
Abstract
Background. Falls are common and disabling in people with Parkinson’s disease (PD). There is a need to quantify the effects of movement rehabilitation on falls in PD. Objective. To evaluate 2 physical therapy interventions in reducing falls in PD. Methods. We randomized 210 people with PD to 3 groups: progressive resistance strength training coupled with falls prevention education, movement strategy training combined with falls prevention education, and life-skills information (control). All received 8 weeks of out-patient therapy once per week and a structured home program. The primary end point was the falls rate, recorded prospectively over a 12 month period, starting from the completion of the intervention. Secondary outcomes were walking speed, disability, and quality of life. Results. A total of 1547 falls were reported for the trial. The falls rate was higher in the control group compared with the groups that received strength training or strategy training. There were 193 falls for the progressive resistance strength training group, 441 for the movement strategy group and 913 for the control group. The strength training group had 84.9% fewer falls than controls (incidence rate ratio [IRR] = 0.151, 95% CI 0.071-0.322, P < .001). The movement strategy training group had 61.5% fewer falls than controls (IRR = 0.385, 95% CI 0.184-0.808, P = .012). Disability scores improved in the intervention groups following therapy while deteriorating in the control group. Conclusions. Rehabilitation combining falls prevention education with strength training or movement strategy training reduces the rate of falls in people with mild to moderately severe PD and is feasible.
Keywords
Introduction
Falls are both common and disabling in people with Parkinson’s disease (PD), with more than half of the people with this progressive neurological condition reporting a fall each year.1,2 Rehabilitation interventions such as movement strategy training (MST) and progressive resistance strength training (PRST) are routinely used alongside pharmacological management to prevent falls and improve mobility.3-8 There is accumulating evidence from large randomized controlled PD trials to show that physical therapy interventions can be effective for some individuals in the short term. Community-based strength and fitness programs, 6 auditory cueing from metronomes, and visual cues,7,8 combined therapy programs that incorporate cues, stretches, functional training, gait and balance training, and relaxation exercises 3 have all been found to be effective for improving movement. Despite their widespread use, there remains a need to establish the effects on falls of movement strategies and strength training coupled with falls education compared with control interventions.
Falls in people with PD have not previously been quantified over a 12-month period posttherapy using falls calendars, which is the gold standard. 9 There has been limited formal analysis of the outcomes of providing outpatient rehabilitation for falls prevention in people with PD. 10 This is important given the debilitating effects of falls on confidence, 11 activity levels,12,13 and quality of life. 14
We conducted a large, 3 group randomized controlled clinical trial across 4 sites to determine the outcomes of 2 rehabilitation interventions (MST and PRST) combined with falls prevention education compared with a control intervention to prevent falls and improve mobility in PD. The primary aim was to determine the effects of PRST or MST compared with a life skills (LS) control group on the falls rate recorded prospectively over a 12-month period in community-dwelling people with idiopathic PD. Secondary aims were to examine the effects of strength training or strategy training on mobility, disability and quality of life. The main hypothesis was that falls rates in the PRST and MST groups would be significantly lower over a 12-month period than for the control group. We also hypothesized that walking speed, performance on the Timed Up and Go test (TUG), performance on the motor and ADL sections of the Unified Parkinson’s Disease Rating Scale (UPDRS), and quality of life would be better in the MST and PRST groups compared with the LS group at 3 and 12 months after therapy.
Methods
Study Design
A single-blind, parallel group randomized controlled clinical trial was conducted between September 2006 and December 2010. Both intervention arms included falls education alongside therapy given that falls prevention is an integral component of therapy management plans. Ethics approval was obtained from the University of Melbourne (0828579) and all participants provided written informed consent. The trial was registered on the Australian and New Zealand Clinical Trials Registry (ACTRN12606000344594).
Participants, Screening, and Randomization
Recruitment details, inclusion and exclusion criteria, and procedures and the full protocol have been previously published.15-17 Patients were recruited from PD support groups, neurologists, medical practitioners, movement disorders clinics, and by advertisements in PD Association newsletters. Inclusion criteria were a Mini Mental State Examination (MMSE) 18 score greater or equal to 24, Hoehn and Yahr stage 19 less than 5, a diagnosis of PD confirmed by a medical practitioner, and being medically able and safe to perform the interventions. People who had received deep brain stimulation were excluded from the study.
After screening for eligibility and providing informed consent, participants were randomized to 1 of 3 groups, PRST, MST, or the LS control group. An independent external organization performed block randomization with fixed block sizes of 12 with a 1:1:1 allocation using a computer-generated random allocation sequence with sequentially numbered envelopes and concealment of the sequence until interventions were assigned. Participants were notified of their group allocation and enrolled by a research assistant who was not informed of the trial aims and did not provide therapy or testing. All therapists who performed assessments were kept blind to group allocation. Therapists delivering interventions did not assess participants or record outcome measures. Investigators, assessors, and staff were not aware of the trial results until all participants completed the trial.
Assessment and Interventions
Participants were in the trial for 14 months, including an initial 8 weeks of intervention, followed by 12 months of ongoing falls measurement. They were measured at baseline, after 8 weeks of therapy and at 3 months and 12 months after therapy. Experienced physiotherapists responsible for recording outcome measures received the same standardized training and assessed according to a defined protocol. The UPDRS and all other assessments were performed by registered physiotherapists who were blinded assessors. They were fully trained in the use of the UPDRS and other assessment tools. The assessment and intervention sessions were conducted at outpatient departments in 4 rehabilitation centers in metropolitan Melbourne, Australia. Participants attended the center that was convenient for them and received transport assistance as required.
Therapists conducting the interventions were trained in trial protocols at 3 training workshops and by one-to-one instruction. 16 The 2-hour therapy sessions were held once weekly for 8 consecutive weeks. The intervention groups, but not the control group, received education focused on falls risk and prevention at the commencement of each session, based on the content of Don’t Fall for It. Falls Can Be Prevented. 20 A single home visit conducted by an experienced therapist or nurse ensured that home exercises were performed safely and according to protocols, and constituted a routine check for the LS group. All participants continued with their usual care and activities during the trial. The participants were not restricted from undertaking any strength training or exercise classes outside of the research study during the follow-up period. During the intervention phase, participants recorded home exercises performed, all falls, adverse events, including exercise-related soreness, and any associated health service use as a result of exercise sessions or falls. 16 In the period after the intervention participants were instructed to participate in their usual care activities and they did not receive strength training or strategy training classes.
Based on contemporary practice in Australia we chose to focus on PRST and MST as the active interventions, selecting these from the broad range of physiotherapy interventions, such a Tai Chi, hydrotherapy, treadmill training and yoga. The selected interventions reflected most closely contemporary rehabilitation methods for Parkinson’s disease in Australia at the time of testing.
Progressive Resistance Strength Training
The PRST group performed set functional resistance exercises individualized and supervised by a registered physiotherapist. 15 When the perceived exertion of participants dropped below the required level (≈5) on the Modified Perceived Exertion scale, 21 exercises were progressed by increasing: repetitions to a maximum of 15; sets to a maximum of 3; or weights by 2% of the person’s body weight. Resistance was provided by weighted vests, Thera-Band (Hygenic Corp, Akron, OH) or body weight. Tasks were progressed by increasing repetitions and sets, and by adjusting the difficulty of the task. 16
At the commencement of each session, the participants were monitored for health changes or new muscle soreness since the last session and the program was adjusted as appropriate. A home program was prescribed each week, with photographs of each exercise, a gym step, vest with weights, and Thera-Band supplied for home use. The progressive resistance strength training group had 1 home exercise program per week in addition to the clinic-based therapy sessions. The home program sessions closely matched the content and duration of the outpatient therapy sessions.
Movement Strategy Training
The MST sessions included strategies to prevent falls, improve mobility and balance during functional tasks, such as transfers, according to rehabilitation guidelines in Morris et al. 15 Participants practiced strategies using attention, mental rehearsal and visualization of the movement, verbal cues, rhythmical cues, and visual cues under supervision of the therapist, family member, carer, or independently at home, as detailed previously. 15 Participants practiced strategies at home once a week using home exercise sheets and booklets with photos of exercises and strategies. The home program sessions were very similar to the content and duration of the outpatient therapy sessions.
Control Group: Life Skills Program
Physiotherapists, occupational therapists, speech pathologists, or social workers conducted the life-skill sessions. These included social activities, practical advice, information sessions and group discussions but not any content related to falls or mobility.15-17 The home programs comprised similar life skill activities using brochures, DVDs, booklets, and audiotapes for 2 hours each week.
Outcome Measures
The primary end point was the falls rate, recorded prospectively over a 12-month period, starting from the completion of the intervention. The falling rate refers to the number of falls per person over the period of time they remained in the study (exposure). The number of falls was calculated from the end of the intervention period to 12 months later (or to the last day in the trial if the participant did not complete the entire trial). A fall was defined as “an unexpected event resulting in the person coming to rest on the ground, floor or lower level.” 9 An investigator instructed participants on the definition of a fall and the procedures for recording and reporting falls at their first intervention session. The definition of a fall was printed on all falls calendars to help remind participants. Details of falls were taken from structured interviews with participants who telephoned our falls hotline and from monthly falls calendars. Calendars were returned at the end of each month and outstanding calendars were followed up by telephone. Falls were also monitored during the 8 week intervention phase, using the falls calendars; however, they were not included in the falls rate calculation but monitored to track the safety of the interventions. 16
Secondary outcome measures were obtained at baseline and at 3 months and 12 months after therapy by trained assessors blinded to group allocation. They included disability (UPDRS motor and ADL sections), 22 mobility (speed calculated from the 6-m walk test, 23 and time taken to perform the TUG test 24 at self-selected speed with time measured using a stop watch); changes in PD-related quality of life using the PDQ39 25 and health-related quality of life using the visual analogue scale (VAS) of the Euroqol-5D; 26 the number of injurious falls (a fall resulting in the person attending a health service); and time to first fall. The 6-m walk test was chosen because it is a reliable measure of motor performance and discriminates change over time in neurological patients. 15 The TUG was chosen because it incorporates walking and turning, which is important given that PD patients have particular difficulty with complex motor skills and dual tasking. If participants experienced freezing of gait during testing, but were able to complete the test without assistance, the tasks were timed as per protocol. Two quality-of-life tools were chosen as one represents a disease-specific measure (PDQ39), useful for comparison with other PD studies, and the other represents a generic health-related quality-of-life tool, (VAS of the Euroqol-5D).
Statistical Analysis
Calculations for sample size were based on falls and mobility effect sizes from previous studies in people with and without PD.27-29 An a priori sample size calculation, based on 60% falls in the control group, a 20% difference in the proportion of fallers between the three groups, a 15% dropout rate, 80% power, and a significance level of 5%, initially indicated that we needed 330 participants (110 per group).
All analyses were carried out using the intention-to-treat principle. Descriptive statistics were used to report demographics. Negative binomial regression was used to estimate the difference in falls rate between the control group and each intervention group by analyzing the number of falls per participant, adjusting for varying duration of follow-up. 30 The falling rate refers to the number of falls per person over the period of time they remained in the study (ie, exposure). For example, a participant who completed the entire study would have an exposure of 12 months, whereas a person who withdrew after 6 months would only have an exposure of 6 months. This type of analysis therefore allows falling rates to be documented for participants with partial follow-up data. We also compared the continuously scored secondary outcome measures using the linear regression approach to analysis of covariance, with baseline scores entered as independent covariates. 31 Missing secondary outcome data were imputed with 5 iterations using baseline scores and group allocation as predictors. SPSS version 20.0 (IBM, Armonk, NY) and STATA 11 (Stata Corp, College Station, TX) were used for the statistical analyses.
There were 2 variations to the original protocol. The design planned for participants to be treated in groups of 4. This was not always feasible in the outpatient clinics and participants were treated in groups of 3 to 6. Although we originally estimated that we would require 330 participants this was based on existing information at that time from small clinical trials. An interim analysis by an independent data monitoring committee after 180 participants had been randomized showed that falls were higher than anticipated and there were more falls in the control group compared to the intervention groups (P < .001). Therefore we considered full recruitment not to be necessary 32 and revised our sample size. This was revised to 210 (approximately 70 participants per group) as additional participants had already been recruited and randomized during the period of time needed to review the interim data. Although we believe the revised sample size was justified, we acknowledge that trials that are stopped early may sometimes overestimate treatment effects. 33
Results
In all, 210 participants were randomized to 1 of 3 groups (Figure 1). One participant allocated to the MST group and 6 in the LS control group did not receive any intervention. Three participants in the PRST group, 2 in the MST group, and 8 in the control group did not complete the 12-month follow-up for secondary outcome measures.
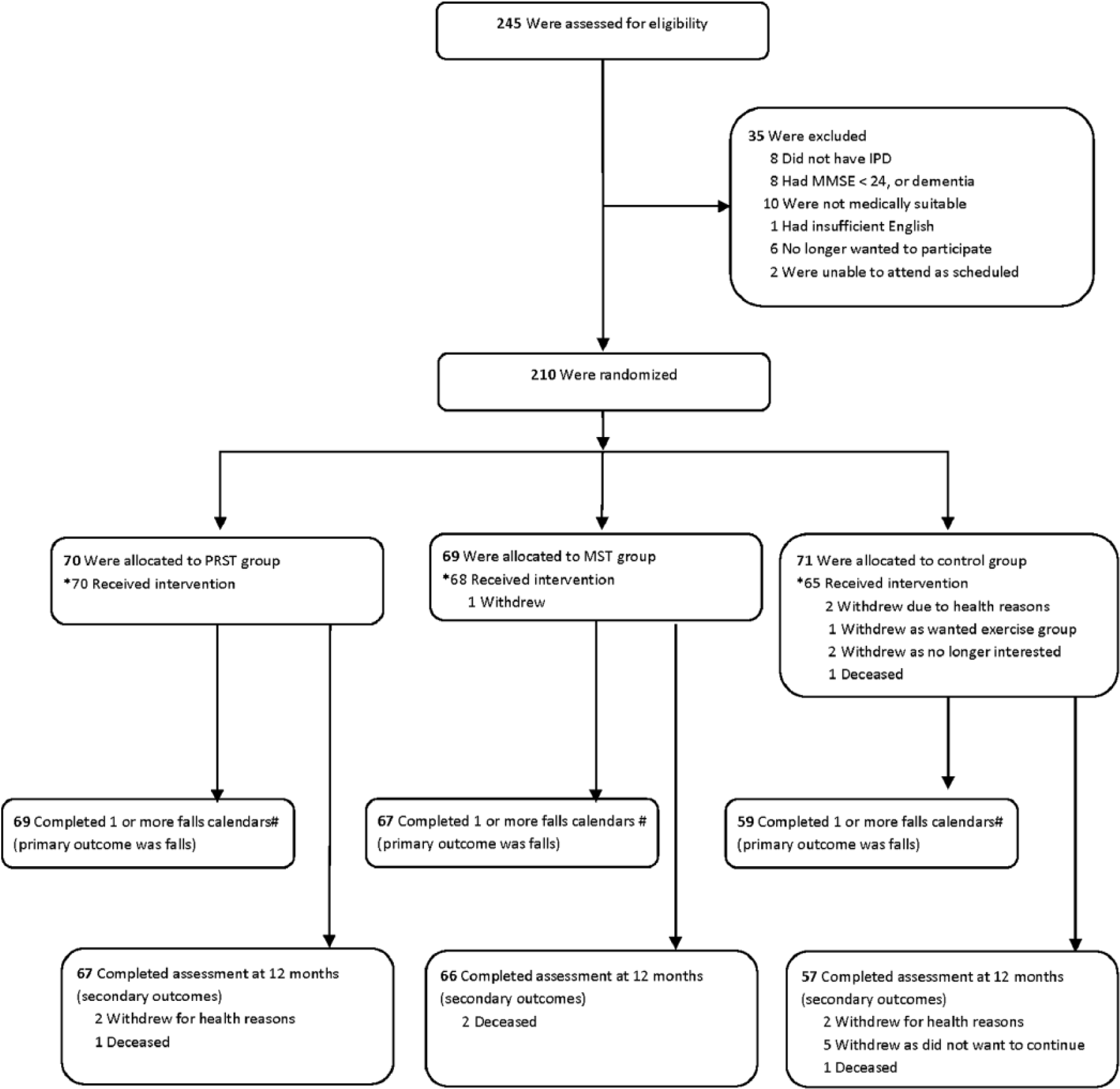
Flow of participants through the trial.
Baseline Characteristics
Baseline characteristics and comorbidities are presented in Table 1. The 140 men and 70 women had a mean age of 67.9 years (range 44-89 years). More than 58% of participants had comparatively mild PD, modified Hoehn and Yahr stage 1 to 2.5, whereas 41% had moderate to severe disease, stage 3 to 4. There were marginally more subjects with a modified Hoehn and Yahr score at stage 3 to 4 in the LS group compared with the intervention groups, yet this was not statistically significant. Hence it is unlikely that a difference in PD severity contributed to more frequent falls in the follow-up periods for participants in the life-skills group. Most were taking either levodopa preparations or a combination of PD medications, with 19 reporting they had not commenced pharmacological therapy for PD. More than 50% of participants reported previously experiencing freezing of gait.
Participant Characteristics at Baseline.
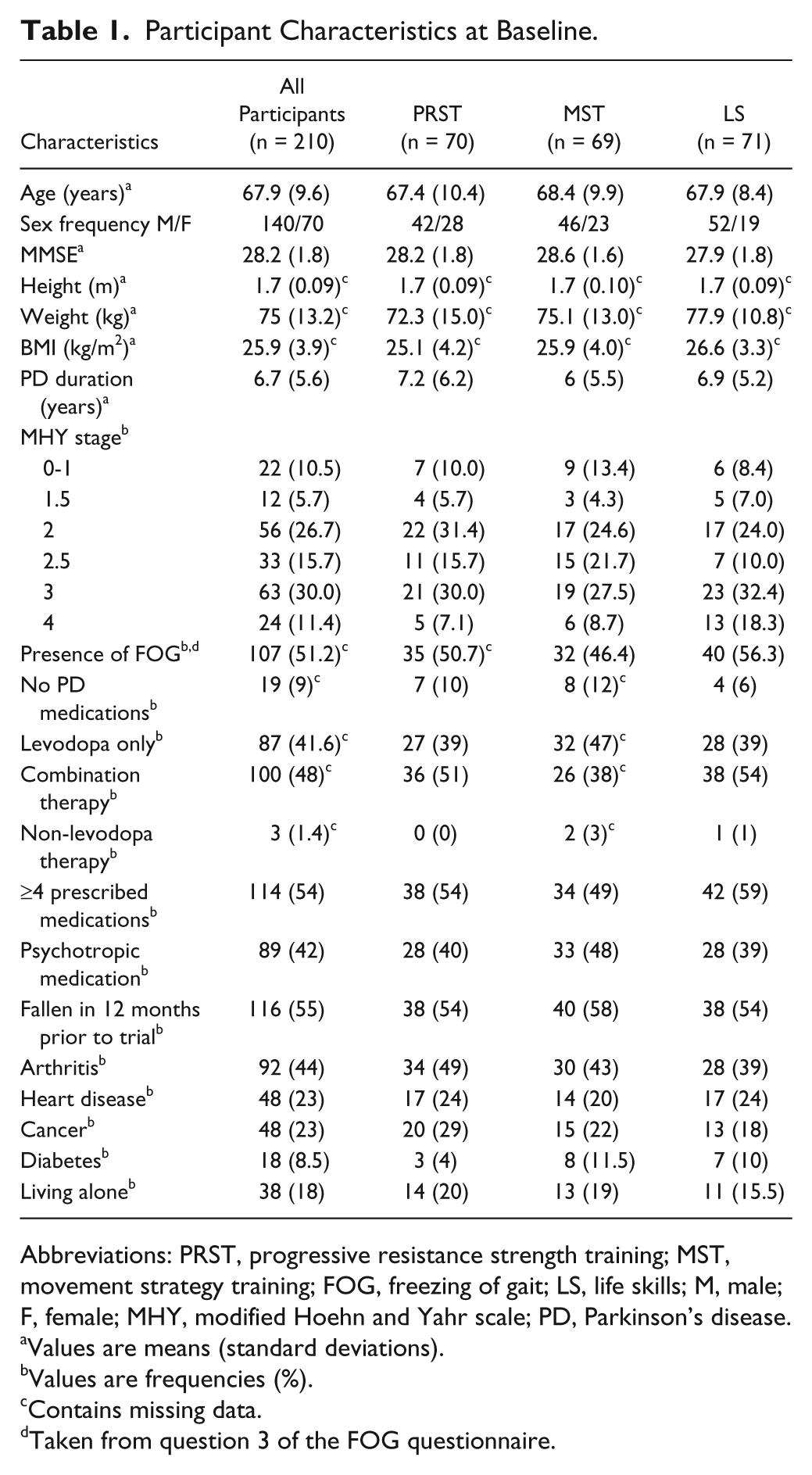
Abbreviations: PRST, progressive resistance strength training; MST, movement strategy training; FOG, freezing of gait; LS, life skills; M, male; F, female; MHY, modified Hoehn and Yahr scale; PD, Parkinson’s disease.
Values are means (standard deviations).
Values are frequencies (%).
Contains missing data.
Taken from question 3 of the FOG questionnaire.
Falls Rates During 12-Month Follow-up Period
We received falls calendars from 195 participants after the intervention period with 184 participants returning calendars for the full 12 months. The falls rates are summarized in Table 2. 1547 falls were reported over the 12-month period; 193 for the progressive resistance strength training group, 441 for the movement strategy group and 913 for the control group. The strength training group had 85% fewer falls than controls (incidence rate ratio [IRR] = 0.151, 95% CI 0.071-0.322, P < .001). The movement strategy training group had 61.5% fewer falls than controls (IRR = 0.385, 95% CI 0.184-0.808, P = .012). There were no differences in the proportion of multiple fallers between groups. Of the 195 people who returned their falls calendars, 142 fell more than once in 12 months; and 86 people were multiple fallers who fell more than 2 times per annum.
Falls Rate, Proportions of Fallers, and Multiple Fallers per Person by Treatment Group.
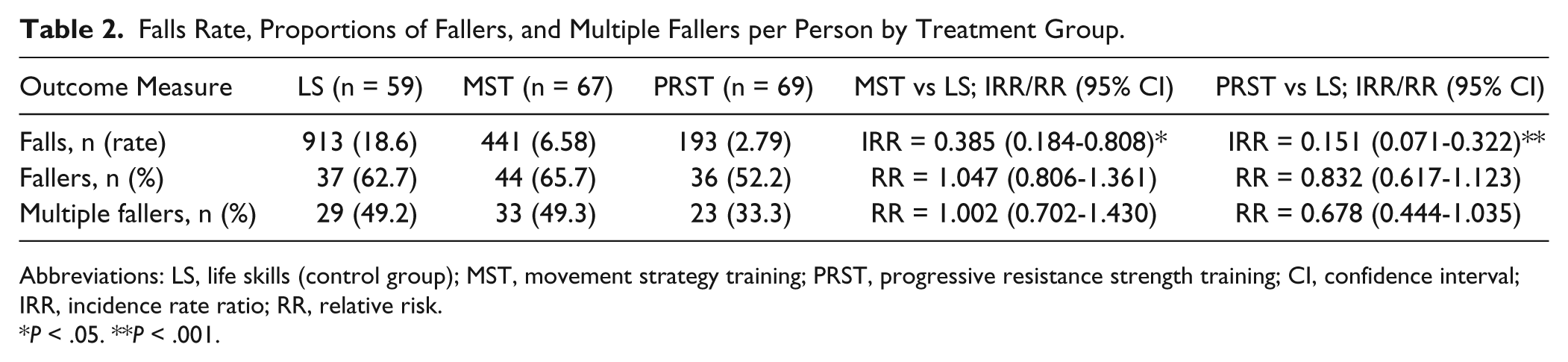
Abbreviations: LS, life skills (control group); MST, movement strategy training; PRST, progressive resistance strength training; CI, confidence interval; IRR, incidence rate ratio; RR, relative risk.
P < .05. **P < .001.
The time to first fall did not differ between the intervention groups and controls (log rank test (Mantel-Cox), χ2 = 2.08, df = 2, P = .35). A total of 44 injurious falls, defined as attending a health service as a result of the fall, were reported by 33 participants: 11 participants in the PRST group, 12 in the MST group, and 10 in the control group. Fractures occurred as a result of a fall in 8 participants; 3 participants in each of the PRST and MST groups and 2 in the LS control group. Falls resulted in 16 participants (6 from the PRST group and 5 each from the MST and control groups) being taken to hospital, with 6 being admitted for at least one night. Local doctors were consulted by 25 participants on 28 occasions following a fall.
Disability, Walking Speed, and Quality of Life
Table 3 reports baseline and 3- and 12-month postintervention measures of disability (UPDRS sections II and III), health related quality of life (PDQ39, Euroqol-5D VAS), walking speed derived from the 6-m walk test, and time taken to perform the TUG for the 3 groups. For the 12-month follow-up test, the PRST and MST groups had greater improvements in their UPDRS activities of daily living scores compared with the life skills group (P < .01 and P < .01, respectively). Over the 12-month follow-up the MST group had greater improvement in the UPDRS motor score compared with the LS group (P = .017). There were no differences between groups for change in walking speed, the TUG or quality-of-life measures from baseline to 12 months, with the exception of a greater improvement in PDQ39 score in the PRST group compared with the LS group (P < .05).
Secondary Outcome Measures at Baseline, 3-Month, and 12-Month Follow-up. a
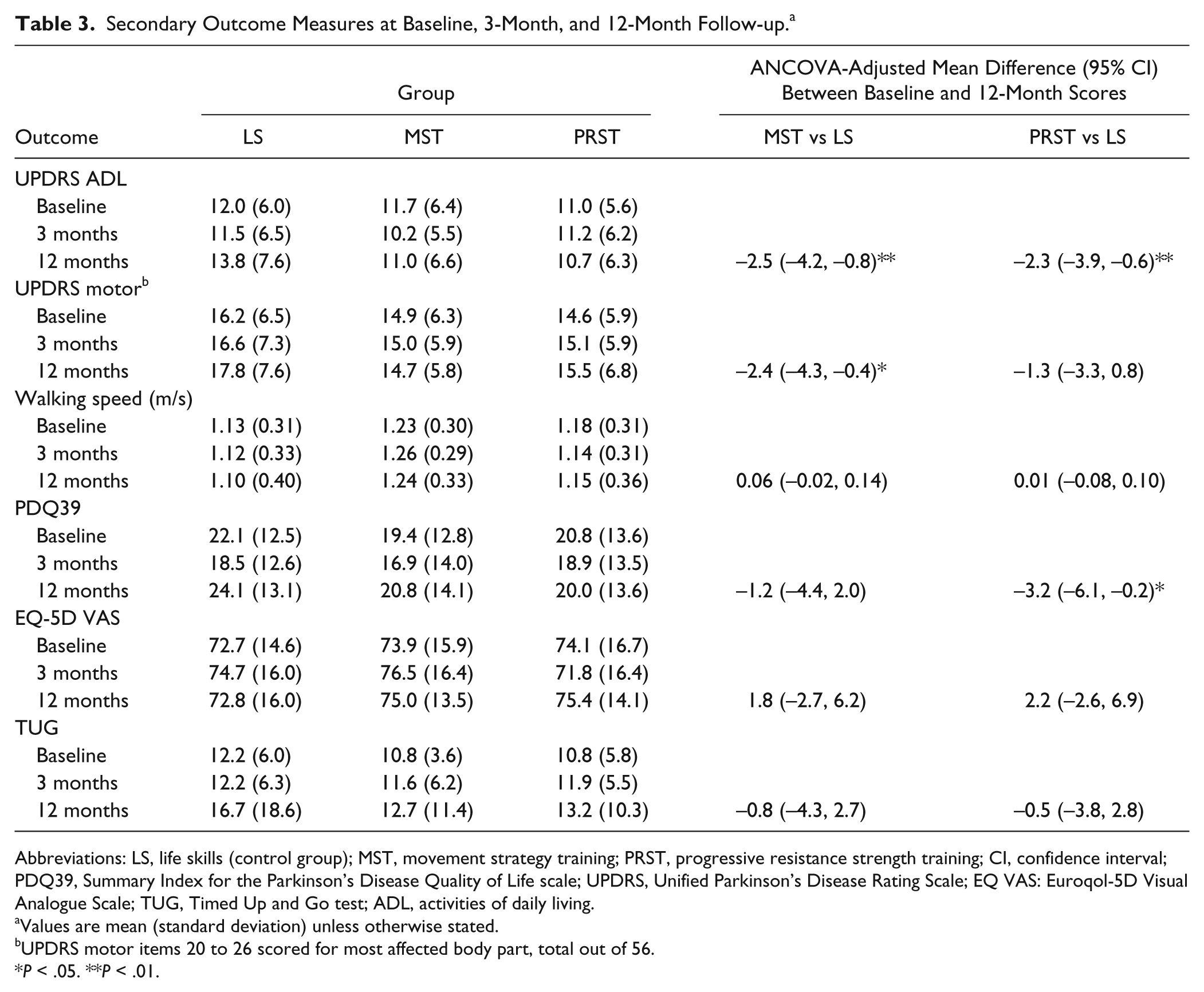
Abbreviations: LS, life skills (control group); MST, movement strategy training; PRST, progressive resistance strength training; CI, confidence interval; PDQ39, Summary Index for the Parkinson’s Disease Quality of Life scale; UPDRS, Unified Parkinson’s Disease Rating Scale; EQ VAS: Euroqol-5D Visual Analogue Scale; TUG, Timed Up and Go test; ADL, activities of daily living.
Values are mean (standard deviation) unless otherwise stated.
UPDRS motor items 20 to 26 scored for most affected body part, total out of 56.
P < .05. **P < .01.
Drop out in the control group was higher than for the therapy groups. Six control subjects did not receive the intervention compared to one withdrawal from the MST group. Of those who received the intervention, 6 control subjects did not complete one or more fall calendars compared with one in each of the physiotherapy arms.
No serious adverse effects or important harms were reported and there were no unintended effects in any of the groups. A previous publication 16 provides details of the safety, feasibility, and compliance with MST and PRST in this sample. Adherence to all sessions was excellent, with 90% of participants attending 6 or more of the 8 scheduled sessions. Participant attendance (as defined by attendance at ≥6 sessions) did not differ across the 3 groups.
Discussion
This trial provides evidence that rehabilitation in addition to usual care is effective for reducing falls and disability in community-dwelling people living with PD. The falls rate was higher in the control group compared with the groups that received strength or strategy training. When coupled with falls prevention education, strength training resulted in 85% fewer falls compared with a control group. This concurs with recent findings on strength training in PD and elderly samples.5,34 When delivered in conjunction with falls prevention education, movement strategy training incorporating cueing, attention strategies, segmentation, and mental rehearsal resulted in 62% fewer falls than for the control group.
When combined with a falls education program, both strategy training and strength training were associated with reductions in disability over the 12-month follow-up. The UPDRS activities of daily living score changed positively (lower scores) in the 2 intervention groups over the 12-month follow-up, in contrast with the control group, where the change in score was negative. For the MST group the UPDRS motor score also changed positively after therapy. Surprisingly, there were no differences between groups for change in walking speed, the TUG or quality-of-life measures from baseline to 12 months. This raises questions about the likely mechanisms associated with reduced falls rates, suggesting that interventions that focus on functional task performance might be particularly helpful.
Although this study did not set out to directly examine neural correlates associated with motor performance gains, it could be speculated that movement strategy training and strength training impact central motor control mechanisms in PD. In turn, this might have reduced the rate of falling through more optimal motor performance. Laboratory studies have shown that attention to visual and auditory cues and strategies that focus on large amplitude movements enable people with PD to bypass the defective basal ganglia and to use frontal cortical mechanisms to control movements. 35 This could be associated with fewer falls due to an improved ability to walk with larger steps, avoid obstacles and respond to perturbations to the center of mass. Previous studies have also shown that progressive resistance strength training enables people with PD to optimize peripheral motor control mechanisms to increase strength and power generation. 36 Moreover, Morberg et al 37 demonstrated that in a sample of PD fallers there were strength impairments arising from central motor control mechanisms rather than simply peripheral muscle contractile capacity. They speculated that progressive strengthening might increase neural drive, reduce abnormal movements and consequently diminish falls risk.
Many people living with PD are deconditioned due to low habitual physical activity, especially older adults, hence it is not surprising that our rehabilitation program was associated with improved outcomes, either due to strengthening or by more effective cortical processing through progressive resistance or the use of attentional strategies.36,37 One possibility is that movement rehabilitation interventions such as these increase brain neurotrophic factors associated with amelioration of Parkinson’s signs, as shown in a preliminary trial by Frazzitta et al. 38 Such findings need to be verified in large scale RCTs including patients with a range of levels of disease severity.
In keeping with previous prospective PD studies1,4 falls occurred frequently over the 12-month period in our sample. Overall, 60% of participants fell at least once, which was a little lower than reported by Wood et al 39 (68.3%). Nevertheless Wood et al 39 aimed to examine factors that predicted future falls whereas the present study aimed to examine the effectiveness of training interventions. It is likely that both movement strategy and strength training interventions lessened the rate of falls in our study population. Of the 195 who returned their falls calendars, 44% were multiple fallers, who fell more than 2 times per annum. Of those who fell, 73% fell more than once in 12 months. Multiple factors have been associated with recurrent falls in people with PD, with strong predictors, including previous falls,40,41 disability as measured by Hoehn and Yahr stage, and the UPDRS. 11
Of the 1547 falls reported, 44 required medical attention. Sixteen of these required hospital attendance. Although a high rate of soft tissue injury has frequently been reported following falls in people with PD,39,41 the incidence of serious injury and particularly fractures appears from prospective studies such as ours and others39,42,43 to be lower than for earlier retrospective trials. 44 This could possibly relate to the specific elements of treatment provided. The observation that the reduction in falls did not translate into a reduction in injurious falls was surprising. This reinforces the need for a multifaceted falls prevention approach as discussed by Morris. 45
There were some limitations of this trial. First, all patients were treated and tested during the “on” phase of their medications and the effects of therapy when “off” awaits confirmation. Second, it is possible that the allocation of a very frequent faller could have a disproportionate influence on the falls rate. However, as participants were randomized to groups, it can be assumed that the baseline physiological risk of falling was equivalent between groups. Third, because both rehabilitation interventions were accompanied by falls education training, future research will be necessary to elucidate the amount of benefit received from the separate components of intervention. Fourth, the trial was not powered to perform a between-group comparison of the improvements induced by the two active interventions and future trials will be needed to answer this question. Fifth, there was a higher rate of drop outs in the control group that could be a potential source of bias, especially given that participants knew their group assignment. Sixth, the results of this trial are generalizable to people with mild to moderately severe idiopathic Parkinson’s disease. They may not necessarily be applicable to those with end-stage disease or those with cognitive impairment. Finally, it would be useful for future trials to measure muscle strength.
To conclude, outpatient rehabilitation incorporating strength training or movement strategy training and falls education was found to be effective in reducing falls and was a feasible adjunct to medical management to reduce falls and improve mobility in people with PD.
Footnotes
Acknowledgements
We would like to acknowledge and thank the participants and their families for their participation and support. We also acknowledge the enthusiasm and support provided by the blinded assessors and by the therapists who implemented the 3 arms of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This trial was funded by a Michael J. Fox Foundation (US) Clinical Discovery Grant. HBM is a National Health and Medical Research Council Senior Research Fellow (ID: 1020925).