
Abstract
Background. Body-weight-supported treadmill training (BWSTT) to train both fitness and ambulation has not been investigated. Objective. To compare the effectiveness of BWSTT to dose-equivalent usual care (UC) in improving cardiovascular fitness and walking early after stroke. Methods. Participants were randomly assigned to 1 of 2 interventions: BWSTT + UC or UC. All individuals participated in 60-minute physiotherapy sessions 5 times weekly as inpatients for 6 weeks and 3 times weekly as outpatients for another 6 weeks. Baseline, posttraining, 6-, and 12-month follow-up outcome measures were as follows: primary, fitness (peak oxygen consumption, VO2peak) and walking ability (6-Minute Walk Test [6MWT] and 10-m walk); secondary, Berg Balance Scale (BBS) and motor impairment (Chedoke-McMaster Stages of Recovery [CMSR] Leg and Foot). Results. In all, 50 individuals (mean age, 60 ± 14 years; mean event-to-randomization, 23 ± 5 days; 29 men) participated. No adverse events occurred. BWSTT improved VO2peak by 30%, which was significantly greater than the 8% improvement observed for UC (P = .004 between groups). Similarly, there were significant Time × Group interactions for 6MWT and CMSR Foot, with BWSTT outperforming UC for gains in distance (P = .15; 48% vs 19%, respectively) and stage (P = .01; 1.0 vs 0.3, respectively). No group effect was seen for 10-m walk speed, BBS, or CMSR Leg, with both groups demonstrating significant gains. In general, gains observed were preserved for 12 months. Conclusions. BWSTT elicits greater improvements in cardiovascular fitness and walking endurance than UC in the subacute poststroke period. These gains are largely sustained for 1 year.
Keywords
Introduction
Cardiovascular deconditioning and impaired walking ability contribute significantly to long-term disability and burden of care after stroke. Profoundly low peak oxygen consumption (VO2peak) limits the ability of people poststroke to meet the metabolic demands of daily activities. 1 One-quarter to one-third of people 3 months postonset require assistance or supervision to walk,2,3 and the vast majority remain incapable of full, independent community ambulation. 4 Impaired ambulatory ability leads to physical inactivity, 5 which, in turn, contributes to further cardiovascular deconditioning 6 and increased risk of recurrent stroke or other vascular events.
Body-weight-supported treadmill training (BWSTT) permits safe walking practice in early stages of neurological recovery by mechanically offsetting a proportion of body mass. As a gait retraining modality, BWSTT is aligned with the principles of activity-dependent neural plasticity: task-specificity, 7 practice, 8 repetition, 9 and intensity. 10 Nevertheless, the relative effectiveness of BWSTT on ambulatory function in the subacute poststroke period remains equivocal, and recently BWSTT has been the subject of fairly harsh criticism. 11 Previous trials involving people early after stroke have reported greater gains in 6-Minute Walk Test (6MWT), gait speed, Berg Balance Scale (BBS), and motor recovery with BWSTT than with treadmill training without body-weight support 12 and greater attainment of independent ambulation following BWSTT than assisted overground walking. 13 Eich et al 14 noted more improvement in walking speed and distance with BWSTT than Bobath-oriented gait training. In contrast, lack of superiority of BWSTT for improving functional walking ability was reported in a trial where the comparison intervention was overground walking 15 and also in the recent, large-scale Locomotor Experience Applies Post-Stroke (LEAPS) trial, where the comparison conditions were delayed BWSTT and a home-based walking program. 16 A systematic review on BWSTT suggested that the divergent findings may be a result of variability in training intensities and comparison interventions. 17
Gait training consumes the majority of time spent in physiotherapy after stroke, 18 whereas aerobic fitness training has largely been overlooked.19,20 The fact that potentially modifiable cardiovascular limitations are not being addressed is of clinical concern. Even modest improvements in exercise capacity are associated with reduced cardiac complications in people with coronary artery disease 21 and increased survival in men with cardiac disease. 22 A recent study reported significant gains in VO2peak, 6MWT, and gait speed following 12 weeks of unsupported treadmill training of high-functioning chronic stroke survivors. 23 However, there have been few trials of cardiovascular fitness training early after stroke (ie, within the first 3 months)—the time when most physical rehabilitation takes place and the potential for functional recovery is greatest. 24 Duncan and colleagues 25 reported an improvement of 9% in VO2peak following a 12-week program of stationary cycling in 44 patients who were, on average, 76 days poststroke. Chang et al 26 found that 2 weeks of robot-assisted gait training elicited a 13% increase in VO2peak in 20 patients who began training a mean of 16 days poststroke. No studies have been published that have examined the application of BWSTT for aerobic training in the early poststroke period. Given the number of physical impairments requiring attention in the limited time available for stroke rehabilitation, an intervention that provides concurrent repetitive walking practice and cardiovascular conditioning would be time efficient and clinically appealing. Thus, we undertook this study to investigate the hypothesis that BWSTT is more effective than overground gait training (usual care, UC) in improving the cardiovascular fitness and functional walking ability (speed and endurance) of patients during stroke rehabilitation.
Methods
Participants
This single-site, randomized controlled trial with blinded outcome assessment investigated the effects of a 12-week program of BWSTT on the primary end points of cardiovascular fitness and ambulatory function at postprogram and follow-up at 6 and 12 months. We enrolled men and women who were older than 18 years, within 1 month of a first ischemic stroke confirmed by neuroimaging, inpatients in the stroke rehabilitation unit of the QEII Health Sciences Centre, and able to walk 5 m with or without use of ambulatory aids, ankle orthoses, or stand-by assistance. Potential participants were excluded if they had contraindications to maximal exercise stress testing, 27 musculoskeletal or cognitive limitations that could preclude participation in the program, or involvement in other pharmacological or physical intervention studies.
The sample size required was calculated using pooled estimates of within-group standard deviations of VO2peak data reported in previous studies.1,25,28,29 Power analyses indicated a minimum of 20 participants per group would provide an 80% (B = 0.20) chance of detecting a 20% (α = .05) difference between groups. The study was approved by Capital Health Research Ethics Board, and all participants provided written informed consent.
Randomization
Computer-generated, blocked randomization was used with stratification by ambulatory status: walking domain of the Functional Independence Measure of 3 to 5 (ambulatory dependent) and 6 to 7 (ambulatory independent). 30 Participants were randomly assigned to the intervention (BWSTT) or comparison (UC) groups using randomly permuted blocks of 4 and 6 participants. Participants assigned to either group were further randomly allocated to 1 of 2 trial physiotherapists to reduce bias resulting from differences in the therapists’ approaches to patient interaction and treatment delivery. 31 The randomization scheme ensured approximately equal numbers of ambulatory-dependent and -independent participants receiving treatment from either of the 2 physiotherapists. A person not involved in the study prepared and safeguarded individual, opaque sealed envelopes containing group and physiotherapist allocation, which were opened after completion of the baseline assessment.
Interventions
BWSTT and UC groups participated in interventions balanced in terms of exposure that consisted of 60-minute sessions, 5 d/wk for 6 weeks and then three 60-minute sessions per week for 6 weeks, for a total of 48 sessions. Substitute sessions for missed appointments were provided. For patients discharged to home during the 12-week period, all transportation costs to the trial site were reimbursed. Other components of stroke rehabilitation were not controlled. All sessions were led by 1 of 2 physiotherapists, who had more than 15 years of practice in stroke rehabilitation and were trained in the intervention protocols. Audits were conducted at 3-week intervals by a physiotherapist not directly involved in the study to assess compliance of the trial therapists with the trial protocols and provide feedback.
The protocols for the 1-hour UC and BWSTT sessions are outlined in the figure. Both groups received several routine interventions, based on findings from a previous study, 19 which included 5 to 10 minutes of active/passive stretching exercises, 10 to 15 minutes of upper-extremity training (active exercises and strengthening), and 10 to 15 minutes of lower-extremity training (active exercises and strengthening). Only the 25 to 30 minutes allocated for gait retraining differed in content between groups, with the UC group participating in 5 to 10 minutes of pregait activities in standing (ie, weight shifting and balance training) followed by 20 to 25 minutes of overground walking at comfortable, self-selected speeds. For the BWSTT group, gait retraining consisted of treadmill training initiated conservatively, in 5- to 10-minute bouts at the heart rate achieved at 40% to 50% of baseline VO2peak. The goal was to achieve target exercise duration (at least 20 minutes, exclusive of warm-up and cool-down) and intensity (heart rates corresponding to 60%-75% of baseline VO2peak 27 ) by the fourth or fifth week. Initially, ambulatory-independent participants walked at a treadmill speed of 80% to 90% of their self-paced overground speed with 20% to 30% of their body weight 32 supported via a Pneu-Weight unweighting system. Ambulatory-dependent participants walked at a treadmill speed of 70% to 80% of their overground speed with 40% body-weight support 32 and manual support to advance the hemiparetic lower extremity. Treadmill speed and grade were gradually increased and percentage of manual and body-weight support decreased, as tolerated. Heart rate was monitored continuously, and blood pressure and rating of perceived exertion on the 0 to 10 scale (RPE0-10) were recorded at regular intervals. Padded cycling shorts were worn to prevent skin irritation while in the harness, and care was taken to ensure adequate hydration. For safety, exercise was terminated, or intensity reduced, if the participant experienced chest discomfort, dizziness, or lightheadedness or the RPE0-10 exceeded 6 (“hard”). During BWSTT, the therapist emphasized trunk and limb alignment, loading of the stance limb, hip extension at terminal stance, and advancement of the swing limb. 12 Whenever possible, removal of ankle orthoses was encouraged, and use of handrail support was discouraged in order to stimulate balance responses and facilitate reciprocal arm swing.
After 12 weeks of training, all participants received a written maintenance program to be performed at home or in the community for 30 min/d, 3 d/wk. Participants in both groups were provided with a 10-minute individualized program of active upper- and lower-extremity exercises. In addition, the UC participants were prescribed 20 minutes of overground walking, and BWSTT participants were instructed to do 20 minutes of aerobic exercise (eg, brisk overground walking, stair climbing, stationary bike, and treadmill) at the target heart rate used in their last week of training. The research assistant phoned each participant once monthly to reinforce the importance of adhering to the prescribed maintenance program.
Blinding
During the consent process, participants were advised that they would be randomized to 1 of 2 intervention groups. To minimize exposure between groups, the BWSTT and UC programs were administered in different sections of the rehabilitation center. The 2 trial physiotherapists could not be blinded to intervention group, but all outcome assessments were conducted by a blinded assessor located off-site. Trial staff instructed participants to avoid mentioning anything about their intervention to the assessor. To ascertain the effectiveness of blinding, the assessor was asked at each assessment to indicate in writing their “guess” of the group assignment of each participant.
Measurement
Participant characteristics collected at baseline included age, sex, comorbidities, medications, and smoking history and date, type, and location of stroke. Primary and secondary outcome measures were assessed at baseline (0 months) and repeated by the same independent assessor after completion of training (3 months) and at 6- and 12-month follow-ups.
Primary Outcome Measures: Cardiovascular Fitness and Walking Ability
VO2peak was measured via open-circuit spirometry during a symptom-limited, maximal effort treadmill test with 15% body-weight support using a protocol, described in detail elsewhere, 33 that has been shown to be safe and reliable for patients poststroke. 34 Briefly, participants walked with harness support at a self-selected overground speed and 0% treadmill grade for the initial 2 minutes, followed by a 2.5% increase in grade every 2 minutes until an incline of 10% was reached and, thereafter, a 0.05 m/s increase in speed every 2 minutes until the test was terminated according to standard criteria. 27 Heart rate, respiratory exchange ratio, and RPE0-10 at peak exercise were used to compare maximal effort across tests.
Walking function was assessed by distance walked in 6 minutes (6MWT) 35 conducted over a continuous 100-m course. Walking speed was measured at a self-selected, comfortable pace over a 10-m path, using the average of 2 trials. Usual ambulatory devices, lower-extremity orthotics, and stand-by assistance were permitted.
Secondary Outcome Measures
Functional balance was assessed with the 14-item BBS, which is a reliable and valid measure in older adults. 36 Motor impairment of the paretic lower extremity was documented using the Chedoke-McMaster Stages of Recovery (CMSR) Leg and Foot, which are valid and reliable tools for use in the stroke population that range from 1 (no active movement) to 7 (normal complex movements). 37 After completion of the program, a field-tested survey was used to rate each participant’s level of satisfaction with their program, with the following question. “On a scale of 1 (very dissatisfied) to 5 (very satisfied), please rate the following components of the program: (1) quality of exercise sessions, (2) comfort during exercise sessions, (3) enjoyment of exercise sessions, (4) progress in walking ability, and (5) progress in fitness level.”
Statistical Analysis
Descriptive statistics were used to summarize participant characteristics on admission. Between-group baseline differences were assessed using independent t tests (continuous data), χ2 analysis (nominal data), and nonparametric methods (Kolmogorov-Smirnov test) when assumptions of normality were violated. ANOVA with repeated measures was used to model the treatment effects, with a between-subject factor at 2 levels (2 groups) and a within-subject factor at 4 levels (time: baseline, postprogram, 6-month follow-up, and 12-month follow-up). Interaction of group and time served to determine the efficacy of BWSTT on the outcome measures. In cases where Group × Time interactions were significant, within-group time point comparisons were performed using the Bonferroni correction to adjust for multiple comparisons. We planned to control for baseline differences between groups by using variables that were significantly different at baseline as covariates in the analyses. All analyses were conducted on an intention-to-treat basis, carrying the last observation forward for those lost to follow-up. The numbers of participants per group who exceeded clinically meaningful differences in the primary outcome measures at posttraining were compared using the χ2 test. The Mann-Whitney U test was used to analyze responses to the participant satisfaction survey. A 2-sample test for proportions was performed to determine whether the blinded assessor’s guesses of group assignment at posttesting and 6- and 12-month evaluations were better than chance. Statistical analyses were performed with SPSS Statistics 17.0.
Results
Participants
There were no significant differences in baseline characteristics between groups (Table 1). Of the 50 participants recruited, 45 (90%; 22 BWSTT and 23 UC) completed the 12-week exercise program (see Figure 1). The blinded assessor’s guesses of group assignment were no better than chance, with the correct guess made in 27 of 45 cases at the posttest (P = .46), 25 of 42 cases at the 6-month follow-up (P = .51), and 25 of 37 cases at the 12-month follow-up (P = .21).
Baseline Characteristics. a .
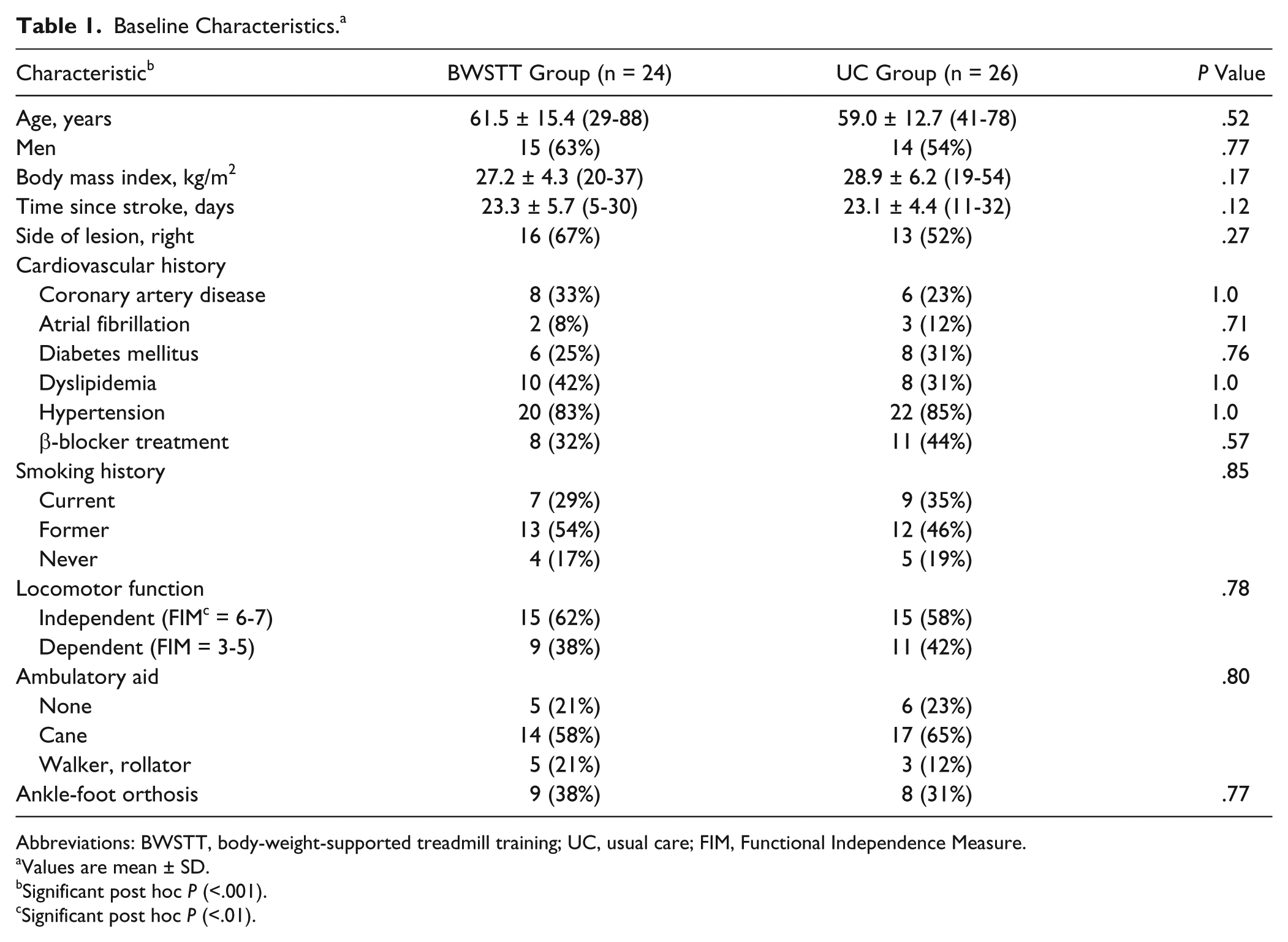
Abbreviations: BWSTT, body-weight-supported treadmill training; UC, usual care; FIM, Functional Independence Measure.
Values are mean ± SD.
Significant post hoc P (<.001).
Significant post hoc P (<.01).
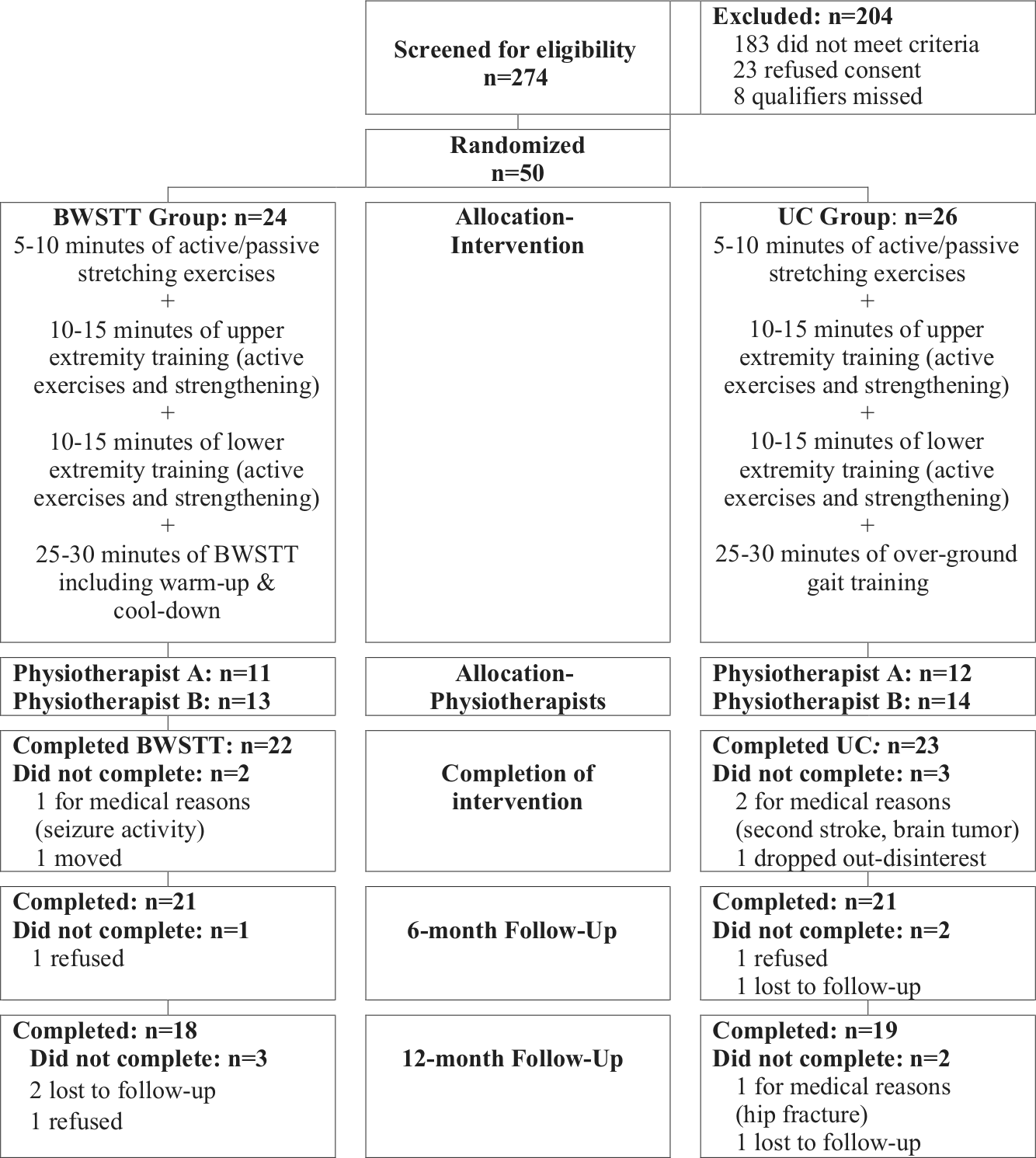
CONSORT flowchart with training protocols.
Training Protocols
The training protocols were well tolerated, and no adverse events occurred. Rates of participant adherence (sessions attended/sessions scheduled) were 90% for BWSTT and 86% for UC groups. Protocol audits revealed that the trial therapists were compliant with both BWSTT and UC protocols. Within the BWSTT group, the initial training speed was 0.49 ± 0.23 m/s for the ambulatory-independent subgroup (n = 15) and 0.26 ± 0.12 m/s for the ambulatory-dependent subgroup (n = 9). By the end of the 12-week intervention period training, training speed was 0.87 ± 0.29 m/s for the ambulatory-independent subgroup and 0.56 ± 0.19 m/s for the ambulatory-dependent subgroup, and a 10° incline was used by most participants in either subgroup. The percentage of BWS was gradually reduced for the ambulatory-independent subgroup from 22.5% ± 8.9% during the first week to 4.8% ± 5.8% during the last week, and for the ambulatory-dependent subgroup, from 36.3% ± 4.4% to 9.5% ± 3.8%. Duration of BWSTT (inclusive of warm-up and cool-down) increased over the course of training from 14.3 ± 4.5 to 24.4 ± 8.5 minutes for the ambulatory-independent subgroup and from 13.5 ± 7.5 to 26.1 ± 7.5 minutes for the dependent subgroup. For the first 2 to 3 weeks of BWSTT, 7 ambulatory-dependent participants required the assistance of 2 people (the trial physiotherapist and a physiotherapy assistant); thereafter, only 2 participants required 2-person assistance.
VO2peak Testing
No adverse events occurred during testing. No significant differences were found across tests at baseline and at 3, 6, and 12 months in heart rate at peak exercise (128.3 ± 15.4, 126.0 ± 16.2, 127.7 ± 12.3, and 129.4 ± 13.6, respectively; P = .31) and peak respiratory exchange ratio (1.01 ± 0.08, 1.00 ± 0.07, 1.02 ± 0.08, and 1.02 ± 0.06, respectively; P = .11), indicative of consistent physical effort exerted across tests, thus ensuring comparability of test results. 38 Although peak RPE0-10 values were also consistent across tests (5.1 ± 2.3, 5.2 ± 2.3, 5.0 ± 2.1, and 5.0 ± 1.8, respectively; P = .86), the values were lower and more variable than previously reported.26,39
Primary Outcomes
Repeated-measures ANOVA revealed significant Group × Time interactions for VO2peak (P = .004, Table 2). Within-group analyses showed no significant change in VO2peak over time in the UC group, whereas VO2peak of the BWSTT group improved significantly compared with baseline values at posttraining, 6-month follow-up, and 12-month follow-up (P < .001, Table 2). At posttesting, VO2peak values of 16 participants in the BWSTT group and 4 in the UC group exceeded the metabolic threshold of 17.5 mL/kg/min for moderately strenuous activities of daily living 40 (χ2 = 13.9, 1 degree of freedom, P < .001).
Primary Outcomes at Baseline, Posttraining, and 6- and 12-Month Follow-ups. a .
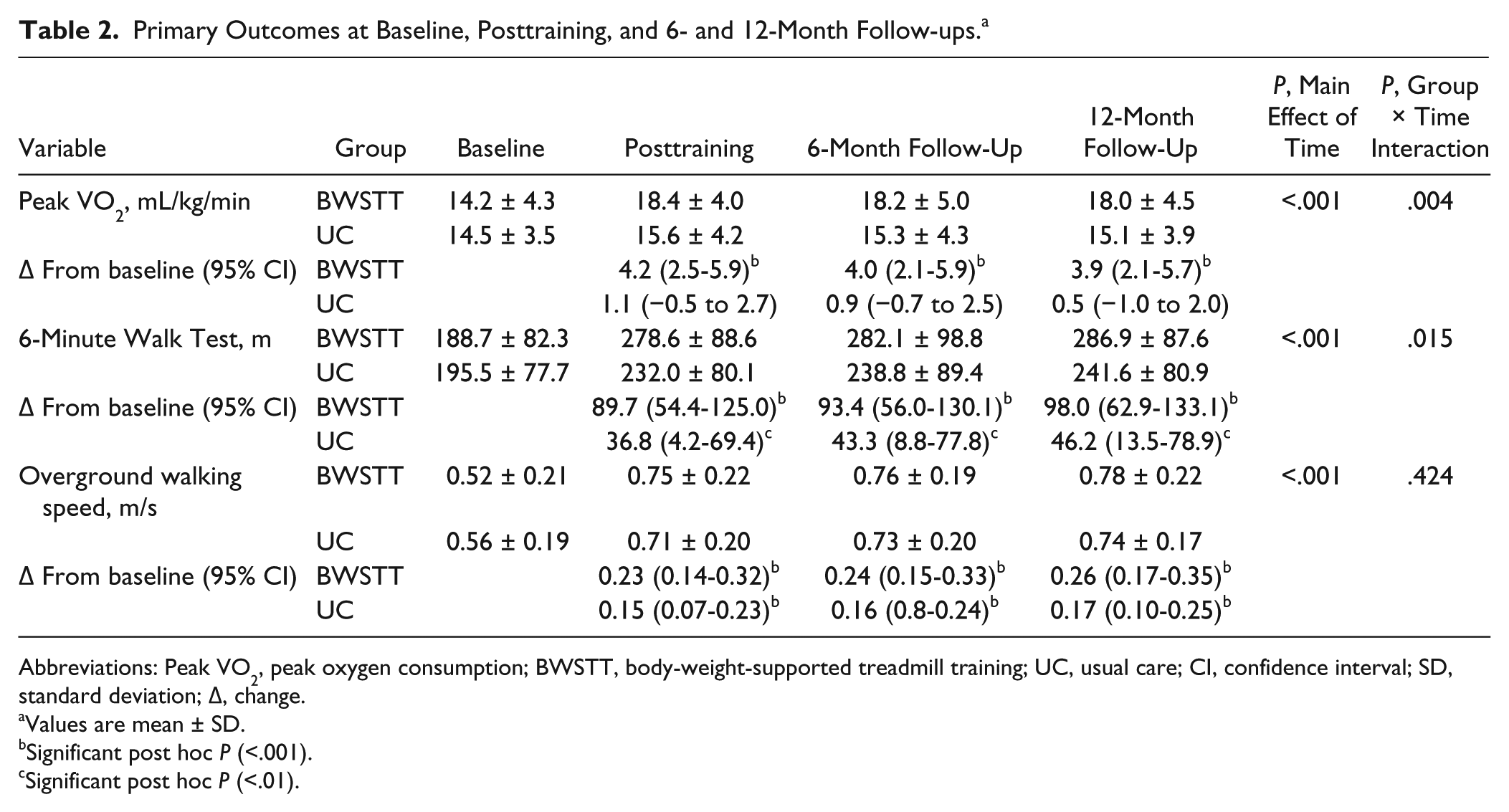
Abbreviations: Peak VO2, peak oxygen consumption; BWSTT, body-weight-supported treadmill training; UC, usual care; CI, confidence interval; SD, standard deviation; Δ, change.
Values are mean ± SD.
Significant post hoc P (<.001).
Significant post hoc P (<.01).
Significant Group × Time interactions were also found for the 6MWT (P = .015, see Table 2) at posttraining and follow-up, despite some overlap in the confidence intervals. Both BWSTT and UC groups showed significant improvements over baseline at posttraining (P < .001 and P < .01, respectively; see Table 2), with 15 participants in the BWSTT group and 6 in the UC group realizing a gain >49 m, the clinically meaningful change for the stroke population 41 (χ2 = 8.0, 1 degree of freedom, P = .005).
There was no significant Group × Time interaction for walking speed; however, within-group analyses revealed that both groups improved from baseline across tests (P < .001; see Table 2). At posttraining, increases in walking speed of the majority of participants (18 in the BWSTT group and 14 in the UC group) surpassed 0.14 m/s, the reported clinically meaningful change for people poststroke 41 (χ2 = 2.4, 1 degree of freedom, P = .12).
Secondary Outcomes
Group × Time interactions were not significant for BBS and CMSR Leg (Table 3). Within-group analyses showed that BBS and CMSR Leg in both groups exceeded baseline values at posttraining and at 6- and 12-month follow-up (see Table 3). A significant Group × Time interaction was found for CMSR Foot (P = .01; see Table 3). Within-group analyses showed that CMSR Foot exceeded baseline values in the BWSTT group at posttraining (P = .01), 6-month follow-up (P = .001), and 12-month follow-up (P = .001; Table 3).
Secondary Outcomes at Baseline, Posttraining, and 6- and 12-Month Follow-up. a .
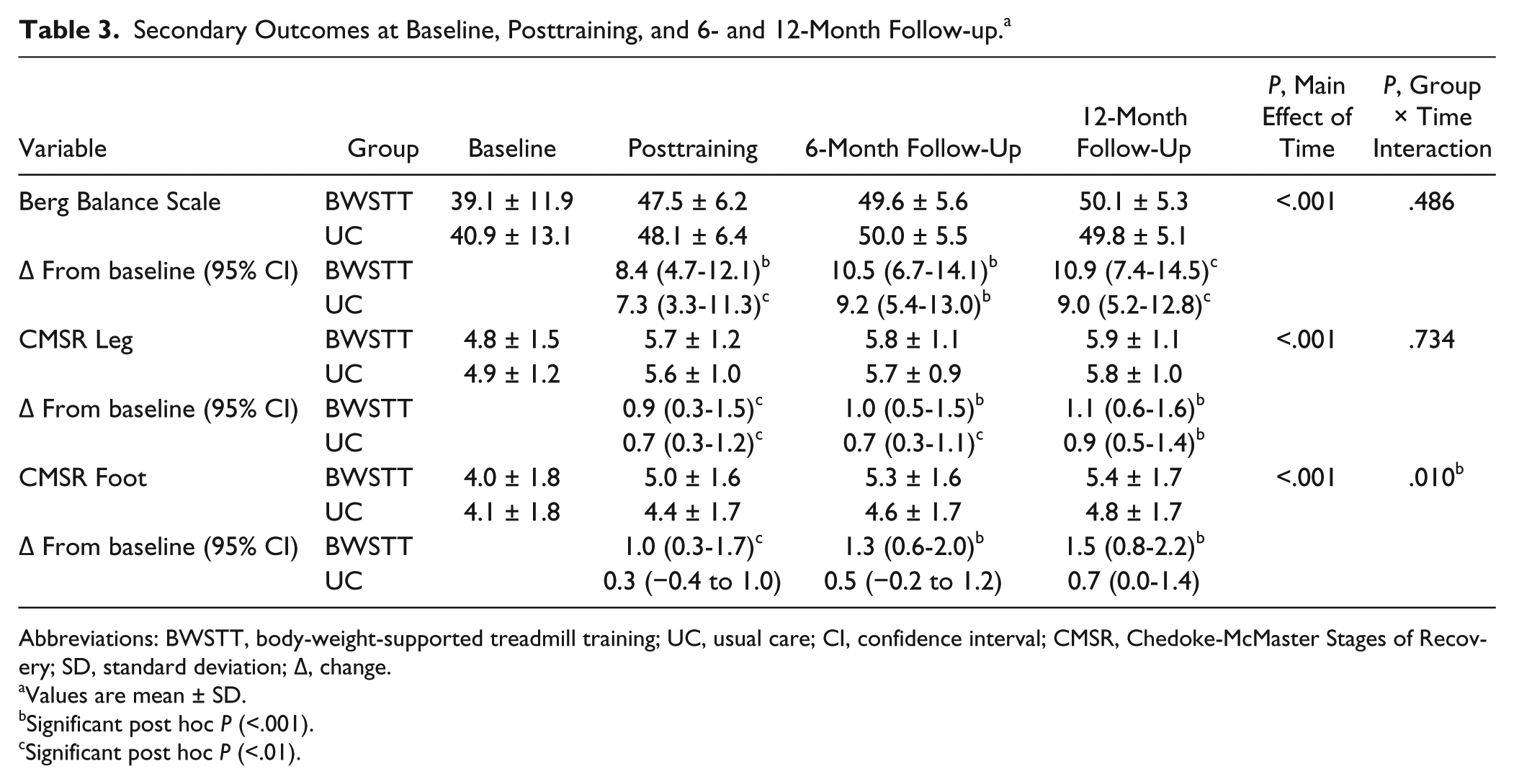
Abbreviations: BWSTT, body-weight-supported treadmill training; UC, usual care; CI, confidence interval; CMSR, Chedoke-McMaster Stages of Recovery; SD, standard deviation; Δ, change.
Values are mean ± SD.
Significant post hoc P (<.001).
Significant post hoc P (<.01).
Between-group differences were not found in the responses to the postprogram satisfaction survey, which was completed by 34 participants (76%; 16 BWSTT, 18 UC). BWSTT and UC participants rated the quality of exercise sessions 4.5 ± 1.0 out of 5 and 4.8 ± 0.3 out of 5 (P = .35); comfort during exercise, 4.3 ± 0.6 and 4.6 ± 0.5 (P = .52); enjoyment, 4.5 ± 0.5 and 4.6 ± 0.7 (P = .79); progress in walking, 4.3 ± 0.7 and 4.4 ± 0.8 (P = .84); and progress in fitness, 4.4 ± 0.6 and 4.3 ± 0.8 (P = .63), respectively.
Discussion
The study hypothesis that BWSTT early after stroke is more effective than conventional physiotherapy in improving cardiovascular fitness and functional ambulation was supported in part. At posttesting, the BWSTT group demonstrated greater improvements than the UC group in exercise capacity and walking endurance but not walking speed. The mean gain in VO2peak of BWSTT participants (4.2 mL/kg/min or 1.2 metabolic equivalents, METs) is clinically meaningful; a 1 MET (equal to 3.5 mL O2/kg/min) improvement has been associated with significantly fewer clinical events in people with coronary artery disease 21 and a 12% increase in survival of men with cardiac disease. 22 The higher posttraining capacity of the BWSTT group (5.2 ± 1.4 METs) compared with the UC group (4.4 ± 1.1 METs) implies greater ability to engage in daily physical activities at a lower percentage of their maximal capacity and, hence, lower physiological burden of performing activities of daily living. 40 Lack of significant change in VO2peak of the UC group is in keeping with previous findings. 39
The magnitude of improvement in VO2peak for the BWSTT group between pretraining and posttraining was almost 4 times greater than that reported in the only other randomized exercise trial that measured exercise capacity of people in the subacute period poststroke. 25 Variables that may account for the more robust response include earlier onset of intervention (mean of 24.5 vs 77.5 days poststroke), younger participants (mean of 60 vs 69 years), exercise setting (rehabilitation center vs home), training mode (BWSTT in the functional upright position vs stationary cycling), and intensity of training (progressing both speed and incline of treadmill vs using a fixed intensity). Previously, the time interval between stroke onset and therapy as well as exercise intensity were shown to be predictive of training-induced gains in cardiovascular fitness. 42
Both BWSTT and UC groups showed significant improvements in the 6MWT at posttesting (90 m, 48% change, vs 37 m, 19% change) but more participants in the BWSTT achieved a clinically meaningful change. These findings contrast with 2 other trials in which BWSTT was not found to be more effective than comparison therapies in improving 6MWT.15,16 Unlike either of these studies,15,16 exercise intensity in the present trial was individually prescribed, and heart rate was continuously monitored to ensure training within the aerobic zone. In addition, the larger dose of BWSTT in our study—a total of 20 hours versus 6.7 hours 15 and 15 hours 16 —may help explain this difference; the amount of physiotherapy poststroke 43 and the extent of repetitive task training of the lower extremities 44 are correlated with mobility outcomes. Also, the introduction of BWSTT earlier in stroke rehabilitation in our study when compared with the LEAPS trial 16 (mean of 24.5 vs 64.1 days poststroke, respectively) may have affected the extent of BWSTT-induced gains in walking endurance.
Lack of superiority of BWSTT over overground training in increasing gait speed is consistent with results of previous trials.15,16 Mean baseline speeds for BWSTT and UC groups were less than 0.6 m/s, which is predictive of poor health and function in nondisabled adults. 45 Thus, the finding that most participants in both groups attained speeds >0.7 m/s at posttraining, which were maintained at the 6- and 12-month follow-ups, is noteworthy. Although many participants in both groups surpassed the reported substantial meaningful change for the stroke population, few advanced from the category of limited community ambulation (0.4-0.8 m/s) to full community ambulation (>0.8 m/s). 46
Balance and motor control of the hemiparetic leg improved to a similar extent with BWSTT and UC, and the effects were sustained at follow-up. Mean changes in the BBS exceeded the minimal detectable change of 6 points 47 at posttraining, and absolute mean BBS scores surpassed the 49-point cutoff score used to distinguish between community-dwelling stroke survivors at low and high risk for falls. 48 Despite lack of specific balance training in the BWSTT protocol, discouraging handrail support and progressively increasing the extent of weight bearing through the lower extremities may have increased the postural training demand. Improved control of ankle movement was evident in the BWSTT group alone, an effect that may be attributable to previously reported increases in ankle plantarflexion angle and power generation in the preswing phase of hemiparetic gait following BWSTT. 49 The greater impact of BWSTT versus UC on VO2peak and 6MWT distance but not on short-distance walking speed, BBS, and lower-extremity motor control suggests that the main differential effect of BWSTT was on cardiovascular endurance.
Ease of accessibility to intervention sessions may have contributed to the high adherence of both BWSTT and UC participants over the 12-week program. “Makeup” sessions were provided for missed appointments. Also, during the first half of the program, all participants were inpatients, and during the second half, all travel costs incurred were reimbursed. Rimmer and colleagues 50 reported that lack of transportation was one of the main barriers to participation in physical activity among community-based stroke survivors.
Sustainability of the substantial cardiovascular adaptations made by the BWSTT group long after cessation of formal training is extremely encouraging. In a trial of treadmill training involving chronic stroke survivors Globas and colleagues 23 reported maintenance of gains in VO2peak and 10-m walk but not 6MWT at the 1-year follow-up. It is possible that by intervening early after stroke, the participants in our study were better prepared to make the behavioral changes necessary for long-term engagement in physical activities. Also, provision of outpatient rehabilitation after hospital discharge, 51 together with individually tailored maintenance exercise programs and monthly telephone contact, may have contributed to sustained improvements at both 6-month and 1-year follow-ups. In 2 previous trials of patients in the subacute phase of stroke, improvements in walking speed and BBS continued in the period between posttesting and follow-up at either 3 months 12 or 6 months. 52 Similarly, in the LEAPS trial, 16 gains in 6MWT and walking speed in all 3 active treatment groups were largely preserved or enhanced 12 months after the intervention phase.
The fact that only the UC group practiced overground walking throughout the study may have biased assessment of walking speed and 6MWT in favor of UC participants. Similarly, because the BWSTT group received treadmill training throughout the study, the symptom-limited exercise test findings may have been biased in the direction of BWSTT participants. However, the level of effort exerted by either group (as reflected by heart rate and respiratory exchange ratio) was consistent across tests. Despite equal exposure of the 2 groups to therapy, delivery of the BWSTT intervention required an average of 8 person-hours more than the UC treatment because of the need for additional assistance for the more disabled participants in the first few weeks of therapy. Outcomes of interest beyond exercise capacity and functional walking ability, such as vascular risk factors, gait pattern, and emotional well-being, were not addressed, and participation in physical activities between completion of formal training and follow-up was not monitored.
Conclusions
Clinically meaningful improvements in exercise capacity and walking endurance were observed with this repetitive, task-oriented training strategy that were sustained at the 6- and 12-month follow-ups and exceeded gains achieved with standard care. Support for BWSTT as an intervention with demonstrated efficacy in addressing concurrently 2 major physical impairments after stroke has substantial clinical implications, given current concerns about enhancing the efficiency of stroke rehabilitation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Heart and Stroke Foundation of Canada.