
Abstract
Background. Use of rehabilitation technology, such as (electro)mechanical devices or robotics, could partly relieve the increasing strain on stroke rehabilitation caused by an increasing prevalence of stroke. Arm support (AS) training showed improvement of unsupported arm function in chronic stroke. Objective. To examine the effect of weight-supported arm training combined with computerized exercises on arm function and capacity, compared with dose-matched conventional reach training in subacute stroke patients. Methods. In a single-blind, multicenter, randomized controlled trial, 70 subacute stroke patients received 6 weeks of training with either an AS device combined with computerized exercises or dose-matched conventional training (CON). Arm function was evaluated pretraining and posttraining by Fugl-Meyer assessment (FM), maximal reach distance, Stroke Upper Limb Capacity Scale (SULCS), and arm pain via Visual Analogue Scale, in addition to perceived motivation by Intrinsic Motivation Inventory posttraining. Results. FM and SULCS scores and reach distance improved significantly within both groups. These improvements and experienced pain did not differ between groups. The AS group reported higher interest/enjoyment during training than the CON group. Conclusions. AS training with computerized exercises is as effective as conventional therapy dedicated to the arm to improve arm function and activity in subacute stroke rehabilitation, when applied at the same dose.
Keywords
Introduction
More than 60% of stroke survivors suffering from hemiparesis have to cope with marked limitations in arm function or dexterity 6 months poststroke, often compromising activities of daily life. 1 One of the mechanisms involved is a loss of selective movement control because of involuntary coupling of shoulder abduction and elbow flexion, reducing work area. 2 There is an urgent and growing need for effective and efficient rehabilitation programs aimed at restoring hemiplegic arm function. These should ideally incorporate a high dosage and intensity, active engagement by the patient, and task-oriented exercises.3-5
Currently, intensive arm therapy is mainly provided through individual therapy (1 therapist for 1 patient) and some group training when possible. An increasingly limited availability of resources and/or personnel is one of the major barriers in providing a high dosage of therapy. In the past few decades, new technologies have emerged in the field of rehabilitation, such as (electro) mechanical devices and virtual reality, which have provided new opportunities to enhance training intensity by enabling more independent training. 6 Several studies have reported that robot-aided therapy has beneficial effects on hemiplegic arm function.7-9 However, it is unknown which aspects of robot-aided therapy contribute most to this effect. 7 Besides, uptake of electromechanical devices in clinical practice is currently limited, which is, among others, related to unfamiliarity perceived with applying such devices, experienced complexity to work with such devices, and the relatively higher costs or limited funding. 10 Therefore, dedicated, relatively simple, less-expensive alternatives can facilitate the use of such devices in rehabilitation care.
Weight support is one aspect that is common among most robots. 11 Weight support of the hemiplegic arm instantaneously results in improved selectivity of movements through a decreased coupling between shoulder abduction and elbow flexion, resulting in increased work area. 2 It also has a facilitating impact on active movements. 12 These direct effects carried over to improved unsupported arm function after training with arm support (AS) in a pilot study, 13 in which the Freebal device allowed practice of 3-dimensional movements while providing consistent AS throughout this work space. 14 Other comparable applications of weight-supported arm training in a 3-dimensional work space have resulted in comparable results in chronic stroke patients.15,16
The effect of treating hemiplegic arm function is expected to be the greatest during the subacute phase after stroke, in which the largest potential for improvement of motor function exists. 17 In addition, it is important to compare new treatment modalities with dose-matched (in terms of frequency and duration of treatment sessions) conventional training (CON) because this is a major determinant of rehabilitation outcome. 4 The current study, therefore, evaluates the effect of AS training in the subacute phase after stroke in a randomized controlled trial, comparing with dose-matched CON.
Weight-supported arm training was combined with computerized exercises with a gaming component (serious games). This is expected to increase motivation and attention, which can stimulate outcome after stroke. 18 It is hypothesized that the combination of AS and computerized exercises is at least as effective as CON in improving arm function, in which case it can pave the way for training programs that are less dependent on availability of therapists and may be more efficient.
Methods
Study Design
The study was a single-blind, multicenter, randomized controlled trial and is reported according to the CONSORT statement. 19 All individuals participated in 6 weeks of training, randomized over dedicated CON or AS training with computerized exercises. All participants were assessed within 1 week before (T0) and after (T1) the intervention period. Random allocation to the groups was performed after the pretraining measurement by an appointed coordinator at each rehabilitation center using concealed envelops, in blocks of 2 participants, to ensure a balanced number in each group.
At each participating rehabilitation center, an independent examiner was appointed, who performed all assessments in a single-blind manner. They were not involved in the allocation procedure or treatment of either the AS or CON group. Examiners were instructed about standardized performance of clinical assessments during a 1-day meeting together with the coordinating researchers. The study is registered in the Netherlands Trial Registry (NTR2539) and was approved by the local medical ethical committee. All participants gave informed consent before enrolling in the study.
Participants
A total of 70 subacute stroke participants, receiving a comprehensive program of rehabilitation care, were recruited for participation at 7 rehabilitation centers throughout the Netherlands (Roessingh rehabilitation center, Enschede; RMC Groot Klimmendaal, Arnhem; Sint Maartenskliniek, Nijmegen; de Hoogstraat, Utrecht; UMCG/Beatrixoord, Haren; Reade, Amsterdam; Rijndam rehabilitation center, Rotterdam), between November 2010 and January 2012. Based on data from a previous study in chronic stroke patients, 13 at least 17 participants per group were required for a 10% difference in the Fugl-Meyer assessment (FM) score with a power of 0.80 (2-sided α of .05).
All participants had suffered from a first ischemic or hemorrhagic stroke 1 to 12 weeks ago and had to be medically stable. Participants further had to display limited arm function but have active control of the elbow/shoulder of at least 15° and had to be free from other conditions or pain, unrelated to stroke, limiting use of the arm. They also had to be able to follow instructions and understand (and see) the visual game display. Participants who were treated with botulinum toxin and/or electrical stimulation to improve arm function before or during participation in the study were excluded.
Intervention
All individuals participated in a 6-week reach training program, consisting of 3 sessions of 30 minutes per week (18 sessions or 9 hours in total). To achieve dose matching, for both groups, 3 physical and/or occupational therapy sessions from the regular stroke rehabilitation program were replaced with either the experimental or control training each week. During 3 education sessions, 2 physical and/or occupational therapists of each clinical site were instructed on the use of the AS device and the application of either standardized training protocol.
During both AS and CON sessions, attention was given exclusively to the upper extremity, whereas other aspects (such as gait, balance, cognition, etc) were addressed in other regular therapy sessions within the rehabilitation program for both groups. It has to be noted that this caused the control intervention to be a more-intensive upper-extremity treatment than what is given regularly in most participating rehabilitation centers.
Arm Support Training
The AS device, ArmeoBoom (Hocoma AG; Volketswil, Switzerland), is based on the previously developed Freebal. 14 It has an overhead sling suspension system with low inertia to provide arm weight support at the wrist and elbow (Figure 1A). It provides consistent support within a 3-dimensional work space, allowing functional movements without restrictions. The amount of support is adaptable to varying arm weights across patients and changing motor abilities within patients over time. The ArmeoBoom device is integrated with a webcam and a laptop on which interactive computerized exercises are played by moving the affected arm in an individually adjusted 3D virtual environment (relative to each participant’s active range of motion). Hand movements in the horizontal plane were monitored via the webcam and a reflective marker on the wrist sling, which controls the cursor in the horizontal plane of the games. Movements in the vertical plane are recorded using a potentiometer measuring the rotation angle of the beam to which the wrist cable is attached, which controls displacement of the cursor in the vertical plane of the games. Points are awarded according to performance or completion time.
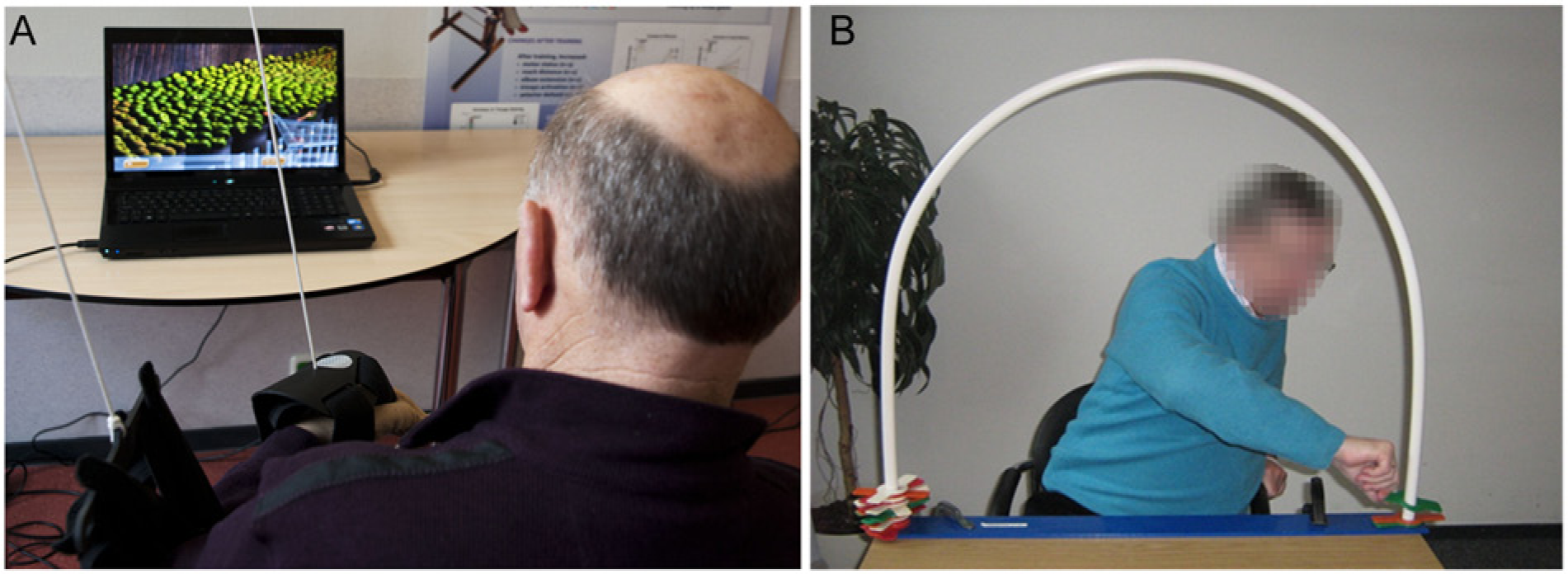
Arm support training setup (A) and example of a conventional exercise (B).
Training of the AS group consisted of playing games with the affected arm supported by the device, working toward maximizing movement ability with as little AS as possible. AS training involved mainly shoulder and elbow movements, with exercises structured according to a categorization of the games for increasing difficulty, to maintain challenge throughout training: 1D (only left/right movements), 2D (movements in horizontal or vertical plane with fixed targets) and 3D movements (movements in all directions with moving targets). In addition, for each game, 3 in-game difficulty levels could be selected (easy/medium/hard), reflecting speed and accuracy of the game. These settings were adjusted to the ability of each patient, based on a standardized protocol defined a priori in consensus with experienced therapists. The amount of AS was set in such a way that an elbow angle of 90° could be achieved (where 180° reflects a fully extended arm), and the amount of AS was reduced by one of the predefined levels on the AS levers of the device when a participant had increased elbow extension with the previous support level by 60°. Within each exercise category, reach distance, game category, and in-game difficulty level were increased subsequently.
Conventional Reach Training
Conventional reach training consisted of a standardized set of arm exercises defined in consensus with therapists to reflect regular physical and occupational therapy. Similarly to AS training, the main aim of CON training (Figure 1B) was to increase the range of motion of the arm (mainly of the shoulder and elbow) with as little support from a surface (eg, table) as possible. All exercises were analog in nature and generally required reaching for objects positioned on a table top/shelves (moving or stacking cups, placing disks, transporting blocks or pegs, etc) without the aid of mechanical supports or computerized training environments. In line with AS training, CON training was categorized with increasing difficulty: movements in 1 direction, movements in horizontal or vertical planes, more complex movements in all directions, potentially including grasp. Again, progression within each exercise category was staged according to increasing reach distance, speed, and accuracy, subsequently.
Evaluation
Assessment of arm function measures was done at T0 and T1, whereas motivation was assessed only at T1. The upper-extremity section of the FM was used to quantify upper-extremity motor function according to a standardized procedure.20,21 The FM consists of 33 items that are scored using a 3-point ordinal scale (0 = unable; 1 = partly able; 2 = fully able to complete movement) with a maximal score of 66. The scale has high intrarater reliability, interrater reliability, and construct validity and is reported to be responsive to change. 22 The minimal clinically important difference is considered to be 10% (ie, 6.6 points). 23 Besides a total FM score, separate scores were calculated for the proximal component of the FM, consisting of shoulder/elbow movements and coordination (FMprox; maximum = 42 points), and the distal component of the FM, consisting of wrist and hand movements (FMdist; maximum = 24 points).
Reach distance was measured using the AS device, with the amount of support reduced to zero while making maximal forward reaching movements with the affected arm in free space (without a table) to prevent participants from using any support. Participants started with their affected hand as close to their sternum as possible while sitting up straight with their back touching the chair. Next, they had to reach as far as possible in a forward direction in the sagittal plane at shoulder height while keeping their back against the chair. The position of the hand in the horizontal plane was determined by the AS device, using the reflective marker on the wrist sling. The position was recorded within the work space section of the software in 2 instances: holding the arm in the start position and holding the arm in the final reaching position. To compensate for differences in absolute position between participants and repeated measurements, the difference between minimal (start position) to maximal (final position) hand position was calculated to represent 2D reach distance in the horizontal plane. Values of 5 reaching movements were averaged to represent mean reach distance.
The Stroke Upper Limb Capacity Scale (SULCS) measures the capacity to perform 10 functional tasks related to daily activities (such as drinking from a glass, buttoning up a shirt, combing hair, etc). 24 Three items focus on proximal upper-limb capacity, 4 items require basic control of wrist and finger movements, and 3 items require advanced control of wrist and finger movements. The items are scored using a 2-point ordinal scale (0 = Unable; 1 = Able to perform task), resulting in a maximal score of 10. The scale has good interrater reliability and construct validity. 25
The Intrinsic Motivation Inventory (IMI) is a multidimensional questionnaire to assess subjective experience of motivation during experimental tasks, including physical activity. 26 It has been used in stroke research to assess perceived motivation during interventions, for instance virtual reality training. 27 Using a 27-item version, participants rated their experience during CON or AS training on a 7-point Likert scale (1 = Do not agree at all; 7 = Fully agree), on 5 dimensions related to motivation: interest/enjoyment, perceived competence, effort/importance, value/usefulness, and pressure/tension. The interest/enjoyment dimension is the primary self-report measure of intrinsic motivation, whereas the other dimensions are influencing factors of intrinsic motivation. 26 For each of the 6 dimensions of the IMI, the average represented the mean dimension score. The average of all dimension scores represented the overall IMI score. High scores (maximum = 7 points) indicated positive ratings for each dimension: high interest, high competence, high effort, high value, and low pressure. Scores for pressure were inverted (8 minus IMI score) to accommodate this interpretation.
To monitor whether either intervention would involve increased pain, participants were asked to mark their currently experienced pain in the arm on a Visual Analogue Scale from 0 (no pain at all) to 10 (worst possible pain). The distance from 0 cm to the mark on the line represents the VAS score.
Statistical Analysis
For all outcome measures, descriptive statistics were calculated per group. Differences between groups at baseline were tested for significance using an independent-samples t test (χ2 test for nominal parameters). A repeated-measures ANOVA was used to compare the effect of AS training on arm function with CON training. Group (between-subjects factor), Time (within-subjects factor), and Group × Time were entered into the model. Additionally, correlations between stroke severity and training-induced changes were examined in each group using Pearson’s correlation coefficient. The ordinal IMI scores were tested for differences between groups using a Mann-Whitney U test. The significance level α was set at .05 for all tests (using IBM SPSS Statistics 19).
Results
Participants
A total of 70 subacute stroke participants were included in the present study, of whom 68 completed the study protocol (Figure 2). Data of 2 participants had to be excluded from analysis because of start of electrostimulation treatment after entering into the present study, which was assigned inadvertently by physicians not directly involved in the current trial. The CON and AS groups were comparable at baseline (Table 1) with respect to age, affected side, time poststroke, and FM and SULCS scores (P ≥ .125), except for male/female distribution (P = .042). Hemiparesis in CON and AS groups was severe in 55% and 66%, moderate in 24% and 28%, and mild in 21% and 6%, respectively, according to the categorization of FM scores used by Luft et al. 28
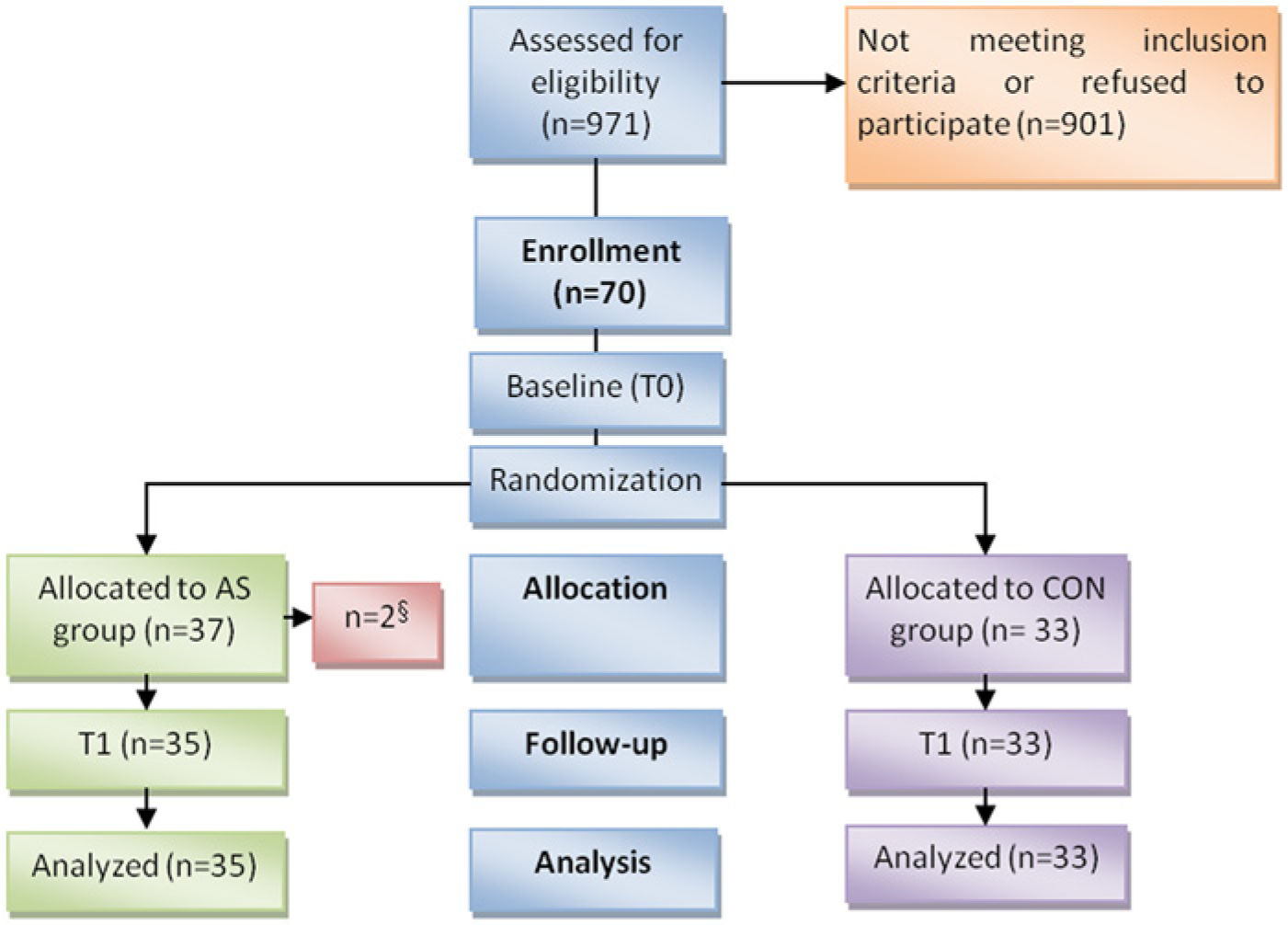
Flowchart of patients through the study.
Participant Characteristics at Baseline, by Group.
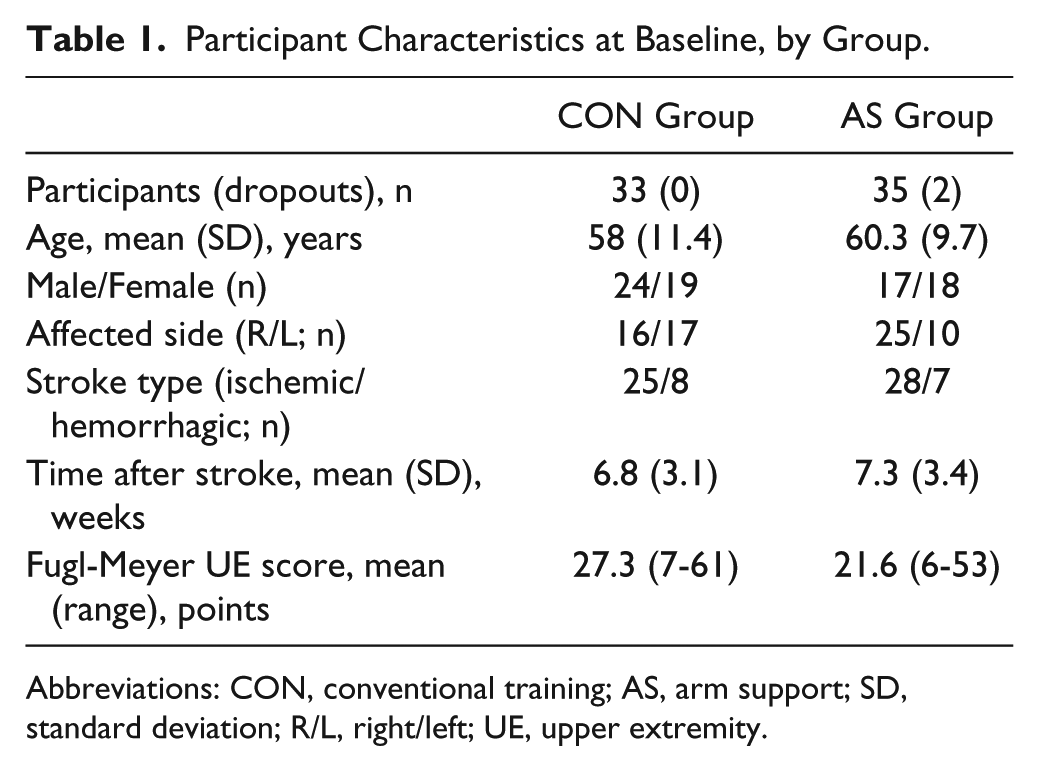
Abbreviations: CON, conventional training; AS, arm support; SD, standard deviation; R/L, right/left; UE, upper extremity.
Clinical Outcomes
VAS scores for pain were low in both CON and AS groups at T0 with 1.4 and 0.8, respectively. After 6 weeks, the mean VAS scores had increased somewhat, to 2.2 and 2.5, respectively. VAS scores did not differ between groups (P ≥ .262) either at T0 or T1.
CON and AS groups were comparable at baseline, although there was a tendency for a slightly worse motor function (FM score) in the AS group (P = .065). After training, both groups had improved significantly in both FM and SULCS (Table 2; P < .001). The average increase in FM was clinically relevant (>6.6 points) in both CON and AS groups. Individually, FM improvement achieved a minimal clinically important difference in 16 participants in the AS group and 20 participants in the CON group. Of these, 10 were severely and 6 moderately affected in both groups, in addition to 4 mildly affected participants in the CON group. Nevertheless, changes in FM were not directly correlated with (categories of) stroke severity (ρ ≤ −0.19) in either group. The changes in FM and SULCS did not differ significantly between AS and CON groups (P ≥ .312).
Changes in Arm Function Between Pretraining (T0) and Posttraining (T1) Evaluations in the CON and AS Groups (Mean ± SD).
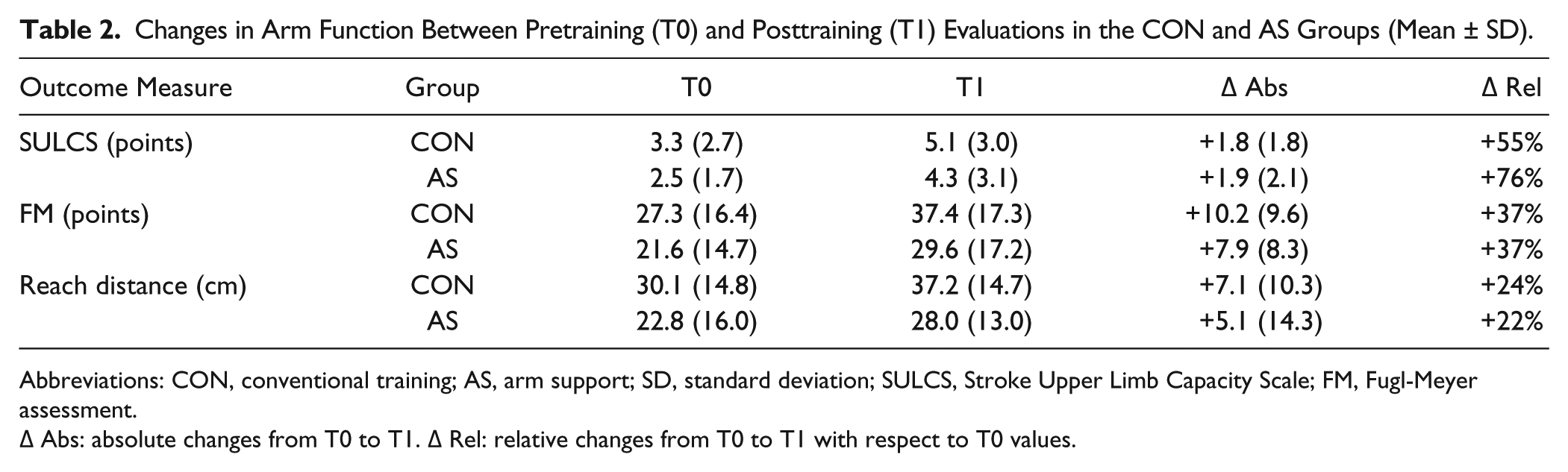
Abbreviations: CON, conventional training; AS, arm support; SD, standard deviation; SULCS, Stroke Upper Limb Capacity Scale; FM, Fugl-Meyer assessment.
Δ Abs: absolute changes from T0 to T1. Δ Rel: relative changes from T0 to T1 with respect to T0 values.
FMprox and FMdist scores were comparable (P ≥ .076) between groups at baseline (with a tendency for slightly lower proximal scores in the AS group). Again, training-induced changes in both FMprox and FMdist (Figure 3) were significant in both groups (P < .001), with no difference between CON and AS groups (P ≥ .327). This indicates that contributions of proximal and distal segments to FM improvement did not vary between groups.
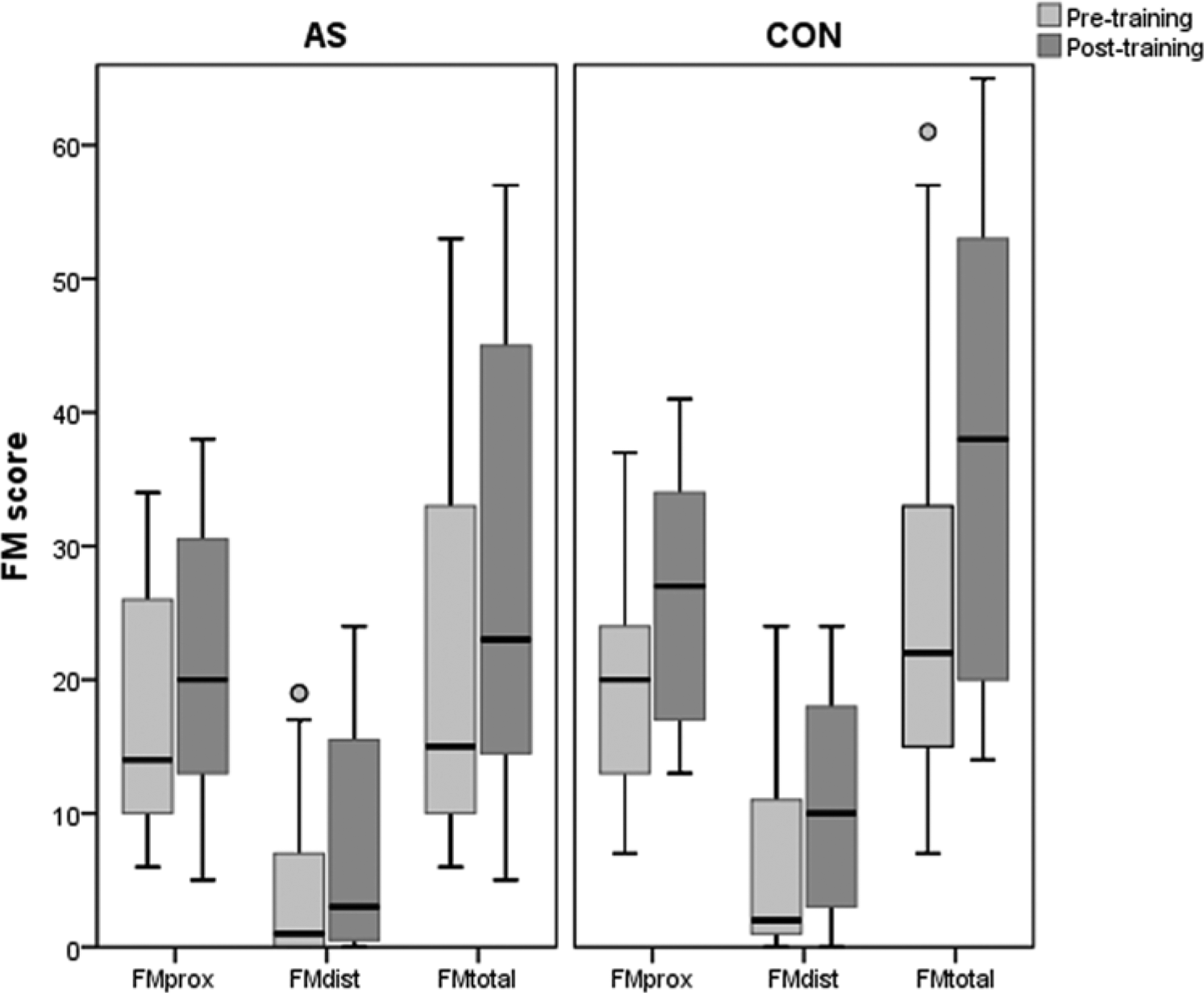
Boxplot of proximal, distal, and total upper-extremity FM scores before (light gray) and after training (dark gray) for AS (left panel) and CON (right panel); circles represent outliers (deviation of <1.5 times the interquartile range).
Reach Distance
A small difference in reach distance was found at baseline between both groups (P = .017), with a 7 cm smaller reach distance for the AS group (Table 2). After training, both groups (AS and CON) had improved reach distance significantly by 5 and 7 cm, respectively (P = .000), with no difference between groups (P = .375).
Motivation
The IMI could not be completed by 8 participants (5 from the CON and 3 from the AS group) because of insufficient understanding of the questions, resulting in IMI data being available from 28 participants in the CON group and 32 in the AS group. Overall, both interventions were rated positively, with a composite score of 4.8 (±0.6) in CON and 5.0 (±0.7) in AS (P = .189). When looking at the primary dimension of intrinsic motivation—interest/enjoyment (Figure 4)—a higher score was found in the AS group (5.9 vs 5.1) compared with the CON group (P = .009).
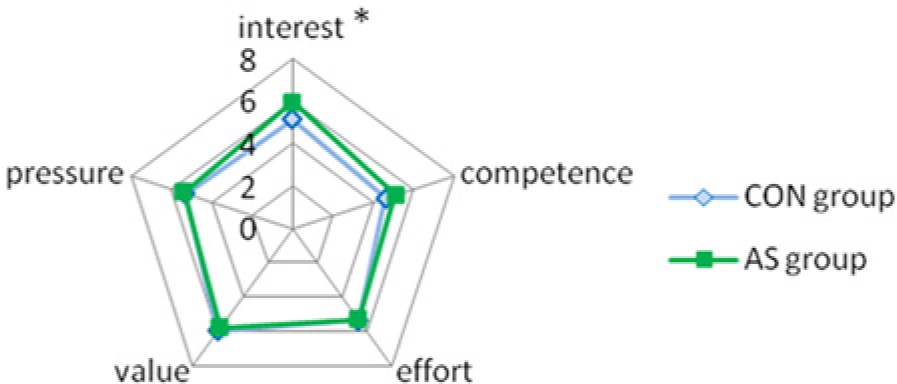
Mean scores per IMI dimension for the CON (light) and AS (dark) groups separately.
Discussion
The aim of the present study was to compare the effect of AS training with computerized exercises with dose-matched conventional therapy on hemiplegic arm function in subacute stroke. The present findings showed that both interventions resulted in significant and comparable gains on both function and capacity of the hemiplegic arm, even though a tendency could be observed toward a lower initial motor function in the AS group. In both groups, the improvements reflected changes in proximal as well as distal arm function. Improvement of proximal arm function was also reflected by increases in reach distance in both groups. Perceived arm pain was not different between both groups. Although accompanying orthopedic complaints emerging during the course of the study may have affected motor abilities in either group, none of the participants had to withdraw from the study as a result of severe problems. Self-reported intrinsic motivation was higher in the AS than the CON group.
Studies looking at comparable applications of AS in chronic stroke found increases in FM score, albeit smaller than those found in the present study, ranging between 3.3 and 5.0 points.13,15,16,29 Those improvements were similar between AS and CON, 16 as we found in the present study in subacute stroke. When comparing AS with robot-aided therapy in chronic stroke patients, improvements after training were also similar between groups. 15
Although AS is not often studied as a separate training approach, it is a common feature integrated within many robotic devices for rehabilitation purposes. 11 When considering equal dosage of robot-aided therapy and conventional therapy in subacute stroke patients, Burgar et al 30 found similar gains in both groups at the 6-month follow-up. Additionally, they showed that intensity of robot-aided therapy was positively correlated with motor control gains. Indeed, similar gains after robot-aided training and conventional therapy have been reported in chronic stroke when considering comparisons with similar number of movement repetitions, whereas gains were larger when compared with usual care of a lower intensity.31,32 As such, the strength of robot-aided therapy is currently mainly regarded as a possibility to increase intensity and/or dosage of treatment. 6 Whether this is also valid for AS as a stand-alone training modality cannot be concluded at this point because the number of movement repetitions (ie, intensity) is not known in the present study. Dosage for both groups was equal, and both groups received equal therapist supervision. AS training, using a passive instrumented arm exoskeleton, with reduced supervision has been shown to be effective in chronic stroke patients. 16 If this also applies to subacute stroke, treatment of multiple patients at once and/or increase of treatment time would be possible.
The present findings indicate that conventional arm therapy in subacute stroke can be partly replaced with AS and computerized exercises with similar results. This needs to be interpreted with care. First of all, the control intervention focused more specifically on the arm than regular rehabilitation, so this effect may be an underestimation in comparison with regular rehabilitation. Additionally, improvements cannot be solely attributed to either intervention because participants received regular rehabilitation. Lack of involvement of the hand in AS training presents another limitation of the study because this resulted in less functional exercises than the control intervention. The fact that 2 participants initially included in the present study were inadvertently started on electrostimulation treatment may also reflect this issue. Integration of hand movements with proximal AS, allowing more task-specific, functional training may enhance its treatment effect further. 33
The motivating component of the integrated games has possibly contributed to a positive effect after AS training in the present study, reflected by a higher rating for self-reported interest/enjoyment in the AS group than the CON group. Serious gaming is thought to enhance motor (re)learning in itself because of higher motivation and better attention during training. 18 Indeed, a review of serious gaming as a stand-alone intervention in upper-extremity stroke rehabilitation reported that it has a positive impact on arm function and activities. 34 Because the present study combined AS with computerized exercises, the present findings cannot be attributed solely to either AS or computerized exercises. Although this can be regarded as a drawback, the combination of electromechanical devices with a computerized training context is common and can also be considered as an advantage, especially in a scenario of self-administered training.
The present findings imply that AS may be a promising tool to increase treatment intensity or dosage. Although application of such (semi) self-administered training should be studied further, it may partly relieve a foreseen limited availability of therapists. One scenario, stated by the majority of the participating Dutch therapists as a feasible way to implement this type of training in clinical practice, is to use AS training in group treatment sessions, where several patients are training under intermittent supervision of one or a few therapists.
Conclusions
Improvements in arm function and activity of subacute stroke participants after AS training combined with computerized exercises matched the gains after CON sessions of equal dosage. This indicates that partly replacing conventional therapy with training using AS combined with computerized exercises is as effective as conventional exercises dedicated specifically to the arm in subacute stroke rehabilitation. AS training enables active arm training, especially in severely affected participants and is perceived as highly motivating by subacute stroke patients.
Footnotes
Acknowledgements
We would like to thank all participating clinical partners from the Netherlands for their valuable collaboration: Roessingh Rehabilitation Center (Enschede), Rijndam (Rotterdam), RMC Groot Klimmendaal (Arnhem), Sint Maartenskliniek (Nijmegen), de Hoogstraat (Utrecht), UMCG/Beatrixoord (Haren), Reade (Amsterdam), as well as A. H. A. Stienen (University of Twente, Enschede) and A. Snoek (Enschede) for organizational support.
Authors’ Note
This study has been registered at the Netherlands Trial Registry (NTR): NTR2539. Although the ArmeoBoom (Hocoma AG; Volketswil, Switzerland) was used in the present study, Hocoma has not been involved in funding of the present study and had no involvement in or posed any restrictions on study conception, data collection, analysis, and reporting of findings. The ArmeoBoom is based on a research prototype (Freebal) developed in a previous project, without any involvement of Hocoma. For transfer of the associated IPR of the Freebal concept to Hocoma at a later stage, limited compensation was received by Roessingh Research and Development of approximately 0.5% per unit sold, with a maximum of 300 units.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financially supported by the Innovation Program (Grant IPR2010-02) of the Netherlands Association for Medical Rehabilitation (Revalidatie Nederland) and the Netherlands Organization for Health Research and Development (ZonMw).