
Abstract
Background. Trunk function is important for standing balance, mobility, and functional outcome after stroke, but few studies have evaluated the effects of exercises aimed at improving core stability in stroke patients. Objective. To investigate the effectiveness of core stability training on trunk function, standing balance, and mobility in stroke patients. Methods. An assessor-blinded, randomized controlled trial was undertaken in a stroke rehabilitation ward, with 32 participants randomly assigned to an experimental group or a control group (n = 16 each). The experimental group received 400 minutes of core stability training in place of conventional programs within total training time, while the control group received only conventional programs. Primary outcome measures were evaluated using the Trunk Impairment Scale (TIS), which reflects trunk function. Secondary outcome measures were evaluated by pelvic tilt active range of motion in the sagittal plane, the Balance Evaluation Systems Test–brief version (Brief-BESTest), Functional Reach test, Timed Up-and-Go test (TUG), and Functional Ambulation Categories (FAC). A general linear repeated-measures model was used to analyze the results. Results. A treatment effect was found for the experimental group on the dynamic balance subscale and total score of the TIS (P = .002 and P < .001, respectively), pelvic tilt active range of motion (P < .001), Brief-BESTest (P < .001), TUG (P = .008), and FAC (P = .022). Conclusions. Core stability training has beneficial effects on trunk function, standing balance, and mobility in stroke patients. Our findings might provide support for introducing core stability training in stroke rehabilitation.
Introduction
Disorders of trunk function are common in stroke patients.1-9 Previous studies have reported muscle weakness and delayed activity of the trunk muscles,1-4 significant error of trunk position sense, 5 inadequate center of pressure control when sitting,6,7 decreased trunk performance, 8 and trunk asymmetry during gait. 9 Trunk function is associated with balance and walking ability in stroke patients,10,11 and has also been found to offer a useful predictor of balance and walking ability 12 and activities of daily living (ADL) outcomes.13-17 Several randomized controlled trials have focused on trunk performance in stroke populations,18-20 and trunk training has reportedly improved trunk performance in experimental groups.20-22 However, those studies either have not equalized the amount of exercise provided with a control group,20,21 or used an overly wide variety of trunk training interventions.20-23 As such, it is not yet clear which types of trunk training are more useful to improve trunk performance in stroke patients. According to a recent review, optimal specific training remains unclear, and evidence is insufficient.18,19
To improve performance of the trunk muscles, stabilization training is generally employed along with muscle strength and muscular endurance training. 24 The concept of the “core” and the need to retrain “core stability” has been a recent focus in the fields of low back pain and sports. 25 The “core muscles” include many muscles supporting the lumbo-pelvic-hip complex. 25 Bergmark 26 classified the muscles acting on the lumbosacral spine as either “local” or “global.” The “local” muscles work for segmental stability system, while the “global” muscles work for movement of the spine. Faries and Greenwood 27 described the transversus abdominis (TrA), diaphragm, pelvic floor muscles, and deep fibers of the lumbar multifidus as local muscles and the rectus abdominis, erector spinae, psoas major, and the like as global muscles. They also provided definitions of “core stability,” referring to the ability to stabilize the spine as a result of local muscle activity. Key 28 emphasized stabilizing co-contraction increasing intra-abdominal pressure via the control of local core muscles as the “stabilization synergy” of the core. “Core stability training” is introduced from the activation of the TrA as a primary local muscle in the “core” muscles. For this purpose, abdominal drawing-in maneuver (ADIM) training is usually used. 29 ADIM training has been found to selectively activate the TrA,30-32 and have the effect of stabilizing spinal segments. 33 Hodges and Jull 34 and Comerford and Mottram 35 proposed stepwise exercises from local muscles to global muscles and integration of these groups in stability training. Some researchers have reported that core stability training could improve not only trunk function but also balance and mobility.20,36 However, the effects of a protocol based on core stability training have yet to be sufficiently verified in stroke patients.
Although core stability training is expected to offer effective trunk training, evidence for its application in stroke is scarce. Since the innervation of the trunk muscles is bilateral, 37 complete paralysis of the trunk seems unlikely to occur in stroke hemiplegia. 38 Based on the core stability theory, the combination of ADIM as a deep muscle movement and selective pelvic exercises providing superficial muscle movements would be more effective trunk training. Selective pelvic exercises were employed in our protocol because high feasibility for stroke patients has been reported in previous studies showing positive effects of stroke rehabilitation including selective pelvic exercises.20-23 We developed a step-by-step core stability training program using selective pelvic exercises customized for stroke rehabilitation. This program was defined as “core stability training” in the present study.
The novelty of this study lies in the focus on core stability training and the development of an intervention protocol based on the theory that an original, detailed protocol using selective pelvic exercises would benefit patients who had experienced stroke. Participants in the control group received a conventional physical therapy program, including general trunk exercises. In addition, rehabilitation intervention time for the experimental and control groups were comparable, with the time in which participants in the experimental group received core stability training lying within the time allocated for physical therapy. If specific core stability training in this study were to show efficacy in stroke rehabilitation, this approach could represent an effective therapeutic strategy for stroke rehabilitation. The purpose of this study was thus to investigate the effectiveness of core stability training in improving trunk function, standing balance, and mobility among patients showing hemiplegia after stroke. Our hypothesis was that customized and specific core stability training for stroke patients would improve not only trunk function but also balance and mobility, to a greater extent than seen with a conventional comprehensive rehabilitation program.
Methods
Patients
Patients were recruited from among subacute stroke patients hospitalized in Higashisaitama National Hospital between September 2013 and December 2014. Inclusion criteria were a history of first stroke, definite diagnosis of stroke based on computed tomography and/or magnetic resonance imaging, a supratentorial and hemispheric lesion, and more than 1 month and less than 6 months since onset. Exclusion criteria were age 80 years or more, inability to keep a sitting position for 30 seconds, communication problems, comorbidities affecting motor performance such as orthopedic and neurological disorders that could influence postural control, maximum score (score = 23) for trunk performance as assessed by the Trunk Impairment Scale (TIS) 39 at the start of the study, or lack of provision of consent to participate. All participants were asked to provide informed consent before participation. Approval was given by the ethics committee at Higashisaitama National Hospital (Approval Number: 13-6).
Design
This study was designed as an assessor-blinded randomized controlled trial. The number of patients required for this study was calculated a priori to ensure sufficient statistical power. Power estimates were based on a prior study investigating the effect of improvements in TIS. 21 This revealed that a sample size of 28 patients would be necessary to achieve an 80% chance (effect size = 0.39, α = 0.05, power = 0.80). We performed interim analysis as soon as the sample size reached the prescribed number based on the adaptive sequential design, confirming sufficient power to identify significant differences in primary outcome measures. However, differences at baseline were observed in some secondary outcome and recruitment was therefore continued. When baseline equalization was confirmed on continual interim analysis at the inclusion of 32 participants, recruitment to the study was ended.
Subjects were randomly assigned to 2 groups: the experimental group, receiving specific core stability training; and the control group, receiving only the conventional rehabilitation program. To allocate patients to one of these groups, occupational therapists who were blinded to the research performed assignments based on a computer-generated random number. To exclude the influence of effects due to differences in trunk function at baseline, we adopted a permuted-block method combined with stratified randomization using the total TIS score. The block size was 2. Total TIS score was stratified to ≥14 or <14, based on the median score reported for stroke patients. 39
The conduct and report of this trial followed the Consolidated Standards of Reporting Trials (CONSORT) statement for Randomized Trials.40,41 The study was registered with the UMIN Clinical Trials Registry (UMIN-CTR number: UMIN000018667).
Intervention
Patients in the experimental and control groups received the conventional multidisciplinary stroke rehabilitation program provided by the rehabilitation hospital. This conventional treatment program is patient specific and consists mainly of physical therapy, occupational therapy, speech therapy, and nursing care. The physical therapy program takes a comprehensive approach, such as improvement of functions and disabilities, including trunk movement, basic activity, task-directed training, and a compensatory approach using supplementary devices. In both groups, activities such as bridge, pelvic movement, and reaching exercises commonly performed in clinical settings were included in the conventional program. We provided physical therapy for approximately 60 min/day, five times a week in both groups. The experimental group intervention was carried out within this time, so overall rehabilitation time provided did not differ between groups.
In the experimental group, patients received 20 minutes of core stabilization exercises within each daily training session, 5 times a week, for 4 weeks. In total, each patient in this group received 400 minutes of training time. Based on previous studies of trunk exercises that showed effects on stroke rehabilitation, we set the amount of core stability training in the experimental group as about 30% of the total time allocated to physical therapy. The core stability training consisted of ADIM as a selective contraction of TrA, selective movements of the pelvis, and pelvic movements with ADIM. In this training, we increased the level of exercise in stages according to our protocol (Supplementary Figure 1).
For ADIM, subjects were instructed to draw the lower part of the abdomen up and in toward the spine, without movement of the trunk or pelvis while continuing to breathe normally. ADIM was performed in a crook lying position, then in a sitting position. Pelvic control exercises were composed from the following three planes of movement: anterior-posterior tilt; lateral lift; and transverse rotation. Any selective movement of the pelvis was conducted in the sitting position, and compensatory movements were inhibited. Furthermore, motions were performed repeatedly to the maximum range voluntarily possible at a low load. In pelvic control exercises with ADIM, selective pelvic movement was performed while drawing in the abdomen. If any movement was insufficient, the physical therapist provided additional verbal instructions, manipulative induction, or assistance. Propriety of ADIM was judged based on palpation of TrA contraction. 29 All exercises in the sitting position emphasized an upright sitting posture (Supplementary Figure 2).
Eleven physical therapists with no direct involvement in the design and reporting of the present study carried out the treatment and intervention. These therapists were provided an explanations based on the protocol (Supplementary Figures 1 and 2) and practiced that protocol for 1 month prior to performing therapy for the study. In the control group, while not intending to restrict approaches involving trunk function, ADIM and the combination exercises were not performed. Common trunk exercises were thus acceptable.
Outcome Measures
Patient characteristics such as age, sex, side of lesion, type and onset of stroke, and comorbidities were registered. Patients were evaluated before and after the intervention. We collected durations of physical therapy and occupational therapy during the intervention, to check whether any differences existed in the amount of training. Clinical evaluations were performed by an independent assessor who was blinded to group assignment and not involved in treatment. The TIS and its subscales were the primary outcome measures to assess the effects on trunk function. Secondary outcome measures were introduced to elucidate the results of the primary outcome measures.
As the primary outcome measure, the TIS consists of 3 subscales of static and dynamic sitting balance and trunk coordination, scored up to 7, 10, and 6 points, respectively. 38 The static sitting balance subscale assesses whether a person can sit independently and remain seated when the legs are either passively or actively crossed. The dynamic sitting balance subscale evaluates the ability to actively shorten each side of the trunk, first initiated from the shoulder and subsequently initiated from the pelvic girdle. Trunk coordination tests the ability to independently rotate the shoulder girdle and pelvic girdle. Total TIS score ranges between 0 and 23 points, with a higher score indicating better trunk function. Reliability, validity, measurement error, and internal consistency of the TIS for stroke patients have been reported.11,17,39
For secondary outcome measures, selective motor ability and flexibility of the lower trunk using pelvic tilt active range of motion in the sagittal plane (pelvic AROM), comprehensive balance ability using the Balance Evaluation Systems Test–brief version (Brief-BESTest), standing stability using the Functional Reach test (FRT), performance of gait using the Timed Up-and-Go test (TUG), and level of dependency during walking using the Functional Ambulation Categories (FAC) were assessed. Pelvic AROM was the range of angles (angle between the horizontal plane and a line connecting the anterior and posterior superior iliac spines) at which the subject had been tilted between anterior and posterior to the maximum sustainable pelvis when sitting on the treatment table at a height permitting the subject to place the foot flat on the ground. Range of angle was measured on the paralyzed-side pelvis using a digital inclinometer (HORIZON; YU-KI Trading, Tokyo, Japan). Although pelvic AROM is not generally used as an evaluation method internationally, we adopted this measure as a secondary outcome because we wanted to ascertain the effect of training for core stability using a continuous variable. The Brief-BESTest 42 is an 8-item balance assessment containing 1 item from each of the 6 subsections of the BESTest. 43 The interrater reliability, internal consistency, and construct validity of the Brief-BESTest have been evaluated and noted to be high in a mixed group that included individuals with/without neurological diagnoses. 42 This text has also been confirmed as useful in patients with Parkinson’s disease. 44 In this study, the item for evaluating the left and right sides is shown as the average of right and left scores, so as not to change the ratio of the total score. Total score thus ranged from 0 to 18, with higher scores denoting better balance ability. The FRT was measured by asking the participant to reach forward with the non-paretic arm as far as possible without taking a step. The validity and reliability of the FRT have already been reported.45,46 The TUG measures the time a subject takes to stand up from an armchair at height 45 cm, walk a distance of 3 m, turn, walk back to the chair, and sit down. This tool was originally developed as a clinical measure for elderly individuals by Mathias et al 47 and later modified by Podsiadlo et al 48 for use as a short test of basic mobility skills among frail, community-dwelling, elderly individuals. TUG offers good reliability and validity in individuals who have experienced stroke. 49 FAC 50 was assessed as ranging from 0 (requiring continuous support from 2 individuals) to 5 (able to walk in- and outdoors without supervision). The reliability of the FAC score has been reported.51,52
Statistical Analysis
Descriptive data analysis was performed for the collected variables of the participants. Patient characteristics measured on a continuous scale were examined using the Shapiro-Wilk test to evaluate normal data distribution. Parametric statistics were used to analyze normally distributed data, while non-parametric comparisons were applied for variables that did not display normal distributions. To examine the effect of our randomization procedure, differences between all variables for the experimental and control groups were evaluated using an independent t test or the χ2 test for continuous or dichotomous data, respectively.
To analyze the results, a general repeated-measures model was used. Pre- and posttreatment results were entered as the within-subjects variable “time,” and the experimental and control groups were included as the between-subjects factor “condition.” Probability values for the variable time would indicate whether a significant change occurred between pre- and posttreatment assessments. A significant interaction of “time × condition” would mean that the change between pre- and posttreatment evaluation differs significantly between groups. Probability values for the TIS and its subscales were Bonferroni corrected. The significance level was set at P < .013 for the primary outcome measures. Secondary outcome measures were not corrected for multiple testing, with a significance level of P < .05. A post hoc power calculation was performed together with determination of the effect size and numbers needed to treat based on the assumption of a 10% improvement. SPSS version 22.0-J (IBM, Tokyo, Japan) and G*Power version 3.1 53 were used for statistical analyses.
Results
A total of 16 patients from the experimental group (conventional rehabilitation program including 400 minutes of core stability training over a 4-week period) and 16 patients from the control group (only conventional rehabilitation program) were included in the analysis. In the control group, one patient could not be analyzed because he had changed hospital due to recurrence of stroke during the study, while another patient who had been discharged after completing 13 of the 20 training sessions was still included in the analysis. Figure 1 shows the flow diagram for the study. No adverse events associated with either intervention were encountered.
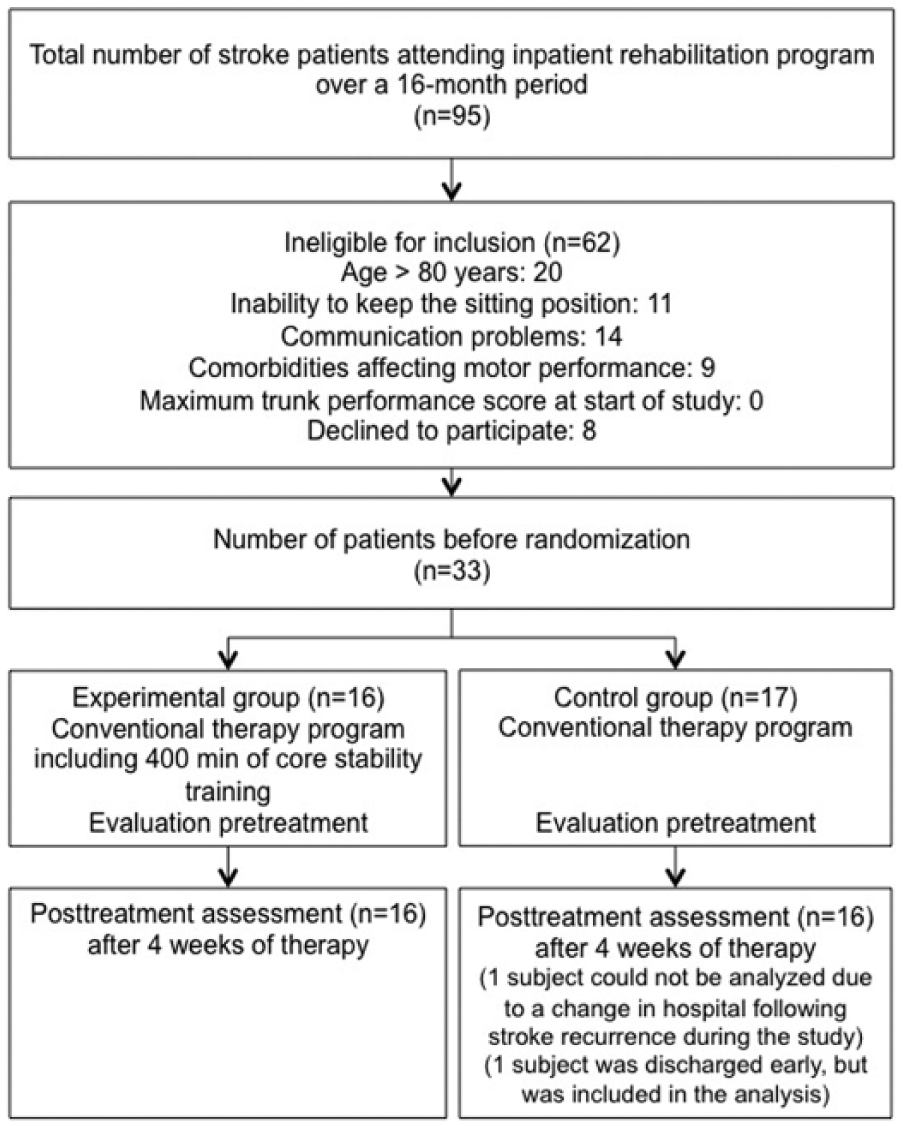
Flow diagram for subject assignment in the study. A total 16 patients were included in the experimental group and 16 patients in the control group.
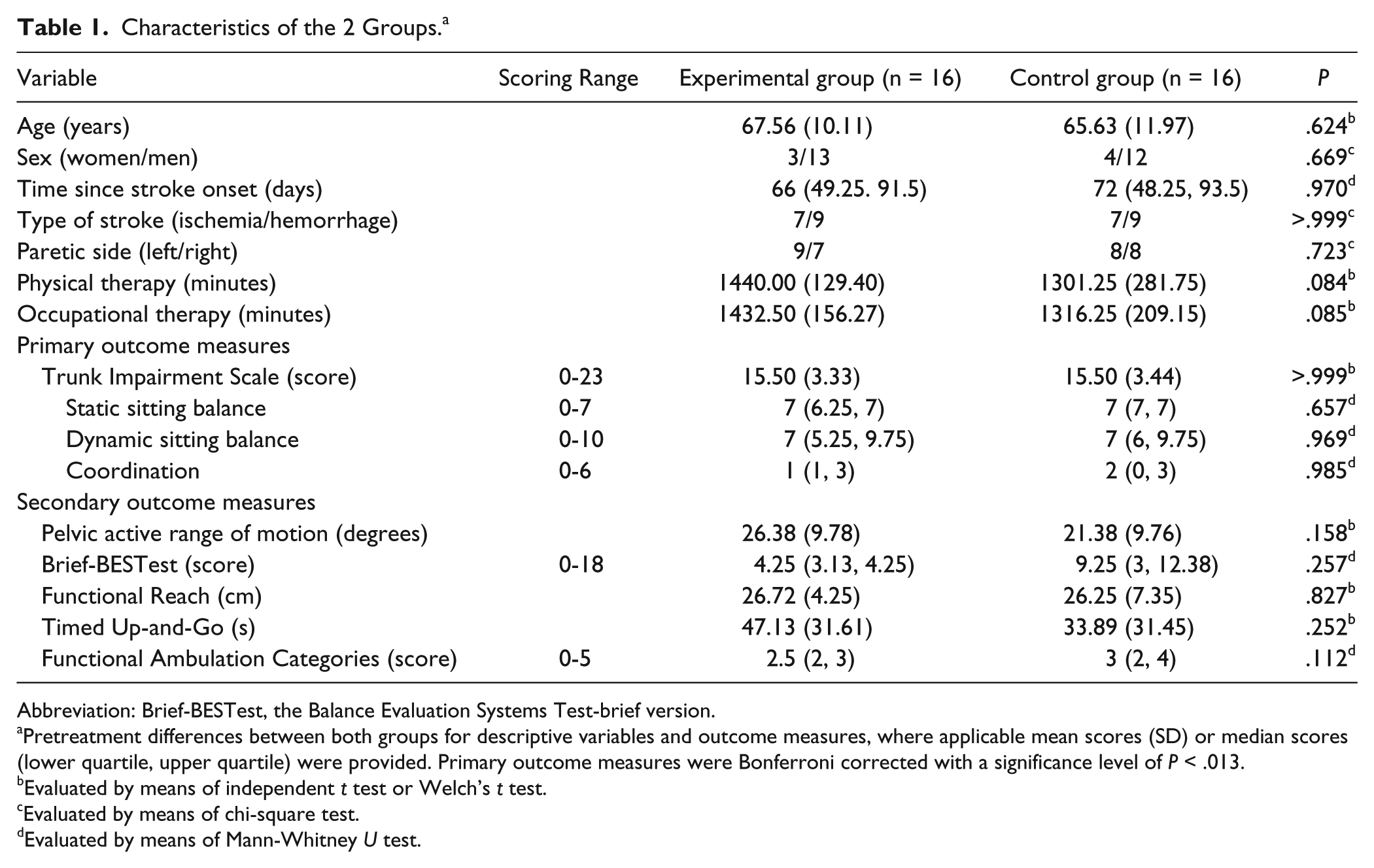
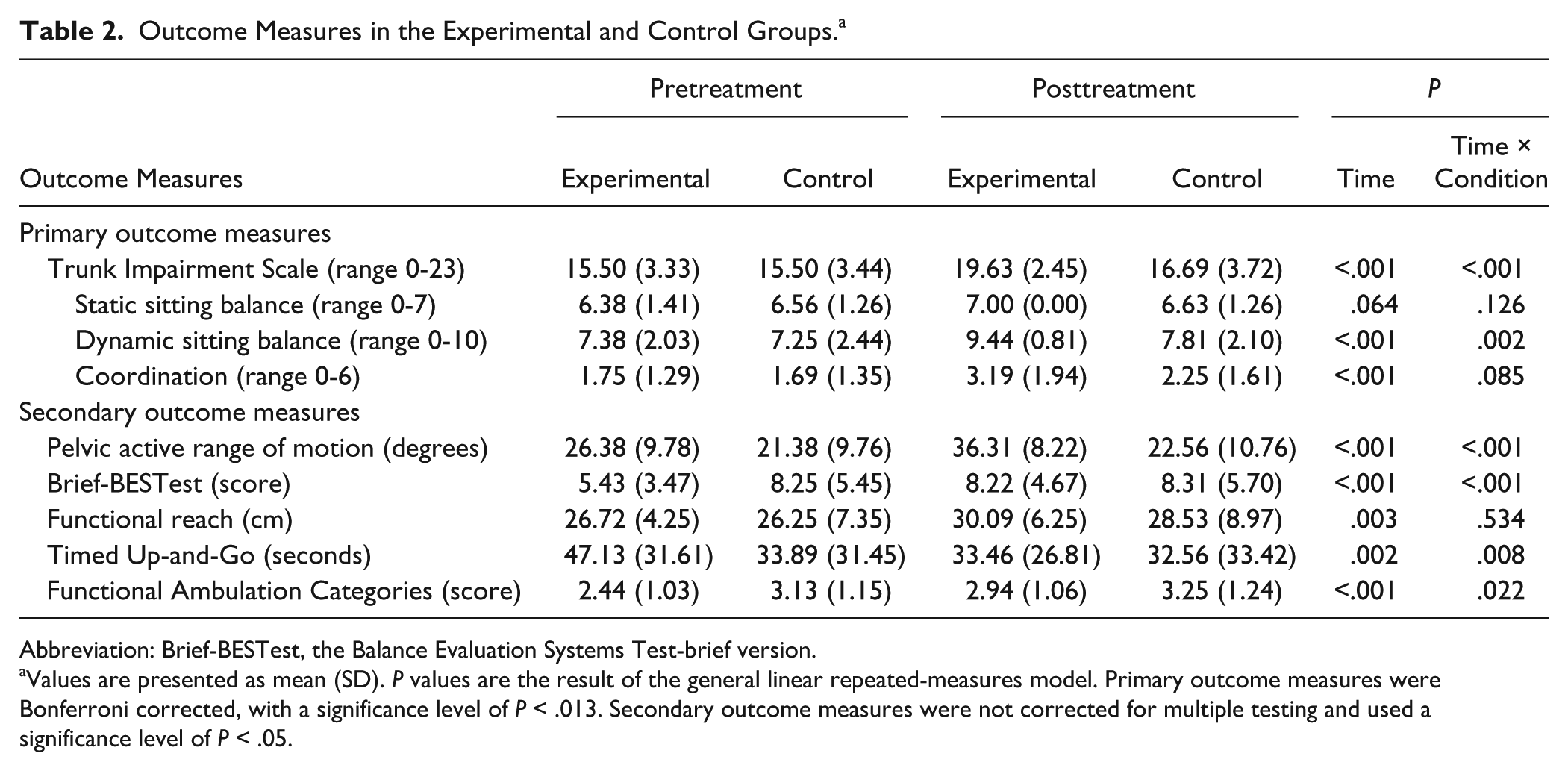
Characteristics of both groups are presented in Table 1. No significant differences were found between the 2 groups in terms of outcome measures. Both groups showed significant improvements in all outcome measures during the 4 weeks between pre- and posttreatment assessment, with the exception of the static sitting balance subscale of the TIS. The “time × condition” effect was significant for total score (P < .001) and the dynamic sitting balance subscale (P = .002) of the TIS as primary outcome measures, and pelvic AROM (P < .001), the Brief-BESTest (P < .001), TUG (P = .008), and FAC (P = .022). These results are summarized in Table 2.
Characteristics of the 2 Groups. a
Abbreviation: Brief-BESTest, the Balance Evaluation Systems Test-brief version.
Pretreatment differences between both groups for descriptive variables and outcome measures, where applicable mean scores (SD) or median scores (lower quartile, upper quartile) were provided. Primary outcome measures were Bonferroni corrected with a significance level of P < .013.
Evaluated by means of independent t test or Welch’s t test.
Evaluated by means of chi-square test.
Evaluated by means of Mann-Whitney U test.
Outcome Measures in the Experimental and Control Groups. a
Abbreviation: Brief-BESTest, the Balance Evaluation Systems Test-brief version.
Values are presented as mean (SD). P values are the result of the general linear repeated-measures model. Primary outcome measures were Bonferroni corrected, with a significance level of P < .013. Secondary outcome measures were not corrected for multiple testing and used a significance level of P < .05.
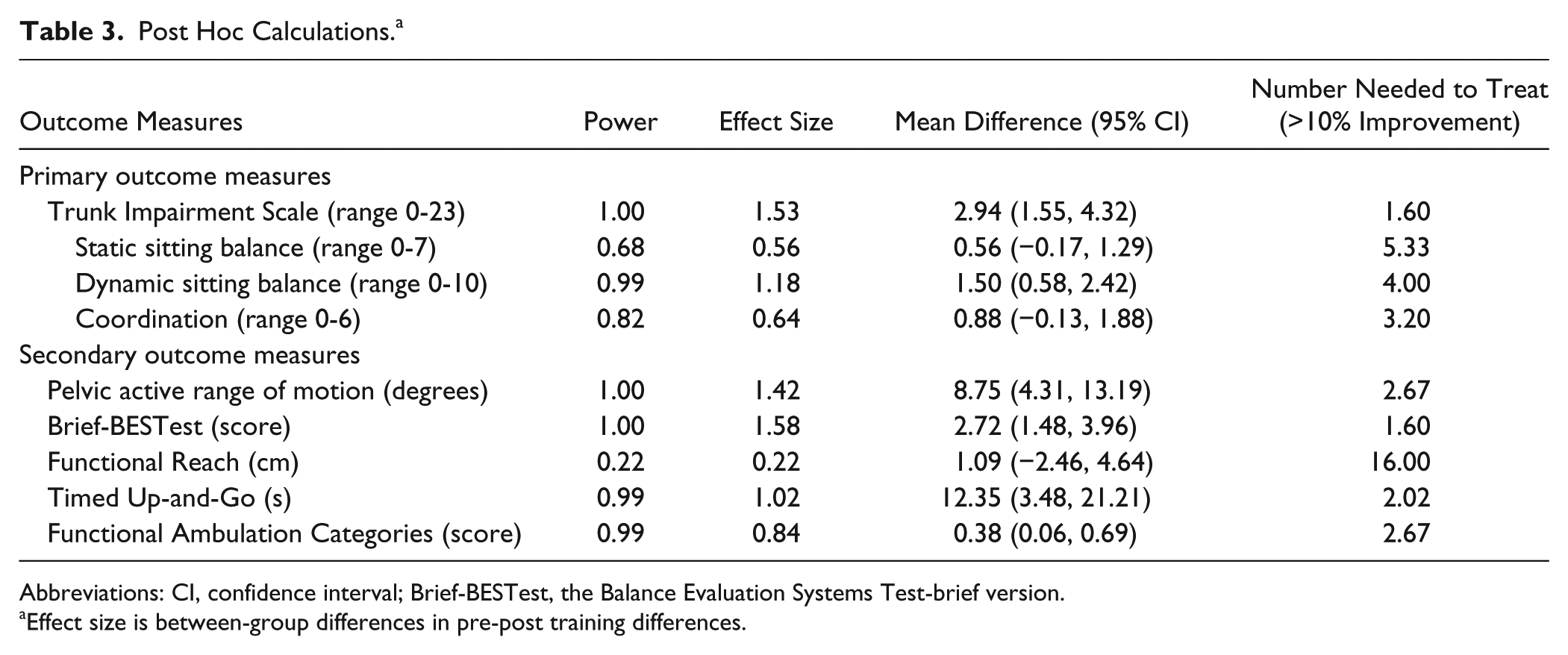
The significant “time × condition” effect showed a strong effect size (>0.80) and power greater than 0.80 (Table 3). The numbers needed to treat were small, ranging from 1.60 to 4.00, for all outcome measures with a significant “time × condition” effect.
Post Hoc Calculations. a
Abbreviations: CI, confidence interval; Brief-BESTest, the Balance Evaluation Systems Test-brief version.
Effect size is between-group differences in pre-post training differences.
Discussion
The present study showed that core stability training (ie, stepwise core stability training using selective pelvic exercises) improved balance and mobility, in addition to trunk function, more than the conventional physical therapy program in stroke patients. We found that a total of about 6.5 hours (20 min/d for 20 days) of exercises to improve core stability increased trunk performance, particularly in terms of dynamic sitting balance. In addition, the results showed that improved trunk function increased standing balance and mobility. These results offer evidence that interventions aimed at trunk muscle activation based on the core stability theory result in positive effects for patients with stroke.
Core stability training achieved similar results to the trunk training that has been previously reported, particularly for improvement of dynamic sitting balance. 18 The TIS as a primary outcome showed a significant change in total score and suggested improvements in comprehensive trunk function. Among the subscales, the lack of a difference in static sitting balance was not surprising. The static balance subscale has been pointed out to readily show a ceiling effect21,22 and low internal validity. 54 The coordination subscale showed no significant difference in treatment effect between groups in this study. Results for coordination have been inconsistent in previous research; Saeys et al 22 reported benefits for coordination, whereas Verheyden et al 21 found no improvements. Although the kinds of exercise performed in those reports were relatively similar, training time was much greater in the study by Saeys et al than in that by Verheyden et al. The amount of training in our study might have been insufficient to improve coordination. In addition, one report suggests that the subscales of the TIS are hierarchical. 55 That report stated that static sitting balance appeared easier to improve than dynamic sitting balance, which in turn was easier to improve than coordination. Such a hierarchy may explain why our study did not demonstrate beneficial effects for the experimental group compared to the control group for coordination.
In our results, core stability training also improved standing balance and mobility. Van Nes et al 56 reported that lateral trunk control might be a primary target for rehabilitation, since lateral balance was more affected by stroke than balance in the anteroposterior direction, and showed the strongest association with the Berg Balance Scale. Improvement of the dynamic sitting balance subscale was seen to reflect lateral trunk control in this study, resulting in improved balance and mobility despite not performing a specific exercise. Improvement of mobility, which is described in the TUG, was confirmed in our study. Furthermore, differences in the level of improvement of functional ambulation level were seen between groups, demonstrating the effect of improvements in trunk function on gait ability. However, the tendency toward a difference in TUG scores at the baseline evaluation between groups may warrant consideration, although no significant difference was present. Participants in this study showed slow TUG times compared with some previous reports.57,58 Because participants in this study had been admitted for rehabilitation in the subacute phase, a relatively high proportion may have shown severe gait disorder. Although greater improvement was shown in the experimental group, the effect of core stability training for mobility should only be generalized with caution.
We also found improvements in pelvic AROM angle. Core stability training, including pelvic control exercises enhanced the voluntary range of motion of the pelvis in the sagittal plane, and improved lumbo-pelvic flexibility was suggested. In a report by O’Sullivan et al, 59 upright posture of the pelvis was considered to result in greater activation of local muscles in healthy individuals. Because core stability training likewise activates local core muscles, pelvic exercises with core stabilization might prove more effective than either form in isolation.
Improvement of the TIS seen in this study is not surprising given the results of previous studies. 18 We think it is important that balance and mobility as secondary outcomes were improved in addition to trunk function. This shows similar results to Saeys et al 22 with comprehensive trunk exercise and their larger intervention in terms of the amount of training. In addition, Cabanas-Valdés et al 20 also showed a positive effect of comprehensive trunk exercises in raising stepwise difficulty from a stable surface to an unstable surface using a comparable intervention time to the present study. Compared with their comprehensive trunk exercise intervention, the training protocol in the present study was focused on core stability exercises to clarify the effect of trunk exercise. The training protocol in this study used only localized exercises and their combinations, mainly based on activation of deep trunk muscle. Features of our training protocol were as follows: (1) a progressive program, (2) use of an upright sitting position, and (3) integration of core local muscles and global muscles. Given the results showing positive effects of a definite protocol, clinicians might be able to easily plan trunk exercises for stroke patients.
Activities of the deep abdominal muscles (ie, TrA and obliquus internus muscles) remain intact in stroke hemiplegia. 38 Stroke patients can thus achieve co-contraction of the global muscles of the trunk while the core is activated. As for the intervention in this study, we set the program based on the basic strategy of improving core stability through the activation of local core muscles. Consequently, we found that the trunk stabilization achieved through core stability training improved balance and mobility. This result was consistent with the report on the intervention effect of core stability improvement by Cabanas-Valdés et al. 20 However, their core stability training comprised selective trunk or pelvic movement exercises, bridge exercises, and reaching exercises, and exercises of the local core muscles were not emphasized in contrast to our protocol. Although they confirmed an intervention effect using core stability training as additional training, our protocol based on the activation of the local muscles of the core showed positive effects without additional training. We thus emphasize that activation of core muscles is essential in trunk exercises for stroke rehabilitation.
Recent research has observed the effect of progressive programs, 60 and has shown their utility in core stability exercises. 20 We therefore made an original progressive protocol for core stability exercises. As for the content of the protocol, we selected a few particular types of training because we wanted to make a more focused protocol than previous studies.20-22 Additionally, most training was carried out in an upright sitting position. Core stability training in an upright, anti-gravity position is more effective than that in a lying position61,62 and was safe and easy to implement in a clinical setting. Furthermore, we emphasized the integration of local core muscles and global muscles as a process of core stability training (see Table 1, selective pelvic exercises with ADIM).29,36 In healthy subjects, a combination of ADIM and exercise of global muscles has shown increased activation of the TrA. 63 Pelvic exercises result in the increased recruitment of global muscles as the movement system.31,64-66 We therefore combined ADIM exercise and selective pelvic control exercises. The training protocol in this study started from ADIM in supine and antigravity positions, pelvic control exercises, and synchronization of both exercises in a step-by-step manner. As efficacy was achieved in less intervention time than applied in other studies, the effectiveness of our protocol is suggested.
Some limitations warrant caution when interpreting the results of our study. This investigation involved a relatively small number of subjects from a single center. The findings of this study must therefore be generalized with caution. Additionally, the lack of quantitative assessment of the success of core stability training and nonblinding of the patient and therapist were less than ideal. Outcomes of the present study were determined from impairment/function level, and the effects of core stability training on ADL and quality of life remain unclear. Furthermore, no follow-up assessments were performed. As future research, comparison between groups with the same amount of core stability training and general trunk exercise is needed to examine the effectiveness of core stability theory more precisely.
Conclusions
Our findings provide support for introducing core stability training to address trunk dysfunction in stroke patients. Core stability training based on a graded protocol was found to be beneficial to balance and mobility measures, as well as trunk performance. Future research is needed to clarify the effects on functional activities once training has proceeded to advanced strategies for achieving stability.
Footnotes
Acknowledgements
We wish to thank Takaharu Kondo, Toru Tanaka, and Katsumi Shimizu for their assistance with this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.