
Abstract
Background. Perinatal stroke is the leading cause of hemiparetic cerebral palsy. Motor deficits and their treatment are commonly emphasized in the literature. Sensory dysfunction may be an important contributor to disability, but it is difficult to measure accurately clinically. Objective. Use robotics to quantify position sense deficits in hemiparetic children with perinatal stroke and determine their association with common clinical measures. Methods. Case-control study. Participants were children aged 6 to 19 years with magnetic resonance imaging–confirmed unilateral perinatal arterial ischemic stroke or periventricular venous infarction and symptomatic hemiparetic cerebral palsy. Participants completed a position matching task using an exoskeleton robotic device (KINARM). Position matching variability, shift, and expansion/contraction area were measured with and without vision. Robotic outcomes were compared across stroke groups and controls and to clinical measures of disability (Assisting Hand Assessment) and sensory function. Results. Forty stroke participants (22 arterial, 18 venous, median age 12 years, 43% female) were compared with 60 healthy controls. Position sense variability was impaired in arterial (6.01 ± 1.8 cm) and venous (5.42 ± 1.8 cm) stroke compared to controls (3.54 ± 0.9 cm, P < .001) with vision occluded. Impairment remained when vision was restored. Robotic measures correlated with functional disability. Sensitivity and specificity of clinical sensory tests were modest. Conclusions. Robotic assessment of position sense is feasible in children with perinatal stroke. Impairment is common and worse in arterial lesions. Limited correction with vision suggests cortical sensory network dysfunction. Disordered position sense may represent a therapeutic target in hemiparetic cerebral palsy.
Introduction
The perinatal timeframe carries high risk for ischemic stroke, occurring in >1:2500 live births. 1 Modern neuroimaging has defined specific perinatal stroke diseases. 2 Arterial ischemic strokes (AIS) are usually large, middle cerebral artery occlusions resulting in cortical and subcortical injuries acquired near birth. In contrast, periventricular venous infarctions (PVI) are smaller, subcortical white matter lesions acquired in utero. Both injuries damage components of the sensorimotor system. As a focal injury of defined timing in an otherwise healthy brain, perinatal stroke represents an ideal human model of developmental plasticity. 3
Cerebral palsy (CP) is a syndrome of nonprogressive impairment of motor development secondary to perinatal brain disease and accounts for most lifelong physical disability. 4 Perinatal stroke causes most hemiparetic CP. The majority of perinatal stroke survivors suffer functional motor impairments. 5 Sensory dysfunction may also be a common contributor to CP disability but studies have been limited by heterogeneous populations and a lack of accurate outcome measures.6,7
Proprioception utilizes input from muscle, joint, and cutaneous afferent fibers to accurately perceive the perception of position, motion, and force generated by the body.8,9 Individuals with proprioceptive loss but intact motor functions can exhibit marked deficits in movement control.10,11 One component of proprioception is position sense, 12 the ability to accurately identify the static position of the limb. Dysfunction in position sense in adults with stroke has been shown to negatively affect safety, postural stability, and motor function.13-15 In one study, 50% of adult stroke survivors presented with some degree of position sense impairment, demonstrating that sensory dysfunction is common. 8 Studies of position sense in children with CP have been limited,6,16 the major barrier being a lack of objective measurement tools.
Robotic technologies have revolutionized the quantification of sensorimotor function including limb position sense. 8 The kinesiological instrument for normal and altered reaching movements (KINARM) robot provides reliable and objective quantification of position sense and visuomotor function. 17 KINARM applications in adult stroke are well established8,17-20 where detailed measures of position sense dysfunction have been correlated with clinical outcomes and disability.8,18 Despite this utility, such measures have not been applied to the disabilities of children with perinatal stroke and CP.
We performed a case-control study to quantify position sense in children with hemiparetic CP secondary to perinatal stroke. We hypothesized that children with perinatal stroke would show impairments in position sense compared to healthy controls with greater dysfunction in AIS compared to PVI lesions.
Methods
Participants
Participants were recruited from the Alberta Perinatal Stroke Project, a population-based research cohort based at the Alberta Children’s Hospital (Calgary, Canada). Inclusion criteria were the following: (a) age 6 to 19 years; (b) magnetic resonance imaging–confirmed unilateral perinatal stroke (AIS, PVI) according to validated criteria 2 ; (c) clinical confirmation of symptomatic, disabling hemiparetic CP (Pediatric Stroke Outcome Measure [PSOM] ≥0.5 and Manual Abilities Classification System [MACS] grade I-IV), and child/parent perceived functional limitations; (d) term birth (≥36 weeks); and (e) written informed consent/assent. Participants with any of the following were excluded: (a) multifocal stroke; (b) severe hemiparesis (MACS grade V); (c) severe upper limb spasticity (Modified Ashworth Scale = 4) or contracture; (d) additional neurological condition not attributable to stroke; (e) developmental disability precluding compliance with study procedures; or (f) botulinum toxin or upper limb surgery within the previous 6 months. Typically developing controls within the same age range recruited from the community underwent identical evaluations. Methods were approved by the institutional research ethics board.
Robotic Assessment
Assessments were performed at the Foothills Medical Centre Stroke Robotics Laboratory. A KINARM exoskeleton robotic device (BKIN Technologies Ltd, Kingston, Ontario) assessed position sense as described previously in adults including those with stroke-induced hemiparesis. 8 Participants sat in a modified wheelchair base with each arm supported by the robotic exoskeleton fitted to each individual. 18 The robotic device permits movement of the arms in the horizontal plane while monitoring shoulder and elbow joint motion. For smaller children, 2 simple modifications were made by adding risers to the arm troughs and a booster seat with added foam padding to achieve comparable upper limb positioning (Figure 1A).
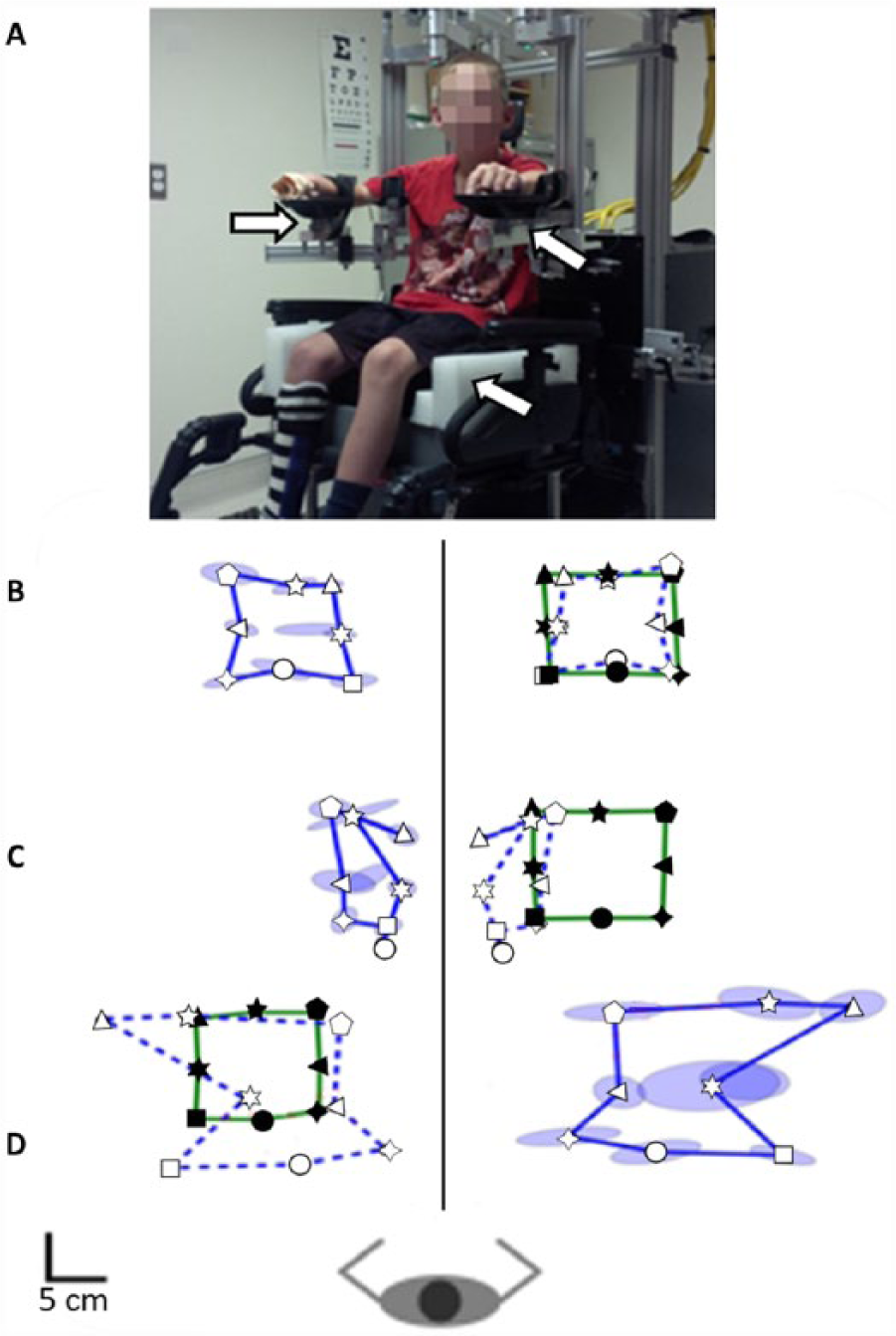
KINARM robot for children and performance outcomes of the position matching task. (A) Frontal view of the robotic apparatus with its modified wheelchair base and exoskeleton arms. Pediatric modifications (risers, booster seat, foam padding) are shown (white arrows). Closed symbols represent the different positions where the robot moved the passive arm. Solid green lines represent the border of the outer 8 targets. Open symbols represent where the subject mirror matched with the active arm. Solid blue lines represent the border of the outer 8 targets for the active arm. Ellipses around targets demonstrate variability of successive matching attempts and represent 1 standard deviation. For display, we have mirrored the subject’s active arm performance on top of the robotically moved arm using open symbols and outlining the outer target locations with a blue dashed line. (B) In a healthy control, the robot moved the right arm and they matched with their left. The subject displays little variability and is highly accurate in their matching. (C) A participant with AIS (arterial ischemic stroke) shows contraction of the workspace, increased variability, spatial shift to the left, and inability to match the overall square shape pattern of passive arm movement. (D) A participant PVI (periventricular venous infarction) demonstrates marked increased variability and an expansion of the workspace.
Arm-Position Matching Task
This task has been validated as a measure of the static awareness of limb position. 8 The child sat comfortably with both arms held in position with elbows flexed. The robot then moved the stroke affected arm (passive arm) to 1 of 9 spatial targets each separated by 6 cm. Once the robot stopped moving, the child was verbally instructed to mirror-match the position with their opposite arm (active arm). Each participant completed a total of 6 blocks of trials in which the order of the 9 targets was pseudo-randomized for 54 total movements. The position matching task was completed twice: first with the vision of the upper extremities occluded and again with vision of the arms restored. Three parameters quantified position sense as previously described (Figure 1) 8 :
Variability (Varxy): Endpoint variability of the matched location of the active arm measured in centimeters.
Contraction/expansion (Areaxy): Perceived workspace area measured bidirectionally from normal (values <1 indicate contraction).
Systematic shift (Shiftxy): Perceived spatial translation of the workspace measured in centimeters.
Clinical Assessment
Clinical Sensory Testing
A series of common clinical tests of sensory function were performed in standardized fashion by the same experienced therapist at the beginning of each session.
Thumb and wrist position sense. With vision occluded, the therapist moved the participant’s wrist up and down at 1 Hz 3 times and asked them to identify the direction of the end wrist position. The same assessment was repeated with the thumb. Outcomes were dichotomized as unable (0) or able (1) to identify position.
Thumb localization task (TLT). The participant was asked to locate the thumb on their affected arm (nondominant arm for controls) with the opposite hand. 21 With the eyes blindfolded, the therapist moved and positioned the participant’s upper limb lateral to the midline and asked the participant to pinch the thumb of that limb with their opposite thumb and index finger. 21 The task was scored on a 4-point scale from 0 (no difficulty locating) to 3 (unable to locate). Outcomes were dichotomized as normal (score = 0) or impaired (score > 0).
Stereognosis. Standardized objects (nickel, key, paperclip) were sequentially placed in the palm bilaterally, beginning with the affected hand in stroke participants with vision occluded. The participant was then asked to verbally identify the object and scored either 0 (unable to identify), 0.5 (identified category but not object), or 1 (able to identify). Failure was defined by a score of 0 for 2 or more objects.
Graphesthesia. The therapist “drew” a 3, 5, or 7 in the participant’s palm with vision occluded and asked them to identify the number. Scores were 0 (unable to identify) or 1 (able to identify). This task was done bilaterally with the stroke/nondominant hand tested first. Failure was a score of 0 for 2 or more numbers.
Functional Measures
Participants underwent a standardized clinical assessment including the following:
Assisting Hand Assessment (AHA) is the evidence-based standard for bimanual upper extremity function in children with hemiparetic CP. 22 Scores are expressed as AHA logit units.
Chedoke-McMaster Stroke Assessment (CMSA) for upper extremity motor recovery is scaled from a range of 1 (flaccid paralysis) to 7 (normal movement). 23
Purdue pegboard (PPB) measured hand dexterity bilaterally (LaFayette Instrument Co, Lafayette, IN). Participants were required to pick up one peg at a time and successively fill a sequence of peg holes as quickly and accurately as possible in 30 seconds. Participants repeated this test twice and the outcome was the best score (total number of pegs placed in 30 seconds). 24
CP functional classifications: MACS.
Modified Edinburgh Handedness Inventory used a 10-item version to determine relative hand dominance. 25
Visual acuity was assessed using a Snellen eye chart to ensure a minimum of 20/30 binocular acuity. Visual fields were assessed using simple confrontation.
Behavioral Inattention Test (BIT) was employed as an objective screen for visuospatial neglect. 26 The 6 conventional subtests of the BIT were collected for a total possible score of 146. BIT scores <130 indicated neglect.
Analysis
Kolmogorov-Smirnov tests determined data distribution. In the primary analysis, Varxy was compared across stroke groups (AIS, PVI) and controls using one-way ANOVA with Tukey’s post hoc test. Wilcoxon rank sum or paired t tests compared between vision conditions within each group. Proportions falling outside the normal 95% range of control performance were compared across position matching outcomes and stroke type (χ2). As the Areaxy parameter measures both expansion and contraction, reciprocal values were used for the analyses mentioned above. To examine associations between robotic position sense and clinical function measures, Spearman’s correlation (continuous) or ANOVA (dichotomized measures) were employed. Varxy was used as the gold standard to calculate the sensitivity, specificity, and predictive values of each clinical test.
Sample size was estimated on the primary hypothesis that position matching variability (Varxy) would be increased in stroke participants. Typical mean values of 4.0 cm in adult controls and 6.0 cm in adult stroke participants with a standard deviation of 1.7 for an effect size of 20% between controls, AIS, and PVI (ANOVA) with power of 90% and type 1 error of 0.05 estimated a sample size of 12 per group (N = 36). Statistical analyses were performed using SigmaPlot (Systat Software Inc, San Jose, CA) and SPSS (IBM, Armonk, NY).
Results
Robotic Outcomes
All robotic measures were obtained on a total of 100 participants (N = 22 AIS, N = 18 PVI, N = 60 controls). All 3 groups were comparable with respect to age and sex (Table 1). Examples of position matching performance are depicted in Figure 1. No correlation between age or sex and position sense outcomes was observed but age distributions are demonstrated in the figures below.
Subject Characteristics and Clinical Details a .
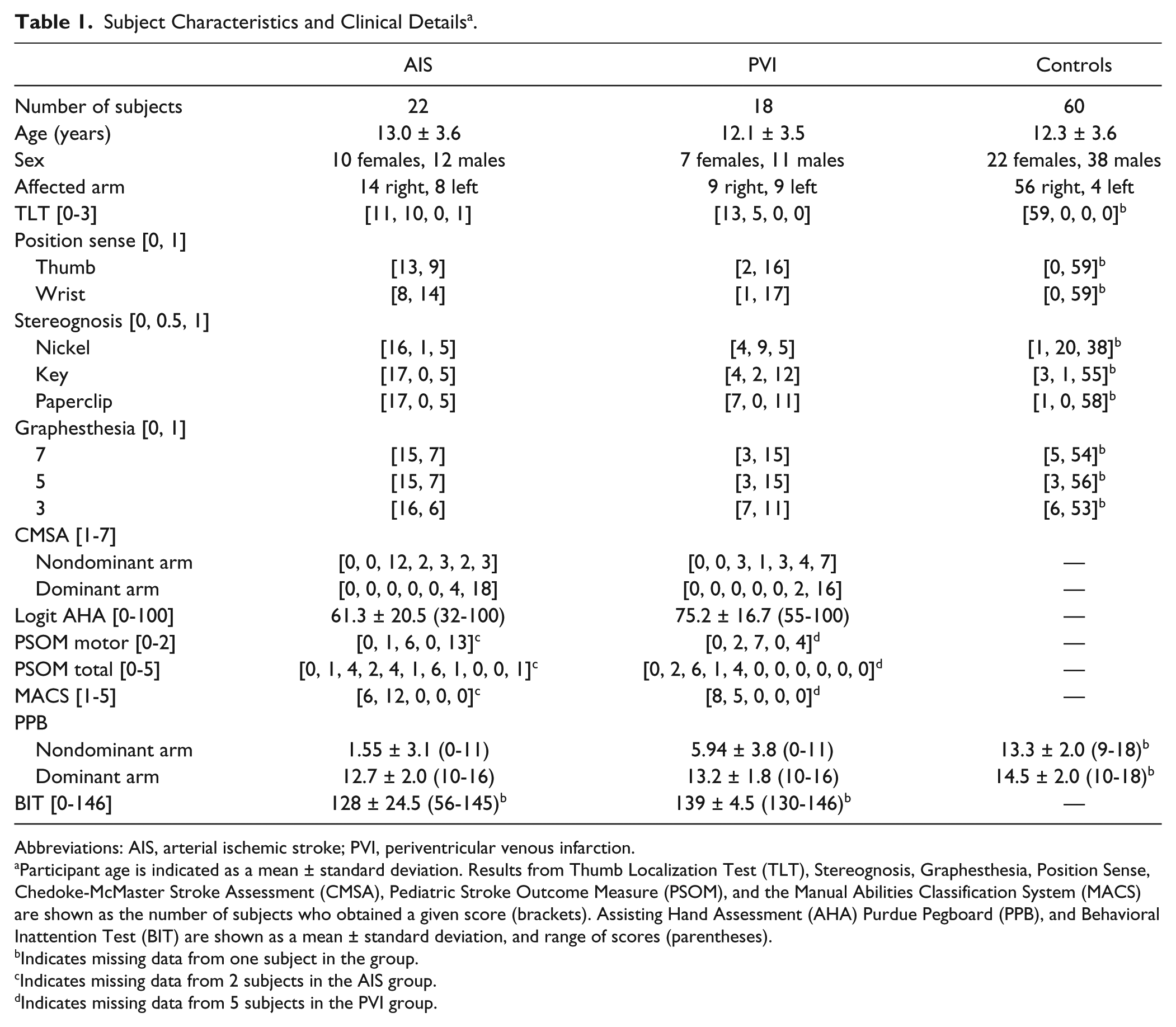
Abbreviations: AIS, arterial ischemic stroke; PVI, periventricular venous infarction.
Participant age is indicated as a mean ± standard deviation. Results from Thumb Localization Test (TLT), Stereognosis, Graphesthesia, Position Sense, Chedoke-McMaster Stroke Assessment (CMSA), Pediatric Stroke Outcome Measure (PSOM), and the Manual Abilities Classification System (MACS) are shown as the number of subjects who obtained a given score (brackets). Assisting Hand Assessment (AHA) Purdue Pegboard (PPB), and Behavioral Inattention Test (BIT) are shown as a mean ± standard deviation, and range of scores (parentheses).
Indicates missing data from one subject in the group.
Indicates missing data from 2 subjects in the AIS group.
Indicates missing data from 5 subjects in the PVI group.
Variability XY
Compared with controls, stroke participants demonstrated increased variability (Figure 2A). With vision occluded, the AIS group demonstrated greater Varxy than controls (6.01 ± 1.8 cm vs 3.54 ± 0.9cm, F[2, 97] = 33.8, P < .001). The PVI group also demonstrated greater Varxy (5.42 ± 1.8 cm, F[2, 97] = 33.8, P < .001). Fifteen (68%) AIS and 9 (50%) PVI participants fell outside the normal range on Varxy with vision occluded (Figure 2B).
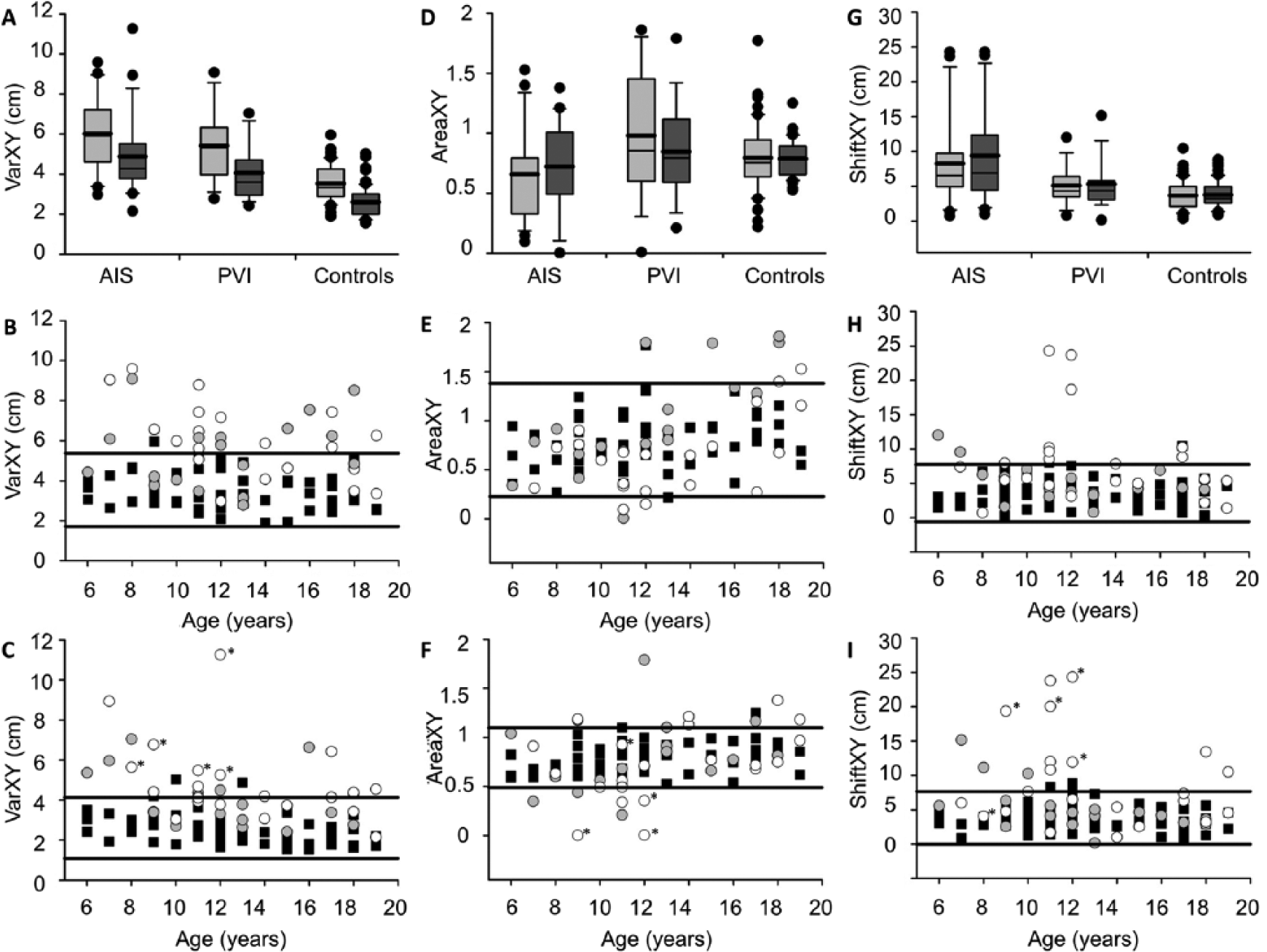
KINARM robot position matching performance across stroke and control groups. Boxplots of each parameter (top row) are shown for each of the 3 groups with vision removed (light bars) and vision restored (dark bars). Scatter plots without (middle row) and with (bottom row) vision show the performance in each parameter for stroke cases (AIS [arterial ischemic stroke] filled circles, PVI [periventricular venous infarction] open circles) and controls (filled squares) with 95% ranges of control performance defining normal boundaries (horizontal lines). Both AIS and PVI groups demonstrate increased Varxy (A) and Shiftxy (G) relative to controls. All scores improved with vision restoration but both stroke groups remained abnormal. Stroke cases demonstrated consistently greater Varxy (B, C) and Shiftxy (H, I) across all ages (x-axis). AIS and PVI groups were more likely to fall beyond the normal range of Areaxy in the vision restored condition (F). AIS participants with BIT scores <130 indicating visuospatial neglect are starred (C, F, I).
Mean Varxy decreased in all 3 groups when vision was restored: AIS (−11.2%, Z = −2.9, P < .01), PVI (−13.8%, t[17] = 4.0, P < .001), and control (−15.5%, t[59] = 8.3, P < .001). The degree of improvement did not differ between groups (F[2, 97] = 0.6, P = .6). With vision, Varxy was greater in AIS than controls (4.89 ± 2.0 cm vs 2.61 ± 0.8 cm, F[2, 97] = 29.6, P < .001). Varxy was also increased in PVI with vision (4.06 ± 1.4 cm, F[2, 97] = 29.6, P < .001). Varxy did not differ between AIS and PVI in the no vision (F[2, 96] = 32.2, P = .3) or vision (F[2, 97] = 0.7, P = .1) conditions. When vision was restored, 11 (50%) AIS and 7 (39%) PVI participants fell outside the normal range (Figure 2C).
Area XY
No differences in Areaxy were observed within or between the 3 groups with or without vision (Figure 2D). However, 4 (18%) AIS and 5 (28%) PVI participants fell outside the normal range on Areaxy without vision (Figure 2E). When vision of the upper extremities was restored, 9 (41%) AIS and 7 (39%) PVI participants fell outside the normal range on Areaxy (Figure 2F).
Shift XY
Compared to controls, stroke participants demonstrated increased spatial shift (Figure 2G). The AIS group (8.27 ± 6.3 cm) demonstrated larger shift of the workspace than controls (3.69 ± 2.0 cm) with vision occluded (F[2, 97] = 13.6, P < .001). Compared to PVI (5.13 ± 2.7 cm), AIS participants exhibited larger shift with vision occluded (F[2, 97] = 13.6, P < 0.05). Nine (41%) AIS and 3 (17%) PVI participants fell outside the normal range on Shiftxy when vision was occluded (Figure 2H).
When vision of the upper extremities was restored (Figure 2I), the AIS group (9.42 ± 7.0 cm) still displayed increased Shiftxy compared to controls (3.79 ± 1.9 cm, F[2, 97] = 17.1, P < .001) and PVI (5.34 ± 3.6 cm, F[2, 97] = 17.1, P < .01). Shiftxy in the PVI group did not differ from controls in neither the no vision (F[2, 97] = 13.6, P = .3) or vision (F[2, 97] = 17.1, P = .3) conditions. No differences were found when comparing Shiftxy or the percent change in Shiftxy between the 2 vision conditions within each group. With the restoration of vision, 9 (41%) AIS and 3 (17%) PVI participants fell outside the normal range on Shiftxy (P = .1).
Clinical Measures of Sensorimotor Function
Clinical Functional Outcomes
Mean logit AHA scores were lower in AIS (61.3 ± 20.5) than PVI (75.2 ± 16.7), t[31] = −2.04, P < .05. AHA scores were inversely correlated with Varxy (no vision) in AIS (ρ = −0.64, P < .01) but not PVI (ρ = 0.12, P = .7; Figure 3). AHA scores correlated with Shiftxy (vision) in AIS (ρ = −0.49, P < .05) but not PVI (ρ = 0.20, P = .5). Fine motor function as determined by the PPB was inversely correlated with both Varxy (ρ = −0.51, P < .01) and Shiftxy (ρ = −0.52, P < .01) in AIS but not PVI or controls. CMSA scores were lower in AIS compared to PVI (U = 95.5, P < .01; Table 1). Five AIS participants had BIT scores <130 consistent with visuospatial neglect and this was associated with poor position matching task performance including increased Varxy without (t[20] = 2.5, P < .05) and with (U = 7.0, P < .01) vision. BIT scores correlated with Varxy (no vision) in AIS (ρ = −0.54, P = .01) but not PVI (ρ = −0.068, P = .8). Conversely, BIT scores were correlated with Varxy (vision) in PVI (ρ = −0.49, P < .05) but not AIS (ρ = −0.31, P = .2).
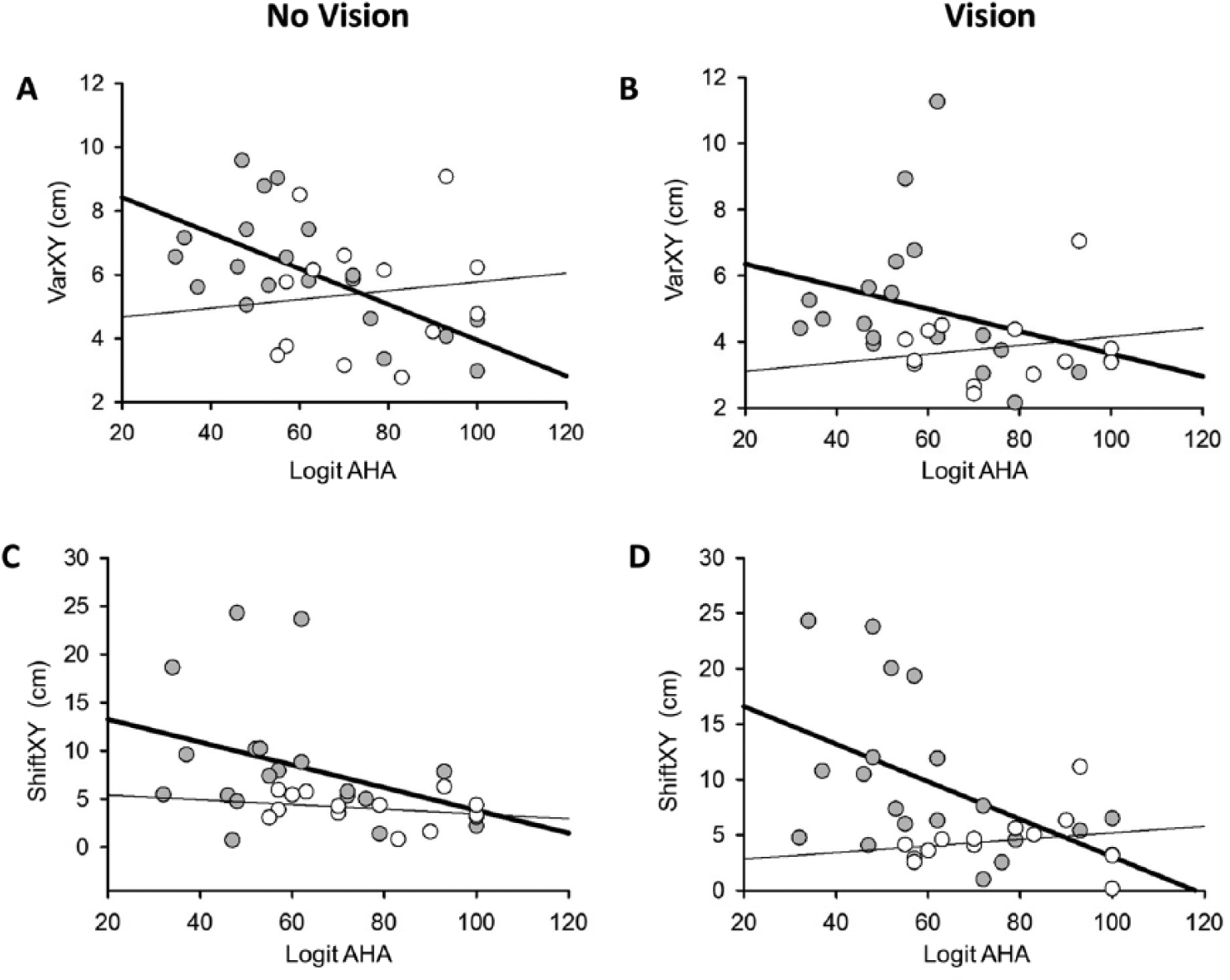
Position matching outcomes and their association with clinical logit based Assisting Hand Assessment (AHA) scores in arterial ischemic stroke (AIS; filled circles, bold regression line) and periventricular venous infarction (PVI; open circles, thin regression line). (A) Robotic Varxy (no vision condition) correlated with AHA in the AIS group (ρ = −0.64, P < .01) but not PVI (ρ = 0.12, P = .7). (B) Robotic Varxy (vision condition) was not correlated with AHA in AIS (ρ = −0.33, P = .2) or PVI (ρ = 0.19, P = .5). (C) Robotic Shiftxy (no vision condition) was not correlated with AHA in AIS (ρ = −0.37, P = .1) or PVI (ρ = −0.25, P = .4). (D) Robotic Shiftxy (vision condition) correlated with AHA in AIS (ρ = −0.49, P < .05) but not PVI (ρ = 0.20, P = .5).
Clinical Position Sense
Impaired thumb localization was associated with AIS where 11 (50%) failed compared to zero controls (χ2[1] = 34.1, P < .001). Varxy was associated with TLT performance in AIS (χ2[1] = 5.2, P < .05) where 10/11 with clinical impairment had abnormally high Varxy. Six AIS participants had normal TLT scores and Varxy and 5 had abnormal Varxy but normal TLT (P < .01). Mean Varxy was larger in AIS participants failing the TLT (6.80 ± 1.7 cm vs 3.62 ± 0.6 cm, U = 0.0, P < .001).
Impaired thumb localization was also associated with PVI where 5 (28%) failed compared to zero controls (χ2[1] = 17.5, P < .001). Varxy was not associated with thumb localization in PVI (χ2[1] = 2.5, P = .1) where only 1/5 failing the test had abnormal Varxy. Five PVI participants had normal TLT and Varxy, 8 with abnormal Varxy passed the TLT, and 4 with normal Varxy failed the TLT. Mean Varxy did not differ between PVI participants passing and failing thumb localization (4.02 ± 1.4 cm vs 4.18 ± 1.4 cm, U = 28.0, P = .7).
Impaired clinical position sense (thumb and wrist) was associated with AIS where 14 (64%) failed compared to zero controls (χ2[1] = 45.4, P < .001). Eleven of 14 AIS participants failing the clinical position sense test had abnormally high Varxy. Mean Varxy scores in the AIS group did not differ between passing and failing clinical position sense (4.24 ± 1.4 cm vs 5.26 ± 2.3 cm, U = 43.0, P = .4). Clinical position sense was impaired in 2 (11%) PVI participants compared to zero controls (χ2[1] = 6.7, P = .01) and was not associated with Varxy in PVI (χ2[1] = 2.3, P = .10). Mean Varxy scores in PVI participants did not differ between passing and failing clinical position sense (4.09 ± 1.5 cm vs 3.83 ± 0.7 cm), t[16] = 0.3, P = 0.8.
Clinical Cortical Sensation
Stereognosis was impaired in 17 (77%) AIS participants compared to zero controls (χ2[1] = 57.7, P < .001). Varxy was associated with clinical stereognosis in AIS (χ2[1] = 6.9, P < .01) where 14 exhibited both abnormal robotic Varxy and abnormal stereognosis. One participant displayed normal stereognosis but abnormal Varxy while 3 had normal Varxy but impaired stereognosis. Mean Varxy in AIS participants was larger in those failing stereognosis (5.34 ± 2.1 cm vs 3.37 ± 0.8 cm, U = 12.0, P < .05). Stereognosis was impaired in 5 (28%) PVI participants compared to zero controls (χ2[1] = 17.5, P < .001). However, Varxy was not associated with clinical stereognosis (χ2[1] = 0.3, P = .6). Mean Varxy scores in PVI participants did not differ between passing and failing stereognosis (3.96 ± 1.3 cm vs 4.34 ± 1.6 cm, U = 25.0, P = .5).
Graphesthesia was impaired in 16 (73%) AIS participants compared to 4 controls (age 6-9; χ2[1] = 37.5, P < .001). Robotic Varxy was associated with graphesthesia in AIS (χ2[1] = 4.6, P < .05) including 13 with abnormally large Varxy and impaired graphesthesia. Mean Varxy scores in AIS participants were larger in those that failed graphesthesia (5.39 ± 2.1 cm vs 3.55 ± 0.9 cm, U = 19.0, P < .05). Graphesthesia impairment was not associated with PVI (χ2[1] = 1.6, P = .2) nor with Varxy (χ2[1] = 0.4, P = .5). Mean Varxy scores did not differ between passing and failing graphesthesia in the PVI group (3.89 ± 1.4 cm vs 4.92 ± 1.3 cm, U = 11.0, P = .2).
The sensitivity, specificity, and predictive values of each clinical sensory test are summarized in Table 2. Clinical sensory tests designed for position sense performed without vision were the most sensitive including thumb (0.85) and wrist (0.88) position sense.
Sensitivity, specificity, and predictive values of clinical bedside tests compared to robotic variability for all children with stroke. a
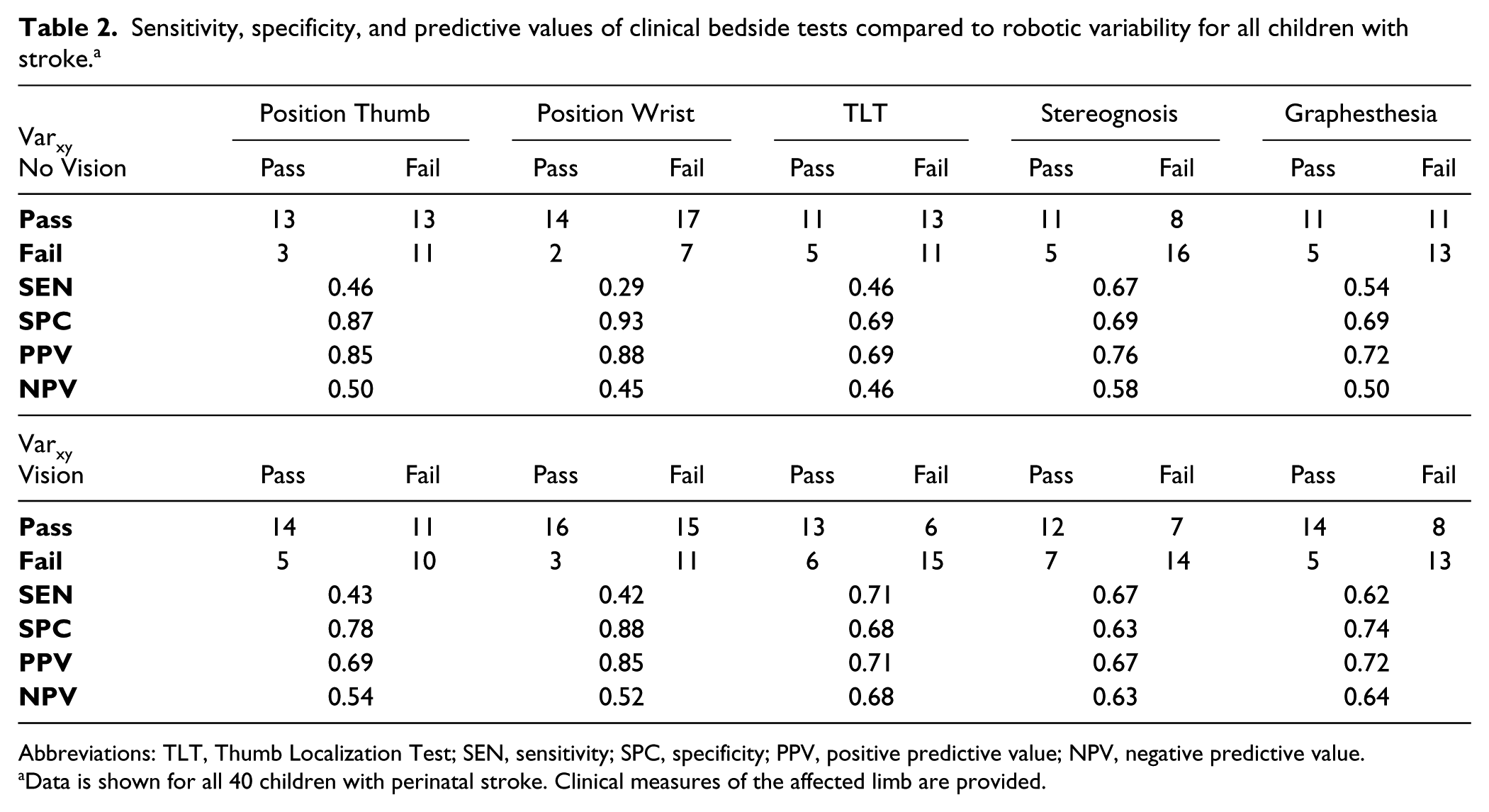
Abbreviations: TLT, Thumb Localization Test; SEN, sensitivity; SPC, specificity; PPV, positive predictive value; NPV, negative predictive value.
Data is shown for all 40 children with perinatal stroke. Clinical measures of the affected limb are provided.
Discussion
We have characterized position sense deficits in children with perinatal stroke and hemiparetic CP. Position sense deficits are common and more severe in children with near-term arterial compared to preterm venous lesions. Such impairments may be difficult to detect with routine clinical tests. Correlations between robotic measures of position sense and evidence-based functional outcome measures confirm clinical relevance with implications for rehabilitation.
Ours is not the first study to recognize sensory deficits in children with early brain injury and CP. 16 Using predominantly clinical measures of sensory function, multiple case series and case-control studies have documented evidence of impaired sensory function in children with congenital hemiplegia that correlates to degree of disability.6,7 Some studies have tried to explore position sense specifically, though measurement tools have been limited.27,28 We believe our study affords 2 important advances. The first is disease specificity, where we have carefully included only those children with perinatal stroke based on validated imaging including subclassification into specific diseases with discrete timing and lesions. 2 Perinatal stroke accounts for most cases of hemiparetic CP, and its focal nature creates an ideal human model of developmental plasticity. 3 Second is the novel application of a more precise, quantifiable robotic measurement tool for position sense. Outcome studies are only as good as the tools that measure them. We demonstrate that robotic assessment is feasible and well tolerated in school-aged children with and without disability. This supports further use as a sensitive and specific outcome measure to understand developmental plasticity following early injury and evaluation of new treatment strategies.
Our results are complimentary to similar robotic position sense studies in adults with stroke and hemiparesis. 8 This study found that position sense deficits occur in >50% of individuals with stroke and that impairment was twice as common in left-side affected than right-side affected individuals. In contrast, no laterality effect was observed across our AIS and PVI population. This is not surprising given the known lack of association with side of lesion and outcomes from perinatal stroke, including even the most strongly lateralized functions such as language. 5 This is just one of many differences between perinatal and adult stroke that must be considered through upcoming advances in stroke robotic measurements and therapeutics. 29 Furthermore, we must consider that findings are likely to be driven by adult populations and will require translation and in some cases reinterpretation for pediatric populations where developmental plasticity plays a role. A limitation is that our robotic task examined only one aspect of proprioception, position sense. Future work will aim to explore additional aspects of proprioception, including kinesthesia and sense of force, which are measureable with the KINARM in adult stroke. 30
Lesion type appears to be an important determinant of position sense dysfunction in children with perinatal stroke. Our results suggest that individuals with AIS show greater impairments in limb position sense compared to PVI participants. Effects may relate to lesion location where arterial strokes within the middle cerebral artery distribution typically injure both cortical and subcortical components of the sensory system while PVI lesions are purely subcortical. Differential timing of these 2 most common lesions may also influence sensory development with PVI lesions incurred before 32 to 34 weeks but most arterial lesions acquired near term. These factors may in part explain the differential and generally milder disorders of position sense that we observed in the PVI population.
Our methods also make an assumption that sensorimotor function in the unaffected limb is relatively normal. However, hemiplegic children may have abnormal “strong-side” function, a problem we are currently defining with additional robotic tasks that will eventually require integration into the sensory results reported here.
Advanced neuroimaging of sensory pathways provides additional insight. Diffusion tensor imaging (DTI) of corticospinal tracts has demonstrated utility in perinatal stroke and CP. 31 However, a recent systematic review confirms that little attention has been paid to sensory pathways. 32 Abnormalities of thalamocortical sensory projections have been demonstrated in children with hemiparetic CP using DTI. 33 More specifically, multimodal imaging studies have shown that ascending thalamocortical sensory pathways often bypass subcortical PVI lesions, connecting to appropriate areas of contralateral sensory cortex.34-36 In contrast, many children with perinatal stroke and hemiparesis develop prominent ipsilateral (contralesional) motor control of the affected hand. 3 The resulting “disconnect” whereby the normally tightly integrated primary and sensory cortices are now dissociated between hemispheres has been hypothesized as a contributor to disability.35,36 Additional advanced imaging studies using resting-state functional magnetic resonance imaging 37 and magnetoencephalography 34 suggest utility in understanding mechanisms of sensory impairment where combination with robotic outcome measures may be particularly fruitful.
The effects of vision restoration on position matching performance appear to be complex. The position match task was originally designed for performance without vision followed by repeat with vision with an expectation of correction. 8 While this does occur in some adults with stroke-induced deficits, the correction rarely returns performance to the normal range and can sometimes get worse. We observed similar effects here across both perinatal stroke groups with AIS children still markedly impaired with vision and some performing no better or slightly worse. These differences did not appear to be explained by hemianopsia or hemineglect though the prevalence of both complications was low. Explanatory mechanisms are speculative but these findings suggest possible dysfunction of cortical networks required to integrate position and visual sensory inputs. Further exploration of this hypothesis combining robotics, imaging, and brain stimulation 38 is indicated as such differences will need to be considered if corrective therapeutic approaches are to be developed.
Our findings may be used to improve clinical assessment of children with perinatal stroke and hemiparetic CP. Taking variability as the gold standard of position matching, the TLT demonstrated moderate sensitivity (69%). Adult stroke robotics studies also described some agreement with the TLT. 8 The easy bedside application of this test suggests clinical utility in screening children for position sense deficits. None of the clinical tests we measured demonstrated both high sensitivity and specificity, suggesting robotic assessments bring additional essential information to the characterization of position sense dysfunction. Unexpectedly, moderate specificity was observed for graphesthesia and stereognosis, the clinical sensory tests not specifically targeting position sense. One study of 41 children with hemiparetic CP found that impairment of clinical stereognosis correlated with function. 39 Overall, clinical sensory measures may suffer from lack of sensitivity to small changes in function, poor reliability, limited normalized values, and subjective examiner judgements.40,41 These limitations may be overcome with robotic technologies to provide more sensitive measurement and advance studies of neurophysiology and interventional outcomes in perinatal stroke.
Our results carry significant implications for perinatal stroke rehabilitation. Traditional strategies and outcome measures often focus on motor performance. Improving motor functions such as strength, speed, or dexterity may result in functional gains for some children. However, if reception or integration of position sense information is abnormal, isolated training of motor function may not translate into meaningful gains for individual children. Adult stroke robotic data suggest motor and sensory dysfunction are often discrete, independent problems. 18 Training to specifically improve position sense has not been established but may be facilitated by our findings here, specifically the importance of position sense dysfunction and the relative role of vision restoration.
The evolution of more evidence-based, functional rehabilitation strategies 42 such as constraint-induced movement therapy and hand-arm bimanual intensive training may help overcome this inattention to sensory function. This approach is in keeping with the World Health Organization International Classification of Functioning, Disability, and Health where therapy interventions should strive to achieve outcomes that translate into increases achievement of functional goals. 43 Evaluating emerging rehabilitation strategies with robotics to gauge effects on position sense would also be valuable. Whether robots can be engaged to deliver such therapies in children continues to be evaluated. 44 The integration of assessment tools such as we described into so-called “Serious Games” for rehabilitation would represent an important step in ensuring that robotic rehabilitation is addressing the needs of patients. It is clear that improving the understanding of developmental plasticity neurophysiology following perinatal stroke can improve outcomes with recent translation of similar work into 2 positive clinical trials (Kirton, unpublished data). 45
Footnotes
Acknowledgements
We would like to acknowledge the efforts and support of M. Metzler, J. Yajure, M. Piitz, and J. Hodge.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded through an Alberta Children’s Hospital CIHR trainee studentship, AIHS Graduate Studentship, Hotchkiss Brain Institute’s Robertson Fund, and a Cerebral Palsy International Research Foundation Grant.