
Abstract
Background. Swallowing dysfunction is intractable after acute stroke. Our understanding of the alterations in neural networks of patients with neurogenic dysphagia is still developing. Objective. The aim was to investigate cerebral cortical functional connectivity and subcortical structural connectivity related to swallowing in unilateral hemispheric stroke patients with dysphagia. Methods. We combined a resting-state functional connectivity with a white matter tract connectivity approach, recording 12 hemispheric stroke patients with dysphagia, 12 hemispheric stroke patients without dysphagia, and 12 healthy controls. Comparisons of the patterns in swallowing-related functional connectivity maps between patient groups and control subjects included (a) seed-based functional connectivity maps calculated from the primary motor cortex (M1) and the supplementary motor area (SMA) to the entire brain, (b) a swallowing-related functional connectivity network calculated among 20 specific regions of interest (ROIs), and (c) structural connectivity described by the mean fractional anisotropy of fibers bound through the SMA and M1. Results. Stroke patients with dysphagia exhibited dysfunctional connectivity mainly in the sensorimotor-insula-putamen circuits based on seed-based analysis of the left and right M1 and SMA and decreased connectivity in the bilateral swallowing-related ROIs functional connectivity network. Additionally, white matter tract connectivity analysis revealed that the mean fractional anisotropy of the white matter tract was significantly reduced, especially in the left-to-right SMA and in the corticospinal tract. Conclusions. Our results indicate that dysphagia secondary to stroke is associated with disruptive functional and structural integrity in the large-scale brain networks involved in motor control, thus providing new insights into the neural remodeling associated with this disorder.
Keywords
Introduction
Neurological oropharyngeal dysphagia is a common and intractable clinical problem encountered in stroke patients, and it is associated with aspiration pneumonia. A recent large cohort study reported that pneumonia was observed in 7.1% of patients presenting with acute ischemic stroke and was associated with lower early, long-term survival, longer hospitalization, and higher disability at discharge. 1 Multiple studies have confirmed the relationship between the severity of the neurological status and the manifestation of dysphagia after stroke.2-9 An improved understanding of stroke severity and examination for the presence of aspiration in the early stages of a stroke may guide the implementation of strategies for the treatment of dysphagia.
We have recently identified the cortical representations of swallowing in dysphagic stroke patients using blood oxygenation level–dependent functional MRI (fMRI) of a voluntary saliva swallowing task. 10 The results supported the hypothesis that the swallowing function in dysphagic stroke patients is associated with compensatory recruitment and activation of regions of the cerebral cortex in the intact hemisphere.
Resting-state fMRI, also known as task-free fMRI, has emerged as an important technique to assess functional connectivity in the brain. Spontaneous neural activity occurs in the brain during rest and is organized into specific functional networks in which the low frequency changes in fMRI signal intensity are highly correlated or in-phase. 11 An increasing number of fMRI studies have implicated multiple regions of the cerebral cortex and subcortex in the process of swallowing in healthy adults.12-16
A substantial effort has been made using connectivity MRI to provide an outstanding framework for merging anatomical and functional data and thus improve our understanding of brain pathologies.17,18 However, little is known about how the effective connectivity among these regions relates to swallowing function. Many neuroimaging studies have been conducted using these tensor-derived quantities as markers for white matter tract maturation and integrity in order to better understand normal brain development and the neural basis of neuropsychiatric and neurodegenerative disorders. 19
Indeed, alterations in functional and structural connectivity networks could help to elucidate the relevant neural mechanisms underlying swallowing impairments and provide evidence for functional changes in the cortex resulting from a stroke. Thus, a functional connectivity analysis based on a blood oxygen level–dependent fMRI signal combined with diffusion tensor imaging (DTI) fiber tractography may provide a better understanding of how the altered functional and structural connectivity within brain networks relates to the neural underpinnings of stroke-induced oropharyngeal dysphagia.
The purpose of this study was to investigate the neural mechanisms responsible for changes in functional and structural connectivity in dysphagic stroke. For the first time, resting-state functional connectivity and DTI tractography were combined to provide a comprehensive evaluation of the neural circuitry underlying unilateral hemispheric stroke with dysphagia compared with that of healthy adults. Given the anatomical and functional abnormalities found in previous fMRI studies of stroke with dysphagia, which suggested a key role for the primary motor cortex and supplementary motor area in swallowing function, we hypothesized that abnormalities were present in the connectivity of the functional and structural network and attempted to demonstrate this using a seed-based correlation approach. We also expected that alterations in the large-scale brain motor network model would be observed in stroke patients with swallowing impairment, which would further elucidate the relevant neurorehabilitation mechanisms responsible for cerebral activation of swallowing following stroke-induced dysphagia.
Methods
Subjects
The study protocol was approved by the institutional ethics committee at Sichuan University, and written informed consent was obtained from all subjects prior to commencing the research. Patients consecutively admitted to the Stroke Center of West China Hospital from January 2010 to July 2012 were included in the study based on the criteria that they had suffered their first (and only) hemispheric ischemic stroke in the distribution of the middle cerebral artery with symptoms lasting at least 24 hours and with objective lesions observable via cerebral imaging (computed tomography and/or MRI). During the initial consultation, we obtained the following information from each patient: sex, age at which the stroke occurred, time elapsed since the stroke, type of stroke, and the location and side (left or right hemisphere) of the lesion. Twenty-four stroke patients were enrolled and diagnosed with their first ischemic stroke, as defined by the World Health Organization criteria (a sudden onset of neurological deficit persisting for >24 hours). 20 All patients were assessed for swallowing dysfunction within 24 hours of stroke onset by a qualified speech and language therapist. The therapist used the Logemann clinical indicators of dysphagia, 21 that is, coughing, oral residue, delayed swallowing, reduced laryngeal elevation (observed by placing one finger on the hyoid and one on the thyroid), throat clearing, and choking. To confirm the diagnosis, patients were subjected to videofluoroscopic swallowing examination (VFSS Imager, Model IA-12LD/HG12, Shimadzu Corporation, Kyoto, Japan). Those who displayed at least one of the following symptoms were considered to be dysphagic patients 22 : (a) food residue occupying more than 50% of the vallecula or pyriform sinus space after swallowing, (b) subglottic aspiration, (c) a pharyngeal transit time >2 seconds (operationally defined as the time taken for the bolus to move from the point at which the pharyngeal swallow is triggered to the cricopharyngeal sphincter), and (d) impaired cricopharyngeal muscle relaxation. Twelve patients with post-stroke dysphagia met the eligibility criteria and were admitted. This group consisted of 6 females and 6 males with a mean age of 65.2 ± 4.3 years (age range: 58-72 years). Twelve stroke patients who were not diagnosed with dysphagia were assessed for comparison (7 males and 5 females, mean age 66.5 ± 5.2 years). The exclusion criteria included (a) prior cerebrovascular disease, (b) preexisting neurological or psychiatric disorders (including a history of seizures, global cognitive impairment, aphasia, neglect, substantial sensory disturbances, severe depression, or claustrophobia), (c) use of an electrically sensitive biomedical device (eg, cardiac pacemaker or cochlear implant), (d) metal clips in the brain, or (e) pneumonia at the time of enrollment.
An age- and gender-matched group of healthy older volunteers (n = 12; 6 females and 6 males; mean age = 65.8 ± 3.3 years; range = 60-70 years) served as the control group. All control subjects had a normal neurological examination, no history of a stroke, and no significant active neurological problems. They were also free of systemic diseases and neurological disorders. All subjects were strongly right-handed according to the Edinburgh Handedness Inventory. The study adhered to the MRI safety depositional guidelines established by the US Food and Drug Administration for clinical scanners.
Data Acquisition and Data Analysis
The resting state fMRI data and DTI data were acquired in 3-T MRI. Three types of structural and functional connectivity analyses were used, including seed-based functional connectivity maps from the primary motor cortex (M1) and supplementary motor area (SMA) to the entire brain, a swallowing-related functional connectivity network calculated among 20 specific regions of interest (ROIs; Table 1), and structural connectivity described by the mean fractional anisotropy (FA) of fibers bound through the SMA and M1. Finally, comparisons between patient groups and healthy controls were processed.
The Coordinates for 20 Regions of Interest Seeds.
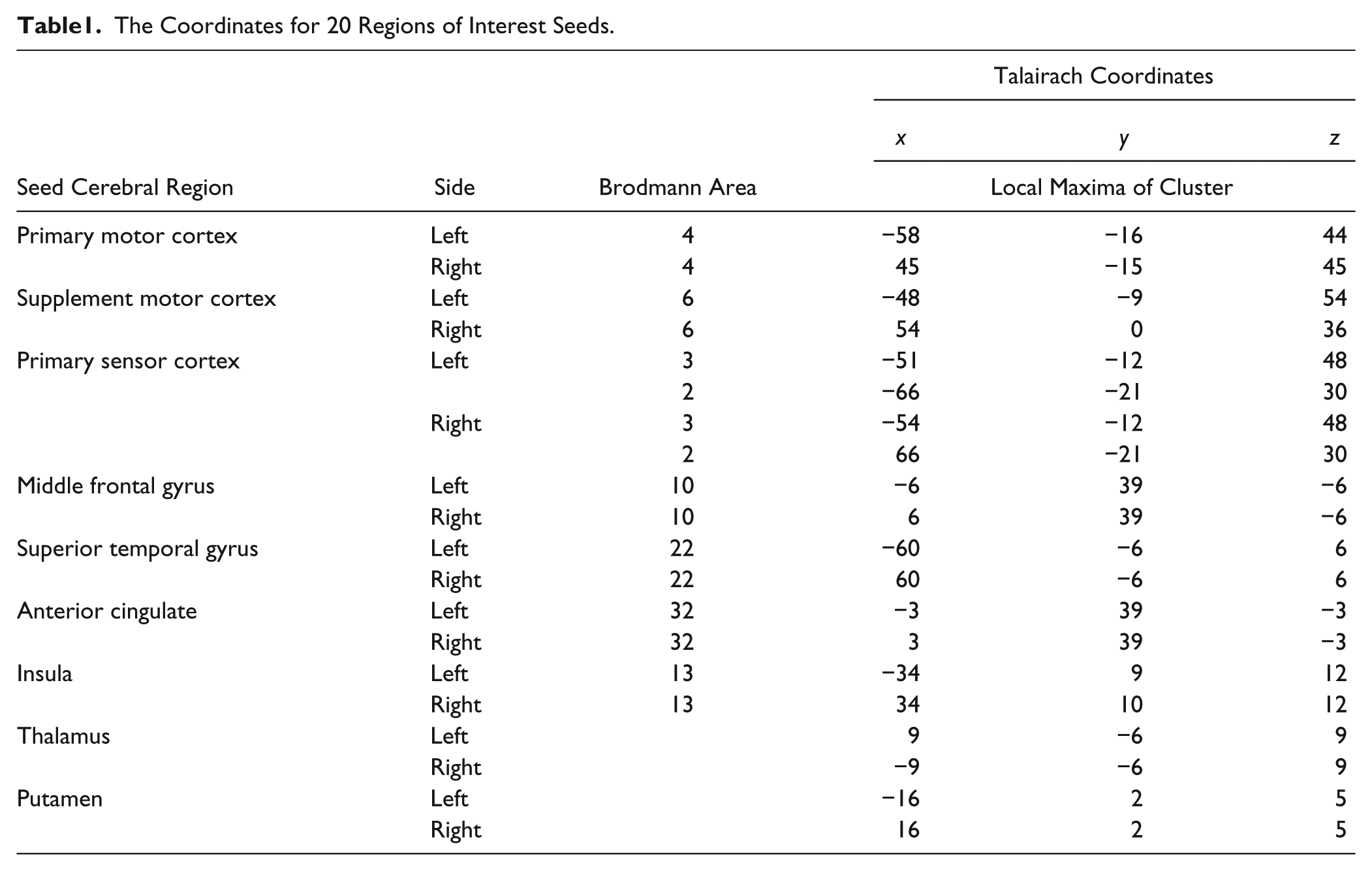
For detail, see online supplementary material file 1.
Results
Clinical Features and Examination of Dysphagia
The clinical features and lesions of stroke patients with dysphagia are summarized in Table 2. The patients had each experienced their first and only middle cerebral artery infarction up to 3 days prior to admission. The time from stroke onset to the start of the fMRI study ranged from 2 to 3 days. Based on the results of the initial VFSS, 5 patients were diagnosed with both oral and pharyngeal dysfunction, 3 with only oral dysfunction, and 4 with only pharyngeal dysfunction. Of these patients, 2 presented with a mild initial penetration–aspiration (P-A) scale score (2), 7 presented with moderate P-A scale scores (3-5), and 3 presented with a severe P-A scale score (6), indicating at least 1 aspiration episode. 23
Clinical Data of Stroke Patients With Dysphagia.
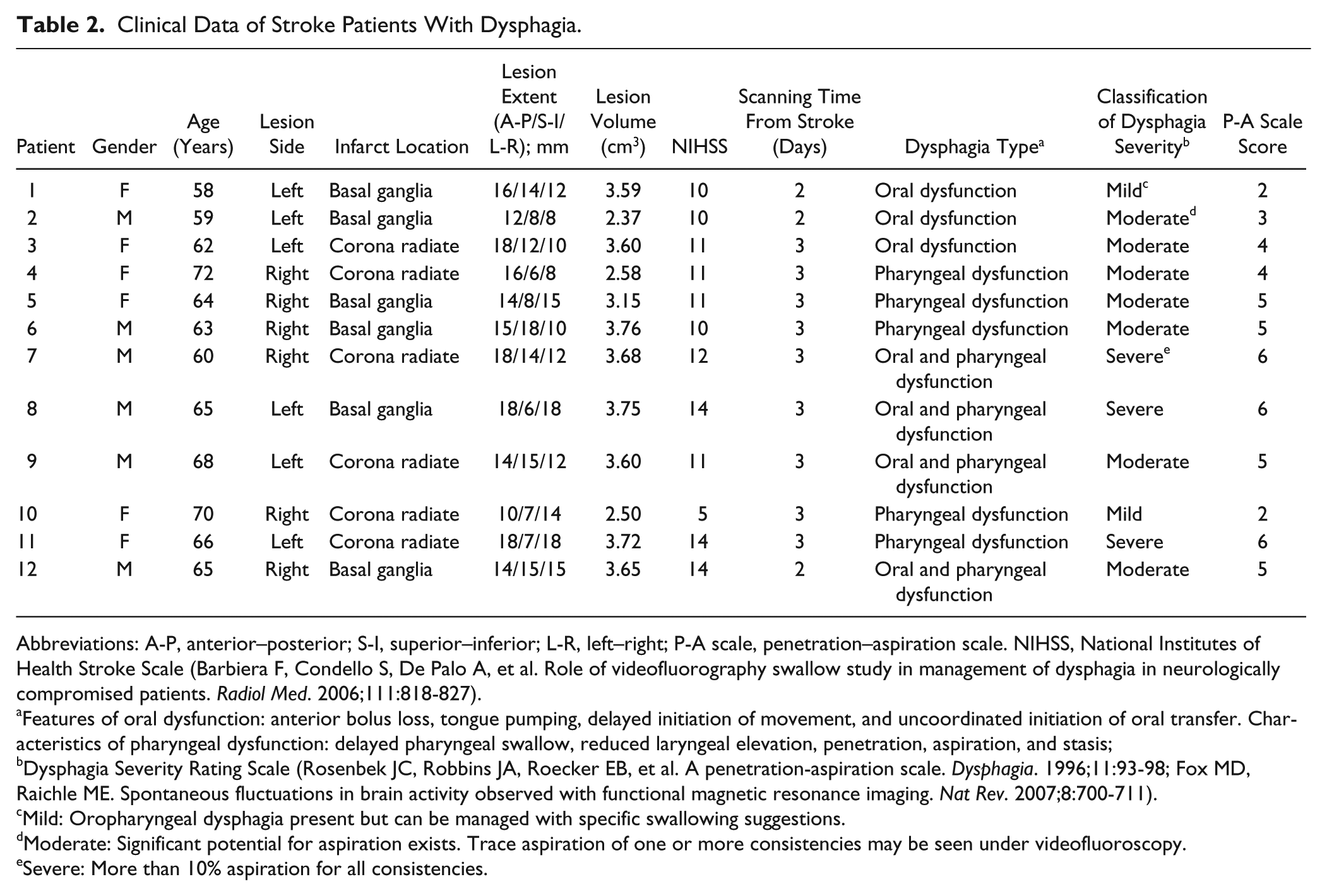
Abbreviations: A-P, anterior–posterior; S-I, superior–inferior; L-R, left–right; P-A scale, penetration–aspiration scale. NIHSS, National Institutes of Health Stroke Scale (Barbiera F, Condello S, De Palo A, et al. Role of videofluorography swallow study in management of dysphagia in neurologically compromised patients. Radiol Med. 2006;111:818-827).
Features of oral dysfunction: anterior bolus loss, tongue pumping, delayed initiation of movement, and uncoordinated initiation of oral transfer. Characteristics of pharyngeal dysfunction: delayed pharyngeal swallow, reduced laryngeal elevation, penetration, aspiration, and stasis;
Dysphagia Severity Rating Scale (Rosenbek JC, Robbins JA, Roecker EB, et al. A penetration-aspiration scale. Dysphagia. 1996;11:93-98; Fox MD, Raichle ME. Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat Rev. 2007;8:700-711).
Mild: Oropharyngeal dysphagia present but can be managed with specific swallowing suggestions.
Moderate: Significant potential for aspiration exists. Trace aspiration of one or more consistencies may be seen under videofluoroscopy.
Severe: More than 10% aspiration for all consistencies.
Twelve stroke patients were defined as having normal swallowing function with P-A scale scores of 0. Across all the patients with lesions, there was no significant difference in the distribution of brain infarction between the left and right hemispheres. Additionally, there was no significant difference in the degree of severity of dysphagia between left and right hemispheric stroke patients (P > .05).
Functional Connectivity Analysis
Seed-Based Functional Connectivity Map
Significant clusters were visualized on the MNI (Montreal Neurological Institute) template as illustrated in Figures 1 to 4. These figures indicate that clusters that were significantly correlated with the seed ROIs were found in various cortical and subcortical structures. Within-group functional connectivity patterns were revealed by one-sample t test in the control group, the stroke with dysphagia group, and the stroke without dysphagia group (Figures 1 and 2). Intergroup functional connectivity alterations were detected by comparing pairs of groups: stroke without dysphagia versus control, stroke with dysphagia versus control, and stroke with dysphagia versus stroke without dysphagia (Figures 3 and 4).
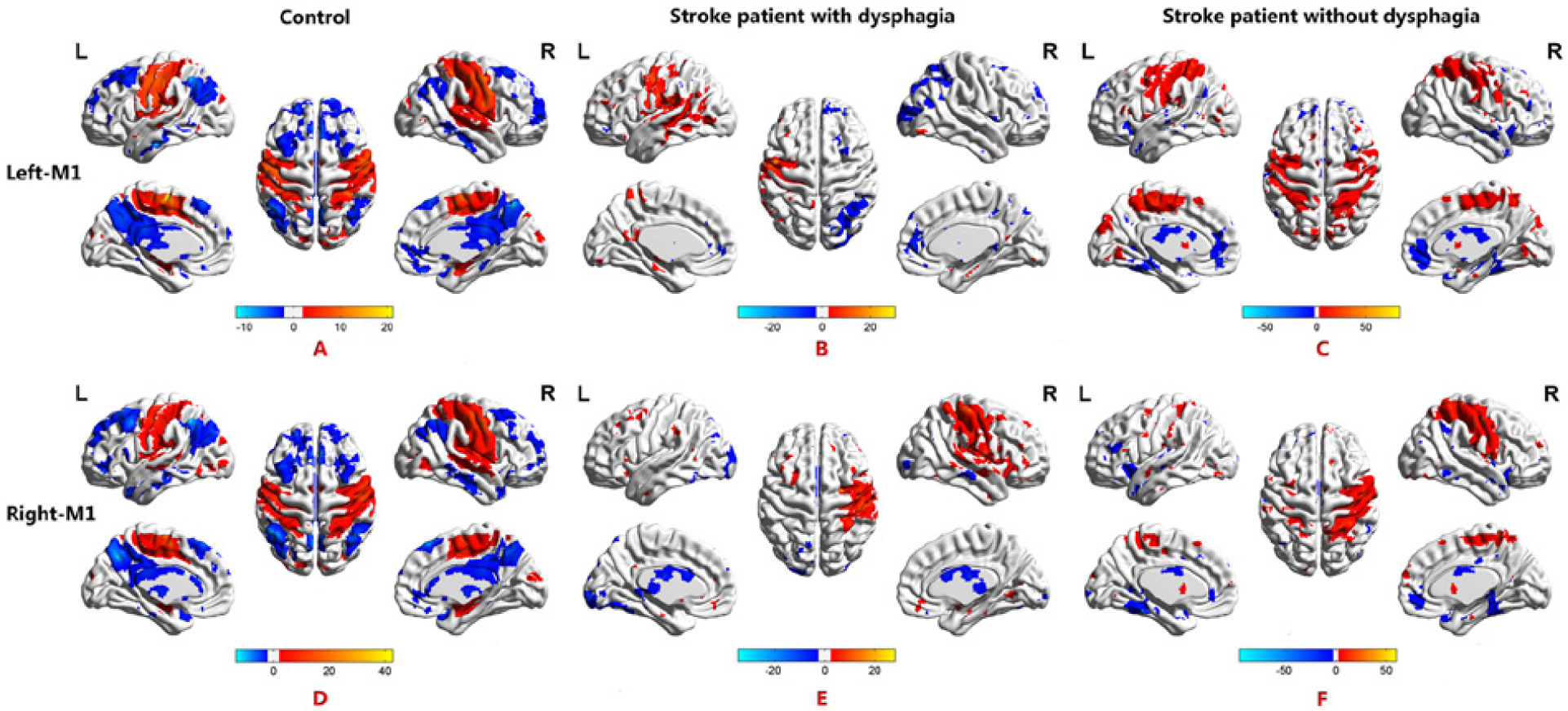
Functional connectivity maps of the seed-based analysis of the primary motor cortex (M1). (A, D) In controls, positive functional connectivity was found in the bilateral sensorimotor-insula-putamen circuits, including the primary motor cortex (BA 4), primary somatosensory cortex (BA 3 and 2), supplementary motor cortex (BA 6), middle frontal cortex (BA 10), middle cingulate gyrus, insula (BA 24 and 13), putamen and thalamus. (B, E) In stroke patients with dysphagia, positive functional connectivity was found in the left BA 4, BA 40, BA 41, BA 13, and the thalamus and in the right BA 3 from seed-based analysis of the left M1; and positive functional connectivity was found in the right BA 6, BA 40, and the putamen and in the left BA 6 from seed-based analysis of the right M1. (C, F) In stroke patients without dysphagia, positive functional connectivity was found in the left BA 6, BA 40, and BA 24 from seed-based analysis of the left M1. Positive functional connectivity was found in the right BA 4, BA 6, BA 3, and left BA 2 and BA 40 from seed-based analysis of the right M1.
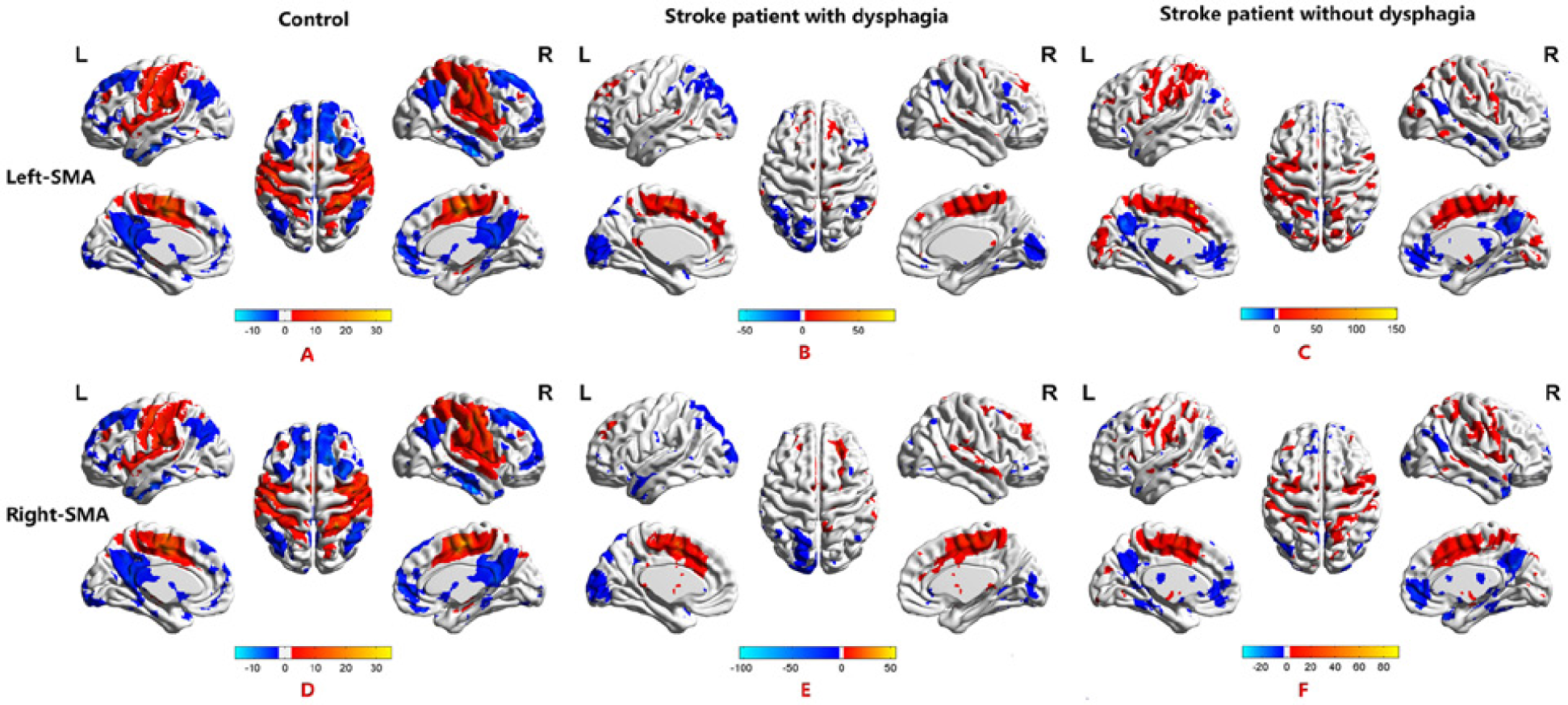
Functional connectivity maps of the seed-based analysis of the supplementary motor area (SMA). (A, D) In controls, positive functional connectivity was found in the bilateral sensorimotor-insula-putamen circuits, including BA 4, BA 3 and 2, BA 6, BA 10, BA 24 and BA 13, and in the putamen and thalamus. (B, E) In stroke patients with dysphagia, positive functional connectivity was found in the left BA 6, BA 24, and thalamus and in the right putamen from seed-based analysis of the left SMA; and positive functional connectivity was found in the right BA 6, BA 24 and in the left BA 40 from seed-based analysis of the right SMA. (C, F) In stroke patients without dysphagia, positive functional connectivity was found in the left BA 6 and in the right BA 13, BA 24, and the putamen from seed-based analysis of the left SMA; and positive functional connectivity was found in the left BA 6 and in the right BA 13 and the putamen from the seed-based analysis of the right SMA.
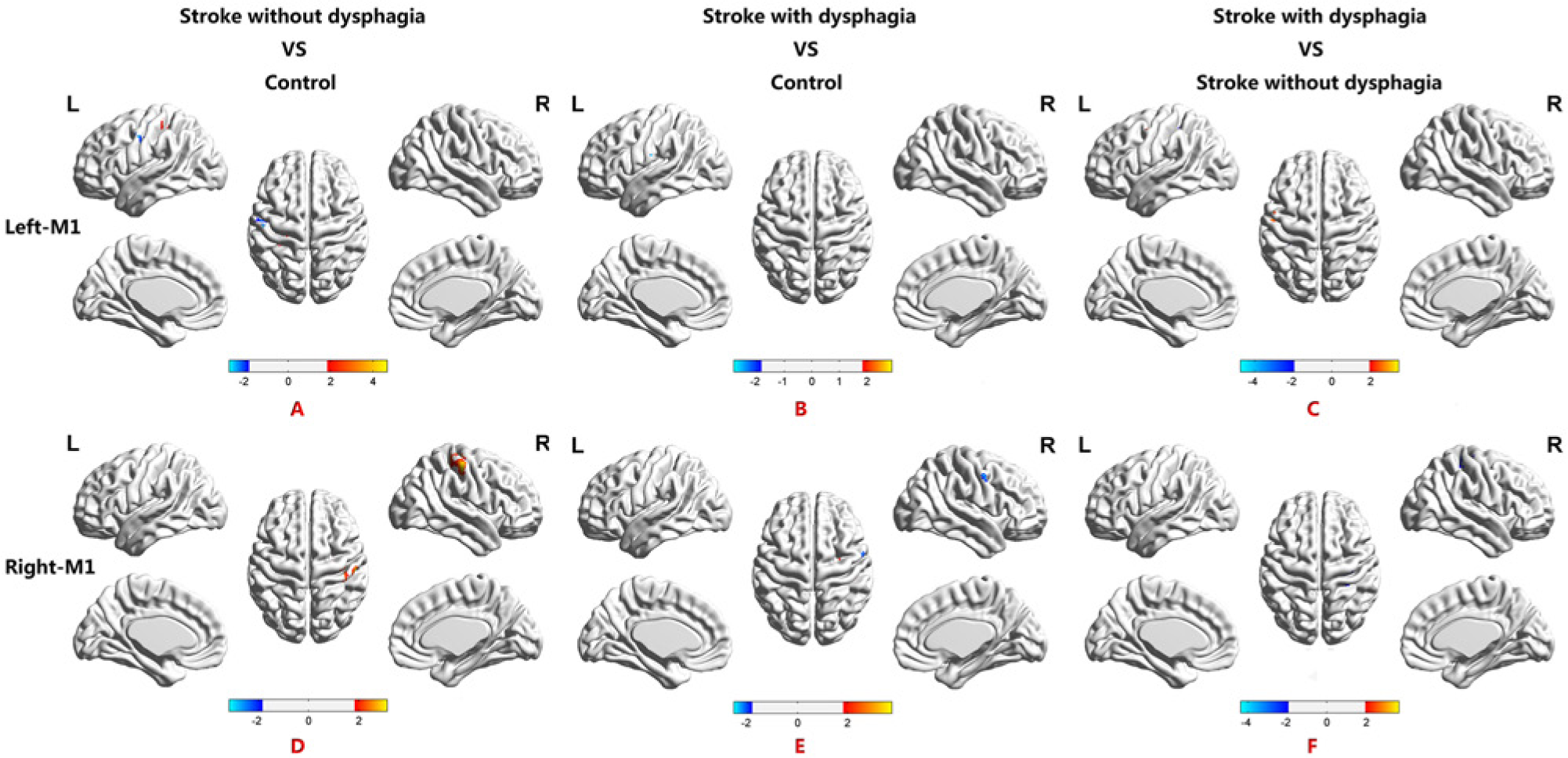
Maps of the intergroup differences in functional connectivity from seed-based analysis of the primary motor cortex (M1). (A, D) Differences in the functional connectivity maps from seed-based analysis of M1 examined using group analysis comparing the stroke without dysphagia group with healthy control subjects. Compared with controls, the number of connections was decreased in the left BA 4 and BA 43 the number of connections were increased in the left BA 40 based on the strength of the left M1 seed-based analysis in stroke without dysphagia. Based on the right M1 seed-based analysis, only the right putamen showed a decreased number of connections, and the right BA 2, BA 4 and BA 40 showed an increased number of connections. (B, E) Functional connectivity maps illustrating group differences from seed-based analysis of M1 for the comparison of the stroke with dysphagia group to healthy controls subjects. Compared with controls, seed-based analysis of the left M1 functional connectivity map showed a significantly decreased connection in the left BA 1 and an increased connection in the left BA 4 in the stroke with dysphagia group. Seed-based analysis of the right M1 functional connectivity map showed a significantly decreased connection in the right BA 3 and BA 4 and an increased connection in the right BA 2 and BA 40. (C, F) Functional connectivity map indicating group differences from seed-based analysis of M1 for the comparison of the stroke with dysphagia subjects to the stroke without dysphagia subjects. Compared to stroke without dysphagia, seed-based analysis of the left M1 functional connectivity map showed a significantly increased connection in the left BA 3 and BA 43 in stroke without dysphagia. Seed-based analysis of the right M1 functional connectivity map showed significantly decreased connections in the right BA 3 and BA 4 and increased connections in the putamen. (The detailed distribution of functional connectivity in Brodmann Areas of seed-based analysis of M1 for intergroups comparisons refers to Table 3.)
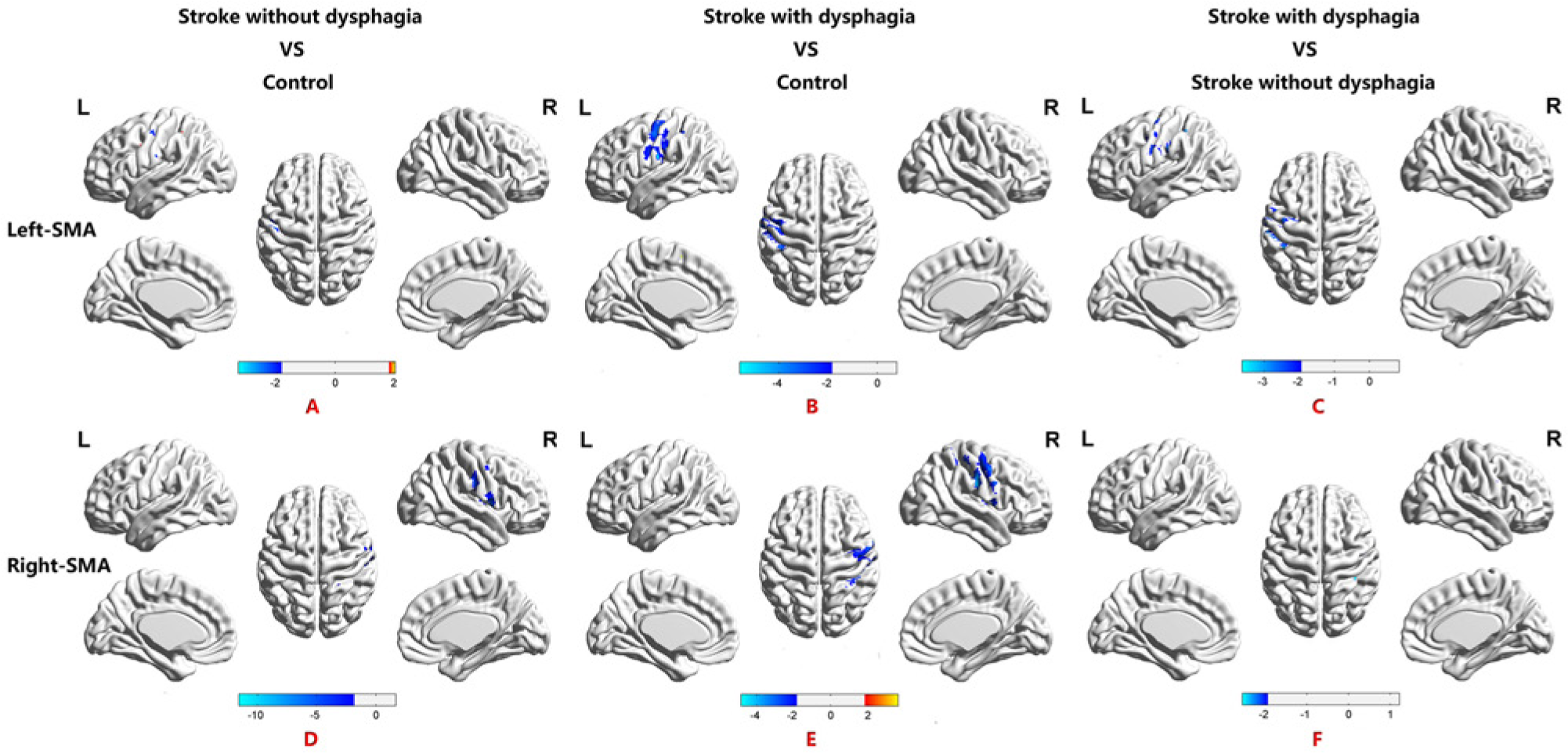
Maps of the intergroup differences in functional connectivity from seed-based analysis of the supplementary motor area (SMA). (A, D) Differences in the functional connectivity maps from seed-based analysis of SMA were examined using group analysis of stroke without dysphagia compared to healthy controls subjects. In comparison to controls, seed-based analysis of the left SMA functional connectivity map showed significantly decreased connections in the left BA 3 and the right BA 4. Seed-based analysis of the right SMA functional connectivity map showed significantly decreased connections in the right BA 3, BA 4, BA 13, and the putamen in the stroke without dysphagia group compared with controls. (B, E) Functional connectivity map illustrating group differences from seed-based analysis of SMA for the comparison of stroke with dysphagia to healthy control subjects. Compared to controls, seed-based analysis of the left SMA functional connectivity map showed significantly decreased connections in the left BA 3, BA 2, BA 4, BA 6, and BA 13 in the stroke with dysphagia group. Seed-based analysis of the right SMA functional connectivity map showed significantly increased connections in the right BA 2 and BA 4. (C, F) Functional connectivity map indicating group differences from seed-based analysis of SMA for the comparison of stroke with dysphagia subjects to stroke without dysphagia subjects. Compared to stroke without dysphagia, seed-based analysis of the left SMA functional connectivity map showed significantly decreased connections in the left BA 3, BA 4, BA 6, BA 40 and BA 13. Seed-based analysis of the right SMA functional connectivity a map showed significantly decreased connections in the right BA 6 and putamen. (The detailed distribution of functional connectivity in Brodmann Areas of seed-based analysis of SMA for intergroup comparisons refers to Table 4.)
Distributions for intergroup comparisons of the seed-based analyses of M1 and SMA in Brodmann areas are shown in Tables 3 and 4, respectivley.
Seed-Based Analysis of the Primary Motor Cortex (M1) for Intergroup Comparisons: Distribution of Functional Connectivity During Resting-Stage Functional Magnetic Resonance Imaging in Brodmann Areas.
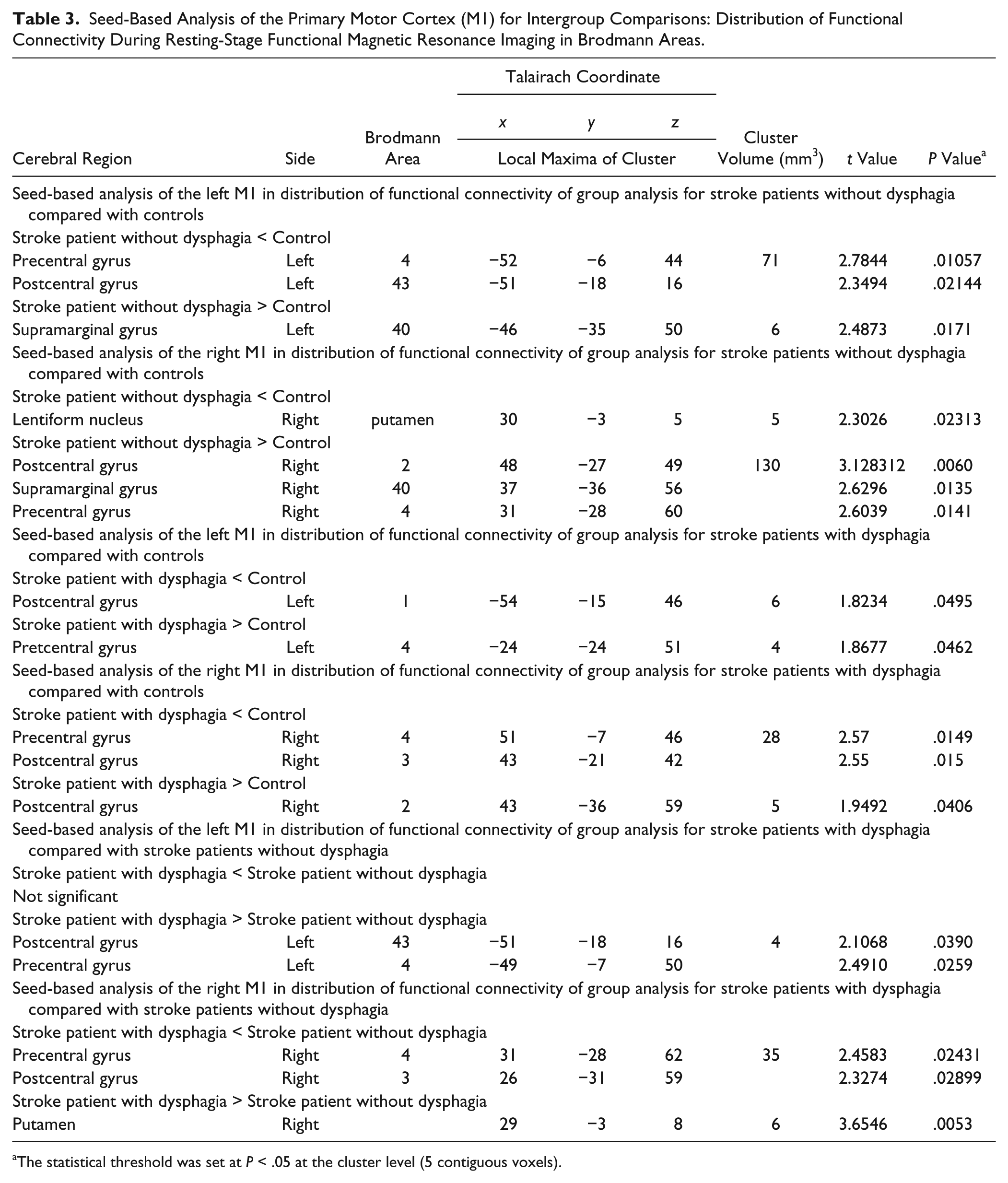
The statistical threshold was set at P < .05 at the cluster level (5 contiguous voxels).
Seed-Based Analysis of the Supplementary Motor Area (SMA) for Intergroup Comparisons: Distribution of Functional Connectivity During Resting-Stage Functional Magnetic Resonance Imaging in Brodmann Areas.
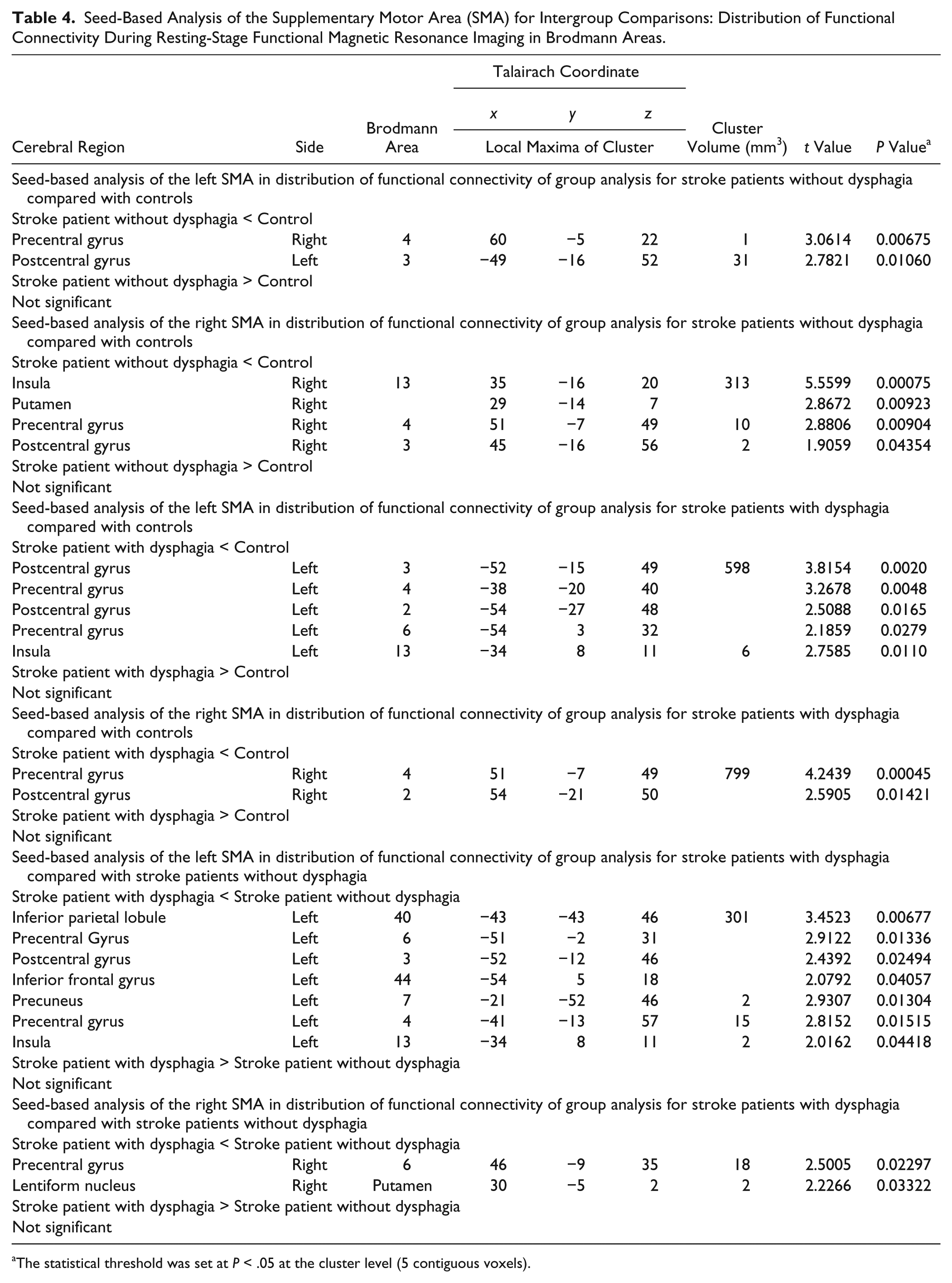
The statistical threshold was set at P < .05 at the cluster level (5 contiguous voxels).
Swallowing-Related Functional Connectivity Network
We used a complementary analysis on predefined ROIs to determine alterations in the swallowing-related functional connectivity network. The use of predefined ROIs avoids the bias of seed selection in the seed-based functional connectivity analysis. Two-sample t tests were performed to investigate the differences in functional connectivity of the 20 ROIs among 3 groups (Figure 5). Regions demonstrating significant positive connections in the bilateral sensorimotor-insula-putamen circuits, including bilateral BA 4, 6, 2, 3, 13, and 32, putamen and thalamus (Figure 5A), were used as controls. Across the 20 seed-based analyses, increased connections were observed within the right BA 3/BA 22, BA 4/BA 22, BA 6/BA 22, and the right BA 32/left putamen in stroke with dysphagia, when compared with stroke without dysphagia (Figure 5F, and the matrix diagram data in the online supplementary material file : Supplementary Figure 1).
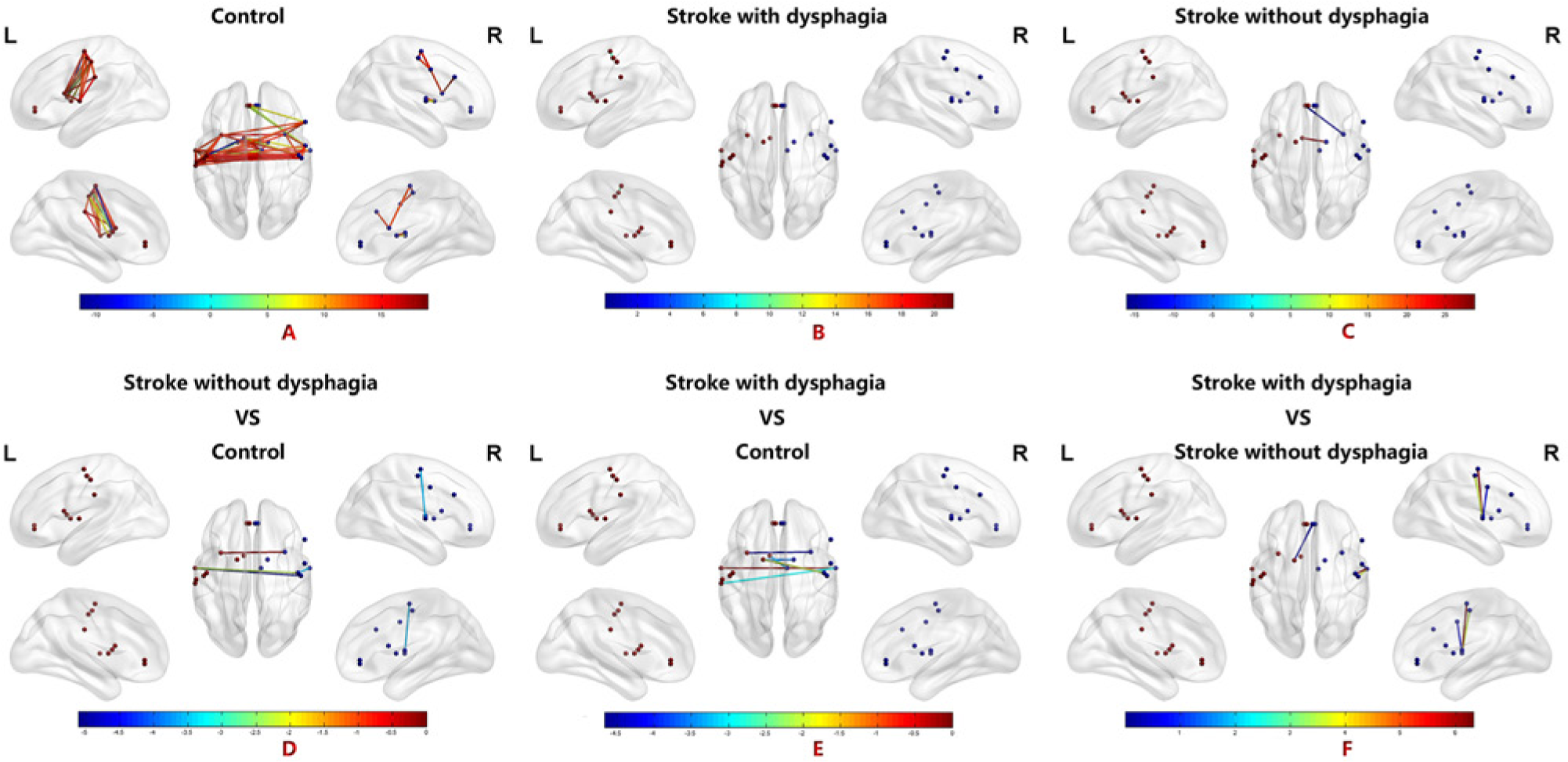
A functional network based on 20 regions of interest (ROIs) in stroke patients and healthy controls. (A) Significant functional connectivity was found in the controls. Functional connectivity of the 20 ROIs for the controls showed a significant increase in bilateral sensorimotor-insula-putamen circuits, including bilateral BA 4, BA 6, BA 2, BA 3, BA 13, and BA 32 as well as the putamen and thalamus. (B) Significant functional connectivity in stroke with dysphagia. A significant number of positive connections were observed between the right BA 10 and the thalamus, the right BA 13 and the left BA 32, the left BA 6 and BA 3, and the left BA 32 and BA 10 in stroke with dysphagia. (C) Significant functional connectivity in stroke without dysphagia. A significant number of positive connections were observed between the left BA 32 and BA 10 and the left thalamus and the right putamen in stroke without dysphagia. (D) Significantly altered functional connectivity in stroke without dysphagia relative to healthy comparison subjects. Compared to controls, decreased connections were observed across the 20 seed-based analyses within the right BA 3/BA 4, as well as the left BA 22, the right BA13/ left BA 13 and the right BA 4/BA 32 in stroke without dysphagia. (E) Significantly altered functional connectivity in stroke with dysphagia relative to healthy comparison subjects. Compared to controls, increased connections were observed across the 20 seed-based analyses within the right BA13/left BA 13, the right putamen /left putamen, the right thalamus/left thalamus, the right BA 22/left BA 22, and the right BA 4/left putamen in stroke with dysphagia (F) Significantly altered functional connectivity in stroke with dysphagia relative to stroke without dysphagia. Compared to stroke without dysphagia, increased connections were observed across the 20 seed-based analyses within the right BA 3/BA 22, BA 4/BA 22, BA 6/BA 22 and the right BA 32/left BA putamen.
Relationships Between the Altered Network Properties and Penetration–Aspiration Scale Scores in Stroke With Dysphagia Compared With Stroke Without Dysphagia
Based on Pearson correlation coefficients, left BA 6 and right BA 3/BA 22, BA 6/BA 22, BA 4/BA 22, and the right BA 32/left putamen were significantly (P < .05, uncorrected) positively correlated with the severity scores of the P-A scale (online supplementary material file: Supplementary Figure 2).
Structural Connectivity and Fiber Tract Analysis
Structural connections of dysphagic stroke included the left-to-right SMA and SMA to internal capsule fiber bundle. Fiber tracts in the left SMA passing through the left internal capsule showed a lateral associative bundle, the corticospinal tract, which was composed of long and short fibers connecting the supplementary motor cortex to the internal capsule via the frontal, parietal, and temporal lobes. The fiber tracts in the left SMA passing through the right SMA encountered the corpus callosum, a ventral associative bundle arising from the supplementary motor regions and going toward the right supplementary motor cortex (Figure 6A-C). When stroke patients with dysphagia were compared with controls, the mean FA showed a significant decrease in fibers passing through three ROIs (Figure 6D). Additionally, the mean FA of the seed ROIs showed a significant decrease in stroke without dysphagia compared with controls (Fig. 6D). In addition, there were no significant differences in the FA value between stroke with and without dysphagia group.
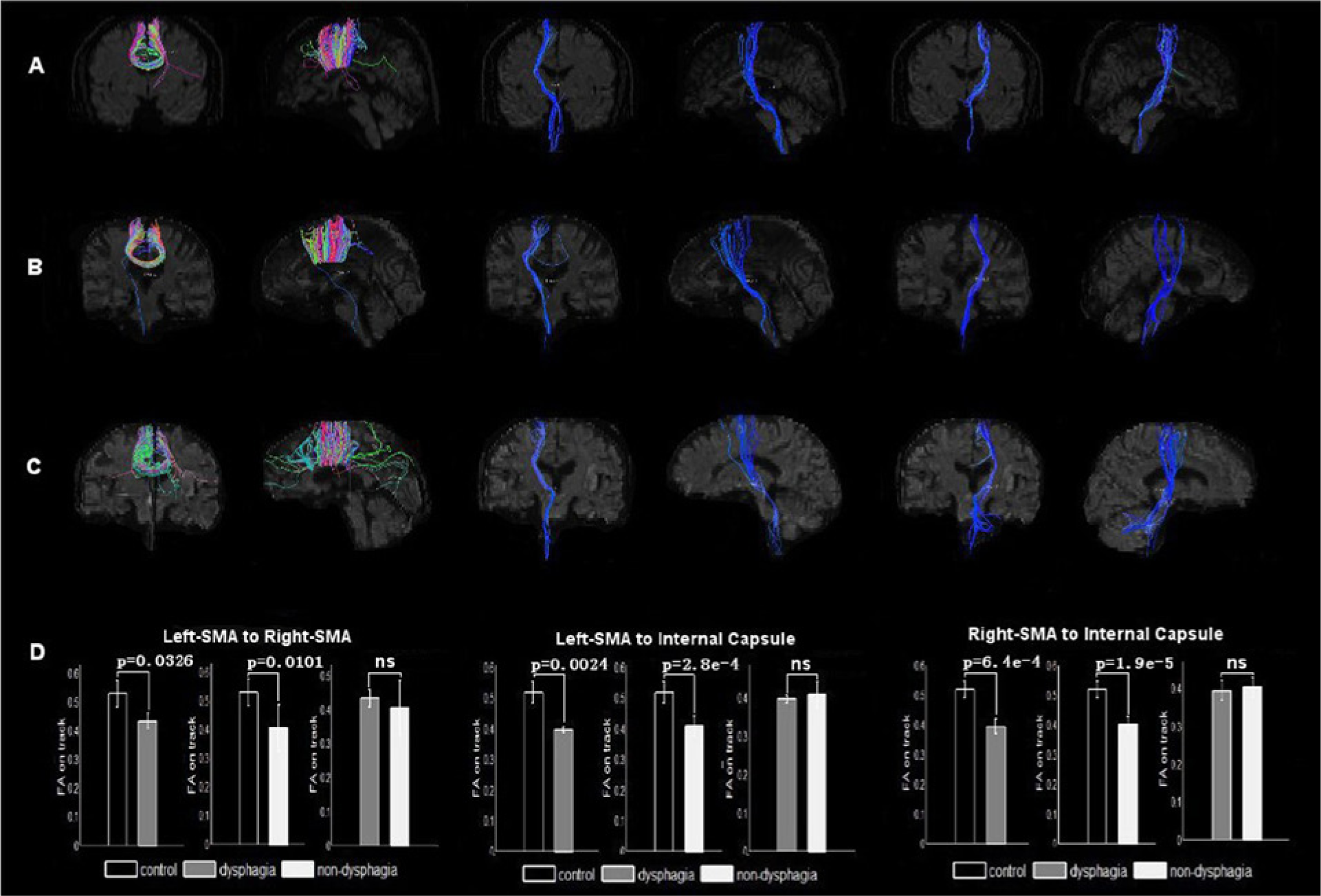
Fiber tracts of the selected regions of interest (ROIs; one subject from the control group and one subject from the stroke group for display purposes). (A). Control: Fiber tracts (corticospinal tract, CST) in the left supplementary motor area (SMA) passing through the left internal capsule; fiber tracts (corpus callosum) in the left SMA passing through the right SMA (red: mediolateral plane, green: dorsoventral orientation, blue: rostrocaudal direction). (B). Stroke with dysphagia: Fiber tracts (CST) in the left SMA passing through the left internal capsule; fiber tracts in the left SMA passing through the right SMA. (C). Stroke with dysphagia: Fiber tracts (CST) in the left SMA passing through the left internal capsule; fiber tracts in the left SMA passing through the right SMA. The color-coding of the obtained fibers is based on the standard RGB code applied to the vector at every segment of each fiber (red: mediolateral plane, green: dorsoventral orientation, blue: rostrocaudal direction). In (A), (B), and (C), the color-coding of the obtained fibers is based on the standard RGB code applied to the vector at every segment of each fiber (red: mediolateral plane, green: dorsoventral orientation, blue: rostrocaudal direction). (D) Bars represent the mean fractional anisotropy (FA) values. Vertical bars indicate estimated standard errors. Comparing stroke patients with dysphagia to controls, the mean FA showed a significant decrease in fibers passing through three ROIs. The mean FA of the seed ROIs showed no significant change in stroke without dysphagia compared with the controls.
Discussion
To the best of our knowledge, this is the first study to demonstrate swallowing-related changes in functional and structural connectivity patterns in brain networks using resting-state fMRI and DTI in stroke with dysphagia. Our investigation revealed 3 main findings: (a) to directly explore resting-state functional connectivity between M1, SMA and motor regions of the whole brain; (b) to provide supporting evidence for the bilateral redistribution of swallowing networks after stroke occurrence based on functional connectivity network analysis of 20 swallowing-related ROIs; and (c) to assess resting-state fMRI in combination with DTI, which allowed us to examine all aspects of functional and structural change in stroke patients with dysphagia.
First, the present study attempted to directly explore resting-state functional connectivity between M1, SMA, and motor regions of the whole brain as well as the relationship between altered connectivity and fiber structure in stroke patients with dysphagia.
Previous data support the notion that M1 and SMA are involved in the motor control of pharyngeal swallowing.5,7,9,10,12,24 In terms of the cortical motor control of human swallowing, M1 is closely linked to the control of the tongue and face, so the presence of swallowing activity in this region is associated with the initiation of swallowing.12,25 We explored SMA as it is related to motor planning and, in particular, planning of sequential movements 25 as occurs with oropharyngeal swallowing. Several previous studies support the idea that unilateral hemispheric lesions may result in dysphagia. However, hemispheric dominance for swallowing is still unclear and so we chose to use bilateral ROIs as seeds in the analysis.13,15,16 As hemispheric dominance in swallowing is still under debate, 13 bilateral seeds were used to increase the statistical power. Our preliminary studies have both concluded that lesions in the left hemisphere may be more disruptive to swallowing behavior than similar lesions in the right hemisphere.2,10 Therefore, we reversed the maps from the right lesion to left and combined these with the maps from the left hemisphere stroke group, and we computed the z-score correlation maps by means of arithmetic subtraction. In this manner, we were able to display the differences in correlation patterns for the left and right cerebral seed regions using the left stroke lesion with or without dysphagia compared with healthy controls.
Through this approach, we first provided evidence that altered functional connectivity mainly occurs in the motor cortex–subcortical circuits, which are strongly associated with the swallowing function.
In our study, we assumed a remodeled network between the M1, SMA, and the basal ganglia–thalamus. First of all, an increased connection between left M1 and BA 3/BA 43 reflects oropharyngeal sensory processing and underscores the importance of afferent information in the regulation of swallowing. Second, deceased connections from M1 and SMA to BA 4, BA 6, BA 40, and BA 13 were connected with weakened the pharyngoesophageal components of deglutition in “priming” swallowing. The former could be understood as one of physiological compensation mechanisms adapting to stroke. The latter, presented as an impairment of the connection in the lesion-containing hemisphere in dysphagic stroke patients. The SMA and basal ganglia are involved in motor representations and the temporal sequence control of movement, and the basal ganglia–thalamus is anatomically connected with the motor cortex. 26 The basal ganglia functionally connect the cerebral cortex and the thalamus and may be involved in gating sensory input to achieve motor control. 27 These data are consistent with the view that voluntary swallowing is represented within distributed networks of functionally distinct cortical foci that participate in the control of swallowing.
Second, this study also provides supporting evidence for the bilateral redistribution of swallowing networks after stroke occurrence based on functional connectivity network analysis of 20 swallowing-related ROIs. The findings suggest that the particular functional connectivity network plays a vital role in swallowing processing. Compared to stroke without dysphagia, increased connections were observed across the 20 seed-based analyses within the right BA 3/BA 22, BA 4/BA 22, BA 6/BA 22, and right BA 32/left BA putamen. The above results reported here could not be fully account for which approach, that is, seed-based functional connectivity maps analysis or 20 ROIs network analysis, is more reliable. The 2 analyses are different from each other in procedure, mode and method with different value orientations as a result of clinical significance. Factors contributing to the varying functional connectivity may involve reversing the maps from the right lesion to left, different analytical statistical procedure and different signal processing due to seed-based functional connectivity maps or multi-ROIs network. Therefore, the correlation between functional connectivity and P-A score was also analyzed.
Interestingly, we found that the distinct network properties of swallowing-related ROIs were positively correlated with the severity of P-A scale scores in stroke patients with dysphagia compared with stroke without dysphagia. Higher scores were associated with an increasing correlation between right BA 4/BA 22, BA 3/BA 22, BA 3/BA 22, and right BA 32/left putamen. Previous experimental approaches have indicated that M1 and SMA share a considerable amount of common information from the cingulate cortex, including the rostral and caudal cingulate motor areas. 28 We suggest that the rostral cingulate motor areas (BA 32 and BA 22), which are among the higher order motor areas of the cortex, play a part in processing motor selection in the swallowing function. Specifically, the relationship between these altered network properties and P-A scale scores showed a significant positive correlation. As has been mentioned, positive functional connectivity may indicate synchronization between different brain regions. We hypothesized that the increased positive functional connectivity found in stroke with dysphagia was associated with the severity of dysphagia, and this may reflect an impairment of the balance between the networks of 20 ROIs that are related to swallowing function.
Last but not least, strength of this study lies in the fact that we have assessed resting-state fMRI in combination with DTI, which allowed us to examine all aspects of functional and structural change in stroke patients with dysphagia.
In the ROI fiber tracking analysis, a distinct pattern of changes in diffusion parameters within the ROIs was revealed in stroke patients. From this first study, we determined that in stroke patients with or without dysphagia, FA was more sensitive and specific than conventional MR for detecting these structural changes and was able to show abnormal diffusion in the white matter, bilateral corticospinal tract and corpus callosum. These abnormalities could be explained by the reduced cortical functional connectivity in stroke patients.
We initially hypothesized that the abnormalities in the white matter would reflect key structural abnormalities responsible for disrupting planning of sequential movements associated with swallowing after stroke. However, although we found clear differences between controls and stroke patients, there were no significant differences between patients with and without dysphagia. One possibility is that the sample size was too small. Based on our data, we estimate that about 50 patients in each group would be required to find a clear difference.
Consequently, these results indicate that dysphagia secondary to stroke is associated with disruptive functional and structural integrity in the large-scale brain motor system, thus providing new insights into the neural remodeling of this disorder. Because of our relatively small patient sample size, we must interpret our results cautiously; however, our study offers an interesting a priori hypothesis to be tested in future larger studies. Importantly, these initial results may provide guidance for future interventions in the treatment of poststroke dysphagia. The current treatment for dysphagia includes prevention of aspiration in the form of diet and fluid modifications, compensatory maneuvers, position changes and rehabilitation exercises. Recent studies using transcranial magnetic stimulation have demonstrated the presence of a direct corticobulbar projection from the motor cortex to swallowing muscles.29-33 The results of these studies suggest that the addition of cortical stimulation increased the speed of recovery from dysphagia and motor disability caused by cortical damage. Our study established the optimal target, particularly such as bilateral BA 4, BA 6, BA 2, BA 32, and BA 22, for precise cortical stimulation; thus, it might represent a useful therapeutic approach for the treatment of poststroke dysphagia.
The present study has several limitations. First, we only focused on stroke patients who experienced middle artery infarction with dysphagia. It may have been informative to study different lesion sites in stroke patients with or without dysphagia. The present study is the first to investigate functional and structural connectivity in stroke with dysphagia, and we preferentially selected patients with a probable or definite disease to decrease clinicopathological heterogeneity. Second, although the M1 and SMA are involved in the motor control of pharyngeal swallowing, both streamline deterministic and probabilistic methods were employed to perform the fiber tracking, and these found no statistical difference among the groups in the fiber count or FA value between bilateral M1. The reasons that significant white fiber could not be tracked using M1 in the subjects in this study are not clear. This limitation may be due to the position of our ROI at anatomical coordinates (MNI: −58, −16, 44; −48, −9, 54), which, according to the previous study, were located closer to the cortex and thus could not be used to track white matter fibers between the bilateral cerebral hemispheres. Further limitations include the probability that functional ROI might be located in the lesion, which may have an effect on connectivity in the present study. Finally, although possible confounding variables such as age, lesion location, and disease duration were carefully matched between groups, we acknowledge the modest sample size of this study and recognize that a large cohort study would be required to verify the current findings.
Conclusions
To the best of our knowledge, this is the first study documenting the combined acquisition of functional MRI and DTI in stroke patients with dysphagia. We sought to develop an altered neuroanatomical model of dysphagia throughout the brain. In addition to improving our understanding of the neural control of normal healthy swallowing, this new technique will enable visualization of the altered neural components of swallowing abnormalities in stroke patients with dysphagia and thus allow the development of effective direct clinical treatment strategies. This study increases our knowledge of the changes that occur in the brains of stroke patients with dysphagia and highlights the close relationship between functional and structural changes. In future trials, we aim to investigate discrete disease-causing lesions in other parts of the complex sensorimotor network that regulate the act of swallowing.
Supplemental Material
supplementary_material_file – Supplemental material for Altered Resting-State Functional and White Matter Tract Connectivity in Stroke Patients With Dysphagia
Supplemental material, supplementary_material_file for Altered Resting-State Functional and White Matter Tract Connectivity in Stroke Patients With Dysphagia by Shasha Li, Zhenxing Ma, Shipeng Tu, Muke Zhou, Sihan Chen, Zhiwei Guo, Qiyong Gong, Li He, Xiaoqi Huang, Dezhong Yao, Su Lui, Bo Yu, Xiaotong Wang, Dong Zhou and Chengqi He in Neurorehabilitation and Neural Repair
Supplemental Material
supp_1 – Supplemental material for Altered Resting-State Functional and White Matter Tract Connectivity in Stroke Patients With Dysphagia
Supplemental material, supp_1 for Altered Resting-State Functional and White Matter Tract Connectivity in Stroke Patients With Dysphagia by Shasha Li, Zhenxing Ma, Shipeng Tu, Muke Zhou, Sihan Chen, Zhiwei Guo, Qiyong Gong, Li He, Xiaoqi Huang, Dezhong Yao, Su Lui, Bo Yu, Xiaotong Wang, Dong Zhou and Chengqi He in Neurorehabilitation and Neural Repair
Supplemental Material
Supp_2 – Supplemental material for Altered Resting-State Functional and White Matter Tract Connectivity in Stroke Patients With Dysphagia
Supplemental material, Supp_2 for Altered Resting-State Functional and White Matter Tract Connectivity in Stroke Patients With Dysphagia by Shasha Li, Zhenxing Ma, Shipeng Tu, Muke Zhou, Sihan Chen, Zhiwei Guo, Qiyong Gong, Li He, Xiaoqi Huang, Dezhong Yao, Su Lui, Bo Yu, Xiaotong Wang, Dong Zhou and Chengqi He in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The authors acknowledge support from State Key Laboratory of Biotherapy and HMRCC, West China Hospital, Sichuan University. We thank all of the participants for their cooperation. We are also most grateful to Dr Cheng Lou for his collaboration and assistance.
Authors’ Note
Shasha Li and Zhenxing Ma have contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Basic Research Program of China (973 Program Nos. 2011CB707803 and 2007CB512305), the Natural Science Foundation of China (Grant Nos. 81000852, 81030027, 30625024, 61175117, and 30900361), the National High Technology Program of China (863 Program No. 2008AA02Z408), the PCSIRT project (No. IRT0910), the 111 project (No. B12027), the Doctor Training Funding of MOE (No. 20100185110016), the Research Foundation of Zhejiang Province (Grant No. 201022896), and the Supporting Project of Science & Technology of Sichuan Province (Grant No. 2012SZ0140).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.