
Abstract
Background. Prognosis of long-term motor outcome of acute stroke patients with severe motor impairment is difficult to determine. Objective. Our primary goal was to evaluate the prognostic value of corticospinal tract (CST) injury on motor outcome of the upper limb compared with motor impairment level and lesion volume. Methods. In all, 10 acute stroke patients with moderately severe to severe motor impairment of the upper limb underwent diffusion tensor imaging (DTI) and testing of upper limb strength and dexterity at acute, subacute, and chronic poststroke time points. A density-weighted CST atlas was constructed using DTI tractography data from normal participants. This CST atlas was applied, using a largely automated process, to DTI data from patients to quantify CST injury at each time point. Differences in axial diffusivity (AD), radial diffusivity (RD), and fractional anisotropy (FA) of the ipsilesional CST relative to the contralesional CST were measured. Results. Acute loss in CST AD correlated most strongly and significantly with subacute and chronic strength and dexterity and remained significant after adjusting for acute motor impairment or lesion volume. Subacute loss in CST FA correlated most strongly with chronic dexterity, whereas subacute behavioral measures of limb strength correlated most strongly with chronic strength measures. Conclusions. Loss in acute CST AD and subacute CST FA are strong prognostic indicators of future motor functions of the upper limb for stroke patients with substantial initial motor impairment. DTI-derived measure of CST injury early after stroke may have utility in health care planning and in design of acute stroke clinical trials.
Keywords
Introduction
Acute stroke often causes upper-limb paresis ranging in severity from mild to severe. Most patients experience some degree of motor recovery over time, with final motor outcome typically achieved within 6 months.1,2 For acute stroke patients with mild to moderate motor impairment of the upper limb, motor outcome is well predicted by the initial level of impairment measured by behavioral tests.1,3-5 However, for acute patients with severe motor impairment of the limb, motor outcome is only weakly predicted by initial impairment level, with approximately equal numbers achieving good and poor motor outcomes.4-6 An accurate prognostic indicator for acute stroke patients with severe motor impairment could have substantial utility in discharge and rehabilitation planning and in the design of acute stroke clinical trials.
As the corticospinal tract (CST) is a brain structure critical to voluntary movement of the upper limb, the severity of stroke-induced injury to the CST would be expected to affect motor outcome of the limb. Transcranial magnetic stimulation studies of the neurophysiological status of the CST in acute stroke patients with severe motor impairment of the upper limb have shown that motor outcome is generally better if motor-evoked potentials (MEPs) can be elicited in the affected hand than if MEPs are absent.7,8 However, some severely impaired acute stroke patients with absent MEPs make substantial recovery,9,10 indicating that accurate prognosis on a per-patient basis requires an alternative approach. Diffusion tensor imaging (DTI) is a noninvasive magnetic resonance imaging (MRI) technique that can be used to assess structural integrity of the CST. Greater proximity between the CST, localized by DTI tractography, and an acute infarct is associated with poorer motor outcome.11-14 Quantitative DTI studies in patients early after stroke have shown that greater loss in diffusion anisotropy of selected regions of the CST is associated with poorer motor outcome.13,15-21 However, among these prior DTI studies, only a few restricted enrollment to stroke patients with severe motor impairment,13,16,22 the subset of patients for whom behavioral testing is an inadequate prognostic tool. Also, only 1 prior study compared the prognostic value of CST injury with initial motor impairment. 21 Therefore, it is unclear if motor outcome of acute stroke patients with severe motor impairment is better predicted by a DTI-derived measure of CST injury than initial motor impairment.
Toward addressing this gap in knowledge, the current exploratory study assessed the prognostic value of DTI-derived measures of CST injury in acute stroke patients with moderately severe to severe motor impairment, relative to behavioral measure of motor impairment and lesion volume (ie, a cruder measure of brain injury). The vast majority of DTI studies of stroke-induced injury to the CST have quantified tract injury by the loss in fractional anisotropy (FA), a diffusion anisotropy metric reflecting the relative magnitude of principal diffusivities. 23 Because each principal diffusivity undergoes time-varying changes in ischemic and spared white matter after acute stroke, 24 it is possible that change in a principal diffusivity of the CST might be more tightly linked to motor outcome than FA. Accordingly, we explored the relative prognostic value of FA and principal diffusivities of the CST. Furthermore, with an eye toward future clinical utility, we sought to develop an automated process for measuring CST injury rather than relying on manual delineation of CST regions of interest in the DTI data, the time- and expertise-demanding approach typically used now.
Methods
Study Design
Stroke patients participated in serial testing of motor function of the upper limb and MRI at 3 to 7 days (S1, acute), 1 to 2 months (S2, subacute), and 6 to 7 months (S3, chronic) after stroke onset.
Participants
A total of 10 patients with at least moderately severe motor impairment of the upper limb caused by acute ischemic stroke in the middle cerebral artery territory were enrolled (Table 1). In addition, 12 healthy adults with no history of stroke were enrolled for MRI in order to create a CST atlas. Details regarding participants are provided in the Supplementary Text, Part I.
Patient Characteristics.
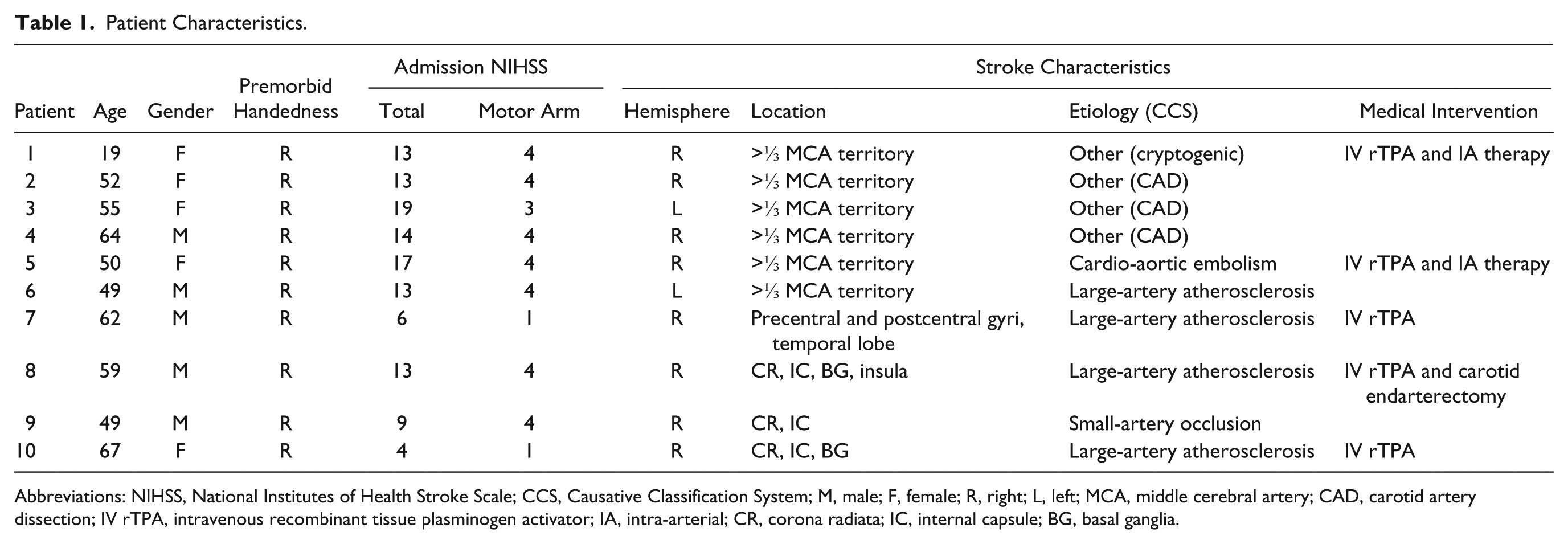
Abbreviations: NIHSS, National Institutes of Health Stroke Scale; CCS, Causative Classification System; M, male; F, female; R, right; L, left; MCA, middle cerebral artery; CAD, carotid artery dissection; IV rTPA, intravenous recombinant tissue plasminogen activator; IA, intra-arterial; CR, corona radiata; IC, internal capsule; BG, basal ganglia.
Motor Function Testing
Motor function of the upper limb was assessed by (1) grip strength of the paretic hand relative to the contralateral hand measured by digital dynamometry 25 ; (2) upper limb section of the Motricity Index (MI; scale 1-100); and (3) dexterity of the paretic hand relative to the contralateral hand measured by the Nine Hole Peg Test 26 (NHPT). Details regarding motor function testing are provided in the Supplementary Text, Part II.
Image Acquisition and Analysis
Acquisition
A Siemens 3T TIM Trio MRI scanner and 12-channel head coil were used for imaging. Imaging parameters are provided in the Supplementary Text, Part III.
Preprocessing
The DTI data were processed using standard procedures (Supplementary Text, Part IV) to generate images of each eigenvalue (λ1, λ2, and λ3), FA, the apparent diffusion coefficient, and mean B0 and mean DWI (diffusion-weighted imaging). The dominant diffusivity λ1 is also known as axial diffusivity (AD). The mean of perpendicular diffusivities λ2 and λ3 was computed and is known as radial diffusivity (RD).
CST Diffusion
Figure 1 shows the density-weighted CST atlas in MNI space. Details on atlas construction are provided in the Supplementary Text, Part V.
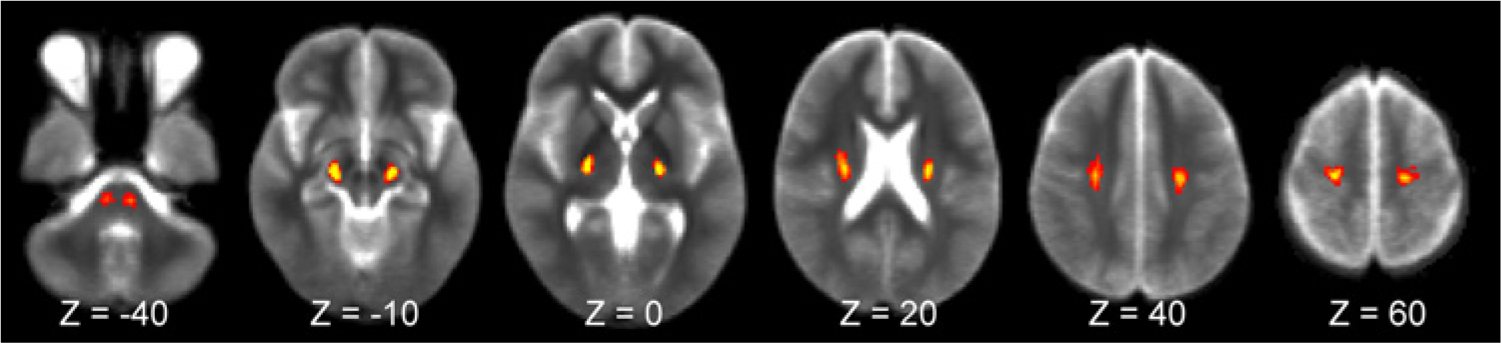
Density-weighted CST atlas in MNI152 space. Several axial (z-level) images from the level of the pons to the precentral gyrus are shown. Voxels are color coded for the relative density (scale of 0-100) of CST streamlines based on tractography of DTI data from healthy individuals.
The CST atlas was used to measure CST injury in each patient at each session by the following process. Using nonlinear registration software 27 from FMRIB’s FSL Library,28,29 each B0 volume was spatially normalized to the T2-weighted MNI152 brain with abnormal hyperintense voxels masked to eliminate them from the registration optimization process. Visual inspection of each registered B0 volume showed good alignment to the MNI152 brain even for brains with structural distortion caused by edema at S1 or atrophy at S3. The density-weighted CST atlas was warped from the MNI152 space to each native diffusion space by inverting the aforementioned registration matrix. At each transverse slice along the length of the ipsilesional CST and contralesional CST, the 10 voxels with the highest CST density were selected. Voxels in ventricular space were removed from the high-density CSTs, whereas voxels in regions of cavitation were retained; details of this process are provided in the Supplementary Text, Part VI. The mean of each diffusion metric of interest (AD, RD, and FA) was computed across the ipsilesional and contralesional high-density CST voxels at each transverse slice. To account for individual differences in brain size, each diffusion measurement series was brought into spatial correspondence by interpolating to 60 points. Each 60-point series was smoothed by replacing each value with the mean of itself ± 2 adjacent points. Because there are age-related changes in white matter diffusion that are roughly symmetric between the hemispheres, 30 we minimized the impact of patient age on estimates of CST injury by subtracting each diffusion measurement of the ipsilesional CST from the corresponding point of the contralesional CST. Finally, each set of 60 delta measurements was summed to provide overall measures of AD, RD, and FA of the ipsilesional CST relative to the contralesional CST, which we hereafter refer to as CST ΔAD, ΔRD, and ΔFA, respectively. Positive values indicate stroke-induced increases in the diffusion metric of the ipsilesional CST relative to the contralesional CST, and negative values indicate stroke-induced decreases.
Lesion Volume
Lesion volume at S1 was measured using the DWI and at S2 using the FLAIR (fluid attenuated inversion recovery) image. Abnormal hyperintense voxels were labeled manually in native image space. Volumes were calculated by multiplying the number of labeled voxels by voxel volume.
Statistical Analysis
An abnormality in CST diffusion (ΔAD, ΔRD, and ΔFA) at S1 was evaluated using the 1-sample Wilcoxon signed-rank test. Mixed-model analysis was used to test for an effect of time on each motor function and each CST diffusion metric, with the Bonferroni-corrected Wilcoxon signed-rank test used for post hoc testing. Spearman’s correlation was used to measure the strength of association between 2 variables, and Spearman’s partial correlation was used when adjusting for a covariate. The value of α was set at the 2-tailed .05 level for all statistical testing. All testing was conducted using JMP software (SAS Institute Inc, v 8.0.2).
Results
Motor Function
Figure 2 shows measures of motor function (grip, MI, and NHPT) at S1 to S3. Patients made significant gains in grip strength and MI over time (each P < .001), with significant increases from S1 to S2 and S2 to S3 for both motor functions. Dexterity, measured by the NHPT, did not improve significantly over time (P = .11).
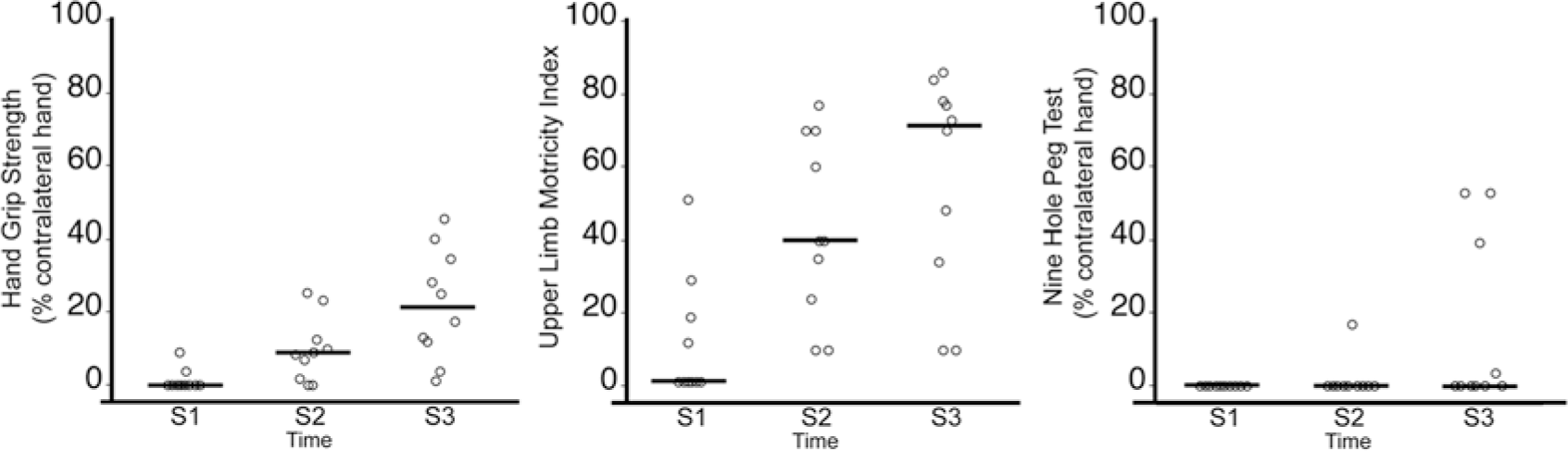
Motor functions of the paretic upper limb of stroke patients (n = 10) at the acute (S1), subacute (S2), and chronic (S3) study time points. Symbols have been shifted along the x axis to allow easier visualization. The line at each time point represents the median. Over time, patients made significant gains in grip (P < .001, mixed-model analysis) and Motricity Index (P < .001) but not the Nine Hole Peg Test (P = .11).
CST Diffusion
Figure 3 shows measures of CST diffusion at S1 to S3. At S1, there was a significant loss in CST ΔAD (P < .001) and CST ΔFA (P < .001) but not CST ΔRD. Patients showed significant change in CST ΔAD over time (P < .001), with significant increases from S1 to S3 and S2 to S3. CST ΔRD changed significantly over time (P < .001), increasing significantly from S1 to S2 and S2 to S3. CST ΔFA also changed significantly over time (P < .001), decreasing significantly from S1 to S2 and S1 to S3.
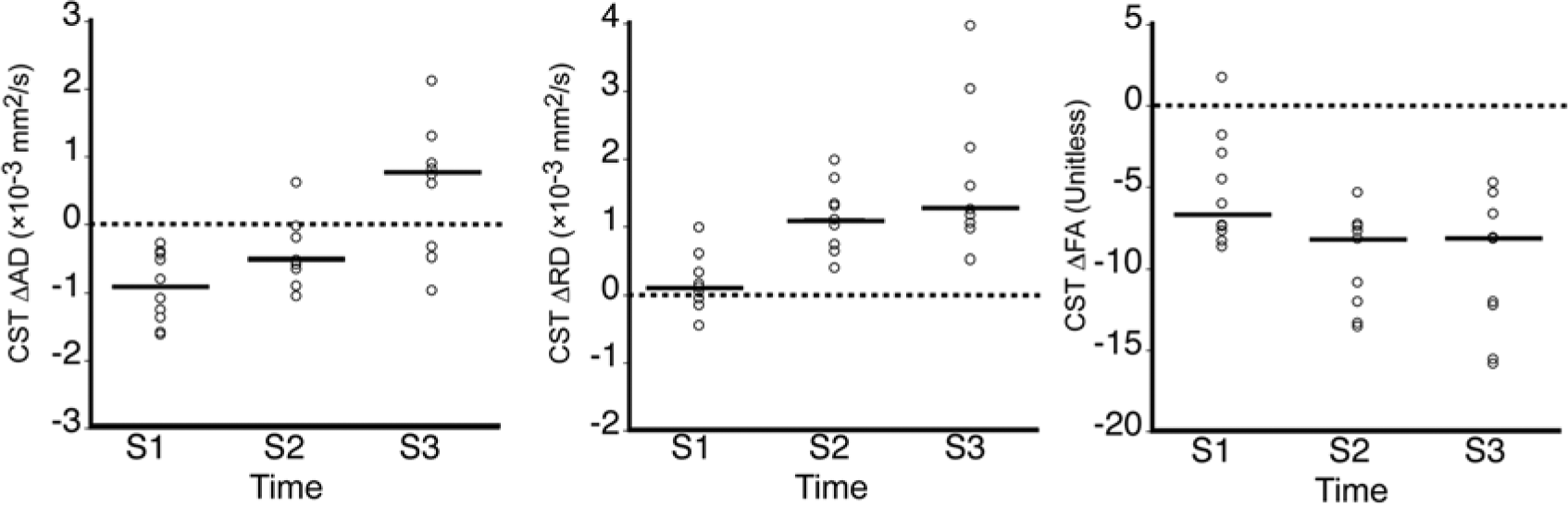
CST diffusion (ΔAD, ΔRD, and ΔFA) at S1 to S3. The line at each time point represents the median. Patients had significant losses in CST ΔAD (P < .001, 1-sample Wilcoxon signed-rank test) and CST ΔFA (P < .001) but not CST ΔRD at S1. There were significant changes over time in CST ΔAD, ΔRD, and ΔFA (each P < .001, mixed-model analysis).
Correlations
We first examined the strength of association between motor outcomes at S2 (ie, grip, MI, and NHPT) and each potential predictor measured at S1 (ie, CST diffusion, respective motor function, and DWI lesion volume). Figures 4A to 4C show that among S1 potential predictors, only CST ΔAD correlated significantly with S2 grip. Confidence and prediction intervals about the regression line relating S1 CST ΔAD to S2 motor functions grip and MI are provided in the Supplementary Text, Part VII. NHPT did not correlate significantly with any S1 potential predictor. The correlations between S1 CST ΔAD and S2 grip and MI remained significant after adjusting for S1 motor function, S1 DWI lesion volume, S1 testing day, or age (Table 2). These findings suggest that acute loss in AD of the CST is a strong predictor of subacute grip and overall strength of the paretic upper limb.
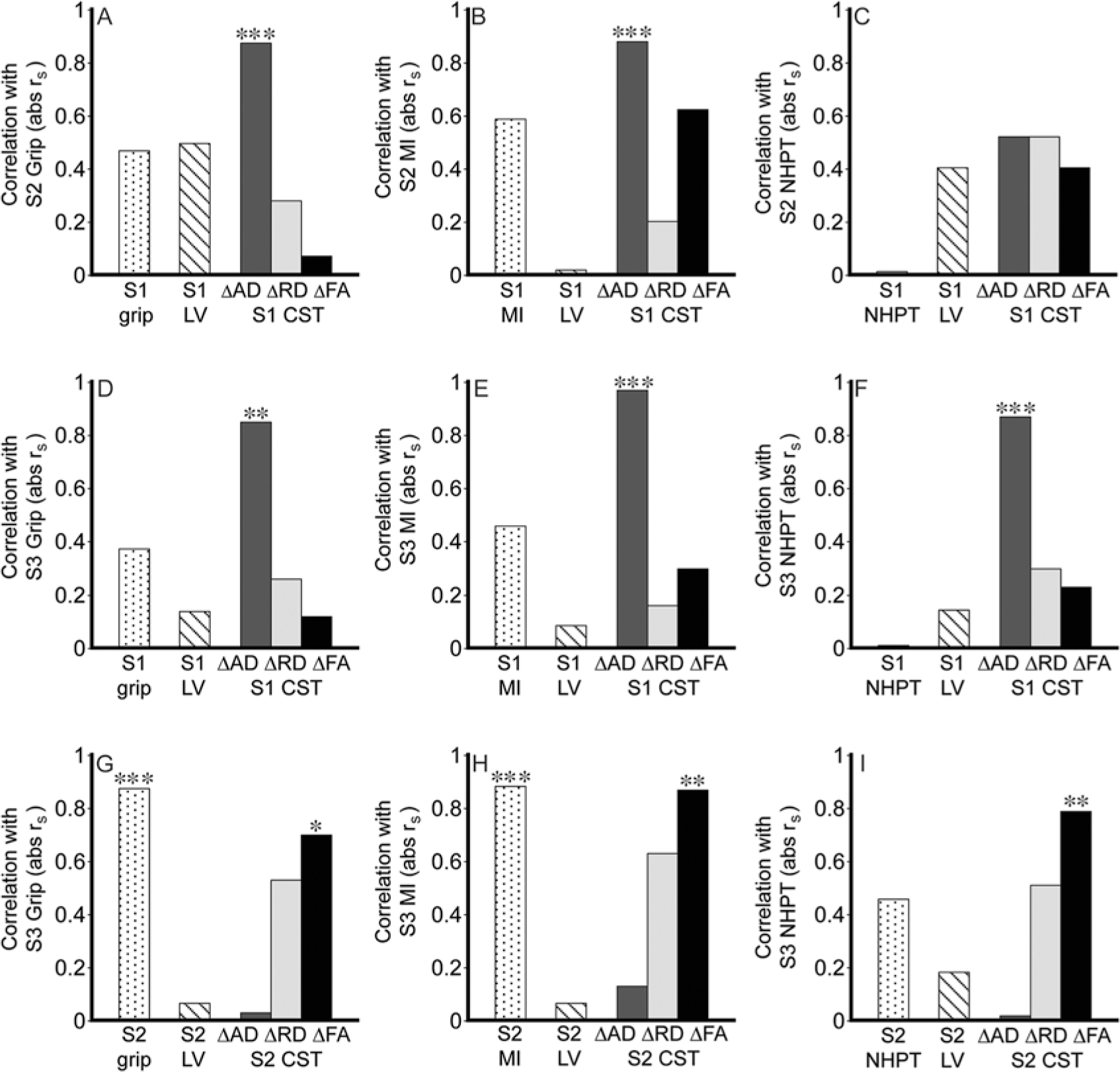
Correlation between motor outcomes and potential predictors: A-C. S1 potential predictors of motor functions at S2. D-F. S1 potential predictors of motor functions at S3. G-I. S2 potential predictors of motor functions at S3. S1 LV = DWI lesion volume. S2 LV = FLAIR lesion volume. Values are Spearman’s correlation coefficients, absolute rs. *P < .05, **P < .01, ***P < .001.
Results of Correlation and Partial Correlation Analyses. a
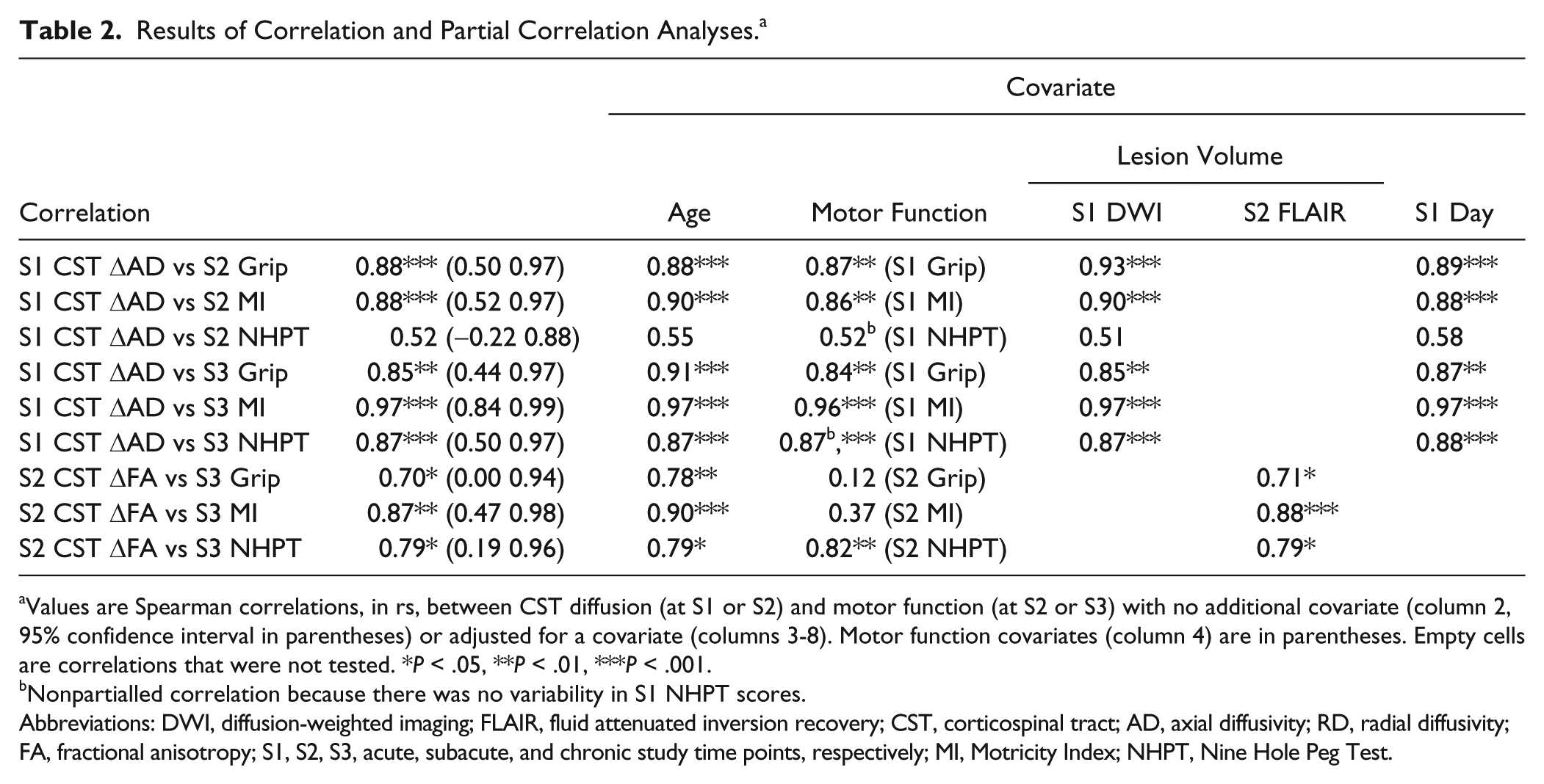
Values are Spearman correlations, in rs, between CST diffusion (at S1 or S2) and motor function (at S2 or S3) with no additional covariate (column 2, 95% confidence interval in parentheses) or adjusted for a covariate (columns 3-8). Motor function covariates (column 4) are in parentheses. Empty cells are correlations that were not tested. *P < .05, **P < .01, ***P < .001.
Nonpartialled correlation because there was no variability in S1 NHPT scores.
Abbreviations: DWI, diffusion-weighted imaging; FLAIR, fluid attenuated inversion recovery; CST, corticospinal tract; AD, axial diffusivity; RD, radial diffusivity; FA, fractional anisotropy; S1, S2, S3, acute, subacute, and chronic study time points, respectively; MI, Motricity Index; NHPT, Nine Hole Peg Test.
We next examined the strength of association between S3 motor outcomes and each S1 potential predictor. Figures 4D to 4F show that S1 CST ΔAD correlated significantly with S3 grip, MI, and NHPT. Confidence and prediction intervals about the regression line relating S1 CST ΔAD to these S3 motor functions are provided in the Supplementary Text, Part VII. The correlation between S1 CST ΔAD and each S3 motor function remained significant after adjusting for each covariate considered above (Table 2). These findings, together with the observed correlations between S1 CST ΔAD and S2 motor outcomes described above, suggest that the prognostic value of acute loss in CST AD extends from the subacute to the chronic poststroke period and from gross to fine motor functions.
Next, we examined the strength of association between S3 motor outcomes and potential predictors measured at S2 (ie, CST diffusion, respective motor function, and FLAIR lesion volume). Figures 4G to 4I show that S2 grip and MI, but not NHPT, correlated strongly and significantly with their respective S3 motor function. Among the diffusion measures of S2 CST injury, CST ΔFA correlated most strongly and significantly with each S3 motor function. The correlation between S2 CST ΔFA and S3 grip as well as between S2 CST ΔFA and S3 MI remained significant when adjusted for age or FLAIR lesion volume (Table 2). However, given the strong correlation between S2 grip and S3 grip as well as between S2 MI and S3 MI (each rs = 0.88), the correlations between S2 CST ΔFA and S3 motor functions grip and MI were no longer significant after adjusting for the respective S2 motor function. The correlation between S2 CST ΔFA and S3 NHPT remained significant after adjusting for each considered covariate. These findings suggest that while subacute loss in CST FA does not improve prognosis of chronic grip and MI, it is a better prognostic indicator of chronic dexterity than behavioral measures of dexterity.
The findings described above led us to examine the basis of acute CST ΔAD and subacute CST ΔFA being good predictors of future motor functions (see Supplementary Text, Part VIII). Analyses revealed that among the 3 measures of CST injury at S1, CST ΔAD correlates most strongly with S2 CST ΔRD and ΔFA, the measures of S2 CST injury that correlate strongly with S2 grip and S2 MI (Supplementary Tables 1 and 2). S1 CST ΔAD also correlates most strongly with S3 CST ΔFA, the strongest correlate of S3 motor functions. Similarly, among the measures of CST injury at S2, CST ΔFA correlates most strongly with S3 CST ΔFA, the strongest correlate of S3 grip, MI, and NHPT. These results suggest that the strong prognostic value of acute CST ΔAD and subacute CST ΔFA for future motor functions is because they are the best surrogates of future measures of CST injury.
Finally, given our interest in assessing the clinical utility of our DTI-based prognostic method, we evaluated the effect on correlations between motor outcomes and CST injury measured using DTI data downsampled from 60 to 30 directions because halving the number of diffusion directions would halve imaging time and thereby may make DTI more easily tolerated by acute stroke patients (see Supplementary Text, Part IX). We found that correlation strength based on the 30-direction data were quite similar to those based on the original 60-direction data (Supplementary Table 3). Accordingly, as suggested based on the 60-direction data, our method may have clinical utility for prognosis of motor outcomes of acute and subacute stroke patients.
Discussion
Prognosis of motor outcome for acute stroke patients with severe motor impairment has proved difficult to determine. The current study explored the prognostic value of DTI-derived measures of CST injury in acute patients 3 to 7 days after stroke onset, with moderately severe to severe motor impairment of the upper limb. We found that acute CST injury, measured by loss in AD of the ipsilesional CST relative to the contralesional CST (ie, CST ΔAD), strongly and significantly correlated with subacute grip and overall upper-limb strength (ie, MI) as well as chronic grip, overall limb strength, and dexterity (ie, NHPT; Figure 4). In contrast, motor outcomes did not correlate significantly with the other measures of acute CST injury (ΔFA, ΔRD), acute motor impairment, or acute lesion volume. Moreover, the significant correlations between acute CST ΔAD and motor outcomes remained significant after accounting for acute motor impairment, lesion volume, or other potentially relevant covariates (ie, age and poststroke day of acute testing; Table 2). These findings suggest that CST ΔAD in patients 3 to 7 days after stroke onset is a strong prognostic indicator of motor outcome.
Although our results suggest that acute CST ΔAD has strong prognostic value, the majority of prior DTI studies in humans have used the FA metric to quantify white matter injury. Motor outcome has been shown to be strongly associated with progressive loss in FA of the CST measured serially over the first few weeks to months after stroke15,17,19 and with FA of the CST measured at approximately 2 weeks after stroke. 31 We found that CST ΔFA at 3 to 7 days after stroke onset correlates weakly to moderately with motor outcomes (range in rs = 0.07-0.62; Figure 4), consistent with prior reports that CST FA at a single time point within the first week after stroke has limited value in predicting long-term motor outcome.18,32 Together, these findings suggest that motor outcome is only weakly to moderately predicted within the first week after stroke by FA of the CST, yet can be strongly predicted by AD. However, Yu et al 19 reported that neither AD nor FA of the CST measured within 1 week of stroke correlated significantly with the 1-year Motricity Index. There are several possible reasons for the partial discrepancy between our results and those of Yu et al, including different methods for measuring CST injury. A recent DTI study in patients with amyotrophic lateral sclerosis showed that AD of the CST, but not FA, differentiated clinical phenotypes. 33 Furthermore, AD but not FA of white matter involved in transmitting information about visual motion differentiates adults with or without susceptibility to motion-induced nausea. 34 Collectively, these studies suggest that AD of functionally relevant white matter tracts can provide greater clinical insight about some neurological conditions compared with FA.
Our acute stroke patients had at least moderately severe motor impairment—that is, they were patients for whom prognosis of motor outcome is currently difficult. Previous DTI studies that similarly restricted enrollment to patients with severe motor impairment have suggested the prognostic value of CST injury.13,16,22 However, CST injury in these studies was measured over a wide poststroke period (~5-30 days), whereas our measurements were generally made earlier (3-7 days). Our earlier measurement translates into increased potential that our prognostic biomarker may have clinical utility for severely impaired, acute stroke patients. A recent study by Puig et al 21 that enrolled acute patients with mild to severe motor impairment found that 90-day motor outcome was predicted strongly at <12 hours by whether or not the CST is damaged, consistent with our findings. However, at 3 days, the level of motor impairment was found to have strong explanatory value, and information about CST damage added little. These later findings of Puig et al may appear inconsistent with ours; however, about 50% of their patients at 3 days poststroke were mildly impaired, whereas all our patients at 3 to 7 days poststroke had at least moderately severe motor impairment. Because motor outcome of acute stroke patients with mild impairment is well predicted by the level of impairment,1,3-5 the prognostic value of CST damage for the Puig et al 3-day patients may have been minimized. Combined, these findings suggest that the value of acute CST injury for predicting motor outcome increases with greater acute motor impairment.
Our study also explored the prognostic value of DTI-derived measures of CST injury in subacute patients (1-2 months after stroke onset) for predicting chronic motor functions (6-7 months after stroke onset). We found that subacute CST injury, measured by loss in FA of the ipsilesional CST relative to the contralesional CST (CST ΔFA), had stronger prognostic value for predicting chronic dexterity (ie, NHPT) than subacute behavioral measure of dexterity, whereas chronic grip and overall limb strength (ie, MI) were sufficiently well predicted by their respective subacute behavioral measure (Figure 4 and Table 2). The differential prognostic value of subacute CST injury among the 3 motor functions may stem from the fact that all our patients had severe impairment in dexterity at the subacute time point, whereas many fewer subacute patients had severe impairment in grip and overall limb strength (Figure 2). Accordingly, as suggested above regarding acute prognoses, the value of subacute CST injury for predicting motor outcome may increase with greater subacute motor impairment.
It is noteworthy that the DTI-derived measure of CST injury that correlated most strongly with future motor functions was ΔAD at the acute time point, whereas it was ΔFA at the subacute time point. These findings prompt several interrelated questions. First, why might these early measures of CST injury strongly predict later motor functions? Our analysis suggests that among the measures of CST injury considered, acute CST ΔAD and subacute CST ΔFA are the best surrogates of future CST injury and, thereby, the best predictors of later motor functions (Supplementary Text VIII, Supplementary Tables 1 and 2).
Second, why might CST ΔAD be the best indicator of acute CST injury compared with ΔRD and ΔFA? Toward understanding this finding, it should be kept in mind that our measures of CST injury reflect diffusion abnormalities along the ipsilesional CST from the precentral gyrus to pons, thus involving both ischemic and spared regions. At 3 to 7 days after stroke onset, all our patients had a loss in CST ΔAD, whereas the direction of change in CST ΔRD was variable: reduced in 7 patients and elevated in 3 patients (Figure 3). These findings are compatible with prior reports that ischemic white matter undergoes progressive reductions in AD over the first few weeks after stroke, whereas RD initially drops and then rises over this time period, diffusivity changes likely resulting from membrane failure and then disrupted cell structure.24,35-37 Also, over the first few weeks after stroke, the spared ipsilesional CST undergoes progressive reductions in AD and later elevations in RD,15,19 corresponding to earlier degeneration of axonal fibers than myelin sheaths.38,39 Given the time-varying changes in RD of ischemic and spared CST regions, CST ΔRD may be an unstable indicator of CST injury at 3 to 7 days after stroke onset. Furthermore, because the FA metric incorporates the magnitude of RD, CST ΔFA may be rendered an unstable indicator of CST injury at 3 to 7 days. On the other hand, the consistent losses in AD of ischemic and spared CST regions early after stroke may explain why CST ΔAD is a good indicator of CST injury at 3 to 7 days poststroke.
Third, why might CST ΔFA be the best indicator of subacute CST injury compared with CST ΔAD and ΔRD? AD of ischemic white matter begins to rise and RD continues to rise during the subacute period, reflecting accumulation of water that freely diffuses in cystic spaces that replaces necrotic tissue. 40 In spared CST regions, reductions in AD and elevations in RD continue, largely because of further degeneration of axonal fibers and myelin, respectively.17,19,41 We propose that because there are no highly time-varying changes in diffusivities of the CST during the 1 to 2 months poststroke, such as those in RD during the 3- to 7-day period, the FA metric that incorporates both axial and radial diffusivities may be the best indicator of subacute CST injury. The inherent noisiness of diffusion-weighted images can be mitigated by using the FA metric, 42 which may contribute to CST ΔFA being a good indicator of subacute CST injury.
A parallel aim of our exploratory study was to set the technical groundwork for future clinical utility of our DTI-based method for prognosis of motor outcome in acute and subacute stroke patients. Our method involves a density-weighted CST atlas that was constructed using DTI-tractography data from normal individuals. This atlas could be made publicly available after future verification of our method. The atlas was utilized to measure CST injury in patients by a process that is currently automated, except for 2 steps. The first of these is manual labeling of abnormally hyperintense voxels in B0 images. With recent advances in automated delineation of ischemic tissue,43,44 manual labeling could be obviated in the future. Our process also currently involves visual assessment of automatically defined high-density CST voxels, and manual removal of voxels that erroneously extend into cerebrospinal fluid and/or the temporal lobe in the cerebral peduncle region, which occurred in a few patients. An automated strategy could be selection of fewer than the default number of 10 highest-density CST voxels in the cerebral peduncle region. Clinical application of our method would also require development of automated quality control, rather than visual and subjective assessments. We showed that prognostic strengths of acute CST ΔAD and subacute ΔFA were essentially unchanged when measured using the original high-resolution (60-direction) DTI data compared with the downsampled, lower-resolution (30-direction) DTI data (Supplementary Table 3). The lower-resolution DTI data would have taken about 5 minutes to acquire, comparable to the duration of current imaging protocols that acute patients typically tolerate well, further supporting the potential clinical utility of our prognostic approach.
Our study has several strengths and limitations. Its strengths include examining the relative prognostic strength of several diffusion metrics, not simply the commonly used FA metric. Furthermore, it is a serial study that evaluated the value of several DTI-derived measures of CST injury at acute and subacute time points for predicting multiple motor outcomes of the upper limb. A limitation of this study is its small sample size and thus low statistical power. As a result, some relationships with moderate correlation were deemed not significant (eg, acute CST ΔFA vs subacute MI, rs = 0.62, P = .054). Also a consequence of low statistical power, to minimize the likelihood of model overfitting and resultant type 1 error, we assessed the prognostic value of DTI-derived measures of CST injury after adjusting serially for each covariate rather than multiple covariates in a single model. Despite these limitations, the novel findings and technical developments of the current exploratory study motivate a future study involving a substantially larger sample size.
In summary, the findings of our current study provide preliminary support that acute CST ΔAD and subacute ΔFA are strong prognostic indicators of motor outcomes for stroke patients with significant initial motor impairment. With future validation by a larger study, our DTI-based prognostic method could allow clinicians to more confidently inform their patients and families about expected outcomes, and the health care system could better project and allocate long-term care and rehabilitation resources. A DTI-based measure of acute CST injury could also be used for patient selection and randomization in stroke clinical trials and as a surrogate biomarker of long-term motor outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Founders Affiliate of the American Heart Association (09GRNT2240036) and carried out using resources provided by the Biomedical Technology Program of the NIH-NCRR (P41RR14075) and the Harvard NeuroDiscovery Center. ABS was supported by grants from the NIH-NINDS (R01NS051412 and 1R21NS077442).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.