences were described. One study with stroke patients reported higher BDNF serum levels in male carriers compared to male noncarriers, but showed no meaningful gender-related differences in concentration of BDNF serum. 46 Also, the distribution of the BDNF polymorphism in healthy subjects (mainly elderly) and stroke patients did not show dissimilarities in gender.47,48 Taking into account these results, we assume that the high number of men in the Met carriers in our study group should be considered a coincidence.
In the present study, we included both ischemic and hemorrhagic strokes. Previous research on the BDNF polymorphism did not show any relation with the type of stroke. 49 Concerning outcome after stroke, studies have reported contradictory findings. Whereas the BDNF polymorphism did not seem related to general—unspecified—outcomes in a study in hemorrhagic stroke patients, 8 the outcomes of recovery after 3 months was described as poorer among those with a Met allele in Chinese ischemic stroke patients. 33 The difference in general outcome after stroke might also be explained by the plasticity of specific intracortical regions, which might be polymorphism specific. 8
The results of the present study do not support our hypothesis that BDNF plays a role in the early phase of language recovery after stroke, when spontaneous recovery interacts with treatment. Studies have shown that BDNF would underlie learning processes; however, the exact role of learning processes in early language rehabilitation is largely unknown. The interaction between spontaneous recovery and treatment in the early phase poststroke remains disputable. One recent study has found no difference in language recovery between a group receiving intensive aphasia treatment compared to a group receiving no treatment. 50 In the context of the present study, it would be interesting to investigate how BDNF may interact with SLT in the chronic phase.
Limitations
The present study has several limitations. First, there was large variation in the improvement of scores on both tests over time, decreasing the chance of detecting a significant difference in a relatively small group of participants. The duration of rehabilitation also varied between patients, depending on many factors (such as severity of stroke, conditions for discharge, social factors), which may also have influenced the progress of recovery during the inpatient rehabilitation.
Furthermore, we did not take into account the severity of stroke. Neuroplasticity might be reduced by the impact and volume of the stroke, as well as the overall intensity of the inpatient rehabilitation program. For example, increased time spent on motor training will give the patient less time to process the aphasia training skills. We did not find any studies describing the relation between lesion volume and BDNF polymorphism on language outcome after stroke.
Third, although aphasia was the most prominent symptom in our participants, a concomitant apraxia could not be excluded. In clinical practice, it is hard to disentangle the impact of apraxia of speech on language performance in people with aphasia. Therefore, we cannot exclude that the presence of apraxia may have had some impact on test performance.
Conclusions
To our knowledge, this study is the first to investigate the effect of BDNF Val66Met polymorphism on neuroplasticity in aphasia after stroke. In contrast to studies describing an effect of the BDNF polymorphism on motor learning and motor function recovery, we found no significant difference in language recovery between poststroke aphasia patients carrying a Met allele compared to noncarriers. Therefore, the present results suggest that the BDNF polymorphism does not significantly influence aphasia recovery through SLT after stroke. However, genotyping this polymorphism after stroke might still be valuable to further unravel the mechanisms that determine recovery of aphasia after stroke. Future longitudinal studies are needed to investigate the influence of the BDNF polymorphism on language recovery during stroke rehabilitation. It might be interesting to investigate whether a distinction can be made between language recovery and language learning after stroke. Multiple measurements should be performed over time within a larger study population to study recovery patterns during the (sub)acute and chronic phases and to study the effect of covariables, for example, stroke severity or type of stroke.
Footnotes
Acknowledgements
The authors wish to express their appreciation to the participating rehabilitation centers, the therapeutic assistants, the participants, and their caretakers for their cooperation during the course of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.