
Abstract
Background. The Nociception Coma Scale–Revised (NCS-R) was recently validated to assess possible pain perception in patients with disorders of consciousness. Objective. To identify correlations between cerebral glucose metabolism and NCS-R total scores. Methods. [18F]-fluorodeoxyglucose positron emission tomography, NCS-R, and Coma Recovery Scale–Revised assessments were performed in 49 patients with disorders of consciousness. Results. We identified a significant positive correlation between NCS-R total scores and metabolism in the posterior part of the anterior cingulate cortex, known to be involved in pain processing. No other cluster reached significance. No significant effect of clinical diagnosis (vegetative/unresponsive vs minimally conscious states), etiology or interval since insult was observed. Conclusions. Our data support the hypothesis that the NCS-R total scores are related to cortical processing of nociception and may constitute an appropriate behavioral tool to assess, monitor, and treat possible pain in brain-damaged noncommunicative patients with disorders of consciousness. Future studies using event-related functional magnetic resonance imaging should investigate the correlation between NCS-R scores and brain activation in response to noxious stimulation at the single-subject level.
Keywords
Introduction
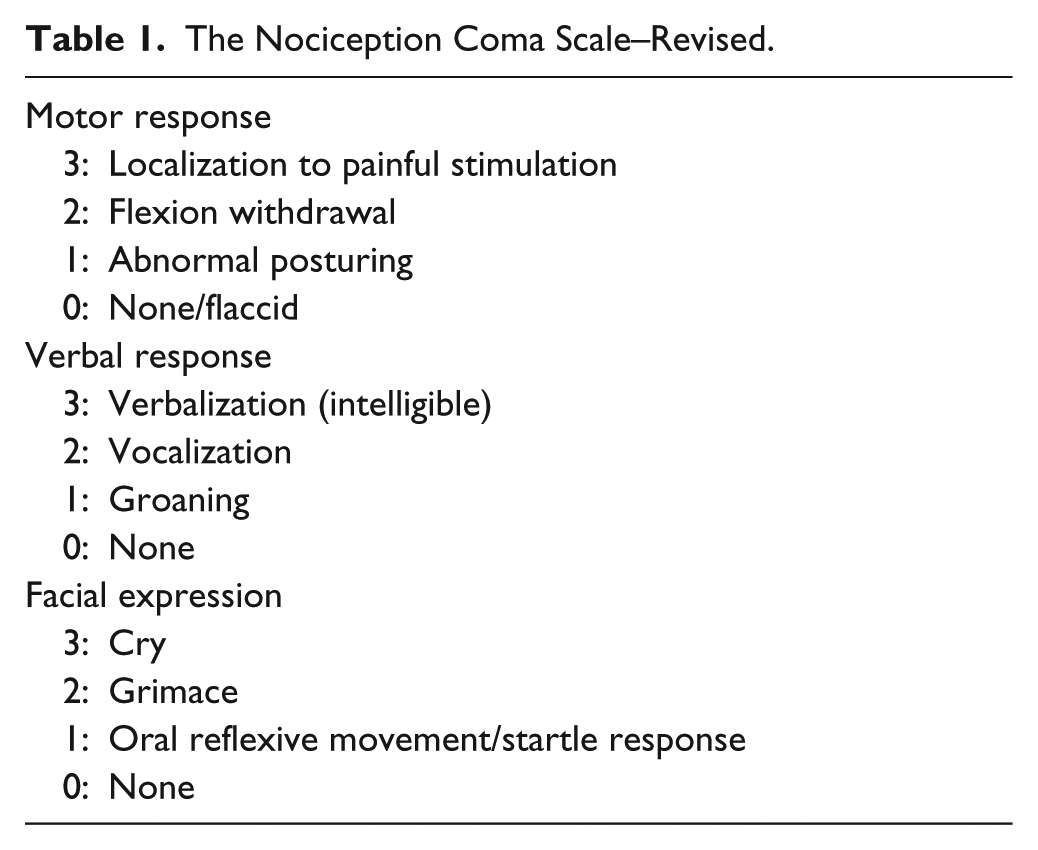
Pain management in patients with disorders of consciousness (DOC; ie, vegetative state/unresponsive wakefulness syndrome [VS/UWS] or minimally conscious state [MCS]) remains challenging, the assessment being limited by the absence of patients’ communication and subjective report, leading to ethical and medical concerns. In acute as in chronic stages, several conditions such as polytrauma, open wounds, spasticity, arthralgia, or peripheral injuries are likely to induce pain, especially during cares and mobilization. Numerous behavioral scales have been developed for noncommunicative patients such as severely demented patients and newborns. We recently proposed a simple, standardized, behavioral “pain” scale adapted to noncommunicative severely brain-damaged patients, the Nociception Coma Scale–Revised1,2 (NCS-R). It is composed of 3 subscales, motor, verbal, and facial expression responses with a total score ranging from 0 to 9 (see Table 1). Here, we investigate which brain regions show a correlation in metabolism with NCS-R total scores in a cohort of patients with DOC (n = 49) assessed by [18F]-fluorodeoxyglucose positron emission tomography (FDG-PET).
The Nociception Coma Scale–Revised.
Methods
Positron emission tomography was performed during resting conditions after intravenous injection of 5 to 10 mCi (185-370 MBq) FDG on a Gemini Big Bore PET/CT scanner (Philips Medical Systems, Best, Netherlands). On the day of PET scanning, a standardized assessment of the patient’s behavioral response to noxious stimulation was performed using the NCS-R. 2 In brief, a pressure of 52 ± 8 N was applied during 5 seconds on the nail bed of the left and right middle fingers in randomized order using a Newton-meter (Force Dial, FDN 200 model, Wagner Instruments, Greemwich, CT). The best limb motor, verbal, and facial expression response was scored (see Table 1) 10 seconds after each noxious stimulus. Patients’ clinical diagnosis was based on the best score obtained from repeated Coma Recovery Scale–Revised 3 (CRS-R) assessments (performed on day of scanning, and 2 days before and 2 days after).
Positron emission tomography data were spatially normalized and smoothed using a 16 mm full width at half maximum Gaussian kernel. Statistical analyses were performed using Statistical Parametric Mapping (SPM8; www.fil.ion.ucl.ac.uk/spm). T-contrasts identified positive and negative linear correlations between regional brain metabolism and NCS-R total scores. Differences in the level of consciousness (ie, CRS-R total scores), diagnosis (ie, VS/UWS vs MCS), etiology (ie, traumatic vs nontraumatic), and interval since insult (ie, acute/subacute vs long-standing; >1 year postinsult) were modeled as additional covariates in the design matrix. Global normalization was performed by proportional scaling. Thresholding of results was done at P < .05 corrected for multiple comparisons within a priori defined regions of interest (using a 10-mm radius spherical small volume correction in SPM—at voxel and cluster level) centered on a priori coordinates for areas previously identified as the most frequently identified in pain processing (ie, anterior cingulate cortex (ACC) and bilateral insula 4 ; respective coordinates x = 12, y = 10, z = 36; x = −34, y = −24, z = 36; and x = 34, y = −24, z = 36, were taken from an independent study on pain perception 5 ). The study was approved by the Ethics Committee of the University Hospital of Liège and written informed consent was obtained from the legal representative of all patients.
Results
Forty-nine patients were included in the study (33 males; aged 43 ± 17 years; 25 ± 31 months postinsult; 21 traumatic; 28 MCS; 26 in an acute/subacute stage (ie <1 year postinsult); see Supplementary Table 1, available online at nnr.sagepub.com/supplemental). Voxel-based parametric analysis for the whole brain showed that the only area with a significant positive correlation with NCS-R total scores was the posterior part of the ACC (areas a24b′/c′ and 32′; Z = 2.76; corrected P = .018; MNI [Montreal Neurological Institute] coordinates x = 10, y = 2, z = 40, see Figure 1). Moreover, this area positively correlated with NCS-R and not with CRS-R total scores (Z = 2.84; corrected P = .015; MNI coordinates x = 10, y = 2, z = 38 mm). We did not find a significant effect of clinical diagnosis, etiology, or interval since insult.
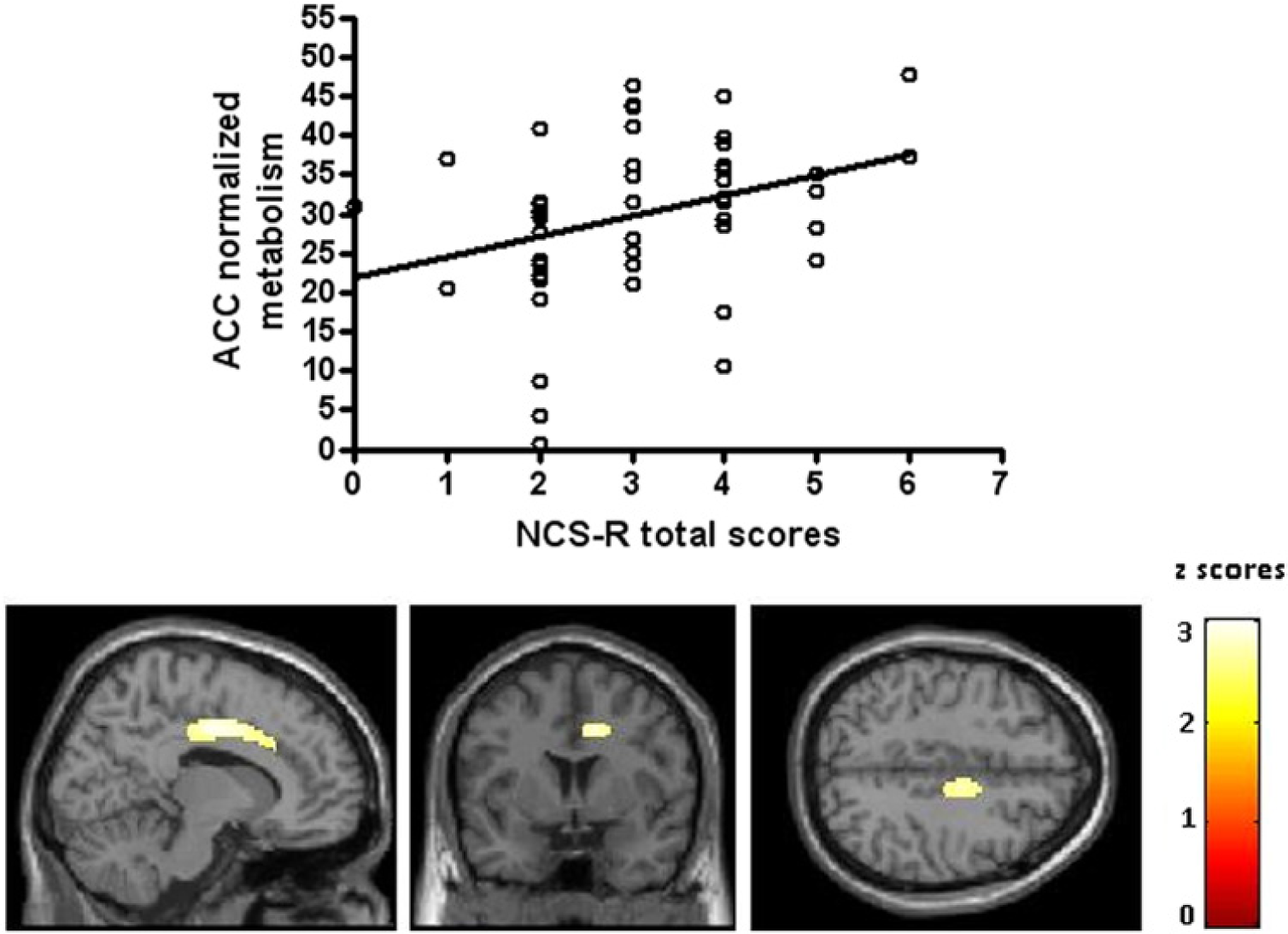
Positive correlation between Nociception Coma Scale–Revised (NCS-R) and brain metabolism. Upper panel: Plot of the effect size (normalized parameter estimates) versus the NCS-R scores (P < .05 with small volume correction for multiple comparisons). Lower panel: Sagittal (x = 14 mm), coronal (y = 4 mm), and axial (z = 43 mm) planes illustrating the peak voxel in the posterior part of the anterior cingulate cortex (ACC; areas a24b′/c′ and 32′).
Discussion
Here, we investigated which brain regions show a correlation in metabolic activity with NCS-R total scores in patients with DOC and identified the ACC. No other cluster reached significance. According to previous neuroimaging studies on pain perception, the posterior part of the ACC is part of the network involved in the cognitive and affective aspects of pain processing. 4 This region (encompassing areas a24b′/c′ and 32′) is considered to constitute a hub where information about negative reinforcers and pain can be linked to motor centers responsible for expressing affect and executing goal-directed behavior. 6 Moreover, previous studies showed that an increased activity in the ACC prior to painful stimulation was linearly associated with increased painfulness in conscious healthy volunteers, 7 and that this area showed a reduced activity during hypnosis-induced analgesia. 8 Importantly, metabolism in the cingulate cortex correlated with NCS-R total scores and not with CRS-R total scores, suggesting that the NCS-R reflects nociception and pain rather than differences in patients’ level of consciousness.
To appreciate the interest of our findings, these results need to be discussed in light of earlier functional neuroimaging studies on possible pain perception in patients with DOC. We previously reported near-normal regional cerebral blood flow increases in response to pain in an MCS group, including in the ACC. 5 In contrast, our study on a group of VS/UWS patients showed isolated primary somatosensory cortex activation to noxious stimuli, disconnected from the rest of the brain, 5 while others have reported activation up to ACC in behaviorally “vegetative” patients. 9 In the present study, we did not find an effect of the clinical diagnosis (VS/UWS vs MCS) on the correlation between ACC metabolism and NCS-R scores, supporting the idea that some behaviorally “unconscious” patients might actually show higher cortical processing. Given the high rate of misdiagnosis reported in this population, 10 we think it is important to use a sensitive scale to manage possible pain in every patient with DOC independently of their clinical diagnosis at bedside. It has, however, to be noted that there is a variability in the observed correlation that is inherent to the studied population (ie, heterogeneity of severely brain injured patients) and the subject of the study (ie, the possible subjective experience of pain).
In conclusion, our data support the hypothesis that the NCS-R is related to cortical processing of nociception and hence may constitute an appropriate behavioral tool to assess, monitor and treat for possible pain perception in patients with DOC. Future studies using event-related functional magnetic resonance imaging should investigate the correlation between NCS-R scores and brain activation in response to noxious stimulation at the single-subject level in this challenging patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Funds for Scientific Research (FNRS), Action de Recherche Concertée, James S. McDonnell Foundation, Mind Science Foundation and University of Liège.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.