
Abstract
Background. Recovery of arm function after stroke is often incomplete. An improved understanding of brain structure–motor behavior relationships is needed for the development of novel and targeted rehabilitation interventions. Objective. To examine the relationship between skilled reach performance and the integrity of two putative white matter motor pathways, corticospinal tract and corpus callosum, after stroke. Methods. Eleven individuals with chronic stroke (poststroke duration, mean 62.5 ± 42.4 months) and mild motor impairment (upper extremity Fugl-Meyer score, mean 54.2 ± 7.6) reached to six targets presented at three distances and two directions. Fractional anisotropy (FA) obtained from diffusion tensor imaging was used to determine the structural integrity of the corticospinal tract and the corpus callosum. Results. Overall reach performance was decreased in the paretic arm compared with the nonparetic arm. While FA was decreased in the ipsilesional corticospinal tract, FA in the corticospinal tract did not correlate with variability in reach performance between individuals. Instead, FA in the premotor section of the corpus callosum correlated with reach performance; individuals with higher FA in premotor corpus callosum tended to reach faster with both the paretic and nonparetic arms. Conclusions. The structural connections between the two premotor and supplemental cortices that traverse the premotor corpus callosum may play an important role in supporting motor control and could become a target for interventions aimed at improved arm function in this population.
Introduction
Recovery of arm function after stroke is often incomplete, leading to long-term difficulty incorporating the paretic arm and hand into everyday activities. While current behavioral therapies can improve arm function, 1 deficits in the ability to perform skilled arm movements often remain. An improved understanding of brain-behavior relationships is needed for the development of interventions that promote use of intact, nonlesioned neural structures to improve motor function. 2 White matter pathways are important structures for the transmission of movement-related signals. The integrity of these pathways and their relationship with skilled movement after stroke may provide an important neural correlate of arm function as well as individual response to targeted interventions.3-6
Two important white matter pathways that support skilled movement are the corticospinal tract and the corpus callosum. Stroke lesions can affect the integrity of these pathways either through direct lesion or through secondary cortical disconnection due to lesion at the pathway’s distal target. 7 Several studies have shown that the integrity of the corticospinal tract correlates with motor impairment and function after stroke; individuals with greater integrity in this pathway tend to show less motor impairment, greater motor function, and better response to motor interventions.4-6,8 However, recent work has suggested that integrity of the corpus callosum, the primary structural connection between the two cerebral hemispheres, may also be an important correlate of motor function after stroke.5,9,10 The role of the corpus callosum may be especially important in individuals with mild motor impairment. 11
Measurement of motor impairment and function across a spectrum of motor impairment levels can be challenging. Common clinical measures such as the upper extremity Fugl-Meyer show a ceiling effect.12-14 Therefore, other measures of motor capacity and skill may be more optimal in quantifying movement ability, especially in individuals with mild motor impairment. Kinematic measures have been used as a tool to measure upper extremity movement capability15,16 and may be more sensitive to milder motor deficits after stroke.17,18 In individuals with minimal motor impairment, kinematic measures of reach performance may better represent arm motor capacity and, therefore, be an appropriate tool in this population for studies investigating motor behavior–brain structure relationships.
To our knowledge, no research to date has investigated the relationship between skilled reach performance and the structural integrity of putative motor pathways in individuals with motor impairment due to stroke. Therefore, the purpose of this preliminary investigation was to examine the correlation between kinematic measures of reach performance and the integrity of two white matter pathways, the corticospinal tract and the corpus callosum. Using sensitive tools of brain and behavior, we hypothesized that reach performance would correlate with structural integrity in both pathways and thereby support the role of corticospinal tract and corpus callosum in the control of skilled movement after stroke.
Methods
Participants
Individuals included in this analysis were a subset of individuals from a parent study19,20 who were able to undergo magnetic resonance imaging (MRI). Participants had to be right-hand dominant, 21 have a history of stroke at least 3 months prior, and have some movement capability in the more affected arm (upper extremity Fugl-Meyer [UE FM] motor score 22 ≥28). Potential participants were excluded if they presented with cognitive impairment (score <25 on the Mini-Mental State Exam 23 ), hemispatial neglect (score <52 on the BIT [Behavioral Inattention Test] star cancellation test 24 ), current pain in either arm, botulinum toxin injection in the paretic arm within the previous 3 months, surgical intervention in either arm within the previous 6 months, or any contraindication to MRI. 25 Arm motor function was measured using the UE FM total motor score (maximum score 66), UE FM proximal subscale (maximum score 36), Action Research Arm Test (ARAT), 26 and Stroke Impact Scale (SIS) hand domain. 27 All participants provided written informed consent prior to participation through a protocol approved by the Health Sciences Institutional Review Board at the University of Southern California.
Reaching Task
The experimental task and procedure have been described in detail previously. 20 Briefly, individuals performed three-dimensional reach movements to six targets (3.8 cm sphere) presented in two directions (+45°, −45°) and three distances (8, 16, 24 cm) (Figure 1) in an immersive virtual environment (VE) (Innovative Sports Training, Inc, Chicago, IL). The target was visible while reaching but the arm and virtual cursor that represented finger position (2 cm sphere) were not, thereby eliminating online visual feedback during movement. Visual postresponse feedback was provided after each trial which showed the proximity of endpoint finger position to the target. Participants were instructed to “Reach to the target as fast as possible when ready”; speed of movement was prioritized over accuracy and participants were reminded to move quickly throughout data collection.
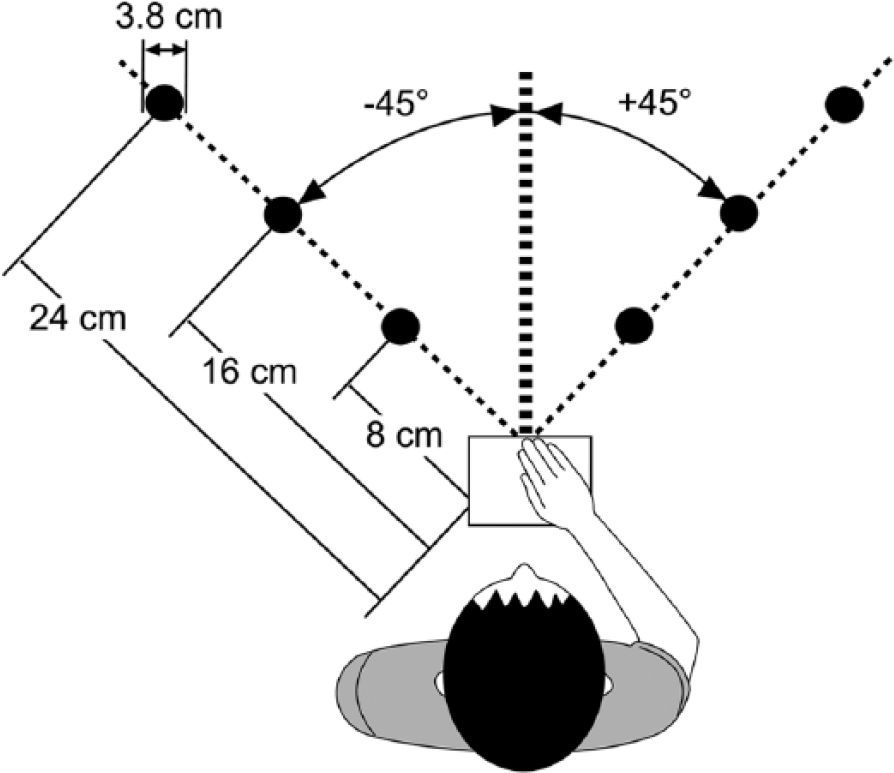
Schematic of reach paradigm. Six targets were presented in two directions (+45°, −45°) and three distances (8, 16, 24 cm) in an immersive virtual environment. The start switch (open square) was aligned with the sternum.
Participants completed the reaching task with the ipsilesional arm first followed by the contralesional arm with a 30- to 60-minute break between arm sessions. For ease of discussion and presentation of results, we will refer to these as the nonparetic and paretic arms, respectively. After a practice period, participants completed a total of 168 reach trials (7 blocks of 24 trials presented in a pseudo-random order) with each arm. The first two blocks (48 trials) were dropped from data analysis to eliminate any effects of learning related to the VE; the remaining 120 trials (20 trials per target, 60 trials per direction) were used in analyses.
Index finger position was collected from an electromagnetic sensor at a sampling rate of 120 Hz throughout each reach trial and analyzed using a custom script in MATLAB (Mathworks, Inc, Natick, MA). Position data were filtered with a low-pass second-order Butterworth filter with a 10-Hz cutoff and differentiated to determine velocity and acceleration. 28 For each trial, peak acceleration (first peak after movement onset), peak velocity (first peak after movement onset), movement time, and endpoint error (3-dimensional linear distance between target and finger position at movement offset) were extracted using previously described methods. 20 To quantify overall reach performance, the mean of each kinematic variable across all target distances was calculated for each participant. Because of the effect of movement direction on the magnitude of kinematic variables,29,30 data for each target direction were analyzed separately. Target direction was converted to indicate either an ipsilateral reach (right arm reaching to +45° targets, left arm reaching to −45° targets) or contralateral reach (right arm reaching to −45°, left arm reaching to +45° targets) for group analyses (see Figure 1).
Brain Imaging
A single brain imaging session was performed on a 3-T GE MRI scanner (General Electric, Fairfield, CT). First, a high-resolution fast SPGR, T1 structural image was acquired (repetition time [TR] = 7.8 ms, echo time [TE] = 3.0 ms), which included 184, 1-mm thick axial slices with no interslice gap (acquisition voxel size 0.94 mm × 0.94 mm × 1.0 mm). Next, diffusion tensor images (DTI) were obtained using echo planar imaging (TR = 16 600 ms, TE = 87.6 ms) and included 60, 2-mm think axial slices with no interslice gap (acquisition voxel size 1 mm × 1 mm × 2 mm). Diffusion images included 25 noncollinear directions with a b value of 1000 and a single volume with no diffusion weighting (b = 0). Total scan time for each session was approximately 30 minutes.
Analysis of DTI images was completed in FSL (FMRIB Center, Oxford, UK) using the FDT toolbox. 31 Diffusion images were corrected for eddy currents and head motion followed by removal of the skull and dura. 32 A voxelwise map of fractional anisotropy (FA) was then created. FA is a measure of the structural integrity of white matter with values ranging between 0 (isotropic) and 1 (anisotropic). 33 Higher FA values indicate greater white matter structural integrity along a primary direction. Region of interest (ROI) masks were manually drawn on sections of the corpus callosum and the corticospinal tract in each participant’s native space using the colorized FA 34 and structural T1 images (coregistered into FA space) as guides (Figure 2). The premotor, motor, and sensory sections of the corpus callosum were defined as sections II, III, and IV, respectively, as described by Hofer and Frahm 35 ; each mask included the center slice and four adjacent slices (two to the right, two to the left). To determine the integrity of the corticospinal tract, an ROI was drawn on the axial slice that showed the largest cross-sectional area of the cerebral peduncle.3,36 The cerebral peduncle was chosen for this measure as it contains descending corticospinal tract motor fibers and was remote from the stroke lesion in this study cohort. The accuracy of all masks was confirmed by a second investigator. Mean FA was extracted from each ROI using a threshold of FA >0.2.
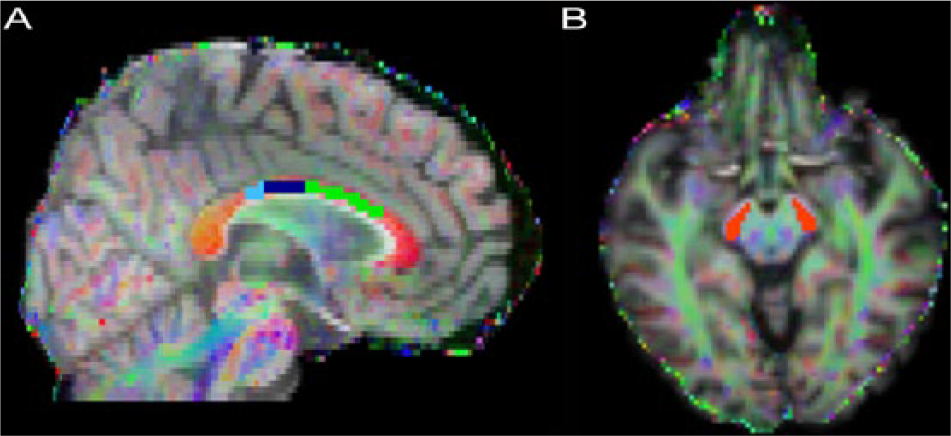
Example region of interest masks for a single participant in the corpus callosum (A) and cerebral peduncle (B). Masks were drawn on colorized fractional anisotropy (FA) images in the motor section (dark blue), sensory section (light blue), and premotor section (green) of the corpus callosum and the corticospinal tract (red).
Statistical Analysis
Data were checked for normality using the Shapiro-Wilk test. All data met the criteria for normality (P > .05) except for a few reach performance kinematic variables (movement time, peak acceleration). A log transform was used on these data and the criteria for normality were met; the transformed data were used for all statistical analyses. Mean peak acceleration, peak velocity, movement time, and endpoint error were compared between arms (paretic/nonparetic) using a paired t test; reaches to ipsilateral and contralateral targets were analyzed separately for all variables. Mean FA in the ipsilesional corticospinal tract was compared with mean FA in the contralesional corticospinal tract using a paired t test.
The relationship between mean FA in each ROI and both clinical measures of motor function and reach performance was determined using correlation analysis (Pearson’s r). Since we did not have an a priori hypothesis about which kinematic variable would be best to examine brain-reach performance relationships and to reduce the number of correlations being performed, reach performance variables were combined using principal component analysis (PCA). Measures of reach speed (peak velocity, peak acceleration, movement time) for both ipsilateral and contralateral targets were combined using PCA to create a single factor for reach speed; the first component accounted for 90% of the variance in these kinematic measures for the nonparetic arm and 87% of the variance for the paretic arm. Endpoint error for reaches in both directions was combined to create a single factor for reach error; the first component accounted for 88% of the variance for the nonparetic arm and 51% of the variance for the paretic arm. The strength of correlations was interpreted based on the value of the correlation coefficient: r < 0.25 = little or no relationship; r of 0.25 to 0.50 = fair; r of 0.50 to 0.75 = moderate; r > 0.75 = strong. 37 Significance level was set at P < .05 for all statistical tests. SPSS 22 (IBM Corp, Armonk, NY) statistical software was used for all analyses.
Results
Participants
Eleven right-hand dominant individuals with chronic stroke (mean months poststroke 62.5 ± 42.4) participated in this study (Table 1). Overall, participants had mild motor impairment (mean UE FM score 54.2 ± 7.6) but reported continued difficulty using the paretic arm and hand to perform functional activities (mean SIS hand domain score 63.2 ± 23.6). The UE FM motor score and ARAT score were very strongly correlated (r = 0.934, P < .001); therefore, correlation analyses were completed with the UE FM only. Stroke lesions were both cortical and subcortical and were equally distributed between the right and left hemispheres. The ROIs used to examine structural integrity of the corticospinal tract and corpus callosum were not directly injured by stroke in any participant.
Participant Demographics.
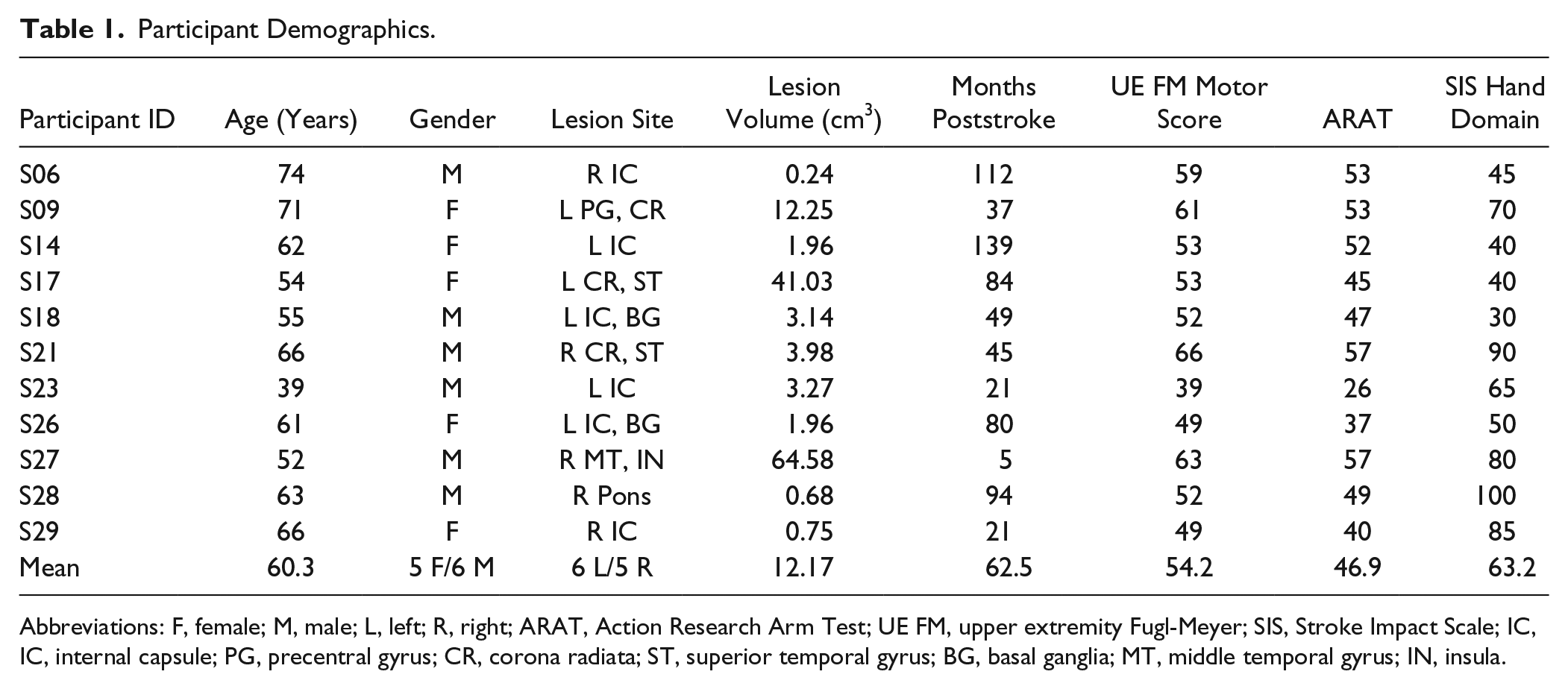
Abbreviations: F, female; M, male; L, left; R, right; ARAT, Action Research Arm Test; UE FM, upper extremity Fugl-Meyer; SIS, Stroke Impact Scale; IC, IC, internal capsule; PG, precentral gyrus; CR, corona radiata; ST, superior temporal gyrus; BG, basal ganglia; MT, middle temporal gyrus; IN, insula.
Reach Performance
Overall reach performance is summarized for the nonparetic and paretic arms in Table 2. For reaches to both the ipsilateral and contralateral targets, reaches with the paretic arm had significantly lower peak velocity, lower peak acceleration, and longer movement time compared with reaches with the nonparetic arm. Endpoint error was larger for reaches in both directions with the paretic arm, however, this difference only reached statistical significance for reaches to the contralateral targets. Neither reach speed nor reach error (score from PCA) for reaches with the paretic arm significantly correlated with UE FM total score (r < 0.531, P > .093), UE FM proximal subscale (r < 0.349, P > .292), SIS hand domain score (r < 0.108, P > .751), stroke lesion volume (r < 0.265, P > .431), or time poststroke (r < 0.120, P > .725). While not statistically significant, UE FM total score did show a moderate correlation with reach error (r = −0.531, P = .093).
Reach Performance. a
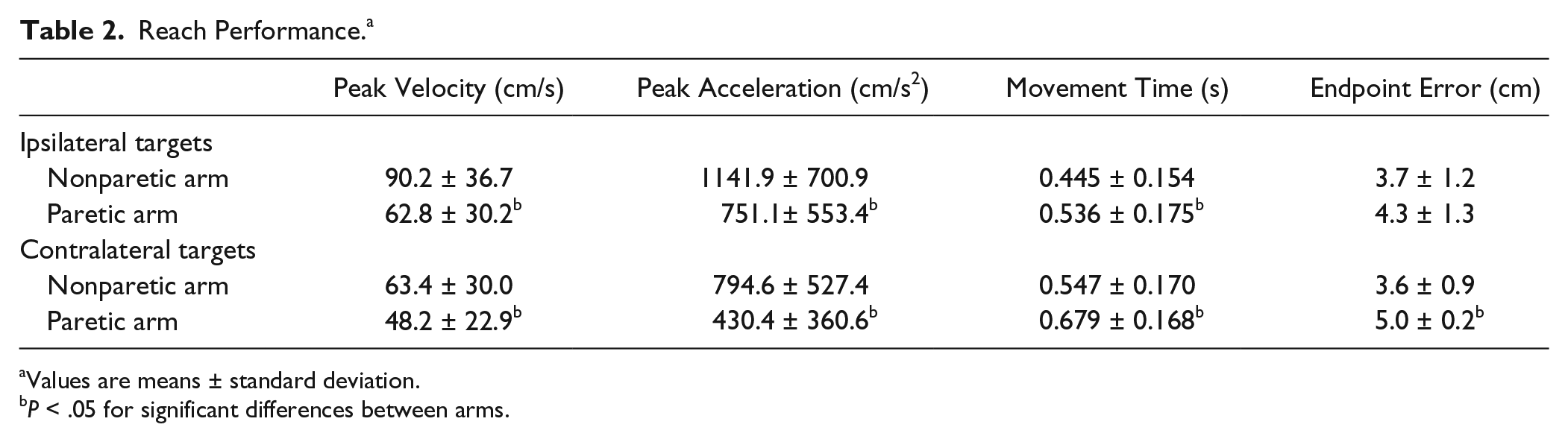
Values are means ± standard deviation.
P < .05 for significant differences between arms.
Structural Integrity of Corticospinal Tract and Corpus Callosum
Mean FA in the corticospinal tract and each region of the corpus callosum are shown in Figure 3. As expected, FA in the ipsilesional corticospinal tract was significantly lower than FA in the contralesional corticospinal tract (P = .002). Mean FA in the corticospinal tract (ipsilesional or contralesional) did not significantly correlate with mean FA in any section of the corpus callosum (r < 0.326, P > .33). FA in the motor section of the corpus callosum significantly correlated with FA in the sensory section (r = 0.751, P = .008) while neither of these regions correlated with FA in the premotor section (r < 0.464, P > .151). UE FM total score and SIS hand domain did not correlate with FA in the ipsilesional corticospinal tract or any section of the corpus callosum (r < 0.462, P > .152); UE FM proximal subscale did correlate with FA in ipsilesional corticospinal tract (r = 0.630, P = .038).
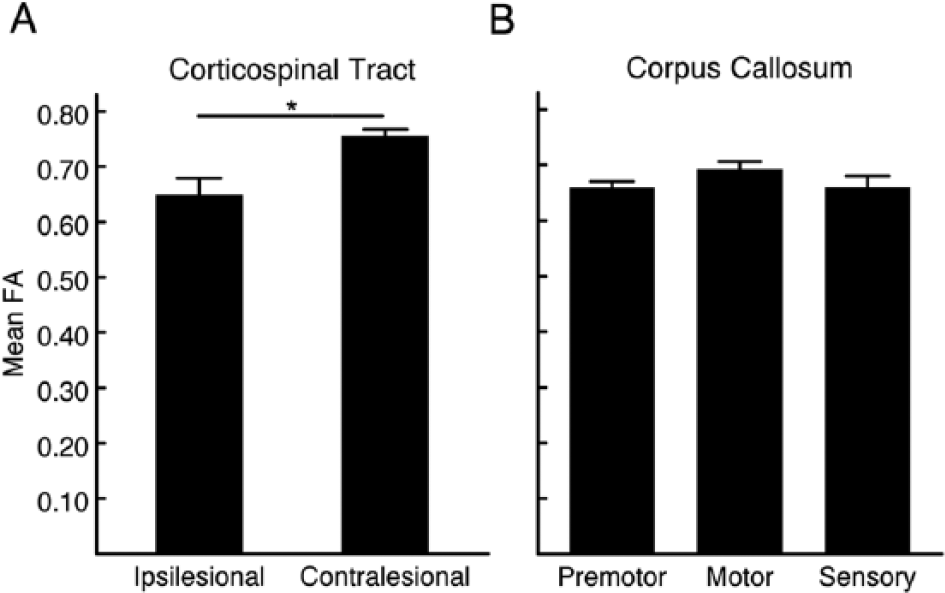
Mean fractional anisotropy (FA) in the corticospinal tract and corpus callosum. Each bar represents the group mean with standard error bars for mean FA in the corticospinal tracts (A) and the premotor, motor, and sensory sections of the corpus callous (B). *P < .05 for differences between sides.
Relationship Between Brain Structural Integrity and Reach Performance
FA in the premotor section of corpus callosum showed a moderate to strong correlation with reach speed in both the nonparetic and paretic arms (Figure 4) but did not correlate with reach error (r < 0.470, P > .145). Overall, individuals with higher FA in this region tended to have faster reach speed in both the nonparetic (r = 0.779, P = .005) and paretic arm (r = 0.594, P = .054). No significant correlation was found between FA in the corticospinal tract, motor section of the corpus callosum, or sensory section of the corpus callosum and reach speed (r < 0.276, P > .406) or reach error (r < 0.385, P > .242) in either arm. A follow-up comparison was done between peduncle FA asymmetry ratio (ipsilesional peduncle/contralesional peduncle; represents the relative integrity of the ipsilesional corticospinal tract compared with the contralesional corticospinal tract for each individual) and reach performance with the paretic arm. No significant correlation was found between FA asymmetry ratio and reach performance (r < 0.295, P > .378).
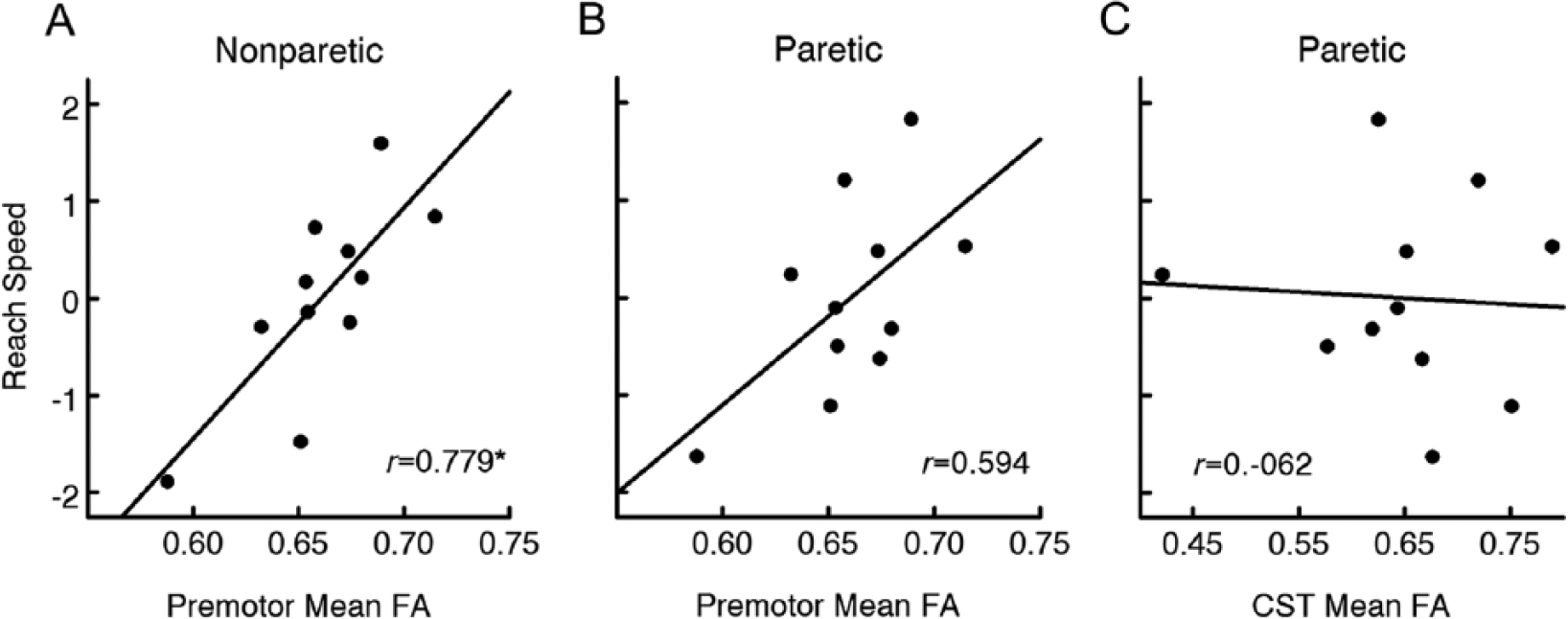
Relationship between reach speed and fractional anisotropy (FA) in the premotor section of the corpus callosum (A, B) and the ipsilesional corticospinal tract (C). Reach speed represents a composite score determined via principal component analysis. Regression line and correlation coefficient shown in each plot. Nonparetic = nonparetic arm reaches; Paretic = paretic arm reaches; CST = corticospinal tract. *P < .05 for significant correlation.
Discussion
This preliminary investigation examined the relationship between kinematic measures of reach performance and the structural integrity of two putative white matter pathways, the corticospinal tract and the corpus callosum, in individuals with mild motor impairment due to stroke. Deficits in reach performance were present in the paretic arm consistent with many previous reports.38-40 Additionally, the structural integrity of the corticospinal tract in the lesioned hemisphere was decreased compared to the same tract in the nonlesioned hemisphere consistent with previous studies.5,41,42 However, variability in reach performance between individuals did not correlate with variability in corticospinal tract integrity as expected. Instead, only the premotor section of the corpus callosum correlated with reach performance, specifically measures of movement speed. This finding increases our knowledge of the neural correlates of skilled arm tasks in individuals with mild motor impairment after stroke and may have implications for the application of intervention protocols aimed at improving arm function in this patient population.
In the current study, the premotor but not the motor section of the corpus callosum correlated with skilled reach performance in both the paretic and nonparetic arms, specifically with reach speed. The premotor section of the corpus callosum (section II from Hofer and Frahm) is reported to contain interhemispheric fibers between dorsal premotor and supplementary motor areas,35,43 regions where functional activation is thought to support movement after stroke.44-46 The integrity of the premotor section of the corpus callosum has been shown to correlate with the performance of skilled motor tasks in older, nondisabled adults.47,48 Less is known about how corpus callosum integrity correlates with skilled movement after stroke. Several studies have suggested that the integrity of the motor section of the corpus callosum correlates with clinical measures of motor impairment and function after stroke.5,9,10 However, conflicting results have been reported suggesting that regions of the corpus callosum other than the motor section are significant correlates of motor function in individuals with motor impairment due to stroke. 49 Our results provide further evidence for the importance of interhemispheric connections contained in the corpus callosum for skilled movement after stroke. Future studies should consider the premotor section of the corpus callosum for examination of brain-behavior relationships in this population.
We did not find a correlation between ipsilesional corticospinal tract integrity and reach performance as hypothesized. The participants in this study had a mean UE FM motor score of 54 out of a maximum of 66, suggesting they had relatively mild upper extremity motor impairment. This lack of correlation between corticospinal tract integrity and measures of movement function in individuals with mild motor impairment is consistent with a recent study in a larger population. Stewart et al 11 found that corticospinal tract integrity correlated with motor impairment when individuals with a wide range of impairment were grouped into a single analysis. However, in the subgroup of individuals with less motor impairment (mean UE FM motor score of 52 out of 66), there was no relationship between corticospinal tract integrity and clinical measures of motor impairment and function. It is also possible that the lack of correlation between corticospinal tract integrity and movement was related to the demands of the motor task. The corticospinal tract is thought to play a greater role in the control of hand and finger muscles than in proximal arm muscles. 50 The reach task used here focused on proximal arm control without a distal hand component; as such, task completion could have been governed more by pathways other than the corticospinal tract. 51 The results of the current study, combined with previous work, suggest that in individuals with mild motor impairment, neural resources other than the corticospinal tract may play an important role in supporting skilled reaching behavior after stroke.
Kinematic measures of reach speed correlated with brain structural integrity in the premotor section of the corpus callosum. The only clinical measure that correlated with brain structural integrity was the UE FM proximal subscale which had a positive relationship with corticospinal tract integrity. These two measures, reach speed and the UE FM, likely measure different aspects of arm motor capacity, for example, the ability to move the arm quickly versus the ability the move the arm and shoulder within and out of synergy patterns. This result provides support for kinematic measures for understanding brain-behavior relationships in individuals with mild motor impairment. Measures of reach error did not correlate with integrity in any brain structure studied. During data collection, movement speed was emphasized over accuracy. Therefore, it is likely the paradigm used here pushed the capacity of the movement system in the speed domain. Paradigms that focus on other important aspects of reach control such as accuracy, may find that different measures of behavioral performance are correlated with brain structure.
The results of the current study may have implications for interventions that target skilled reaching or include brain stimulation in combination with task-oriented training after stroke. Interventions aimed at improving proximal arm function in individuals with mild motor impairment should consider the integrity of transcallosal fibers in the premotor section of the corpus callosum in addition to the integrity of the corticospinal tract when evaluating individual response to treatment. Additionally, response to brain stimulation protocols that target the functional connectivity between the two hemispheres in combination with motor training52,53 may vary based on the structural integrity of transcallosal fibers. Many studies using noninvasive brain stimulation in combination with physical training have focused on ipsilesional and/or contralesional primary motor cortex with mixed results.54,55 The premotor cortices have recently been suggested as an appropriate target for these brain stimulation techniques. 55 The integrity of the interhemispheric connections between premotor cortices may be important in determining the effectiveness of this approach.
This study used an ROI approach to quantify brain structural integrity and focused on two putative motor pathways (corticospinal tract, corpus callosum). The combination of measures of brain structural and functional connectivity and/or inclusion of other motor pathways such as the rubrospinal tract 56 could provide a more robust understanding of brain-skilled reaching behavior relationships. The validity of the ROI approach used to quantify FA in the corpus callosum (Hofer and Frahm 35 ) has not been fully validated in stroke. This approach has been commonly used in studies of brain structure after stroke11,49,57,58 allowing for interstudy comparison. However, the relationship between this ROI approach and other approaches (eg, tracts drawn between two motor cortices or different segmentation approaches 59 ) in individuals poststroke needs additional investigation.
The participants investigated here had mild motor impairment and were in the chronic phase of stroke recovery. The brain-behavior relationships found here may be different in individuals with less movement capability or in the acute phase of recovery. The current study utilized a cross-sectional design. Future longitudinal studies could investigate if the relationship between skilled reaching and premotor corpus callosum integrity changes with training or time. Finally, this was a preliminary investigation with a small sample size, which limited our ability to investigate the effects of possible covariates such as lesion location and extent or level of motor impairment. Our results show promise and suggest further exploration of the relationship between brain structure and kinematic measures of skilled reaching in a larger sample of individuals recovering from stroke.
Conclusions
In individuals with mild motor impairment due to stroke, the structural integrity of the premotor section of the corpus callosum but not the corticospinal tract correlated with speed-based kinematic measures of skilled reach performance. Individuals with higher structural integrity in the premotor corpus callosum exhibited faster reach performance. The structural connections contained in this section of the corpus callosum, between the two premotor and supplemental cortices, may play an important role in supporting movement and could be a target for neurorehabilitative interventions aimed at improved arm function in this population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided in part through a Mary McMillan Doctoral Scholarship and a Promotion of Doctoral Studies II Scholarship from the Foundation for Physical Therapy and a grant from the California Physical Therapy Fund to JCS. The virtual reality system used in this study was provided by Innovative Sports Training, Inc.