
Abstract
Background. Regaining independent ambulation is important to those with stroke. Increased walking practice during “down time” in rehabilitation could improve walking function for individuals with stroke. Objective. To determine the effect of providing physiotherapists with accelerometer-based feedback on patient activity and walking-related goals during inpatient stroke rehabilitation. Methods. Participants with stroke wore accelerometers around both ankles every weekday during inpatient rehabilitation. Participants were randomly assigned to receive daily feedback about walking activity via their physiotherapists (n = 29) or to receive no feedback (n = 28). Changes in measures of daily walking (walking time, number of steps, average cadence, longest bout duration, and number of “long” walking bouts) and changes in gait control and function assessed in-laboratory were compared between groups. Results. There was no significant increase in walking time, number of steps, longest bout duration, or number of long walking bouts for the feedback group compared with the control group (P values > .20). However, individuals who received feedback significantly increased cadence of daily walking more than the control group (P = .013). From the in-laboratory gait assessment, individuals who received feedback had a greater increase in walking speed and decrease in step time variability than the control group (P values < .030). Conclusion. Feedback did not increase the amount of walking completed by individuals with stroke. However, there was a significant increase in cadence, indicating that intensity of daily walking was greater for those who received feedback than the control group. Additionally, more intense daily walking activity appeared to translate to greater improvements in walking speed.
Introduction
Improved walking function is the most common rehabilitation goal poststroke.1,2 Evidence suggests that high-volume,3-5 task-specific6-10 rehabilitation delivered early poststroke3,8 improves function. Therefore, individuals with stroke who wish to improve walking function should do extensive walking practice, if possible, early in rehabilitation. Increasing walking activity outside of structured inpatient rehabilitation could be one strategy to increase walking practice. However, previous studies report that individuals with stroke walk very little during inpatient rehabilitation,11-14 typically in short-duration bouts (<1 minute)11,12,14,15 to essential activities (eg, washroom, dining area, or therapy). 11 Therefore, methods to increase daily walking activity during inpatient stroke rehabilitation should be explored. 16
Goal setting, in which rehabilitation goals are determined by patients in collaboration with the interprofessional health care team, is an essential part of rehabilitation. Appraisal and feedback are important constructs in goal-setting theory.17,18 Feedback of progress toward goals can increase motivation, improve self-efficacy, and aid action planning. 18 Accelerometers can be used to quantify daily walking activity16,19 to provide such feedback.
This study aimed to determine the benefit of providing feedback regarding characteristics of patients’ daily walking activity to their physiotherapists as part of a goal-setting process. Feedback of the amount and intensity of daily walking, durations of walking bouts, and times of day when patients walked was provided. Our primary hypothesis was, compared with a control group, those who received feedback of daily walking activity would increase total daily walking activity, as measured by total walking time and total number of steps. To examine characteristics of daily walking, we also compared changes in length of walking bouts (ie, frequency of walking bouts >5 minutes and longest walking bout) and intensity of daily walking activity (ie, average cadence) between groups. We expected that increased walking activity would translate to better walking outcomes. Therefore, we hypothesized that the feedback group would show greater improvements in walking function and control than the control group, as measured with laboratory-based gait assessment (ie, increased self-selected walking speed, decreased variability, and improved spatiotemporal symmetry). Assuming that feedback improves self-efficacy and that increased walking activity helps participants achieve walking goals, we hypothesized that participants who received feedback would have greater increases in stroke self-efficacy and higher rates of attainment of rehabilitation goals than the control group.
Methods
Study Design
This single-blind randomized controlled trial spanned inpatient rehabilitation, outpatient rehabilitation, and postrehabilitation community reintegration; the current article focuses on data from the inpatient rehabilitation phase. The study was approved by the institution’s research ethics board. Further protocol details can be found elsewhere. 19
Participants
Individuals with subacute stroke attending inpatient rehabilitation at Toronto Rehab were recruited. To be considered for inclusion, participants (a) had a walking-related rehabilitation goal and (b) were able to walk without supervision at the time of enrollment. Patients who were not ambulatory on admission were reassessed for eligibility 2 to 3 times per week until they either became eligible or were discharged. Individuals unable to provide consent due to foreign language or cognitive impairment were excluded. Participants provided written informed consent prior to participation.
Group Allocation and Blinding
Participants were assigned using blocked stratified randomization (block size = 4) to 1 of 2 groups: (a) feedback (FBK) or (b) no feedback (ie, control group; CON). There were 2 strata based on self-selected walking speed at enrollment (slow walkers: <0.42 m/s; moderate-fast walkers: ≥0.42 m/s); stratification ensured that the 2 groups did not differ on walking speed, an important predictor of functional mobility. 20 Concealed group allocation was performed using a computer-generated random sequence by an investigator who was not involved in participant screening. A blinded research assistant screened and enrolled participants, conducted the assessments, processed data, and generated reports. Reports for FBK participants were delivered to the physiotherapist by an investigator who was not involved in data collection. The physiotherapists administered goal-setting/planning, including incorporating the walking activity report for FBK participants. Participants were not blinded and were informed of the chance of being allocated to either group.
Activity Monitoring
Participants wore 2 lightweight commercially available triaxial accelerometers (Model X6-2mini, Gulf Data Concepts, LLC, Waveland, MS), one on each limb, for all waking hours every weekday (excluding statutory holidays) from the time of enrollment into the study until discharge from inpatient rehabilitation. The accelerometers recorded 3-dimensional accelerations in blocks of 8 hours at 40 Hz. Participants were instructed to only remove the accelerometers before going to sleep at night, when showering, and when required for clinical testing. Each morning before the start of therapies (ie, before 9
Data were transferred from the accelerometers and processed using a custom-written algorithm implemented in MATLAB (The Mathworks, Natick, MA). The 3 dimensions of raw accelerations were high-pass filtered at 0.25Hz to remove the gravity component 21 and low-pass filtered at 5 Hz. Data were automatically reoriented to obtain a consistent frame of reference. A supervised machine learning algorithm was used to automatically detect walking sequences. Specifically, a RUSBoost binary classifier 22 was trained on a set of manually labeled data containing walking and various other activities from 17 participants outside of this study. Since accelerometer data have a significant class imbalance, that is, more time not walking than walking, RUSBoost was seen as an appropriate algorithmic choice as it randomly undersamples the majority class in the training data so that the number of examples of each class is equal. We used a MATLAB implementation of RUSBoost that used decision trees internally. The training data included nonwalking segments, including samples where participants used exercise equipment, such as a stationary bike, in order to help differentiate other reciprocal lower-limb activity from walking. By analyzing labeled training data, the algorithm learned to automatically identify patterns corresponding to walking, and was then used to assign a label to short, 1-second long, segments of study data. By sliding a query segment along a long sequence of accelerometer data, we identified times when participants were walking and the duration of each walking bout. A bout of walking was defined by ≥4 consecutive steps with <10 seconds between steps; if there was a pause of 10 seconds or more between steps, a new bout was identified. 11 Number of steps, bout duration, and cadence were calculated for each walking bout.
The algorithm was based on one previously validated for measuring walking activity among individuals with subacute stroke. 11 The older algorithm 11 relied on the 2 accelerometers being precisely synchronized in time, which was not always possible with the current accelerometers, and classified reciprocal nonwalking activity (eg, cycling) as walking. The new algorithm has good agreement with the previously validated algorithm among a subset of 34 participants (intraclass correlation coefficients = 0.89 for walking time and 0.87 for step count).
Intervention
Walking feedback was provided within the context of the rehabilitation team’s standard goal-setting process. Participants identified their own rehabilitation goals at admission. Participants and their physiotherapists collaboratively identified specific and measureable subgoals. For example, one goal might be “to be able to walk to my local subway station.” The physiotherapist could then assign a walking program of incrementally increasing difficulty based on the estimated time to walk to the subway station. For example, if the subway station is 15 minutes from the participant’s home, then the program might involve walking 5 times per day starting with 5 minutes continuously and increasing by 1 minute each day until the target time is achieved. Participants received 1 hour of physiotherapy per day; thus, physiotherapists had daily opportunities to discuss progress with physiotherapy-related rehabilitation goals (eg, walking goals) with participants. Additionally, participants met with their goal coordinators (assigned interprofessional team member) weekly to discuss progress with all rehabilitation goals. Daily individualized occupational therapy, speech and language pathology, and/or group therapies may have been prescribed to participants on an as-needed basis. Involvement in this study did not influence participation in other therapeutic activities.
A daily report was generated for each participant summarizing the previous days’ walking activity data (see the appendix). Reference values for target steps/day for various populations,23,24 and interpretation of cadence values 25 were also provided. Physiotherapists of participants assigned to the FBK group received the walking activity report daily as means to appraise achievement of walking goals and subgoals. 17 Walking reports were provided daily to physiotherapists from the second day of enrollment until the participant either withdrew or was discharged. Physiotherapists decided how best to use the information provided given participant-specific goals and language, communication, cognitive, and mobility impairments. Physiotherapists generally used the information to determine how much daily walking activity participants completed (ie, total walking time, number of steps, or bout durations) and if participants complied with an assigned walking program. In the case of noncompliance, the physiotherapist and participant discussed a strategy for better integrating walking activity into the participants’ day. In the event that the participant met his/her specific subgoals for walking activity, more challenging goals were identified. For CON participants, physiotherapists did not receive accelerometer-based feedback of daily walking activity. Physiotherapists discussed walking goals with CON participants daily, but relied on participants’ self-report for the appraisal portion of the goal-setting process, as per usual practice.
The physiotherapists were involved in all aspects of the study design and were supportive of the implementation of accelerometer-based feedback. The physiotherapists and research team met regularly prior to, during, and after completing data collection to discuss the study, including the format and clinically relevant variables to be included in the report, interpretation of walking data, consensus on guidelines for walking activity feedback, and interpretation of the study results.
Measures
The following cohort descriptors were obtained from clinical charts on admission to rehabilitation: age, sex, stroke onset date, lesion location, usual gait aid, Berg Balance Scale, 26 and Chedoke-McMaster Stroke Assessment leg score. 27 The National Institutes of Health Stroke Scale 28 was scored by the research assistant at enrollment. The primary outcome measure was change in walking activity (total walking duration and total number of steps) from enrollment into the study to discharge from inpatient rehabilitation, as obtained from the accelerometers. Secondary measures of daily walking activity were average cadence of each bout, longest bout duration, and number of long walking bouts (>5 minutes).
Additional secondary outcomes pertained to control of walking, self-efficacy, and goal attainment. Spatiotemporal features of walking were measured using a 4-m-long pressure sensitive mat (GAITRite, CIR Systems, Inc, Havertown, PA). Participants started walking at least 1 m before the start of the mat and were instructed to walk at their usual pace until they reached a mark 1 m after the end of the mat. Gait assessment was completed without participants’ usual walking aid, if possible. Participants completed enough passes across the mat such that at least 18 footfalls were recorded (typically 3-5 passes), with measures averaged over all passes. Step length, step width, swing time, and step time were calculated for each step. Spatiotemporal symmetries were calculated as ratios of left and right step length and swing time, with the larger number used as the numerator such that all values were >1. 29 Standard deviations of step length and time were calculated for each limb separately; variability was the average of the standard deviations for the left and right limbs. Step width variability was the standard deviation of step width. Walking speed was also calculated. The Stroke Self-Efficacy Questionnaire (SEQ) 30 was used to measure stroke-specific self-efficacy. This 13-item questionnaire asks participants to rate confidence in completing various tasks, including walking indoors and outdoors, on a scale from 0 to 10. Goal attainment was determined from patient charts at discharge from inpatient rehabilitation. Goals were classified “achieved,” “partially achieved,” “not completed,” or “discontinued.” Falls were documented for safety monitoring purposes.
Sample Size Estimate
Change in total walking time from the initial assessment to discharge from inpatient rehabilitation was the primary outcome for sample size estimates. Prior to undertaking this work, we measured daily walking activity in 5 consecutive patients attending inpatient stroke rehabilitation (unpublished data). We observed an average increase in total daily walking activity from 35 minutes on initial assessment to 54 minutes at discharge (~13 days apart); the standard deviation for change in walking time was 23 minutes. Assuming an average increase in walking activity of ~20 minutes from admission to discharge with no feedback, we expected that an increase in daily walking activity of 40 minutes in the FBK group would be clinically meaningful (ie, twice that expected with no feedback). Using a sample size formula for repeated measures ANOVA, 31 a 20-minute greater increase in walking time in the FBK than the CON group, standard deviation of 23 minutes, type I error probability of .05, and type II error probability of .1, 28 individuals per group would be required in the final analysis.
Data Analysis
Baseline characteristics were compared between the FBK and CON groups with Wilcoxon–Mann–Whitney tests (continuous or ordinal variables) or χ2 tests (categorical variables).
We initially planned to compare walking activity over the first 3 days with the last 3 days of monitoring. 19 However, due to a change service delivery at the institution between the time of study design and execution, many patients were discharged soon after attaining independent ambulation leaving fewer days between enrollment and discharge. Due to shortened length of stay, physiotherapists requested daily activity reports to begin immediately following study enrollment. Therefore, the first day of monitoring was used as the baseline measure of walking activity, and the mean of the last 3 days was used to measure of change over the course of rehabilitation. The second day was excluded from analysis as feedback was typically initially received during this day. Change in walking activity across the whole sample was initially analyzed using paired t tests comparing the daily mean of each measure over the last 3 days to the baseline value.
To test the hypotheses, we subtracted the baseline value from the mean of the final 3 days of monitoring and included the difference score in the analysis; fewer days were averaged for individuals with <5 days of monitoring. The pre- to postintervention difference was also calculated for walking control measures and SEQ. One-way analysis of covariance (ANCOVA) was used to compare between-group differences in change in walking activity, spatiotemporal characteristics of walking, and SEQ at the end of the monitoring period. The difference score was the dependent variable; the baseline value and time between assessments were included as covariates. The rate of goal attainment was compared between the 2 groups using χ2 tests. Alpha was .05 for all analyses. Intent-to-treat analysis was performed whenever possible.
Results
Participant Recruiting, Screening, and Retention
All patients admitted between October 2012 and January 2014 were assessed for eligibility (n = 238). Of these, 63 were eligible and agreed to participate. Three withdrew prior to completing the gait assessment and could not be randomized; therefore, 60 participants were allocated. Of those allocated, 9 (4 FBK, 5 CON) walked <0.42 m/s at study enrollment. Three withdrew with <3 days of activity monitoring due to early discharge (2 participants) or a change in medical status (1 participant). On chart review it was discovered that 2 participants (FBK) did not identify walking-related rehabilitation goals; however, they were not excluded as they were referred to the study by their physiotherapists who considered them to be appropriate for monitoring and feedback. Therefore, 57 participants (29 FBK, 28 CON) were available for analysis of the primary outcomes (Figure 1). The 2 groups did not differ on any baseline measures (Table 1).
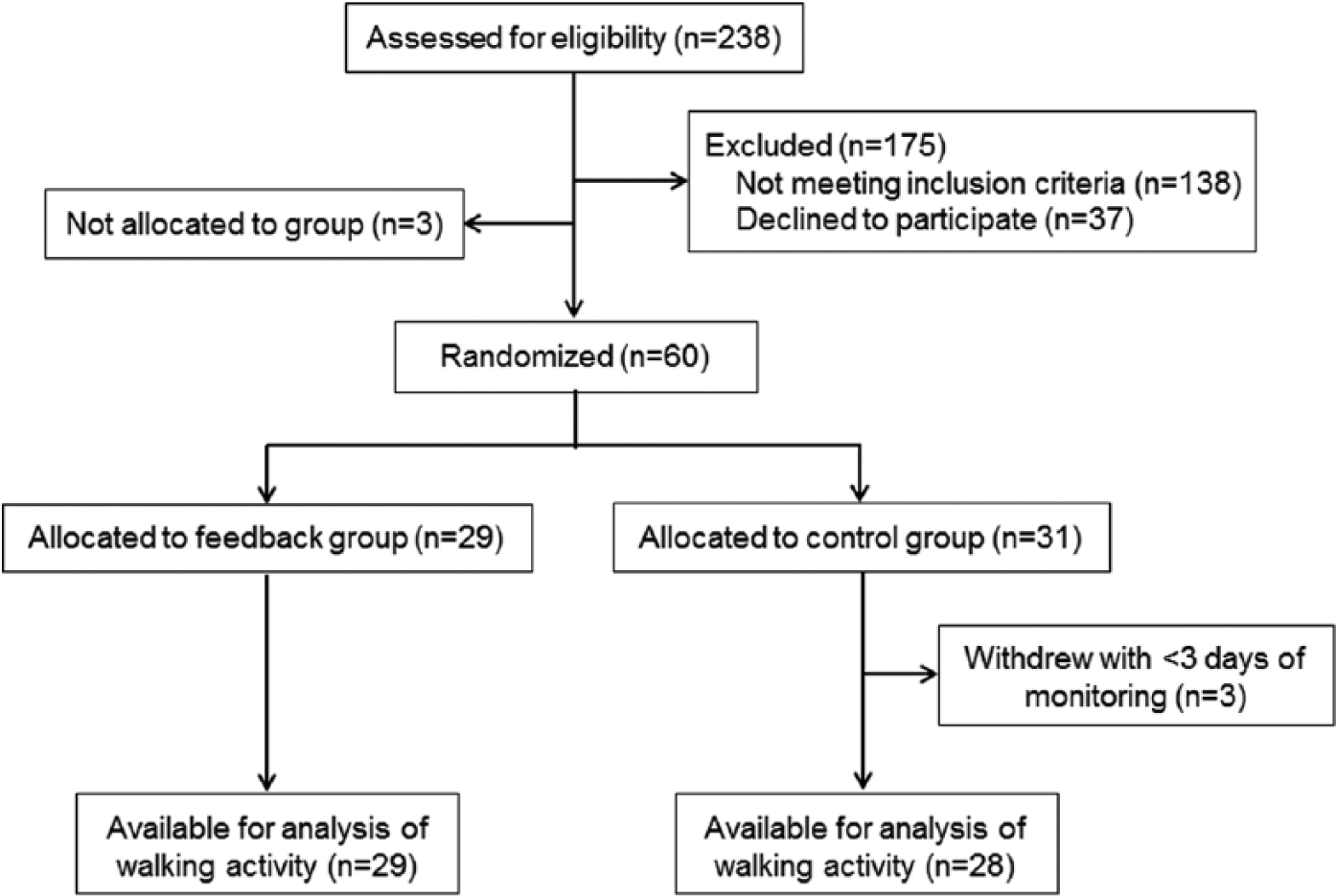
Flow of participants through the study.
Participant Characteristics a .
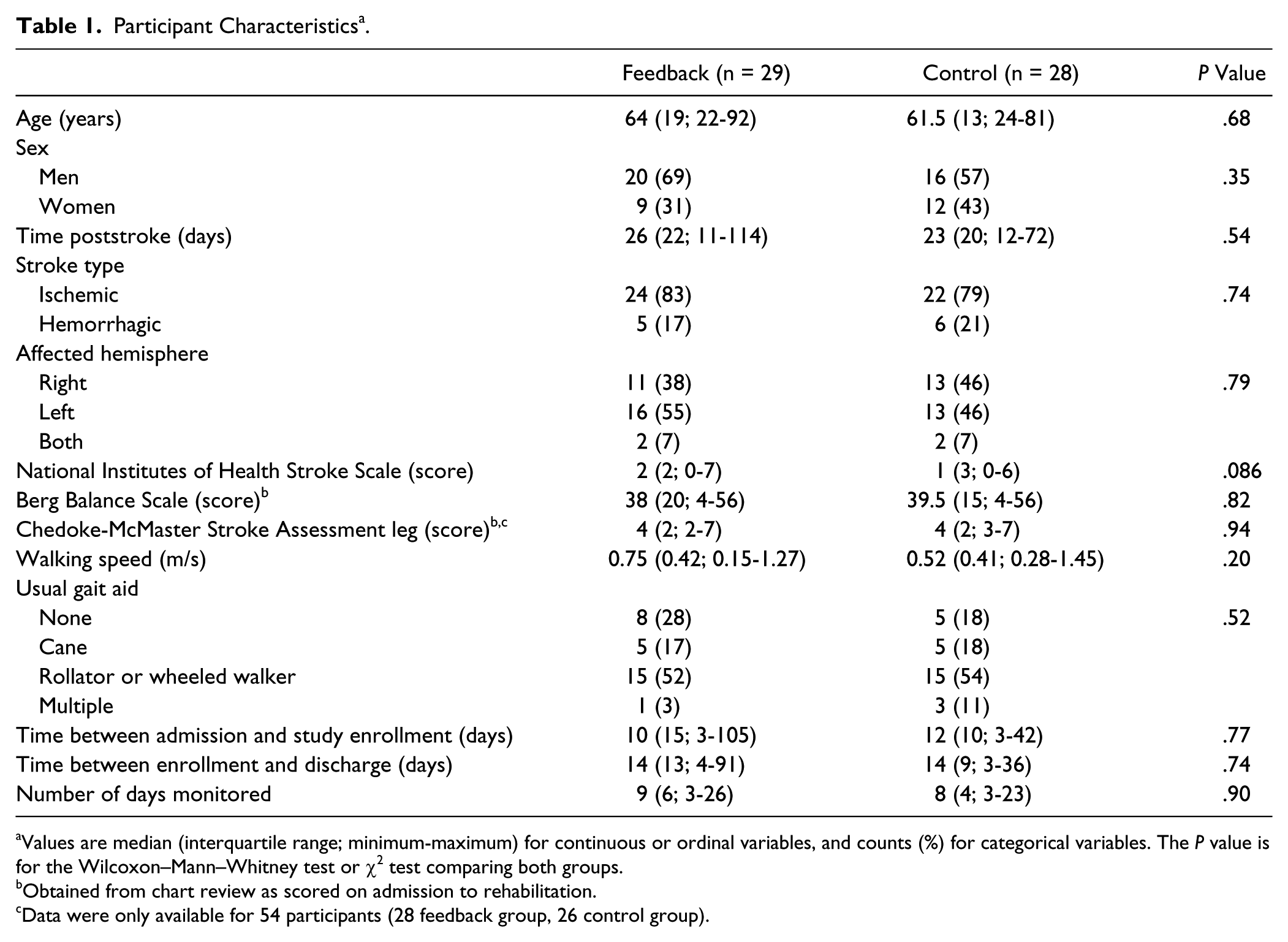
Values are median (interquartile range; minimum-maximum) for continuous or ordinal variables, and counts (%) for categorical variables. The P value is for the Wilcoxon–Mann–Whitney test or χ2 test comparing both groups.
Obtained from chart review as scored on admission to rehabilitation.
Data were only available for 54 participants (28 feedback group, 26 control group).
Six participants withdrew from the study prior to discharge from inpatient rehabilitation; 4 (2 FBK, 2 CON) declined further participation, one (FBK) was withdrawn because of illness, and one (CON) was withdrawn because accelerometers were lost repeatedly. All available walking activity data for these 6 participants were included in analysis.
Intervention Adherence and Adverse Events
There were 508 activity monitoring days for both groups combined; participants completed 3 to 26 days of monitoring (mode = 11 days). Reports were generated for all monitoring days, except those with technical difficulties (5 days), and delivered to the physiotherapists (FBK participants); a note was included with the report when accelerometers were not worn for the full day (16 days) or when temporary illness limited activity (2 days). One participant (FBK) experienced a fall during activity monitoring. The fall occurred while bending to retrieve something from the floor so was unlikely to be related to increased walking activity. No other adverse events were reported.
Missing Data
Ten participants (7 FBK, 3 CON) had fewer than 3 days at the end of activity monitoring for inclusion in analysis. For 9 participants, this was due to discharge soon after enrollment (<5 days), whereas 1 participant (FBK) had 5 days of activity monitoring but 1 day was excluded from analysis as he removed the accelerometers after just 4 hours. In addition to the 6 individuals who withdrew prior to discharge, gait data were not available for 3 participants (2 FBK, 1 CON) who declined discharge assessment. Gait data were also excluded from analysis if participants were assessed under different conditions at the 2 time points (6 FBK, 7 CON); that is, if they were unable to walk without an aid on the initial assessment but no longer required an aid on discharge. Therefore, 35 participants (18 FBK, 17 CON) were included in analysis of gait data. Twenty-nine participants declined the SEQ at one or both time points, or were unable to complete the SEQ due to communication or cognitive difficulties; therefore, analysis of SEQ data was limited to 22 participants (12 FBK, 10 CON). Analysis of goal attainment was limited to those who identified walking goals during inpatient rehabilitation (27 FBK, 28 CON).
Daily Walking Activity
Table 2 shows walking activity for both groups on the first and last 3 days of monitoring. On average, participants increased walking time, number of steps, average cadence, and longest bout duration (t56 > 2.10; P < .040), but not number of long walking bouts (t56 = 1.29; P = .20), from the time of enrollment until discharge. There were no significant between-group differences in changes in walking time, number of steps, number of long walking bouts, or longest bout duration (P -values > .20). FBK participants showed a greater increase in average cadence than CON participants (F1,53 = 6.61; P = .013). To further explore changes in cadence, we calculated the average time spent in slow walking (60-79 steps/min), medium walking (80-99 steps/min), and brisk walking (100-119 steps/min; Figure 2). 25 FBK participants appeared to spend slightly less time in slow walking but increased the amount of time in medium and brisk walking from enrollment to discharge.
Daily Walking Activity a .
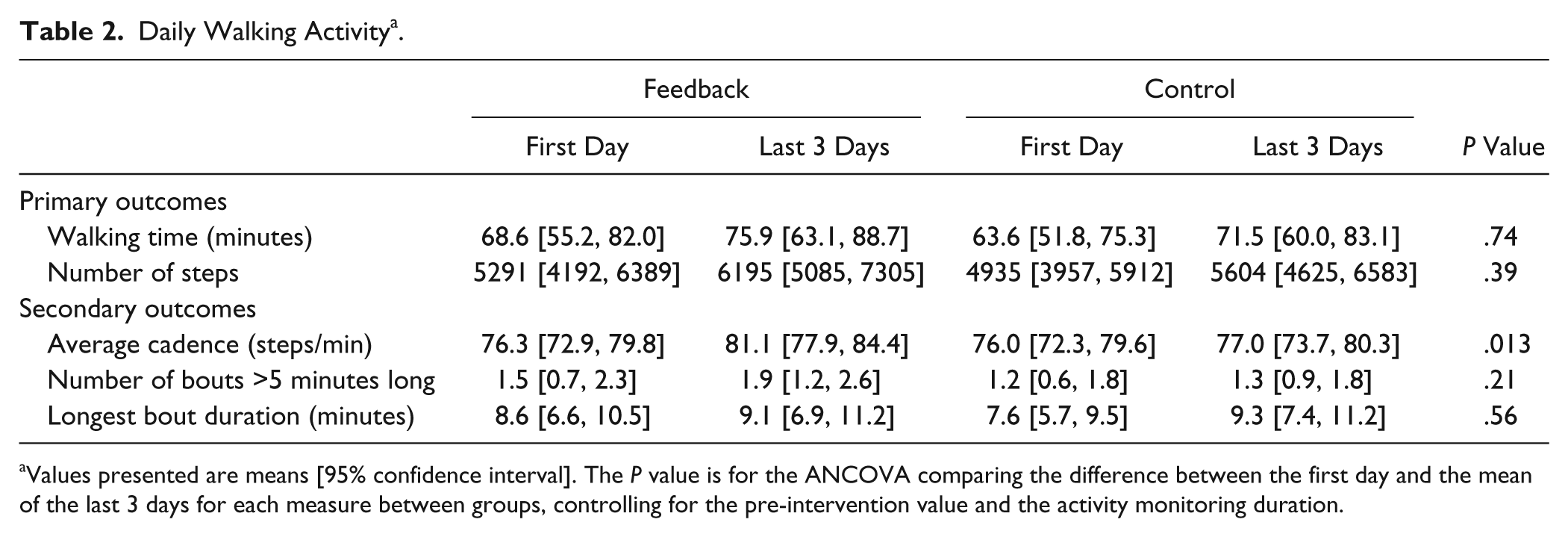
Values presented are means [95% confidence interval]. The P value is for the ANCOVA comparing the difference between the first day and the mean of the last 3 days for each measure between groups, controlling for the pre-intervention value and the activity monitoring duration.
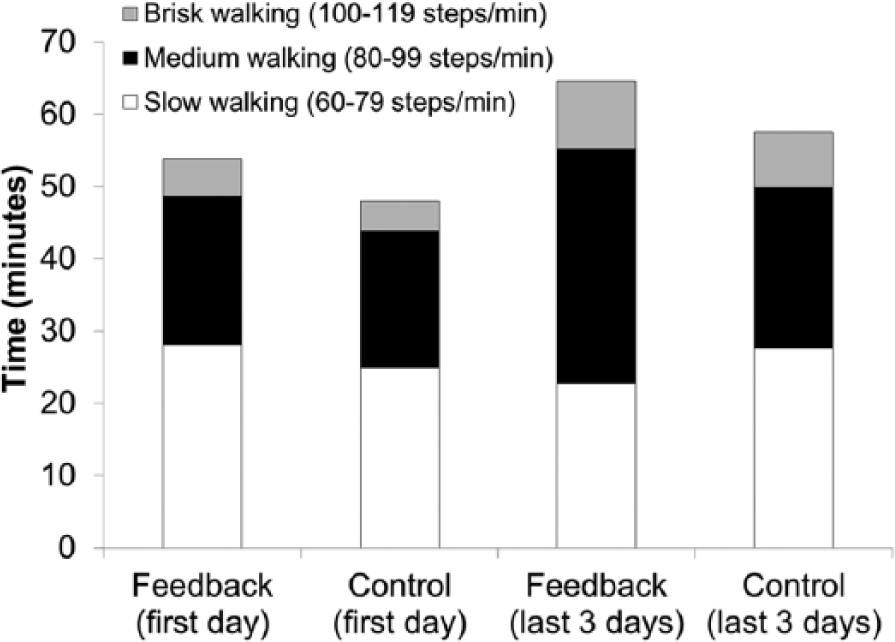
Changes in average cadence of daily walking.
Laboratory Gait Assessment, Self-Efficacy, and Goal Attainment
FBK participants had a greater increase in walking speed (F1,31 = 5.54; P = .025) and a greater decrease in step time variability (F1,31 = 5.29; P = .029) than CON participants (Table 3). There were no other significant between-group differences in changes in gait control measures (P values > .15). There was no significant between-group difference in change in SEQ (F1,18 = 0.53; P = .48; Table 3). Eighty-nine percent of FBK participants (24/27) and 82% of CON participants (23/28) reported that rehabilitation goals were fully achieved. One participant (CON) reported that rehabilitation goals were not completed; the remaining participants (3 FBK, 4 CON) reported that rehabilitation goals were partially achieved. There was no significant between-group difference in goal attainment (P = .56).
Laboratory Assessment of Walking and Stroke Self-Efficacy a .
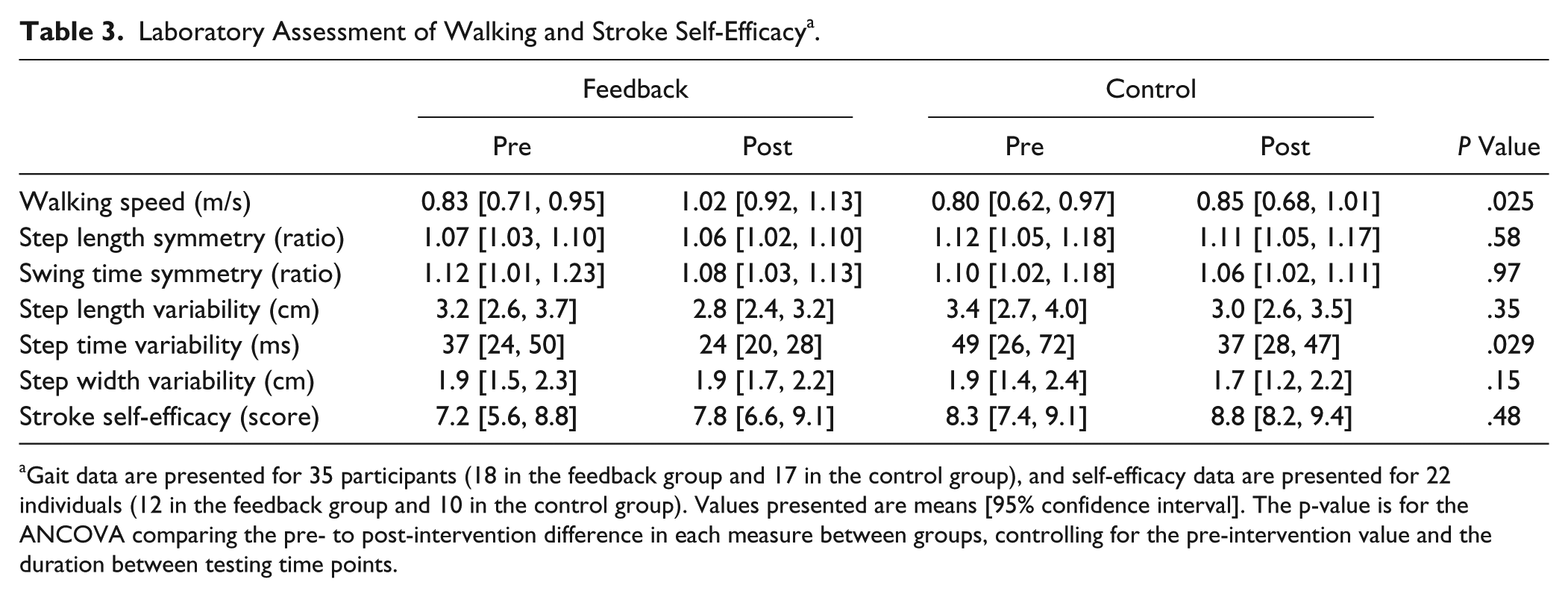
Gait data are presented for 35 participants (18 in the feedback group and 17 in the control group), and self-efficacy data are presented for 22 individuals (12 in the feedback group and 10 in the control group). Values presented are means [95% confidence interval]. The p-value is for the ANCOVA comparing the pre- to post-intervention difference in each measure between groups, controlling for the pre-intervention value and the duration between testing time points.
Discussion
This study aimed to determine if incorporating accelerometer-based feedback about daily walking into patients’ rehabilitation goal-setting process would increase the amount and influence characteristics of daily walking activity, thereby improving walking outcomes among individuals attending inpatient stroke rehabilitation. The hypothesis regarding amount of walking was not supported; there was no greater increase in daily walking activity for individuals whose physiotherapists received feedback than those who did not. However, one feature of daily walking did improve with feedback—average cadence. We interpret the increase in cadence to mean that daily walking was faster (ie, more intense) when feedback was received. Indeed, because the ratio between cadence and step length tends to be consistent at various walking speeds,32,33 the modest increase in cadence of daily walking (6%) likely meant that walking speed was even further increased (ie, by ~12%). Individuals attending inpatient stroke rehabilitation may have limited capacity to increase overall walking time for various reasons, including limited space or suboptimal environmental layout, 11 stroke-related motor impairments, 34 low endurance 15 or fatigue, and limited time due to a busy therapy schedule. However, this work suggests that the intensity (speed of walking) can be increased.
Increased cadence of daily walking appeared to translate to faster in-laboratory walking speed. The FBK group more clearly transitioned from walking speeds typical of “limited community ambulation” (0.4-0.8 m/s) to those of “full community ambulation” (>0.8 m/s). 35 This finding is clinically meaningful as individuals with stroke with gait velocity gains that result in transition to a higher walking speed classification have better function and quality of life than those who do not. 36 Physiotherapists typically provided feedback to participants regarding amount of walking to encourage more walking and rarely referred to cadence. Despite lack of attention to cadence, participants increased intensity of daily walking. A specific focus on cadence could lead to even further increases in daily walking intensity and walking speed. 37 The only other feature of walking control to improve more in the FBK group than the CON group was step time variability, which implies a more consistent cadence and possibly improved stability. 38 These results support specificity of practice; that is, increased intensity of daily walking seemed to lead to greater improvements in walking speed,39,40 but not other features of walking, such as symmetry.
Participants took, on average, 5000 steps/day; this is similar to some studies reporting walking activity in inpatient stroke rehabilitation (~5500 steps/day
12
) but much higher than others (<3000 steps/day11,41). Therefore, it is possible that many participants had little room for improvement, which may partially explain the negative findings for overall walking activity. When comparing activity data between studies, it is important to note that many authors do not identify the daily monitoring duration.12,41 In the current study, we monitored participants for all waking hours—typically at least 12 hours per day—and observed that participants were often active in the evenings. Lower step counts in previous studies could be partially due to only observing participants during “work hours” (eg, 9
There were no between-group differences in goal attainment or change in stroke self-efficacy. The large majority of participants in both groups (>80%) reported that rehabilitation goals were achieved. Thus, it is possible that these measures are not sensitive enough to detect between-group differences with the current sample size.
This study is limited by between-participant variability in intervention duration and method of delivery. The goal-setting process, including feedback and appraisal, was delivered by participants’ physiotherapists, who may have been inconsistent in the manner in which feedback was provided and in how goals were progressed. Additionally, feedback was provided from the time participants achieved independent ambulation until discharge from inpatient rehabilitation. Some participants had very few days of monitoring (<1 week), and those with longer lengths of stay may have had more time to benefit from feedback. However, these inconsistencies reflect the reality of implementation of this type of intervention in clinical practice. Thus, it is reasonable to expect that the effects observed in this study would also be observed on clinical implementation. Our ability to detect changes in walking activity is potentially limited by error in the estimate of baseline activity; due to a short length of stay for many participants, we relied on a single day to measure baseline walking activity.
To conclude, this study found that incorporating accelerometer-based feedback of daily walking activity into the goal-setting process of individuals attending inpatient stroke rehabilitation increased intensity (ie, average cadence, indicating increased speed of daily walking) but not overall amount of daily walking. Increased intensity of daily walking appeared to translate to increases in self-selected walking speeds. Additional feedback (eg, related to gait symmetry) could improve other gait characteristics.
Footnotes
Appendix
Acknowledgements
We would like to thank Akshay Parelkar, Lou Biasin, Jeremy Griffiths, Janice Komar, and Jackie Lymburner for assistance with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was generously funded by a grant from the Ontario Ministry of Health and Long-Term Care, administered and supported by the Ontario Stroke Network (OSN1101-000149). Equipment and space have been funded with grants from the Canada Foundation for Innovation, Ontario Innovation Trust, and the Ministry of Research and Innovation. At the time of this study, Elizabeth Inness was supported by a Canadian Institutes of Health Research fellowship. The views expressed do not necessarily reflect those of the funders.