
Abstract
Background. There is increasing interest in the application of cortical stimulation (CS) as an adjuvant strategy in aphasia rehabilitation. Epidural CS, although more invasive than other methods, can provide high-frequency ipsilesional stimulation with greater spatial specificity. Objective. We review methods and results of a phase 1 study of epidural CS in combination with rehabilitation therapy in aphasia and provide new objective and self-report data collected between 6 and 21 months after the end of treatment. Methods. Eight stroke survivors with nonfluent aphasia received intensive language therapy, 3 hours a day, for 6 weeks. Four participants also underwent surgical implantation of an epidural stimulation device that was activated only during therapy sessions. Behavioral data were collected before treatment, at the end of treatment, and at 6 and 12 weeks after the end of treatment. Of the 8 participants, 7 also participated in the longer-term follow-up visit. Results. Changes in objective scores from baseline were larger in investigational participants than controls at all assessments, including the longer-term follow-up visit. Satisfaction ratings and ratings of overall improvement by investigational participants and their companions were more varied than those of the controls, but all indicated that they would recommend the investigational treatment to others with aphasia. Conclusions. Improvements were generally maintained for at least 12 weeks posttreatment and possibly as long as 21 months posttreatment. Epidural CS is a potentially safe, feasible adjunctive intervention for persons with chronic nonfluent aphasia that spares the ventral premotor cortex and warrants further investigation.
Introduction
Approximately one-third of stroke patients present with the disruptive, often devastating consequences of aphasia.1-3 Aphasia is an acquired multimodality disturbance of language that impairs, in varying degrees, not only the understanding and expression of oral language but also reading and writing. It results from focal damage to the language portions of the brain, typically within the left hemisphere. People with aphasia have higher health care costs compared with stroke survivors without aphasia. 4 They have longer lengths of stay in hospital and increased use of rehabilitation services.1,4,5 They also have poorer long-term outcomes, including social isolation, increased stress, and reduced quality of life.6-8
Aphasia rehabilitation has typically included behavioral and environmental interventions that have resulted in positive short-term outcomes.9-11 Yet most patients with aphasia continue to be left with residual deficits and evidence regarding the long-term direct impact of the various aphasia treatments is generally lacking. Subsequently, there has been increasing interest in biological interventions that may enhance short- and long-term rehabilitation outcomes, with a surge of studies evaluating the use of cortical stimulation (CS) to facilitate brain plasticity and improve language skills in aphasia. There are various methods of CS that modulate cortical excitability, and most studies in aphasia have focused on the noninvasive methods of repetitive transcranial magnetic stimulation (rTMS)12,13 and transcranial direct current stimulation (tDCS).14,15 rTMS has been applied at relatively low frequency to the contralesional cortex, with transcallosal effects on the injured hemisphere. tDCS approaches have used either anodal (ipsilesional excitatory) or cathodal (contralesional inhibitory) stimulation but with very low levels of spatial specificity and a narrow population of target neurons. Neither technique can provide the high-frequency ipsilesional stimulation of high spatial specificity to targeted neuronal populations that is possible with more invasive epidural CS. 16
Numerous studies have investigated epidural CS in animal stroke models with positive outcomes when the CS was combined with behavioral motor training.17-19 Other studies, including a phase 3 randomized controlled trial, have investigated epidural CS as an adjunctive treatment for hemiplegia in stroke survivors.20-22 However, there are few reports of the use of epidural CS to facilitate language improvements in persons with stroke-related aphasia. Only 7 cases, all participants with chronic nonfluent aphasia, have been reported to date (3 case reports and 1 randomized controlled trial). 23
The earliest case report evaluated the effect of multiple sequential blocks of extradural stimulation to the motor cortex in an individual with hemiplegia who was 3 years poststroke. 24 Both low-frequency (50 Hz) and high-frequency (130 Hz) stimulations, first to the lesioned left hemisphere (during four 1-month stimulation intervals) and then to the healthy right hemisphere (during four 3-week stimulus intervals), were administered to areas of maximal functional magnetic resonance imaging (fMRI) activation. In another case report, an individual who was 18 months poststroke received 4 months of treatment involving 50-Hz CS to the premotor and motor cortex as well as Broca’s area. 25 In both cases, the cortical simulation was combined with rehabilitation.
Language improvements occurred and were maintained for some months posttreatment. However, there was no detailed evaluation of the aphasia before and after the application of the CS, and the described changes were mostly anecdotal. Nevertheless, the authors interpreted the effects of the CS as facilitating neural plasticity with reorganization of brain areas.
A more detailed description of the aphasia was provided in the case of a woman with aphasia who, at 4 years poststroke, received continuous epidural CS to address her chronic pain.26,27 Then, at 5 years poststroke, the stimulator was randomly enabled (on) or disabled (off) during 2 consecutive 1-month periods. When the stimulator was off, speech and language deteriorated. In contrast, spontaneous language fluency showed improvements during the on period. The same on/off assessment was performed after 5 years of stimulation and, again, a year later, when the patient was 9 and 10 years poststroke, respectively. Each time she showed better verbal fluency during the on period than the off period. Unlike the first 2 cases, concurrent language rehabilitation was not provided. The investigators concluded that improvements in language skills were dependent on the presence of the stimulation. They suggested that the pathophysiological mechanism of the CS is likely linked to the restoration of the intrahemispheric/interhemispheric functional balance rather than long-lasting neuroplastic changes with reorganization of language areas.
We have conducted the first controlled study of epidural CS in combination with rehabilitation therapy in 4 participants with aphasia. We have previously published the results that were obtained at the end of treatment and at 6- and 12-week follow-up sessions.28,29 In this article, we report on new findings from a longer-term follow-up visit. The purpose of this visit was 2-fold: (1) to determine, based on objective findings, whether improvements had been maintained and (2) to gain a better understanding of the personal perspectives of the participants and their significant others, especially given the invasive nature of the CS. We provide a brief review of the procedures and results of the previously published study. We then report new findings from the longer-term follow-up visit.
Methods
Participants
This single-blind randomized controlled trial compared language outcomes from 4 investigational participants who received CS plus language therapy (CS/LT) and 4 controls who received the identical LT but no CS. The study was approved by the institutional review boards of Northwestern University and the University of Chicago.
Inclusion criteria were as follows: chronic nonfluent aphasia (more than 12 months postonset) following a single left-hemisphere ischemic infarction, confirmed by MRI; aphasia severity determined by the Western Aphasia Battery (WAB) 30 Aphasia Quotient (AQ) score of 20 to 80; premorbidly right handed; at least a 12th-grade education; English spoken as the primary language; and adequate visual and auditory acuity to participate in the LT.
In addition to the behavioral eligibility criteria, potential participants underwent task-dependent BOLD fMRI at 3 T, using T2* gradient echo spiral acquisition with a standard head coil. 31 Tasks were language related and included (1) observation of a woman in a video producing single syllables “ta,” “pa,” “tha,” and “ka”; (2) verbal repetition of the same syllables produced by the woman in the video; and (3) reading aloud 3- to 5-word sentences that appeared on the screen. A volumetric T1-weighted scan (120 axial slices, 1.5 × 0.938 × 0.938 mm resolution) was acquired and averaged to provide high-resolution images on which to identify anatomical landmarks and onto which functional activation maps could be superimposed. Detailed fMRI image processing methods have been described previously. 28 Participants who showed no common areas of activation in the ventral portion of the left precentral gyrus or sulcus (surface anatomy corresponding to Brodmann area 6lv) between the imitation and observation tasks or between the imitation and oral reading tasks were excluded. Other exclusion criteria were seizure disorders, hemorrhage, or depression as measured by the Center for Epidemiologic Studies Depression Scale (CES-D).32,33
The first 4 participants who met the inclusion and exclusion criteria were randomly assigned to the investigational (CS/LT) or control groups (LT). The next 4 participants were matched by aphasia severity (ie, within 10 points on the WAB AQ) to one of the already randomized participants and then assigned to the opposite group. The primary characteristics of the enrolled participants are shown in Table 1. The first 4 eligible randomized participants were participants 001, 002, 005, and 008. In Table 1, participants are ordered in matched pairs according to the severity of aphasia.
Participant Characteristics. a
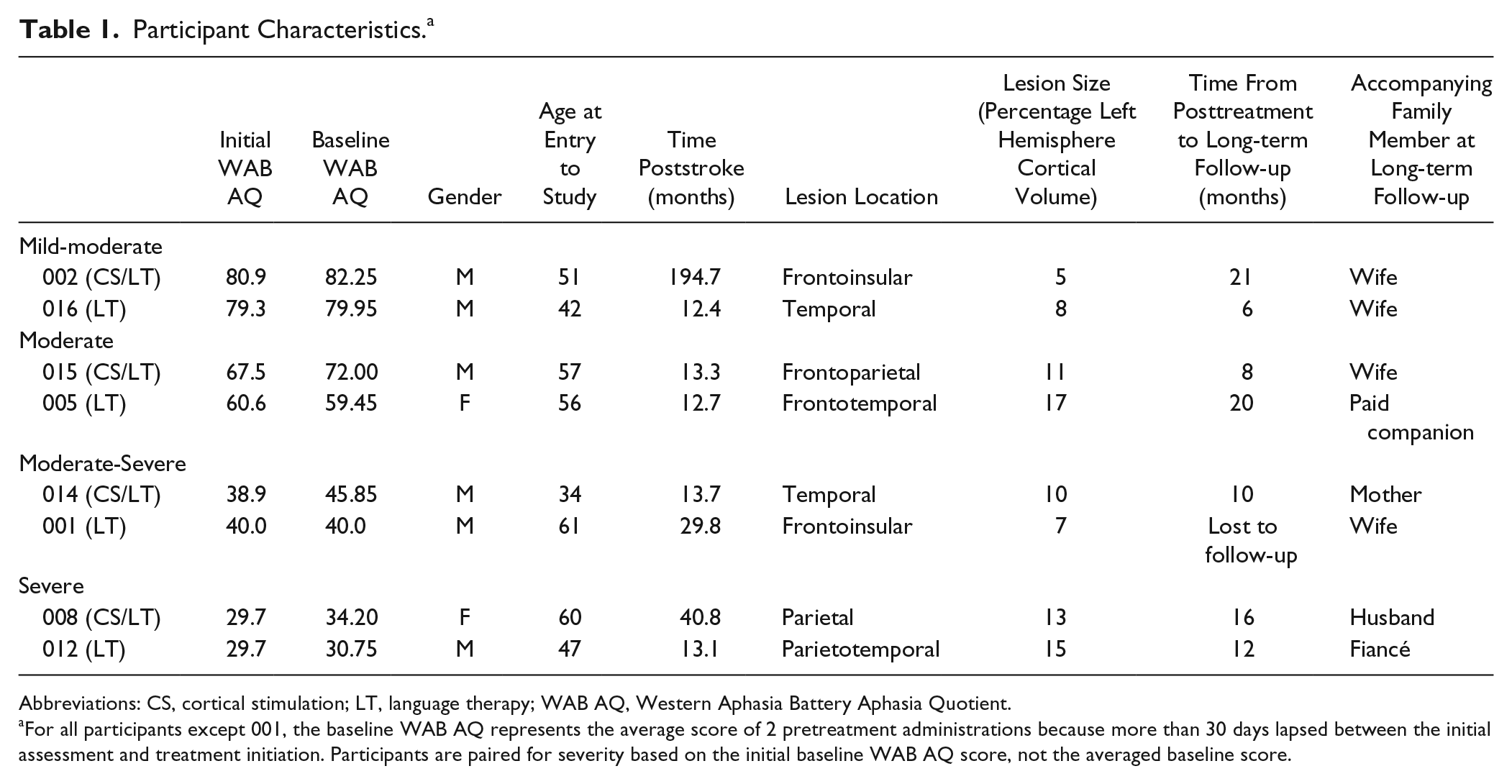
Abbreviations: CS, cortical stimulation; LT, language therapy; WAB AQ, Western Aphasia Battery Aphasia Quotient.
For all participants except 001, the baseline WAB AQ represents the average score of 2 pretreatment administrations because more than 30 days lapsed between the initial assessment and treatment initiation. Participants are paired for severity based on the initial baseline WAB AQ score, not the averaged baseline score.
Procedures
Approximately 2 weeks after randomization, participants in the investigational group (CS/LT) underwent surgical implantation of the CS device. An investigational epidural 2 × 3 grid electrode array, 2.6 × 2.7 cm2 in total area (Northstar Neuroscience Inc, Seattle, WA) was implanted on the dura over the left ventral precentral gyrus at the site closest to the fMRI activation site using frameless stereotaxic neuronavigation. The electrode lead was tunneled to a subclavicular site and connected to an investigational implanted pulse generator (Northstar Neuroscience). A second surgical procedure was performed to remove the implanted system at the end of therapy, following the posttreatment assessment.
Intervention
Both investigational (CS/LT) and control participants (LT) received the identical outpatient speech and language therapy for 3 hours a day, 5 days a week, for 6 weeks. Investigational participants (CS/LT) also received bipolar CS simultaneously with the speech and language therapy. The target stimulation level was determined prior to the first treatment session and defined as 50% of the language function threshold (ie, the minimum amount of current required to inhibit language function during a counting task or to elicit movement of the mouth or tongue). If language function was not affected within the programmed parameter limits of the implanted pulse generator, then the stimulation level was set to the lesser of the maximum stimulator current or 6.5 mA. One participant (002) received stimulation at 4.75 mA. It was set at 6.5 mA for all other participants. The pulse repetition frequency was 50 Hz, and the pulse duration was 250 µs for all participants.
The language treatment protocol provided practice at each of the phoneme, word, sentence, and discourse levels of language and included the following: (1) 30 minutes of apraxia drills that emphasized repetitive articulation of syllables and words, (2) 30 minutes of confrontation naming of black-and-white line drawings with hierarchical semantic and phonological cuing provided by a trained speech-language pathologist (SLP), (3) 60 minutes of computer practice involving choral reading of sentences, and (4) 60 minutes of conversational practice. Details have been described previously. 29
Assessments
As previously reported, participants were assessed at 4 separate time periods: (1) at entry into the study (baseline), (2) immediately after the 6-week treatment period (posttreatment), (3) 6 weeks following the end of the intervention (6-week follow-up), and (4) 12 weeks following the end of the intervention (12-week follow-up). The SLP who conducted the assessments was independent of the SLP who provided the treatment and blinded to the participant’s group assignment; participants wore complete head coverings to hide possible evidence of recent surgery.
The WAB AQ served as the primary outcome measure, with a 5-point improvement from baseline to posttreatment being considered success. If more than 30 days passed between the initial baseline assessment and the beginning of treatment, the WAB AQ was readministered, and the mean of the 2 pretreatment WAB AQ scores was used for all subsequent analyses.
Other assessments administered at each of the 4 assessment times included the Boston Naming Test 34 and caregiver ratings on the Communicative Effectiveness Index (CETI). 35 Picture descriptions of 2 composite pictures were also elicited and scored for content (Correct Information Units) and rate (words per minute). 36 The NIH Stroke Scale, 37 the Box and Block Test, 38 and selected subtests of the Behavioral Inattention Test 39 were given to rule out nonspecific effects of both the language therapy and the CS. In addition, the fMRI tests were repeated at the posttreatment assessment only.
Longer-term Follow-up Assessment
The longer-term follow-up assessment occurred during the same 2-week period when all participants in the study, both investigational and control, were invited to return for a brief assessment and to discuss their impressions about having participated in the study. They were also asked to bring to the visit a family member, friend, or other significant person who knew them well both before and after their participation in the study. Because participants had been recruited over a time period of about 15 months, the length of time from the end of treatment to their return for this follow-up visit varied considerably, as seen in Table 1. For 002, who was enrolled early in the study, the time since the end of his treatment was 21 months as compared with 6 months for 016, the last participant enrolled. Although 001 was contacted, he did not return for this visit. This was not unexpected because he had also refused to return for the 12-week follow-up visit, citing disappointment at not being randomized to the investigational group and subsequent dissatisfaction with his language improvements. The other 7 participants returned for this follow-up visit accompanied by a significant other person, as indicated in Table 1.
This follow-up visit has not previously been reported. It was shorter than prior assessments, lasting about 2 hours. In addition to the WAB and CETI, participants and accompanying persons each completed a questionnaire independently of each other (see Figure 1). It had 6 multiple choice questions that rated the degree of improvement from the first therapy session to the current time with regard to speaking, using the phone, being understood by others, communicating with family, communicating socially, and overall improvement in speech and language function. They were asked how satisfied they were with the results of their therapy and whether they would recommend it to other stroke survivors with aphasia. Finally, they were asked for examples of activities that improved (if any) and for brief comments such as the importance of these improvements for the participant. Because most participants with aphasia had difficulty with written expression, they were given an opportunity to provide oral responses to this final question. The author and one of the treating clinicians facilitated a discussion with the participant and accompanying person to elicit and/or confirm their responses and to clarify the written responses of the accompanying person.
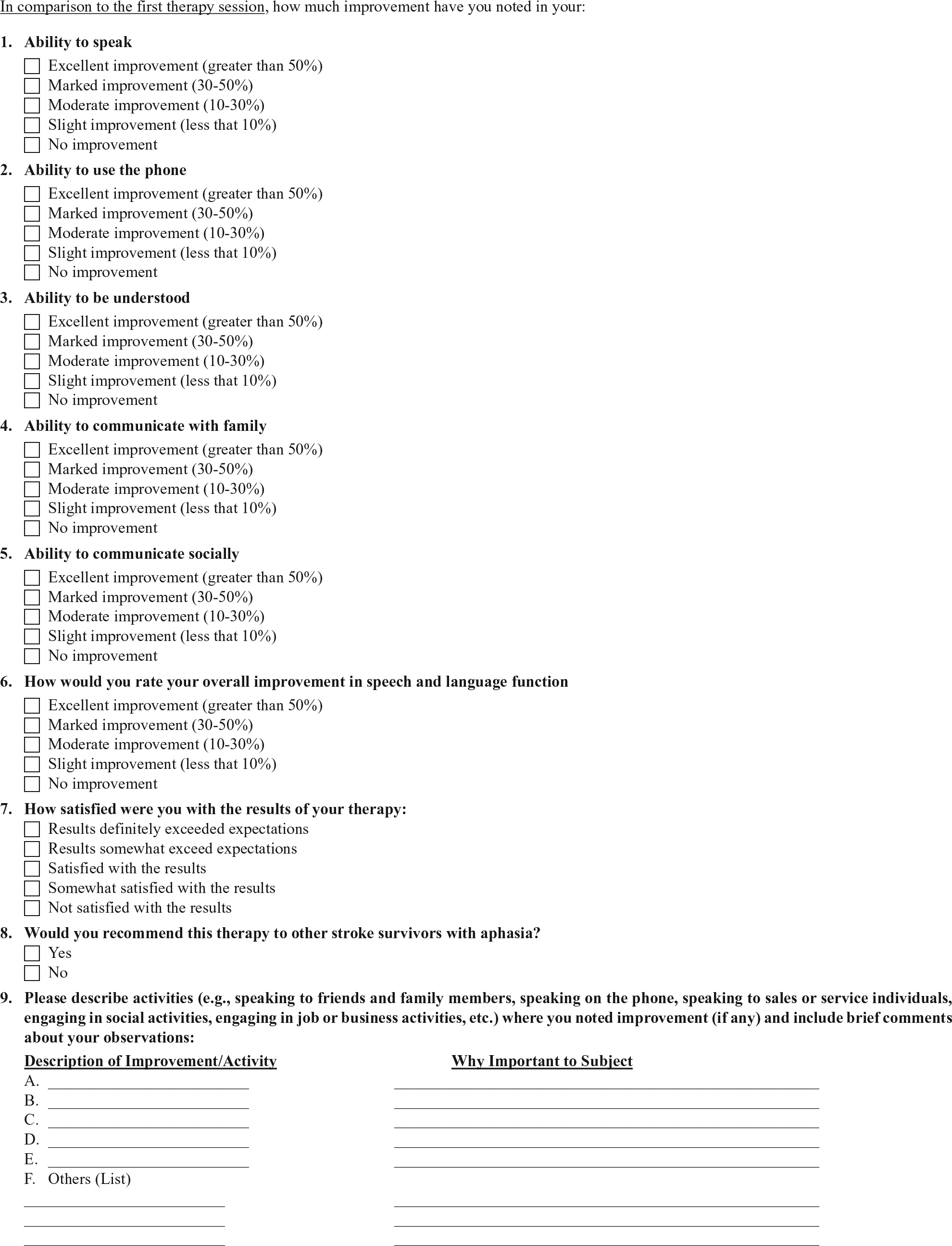
Copy of questionnaire completed by participants and accompanying persons at the longer-term follow-up visit.
In the original study, one way of assessing therapeutic efficacy was with effect sizes—these were computed for the change from baseline to posttreatment, and to the 6- and 12-week visits for the WAB AQ and CETI scores. 29 Effect size measures the magnitude of a treatment effect and, unlike significance testing, is independent of sample size. 40 With Cohen’s d, we calculated the effect size for the change in test scores from baseline to the longer-term follow-up visit using the original means and standard deviations of the independent groups. 41 The effect sizes were benchmarked against Cohen’s definition of effect size as follows: small, d = 0.2; medium, d = 0.5; and large, d = 0.8. 40
Results
As previously reported, both the surgery and CS therapy were safe. No adverse events affected the course of therapy or had an impact on patient well-being. Neurological function assessed with the NIH Stroke Scale, the Box and Blocks Test, and subtests of the Behavioral Inattention Test remained stable in all participants. Neurobiological changes were seen from pretreatment to posttreatment, with functional imaging suggesting increased consolidation of activity in interventional participants. Investigational participants were more likely to have decreases in functional activation throughout the brain than those who did not receive the epidural CS. Furthermore, the moderately and severely affected participants were more likely to have decreases in regions critical to language performance.
Language Outcomes: WAB
Figure 2 displays the mean change from baseline in the primary outcome, the WAB AQ, for the investigational (CS/LT) and control (LT) groups, and Table 2 shows the change from baseline for each participant. Performance on the primary outcome measure, the WAB AQ, at the 4 assessment times has been reported previously. Investigational participants showed a mean WAB AQ change from baseline of 8.0 points at both posttherapy and 6-week follow-up end points and 12.3 points at the 12-week follow-up (Figure 2). The control group had a change of only 4.6 points posttherapy, 5.5 points at the 6-week follow-up, and 3.6 points at 12 weeks. There were no data for 1 control participant at the 12-week follow-up.
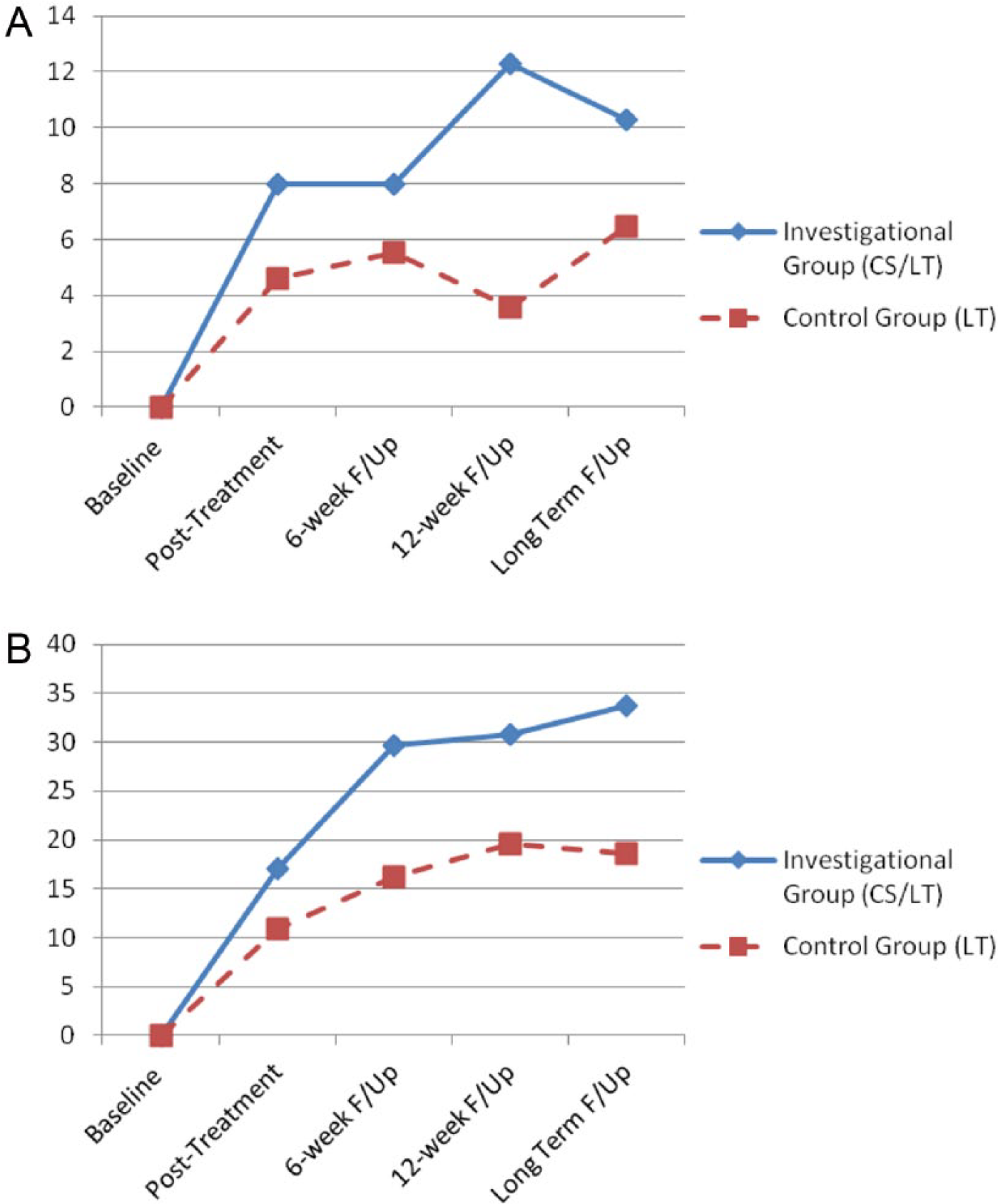
Mean change in Aphasia Quotient of the Western Aphasia Battery (A) and the Communicative Effectiveness Index (B) for the investigational (blue/diamond shape) and control (red/square shape) groups, showing a group difference at all time points. Note that 1 control participant was lost to follow-up at 12 weeks.
Change Scores From Baseline to Each Assessment Period for Participants, Paired for Severity by Initial WAB AQ Scores.
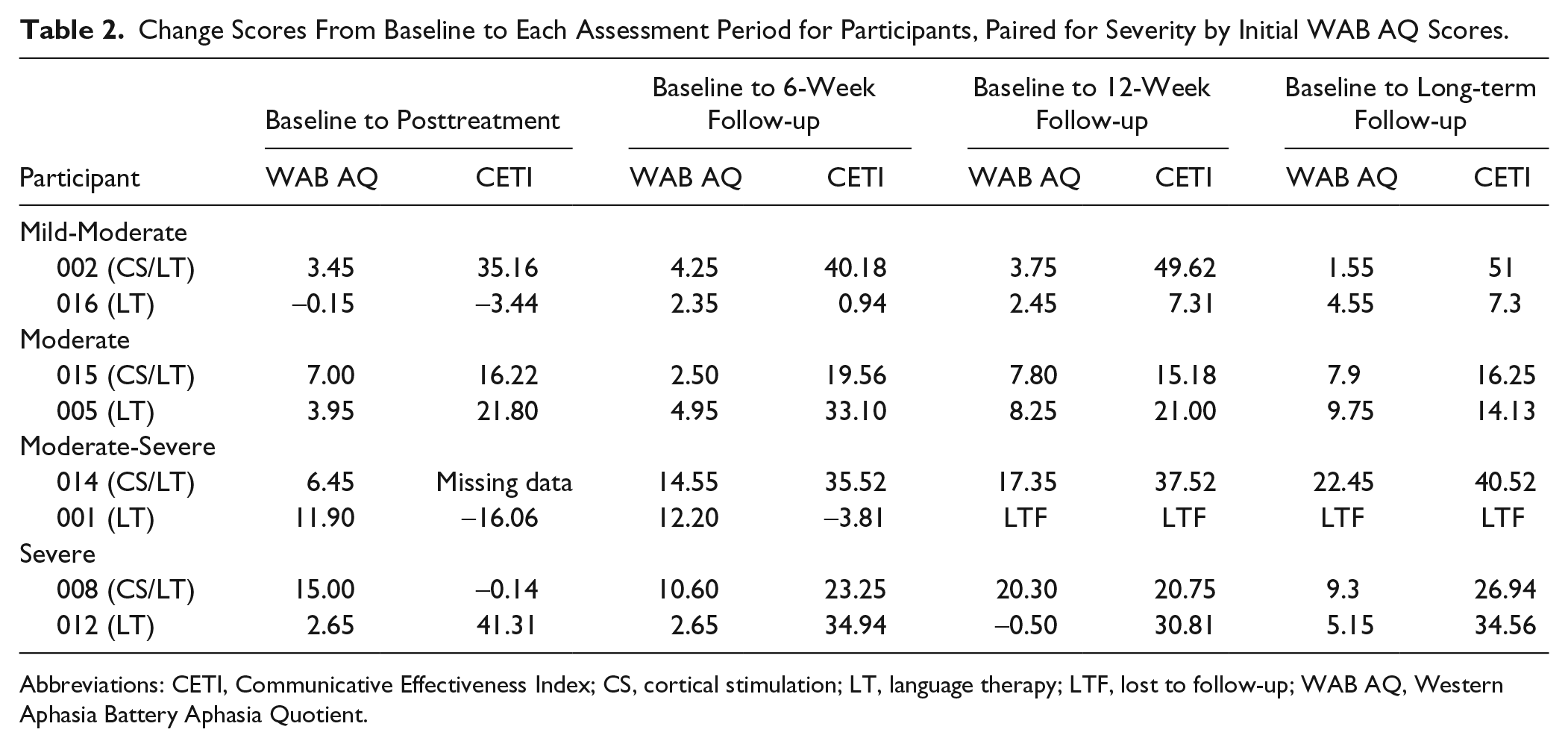
Abbreviations: CETI, Communicative Effectiveness Index; CS, cortical stimulation; LT, language therapy; LTF, lost to follow-up; WAB AQ, Western Aphasia Battery Aphasia Quotient.
At the longer-term follow-up, similar to previous assessment times, the investigational group made a larger change from baseline than the control group. However, the pattern of change differed from the pattern seen at 12 weeks. At 12 weeks, the gap between the mean scores of the 2 groups appeared to widen, with the investigational group continuing to improve and the control group showing some deterioration. In contrast, at the longer-term follow-up session, the gap between the groups was narrowing, with increased improvements in the control group and some deterioration in the investigational group. The effect size of the change from baseline for the investigational group over the control group had been large (Cohen’s d =1.32) at 12 weeks and was now benchmarked as moderate (Cohen’s d = 0.54), as indicated in Table 3.
Means, SDs, and Effect Size (Cohen’s d) of the Change from Baseline to Posttreatment and Follow-up for the Investigational Group (CS/LT) Compared With the Control Group (LT). a
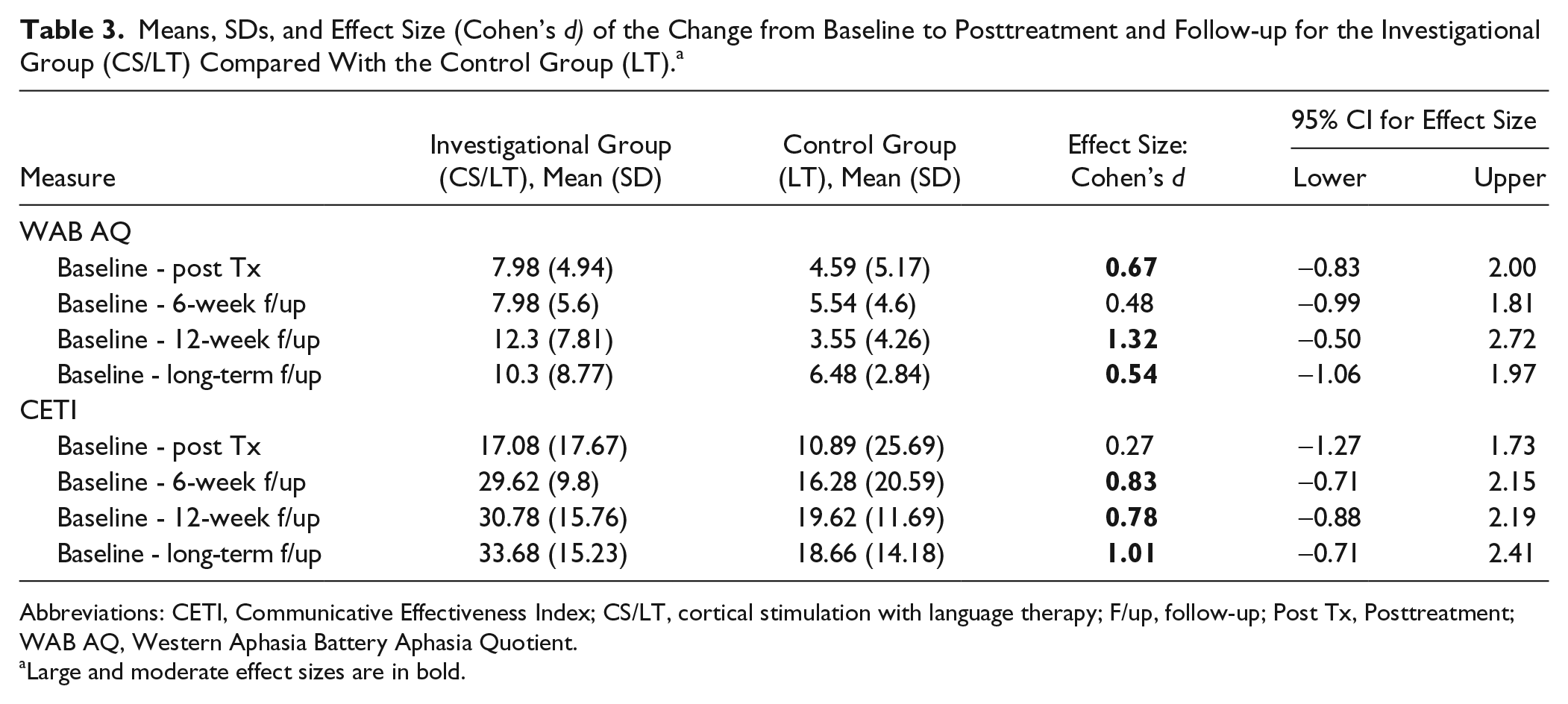
Abbreviations: CETI, Communicative Effectiveness Index; CS/LT, cortical stimulation with language therapy; F/up, follow-up; Post Tx, Posttreatment; WAB AQ, Western Aphasia Battery Aphasia Quotient.
Large and moderate effect sizes are in bold.
Analysis of individual participant’s scores show that the WAB AQ scores from the most severe pair of participants contributed to this change in pattern at the longer-term follow-up. At the 12-week follow-up, the most severe investigational participant (008) had an increase of 20.3 points from baseline, whereas the change from baseline for the most severe control participant (012) was −0.5. At the longer-term follow-up, 012 showed a jump in the WAB AQ to 5.15 points from baseline, thereby closing the gap between his change score and that of the matching investigational participant, 008, whose score from baseline decreased to 9.3 points.
Much of the change in the investigational group was contributed by 014, a participant with moderately severe aphasia. He continued to make improvements after the 12-week posttreatment testing, with the change from baseline increasing from 17.35 points to 22.45 at the longer-term follow-up visit. Unfortunately, the matched control participant (001) was lost to follow-up, so that his data were not available for comparison.
Caregiver Perceived Change: The CETI
Figure 2 displays the mean CETI change from baseline for the investigational and control groups, and Table 2 shows the change from baseline for each participant. Previously, the mean change in caregiver ratings mirrored the trends seen with the WAB AQ. Both groups were perceived to have improved over time, with greater changes consistently noted for the investigational group. Investigational group changes were 17.1, 33, and 30.8 points at posttreatment and 6- and 12-week follow-ups, respectively. The respective control group changes were 10.9, 16.3, and 19.6 points.
At the longer-term follow-up, the differences between the groups had further increased. The effect size of the change from baseline for the investigational group over the control group had been small immediately posttreatment (Cohen’s d = 0.27) and moderate at 6 and 12 weeks posttreatment (0.83 and 0.78, respectively). At the longer-term follow-up, the effect size was benchmarked as large (Cohen’s d = 1.01), as seen in Table 3.
Analysis of individual participant’s scores show that much of the perceived change in the investigational group at the longer-term follow-up was contributed by the ratings for 002, a participant with mild-moderate aphasia. The change from baseline of 51 points at the longer-term follow-up contrasts sharply with a perceived change of only 7.3 points in the matched control participant, 016. Also, 014 scores continued to increase from 37.52 at the 12-week posttreatment session to 40.52 at the longer-term follow-up.
Questionnaire Responses
Table 4 shows the responses of the participants with aphasia and the accompanying person. With regard to overall improvements and satisfaction with the study, responses of the accompanying persons were varied across participants and groups. Yet all the accompanying persons responded that they would recommend the treatment to others with aphasia. Several of the key items identified as important changes for the person with aphasia were not limited to verbal expression but included other language modalities—reading, writing, and auditory comprehension. Examples included talking alone to the doctor, speaking on the phone, doing personal banking, taking phone messages and relaying them to others, following the stock market, and passing the driver’s test. The importance of these activities with regard to the increased independence of the person with aphasia was a recurring theme.
Questionnaire Responses: Participants with Aphasia and Accompanying Persons (APs). a
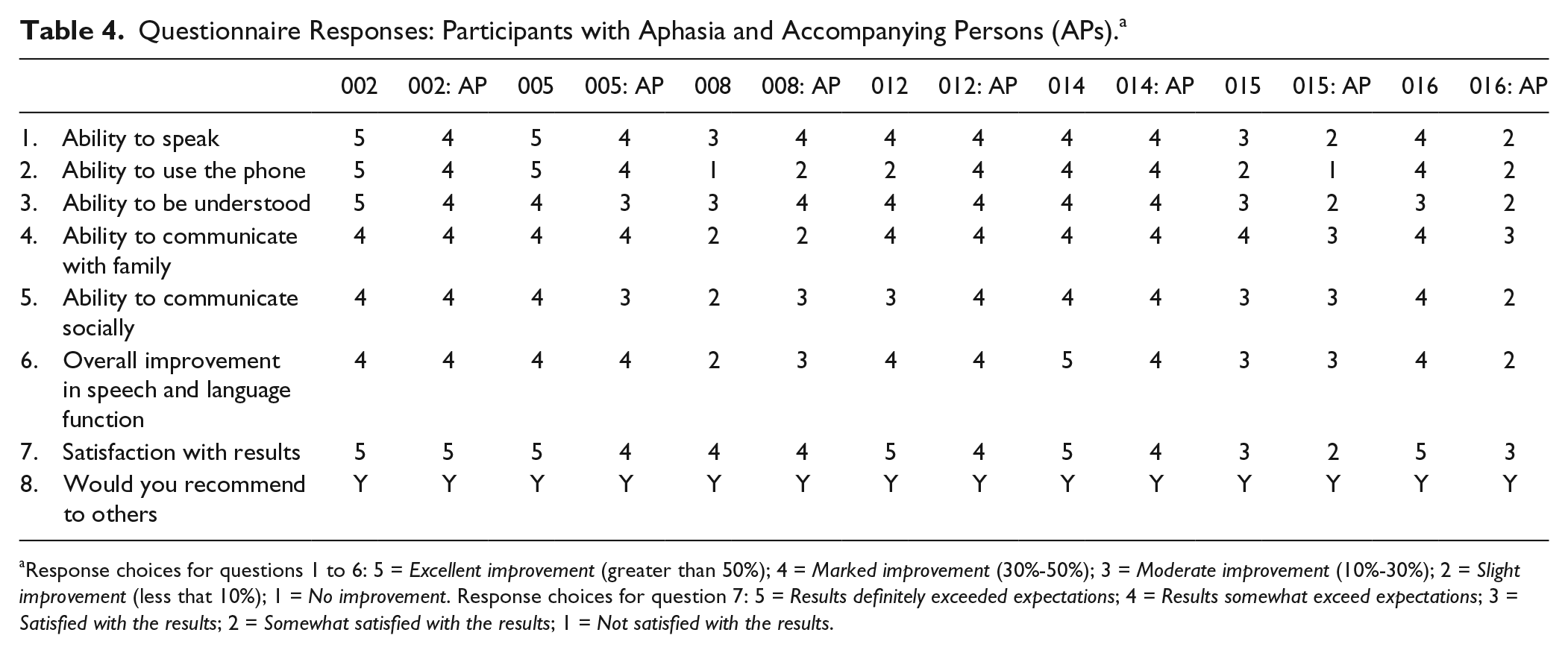
Response choices for questions 1 to 6: 5 = Excellent improvement (greater than 50%); 4 = Marked improvement (30%-50%); 3 = Moderate improvement (10%-30%); 2 = Slight improvement (less that 10%); 1 = No improvement. Response choices for question 7: 5 = Results definitely exceeded expectations; 4 = Results somewhat exceed expectations; 3 = Satisfied with the results; 2 = Somewhat satisfied with the results; 1 = Not satisfied with the results.
For the participants with aphasia, there was a range of responses in the investigational group in terms of overall improvements, with 1 participant responding in each of the categories of excellent improvement, marked improvement, moderate improvement, and slight improvement overall. In the control group, all 3 participants indicated marked improvement. Regarding satisfaction with their treatment, again, there was a range of responses in the investigational group. In contrast, all 3 control participants indicated that results definitely exceeded expectations. Like the accompanying persons, all participants responded that they would recommend their treatment to others with aphasia. Some specific examples of important changes identified by the person with aphasia included travelling alone and able to ask questions along the way, having conversations with neighbors and/or friends, asking and following directions over the phone with a tech support person, looking at apartments and asking questions to enable appropriate decisions, and following the stock market and making investment decisions. In addition to increased independence, better communication for informed decision making seemed to be a recurring theme in the persons with aphasia.
Discussion
This article summarized the methods and results of a clinical trial evaluating epidural CS in combination with LT in aphasia. In addition to previously reported results, we have provided new objective and self-report data that were collected between 6 and 21 months after the end of treatment for 7 of the 8 participants who participated in the original clinical trial.
Because all participants received intensive language treatment, we anticipated that participants in both investigational (CS/LT) and control (LT) groups would demonstrate language improvements, as measured by the primary outcome (WAB AQ). It was also expected that the investigational group who received both CS and LT would make larger changes than the control group who received LT alone. Although the sample size was small with insufficient power to make definitive statements, group-level results from the objective data suggest that CS may enhance LT. There were greater improvements in the WAB AQ in the CS/LT group at each assessment time, including the longer-term follow-up. Similarly, change scores on the CETI were greater in the investigational group at each assessment.
Within the CS/LT group, careful examination of the trajectory of change for the individual participants showed that only 1 participant (014) continued to make improvements after the 12-week follow-up visit. One participant (015) remained stable; 1 participant (002) made a small decline that likely represents normal variability; and 1 participant (008) declined considerably, with a change from baseline of 20.30 points at 12 weeks to only 9.3 points at the 16-month visit. A factor that may account for this decline relates to the richness of the communicative environment to which the participant returned and the opportunities available to her for using communication skills during the interim period. There was no formal assessment regarding the activities that were done during the interim period, but informal discussion revealed that 008 was mostly housebound. Her primary communication partner was her husband, and there were often times that she was alone at home with few opportunities for communication with other people. This contrasts with, for example, 014, who was younger and had access to various environments and communication partners outside of the home. He had returned to a supportive work environment as a cook and interacted with staff and other people in the restaurant. He also frequently visited with friends and participated in social activities with them. Continued practice of communication skills, whether formal or informal, may be necessary to fully maintain, in the long term, the previously made language improvements and associated neuroplastic changes.
Other factors such as initial aphasia severity and lesion location and size have been identified as affecting recovery in aphasia.42,43 These factors also may have differentiated participant 014, who continued to respond in the longer-term interim period, from participant 008, a participant with severe aphasia, who did not. In addition, CS parameters such as electrode placement relative to lesion location may have affected outcomes.
The mechanisms underlying CS remain unknown. Most interpretations suggest that enhanced neuroplasticity with more robust long-term learning and reorganization of neural circuits, possibly mediated by GABA-ergic intracortical networks, may contribute to the improved language associated with CS/LT.24,44 This hypothesis is consistent with the findings of our study, in which language improvements were maintained to some degree for more than 3 months and as many as 21 months after the end of treatment. Improvements were not dependent on the continued presence of CS, unlike the case presented by Balossier et al,26,27 in which language improvements were reversible and occurred only when the CS was on. Importantly, unlike other studies, no associated behavioral therapy was provided to this patient. Therefore, behavioral therapy may be an essential component needed to facilitate the long-term neuroplastic changes associated with true learning, and our findings provide support for the importance of combining CS with behavioral therapy.
Of those participants who received LT alone, all showed small improvements at the longer-term follow-up as compared to the 12-week visit, with the most severe participant making the largest change of more than 5 points. It is known that persons with chronic aphasia improve with intensive treatment,45-47 but none of the participants except 016 had reported receiving speech and LT during the interim. It is, therefore, encouraging that the intensive language treatment alone resulted in improved language skills that were maintained for as long as 20 months (eg, 005).
Because intensive behavioral therapy alone may promote long-term neural organization, it is interesting to speculate further on how the CS may enhance outcomes of the behavioral therapy. If the trajectory of the change lines in Figure 1 were extrapolated further over time, it is possible that they may eventually meet, so that the extent of improvement in those with and without the CS would eventually be the same. We suggest that CS may serve to increase the rate of language improvement and, therefore, the rate at which the underlying neural pathways reorganize, but not necessarily the extent of such reorganization. With time, those receiving LT alone could “catch up” with those who received the CS.
In previous reports, comparisons were made across pairs of participants at posttreatment and at the 6- and 12-week visits. However, comparisons at the longer-term visit should be made cautiously. First, the length of time since the end of treatment differed across participants. For example, 002, an investigational participant with mild-moderate aphasia, returned for the follow-up visit at 21 months posttreatment, whereas the control participant who was matched on severity, 016, returned at only 6 months posttreatment. Similarly, 015, an investigational participant with moderate aphasia returned at 8 months posttreatment, whereas the control participant 005 returned at 20 months posttreatment. Furthermore, as previously discussed, participants returned to environments that differed greatly in terms of their communicative richness and opportunities for continued formal and informal communication practice and exchanges.
The finding that those who received LT alone overall were more satisfied with the treatment than those who received the CS/LT is surprising in view of the greater objective changes observed in the investigational participants. It is possible that the inconvenience of undergoing the implant and explant procedures, which involved an overnight hospital stay with some postoperative pain (even though it was well tolerated), may have contributed to the lower satisfaction of the CS/LT participants. Another factor that may account for this finding relates to the wording of the questionnaire that linked the concept of satisfaction with prior expectations. Participants were not blinded to the treatment that they received; hence those who received the CS/LT may have had higher expectations of improvement than those who received the LT alone. The control participants had lower expectations, and all of them readily indicated that for them, the outcomes definitely exceeded their expectations, whereas the investigational participants, with their high expectations of improvement, tended to be more cautious when answering this question. Careful wording of the questionnaire to avoid tying success to expectations would have avoided this issue and provided a better representation of perceived success. Yet despite the caution with which the investigational participants and accompanying persons responded to the satisfaction question, all readily indicated that they would recommend their treatment to others, as did the control participants and their accompanying persons.
Limitations of the original study have been discussed elsewhere and include the absence of a sham stimulation arm, the small sample size that precludes significance testing, and differences in participant pairs on variables that potentially may affect therapy outcomes such as chronicity, age, lesion location, and lesion size. The additional methodological shortcomings related to the longer-term follow-up visit also warrant cautious interpretation of results. These include variability in the length of time between the end of treatment and the longer-term follow-up visit, which for some participants was relatively short (eg, only 6 months for 016), as well as differences in the communicative environments and the kinds of activities the participants engaged in during the interim. Nevertheless, this preliminary study indicates that excitatory ipsilesional high-frequency epidural CS is a potentially safe and feasible adjunctive intervention for persons with chronic nonfluent aphasia resulting from a single left-hemisphere ischemic infarction that spares the ventral premotor cortex. Participants demonstrated improvements on standard objective measures of language impairment, and these improvements were generally maintained for at least 12 weeks posttreatment and possibly as long as 21 months posttreatment. Those who received epidural CS in conjunction with intensive language treatment were sufficiently satisfied with their outcomes, so that they would recommend the treatment to others with aphasia. Further investigation of factors that may enhance the long-term response to CS/LT is needed.
Footnotes
Acknowledgements
The author acknowledges the contributions to the design and execution of the study made by Steven L. Small, coinvestigator on the main portion of the trial. Special thanks are given to Edna B. Babbitt, Rosalind Hurwitz, and Jaime B. Lee, who assisted with data collection, and to Elliot J. Roth and Richard L. Harvey for their administrative and clinical support.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was sponsored by Northstar Neuroscience through a clinical research study conducted under a Food and Drug Administration–approved Investigational Device Exemption (Clinical Trial Registration Number: NCT00170703).