
Abstract
Background. Predicting walking outcomes poststroke is a challenge for clinicians. Objective. To identify the extent to which exercise dose (repetitions of leg movements) in the first week of a comprehensive stroke unit stay predicts discharge mobility. Methods. A cohort study was conducted on 200 consecutive people admitted to a comprehensive stroke unit who required physical therapy. Results. Discharge and predictor data were available for 191 survivors (99%). On admission, 86 participants were able to walk, and the average walking velocity was 0.42 m/s. On discharge, the average walking velocity was 0.77 m/s, and 152 participants were able to walk. A discharge walking velocity of greater than 0.8 m/s was predicted by the exercise dose achieved in the first week after admission. Adding other predictors did not significantly increase the predictive ability of the model. Completion of more than the median number of exercise repetitions (703) in the first week of admission was associated with a quicker recovery of unassisted walking. This effect persisted after adjustment for walking velocity on admission, cognition, and comorbidity. Conclusion. Exercise dose in the first week after admission for stroke is an important indicator of walking speed at discharge and the time to achieve unassisted walking.
Few prospective studies of persons with stroke have investigated predictors of mobility or physical functioning.1-5 Older age, greater upper-limb hemiparesis, and higher level of disability on admission are among the predictors. A recent systematic review investigated predictors of mobility status 30 days after stroke. 6 These predictors included age, severity of paresis, size of lesion, presence of hemianopia, and type of stroke. The authors concluded that limited factors have been investigated to date. Therefore, there is a need to consider other factors that may affect mobility outcomes. Recent studies found that within 72 hours after stroke, the ability to sit and the strength of the hemiplegic leg could predict walking ability at 6 months 7 and that walking speed and the Motor Assessment Scale (MAS) item 2 (supine to sitting) on admission to rehabilitation predicted discharge walking speed. 8
Repetitive task training can enhance motor skill performance.9-12 It is possible that the ability to participate in repetitive exercise may predict functional outcomes, but this has not been investigated. In this study, we sought to establish whether exercise dose achieved in the early rehabilitation period would be a predictor of mobility outcomes after stroke. We defined exercise dose as the total number of lower-limb-related exercise repetitions stroke survivors were able to achieve during their first week on the stroke unit. In addition, we compared the predictive ability of exercise dose with previously identified or likely predictor variables (age, cognition, level of disability, and walking speed on admission).
We followed the recommendations for prognostic research13,14 by using a prospective cohort study to develop a simple model 13 that could easily be used in clinical practice once validated in another sample.14,15
The research questions were as follows:
To what extent does exercise dose achieved in the first week in a stroke unit predict mobility outcome on discharge from inpatient care after stroke? Does the inclusion of other known/likely predictors of mobility after stroke improve the predictive ability of the model?
Is achieving a larger exercise dose in the first week in a stroke unit associated with a faster recovery of the ability to walk independently? Does this relationship persist after adjustment for other known/likely predictors of mobility after stroke?
Method
Design
A prospective, inception cohort study was conducted at Bankstown-Lidcombe Hospital (BLH) Stroke Unit in Sydney, Australia. This is a 20-bed comprehensive stroke unit in which acute and rehabilitation beds are co-located. All stroke survivors at BLH are admitted to the stroke unit. Consequently, we were able to observe 200 stroke survivors throughout the acute and rehabilitation phases of their hospital stay.
All measurements and data collection were performed by the treating physical therapist. Clinical measures of performance were collected within 48 hours of admission to the unit. Data on most predictors were collected in the first 48 hours after admission, except exercise dose, which was totaled over the first week of admission. The clinical measures were repeated within the 48 hours prior to discharge from the unit. Procedures were outlined in a manual given to all staff. Therapy staff then practiced the assessment procedure and were given feedback from the first author. They had access to standard equipment and ongoing support and feedback.
Participants
A total of 200 people admitted to the stroke unit with a diagnosis of stroke were included in this study. Stroke was diagnosed by clinical presentation and/or CT/MRI scan results. People with both ischemic and hemorrhagic stroke were included. To be included in the study, participants needed to require ongoing physical therapy intervention after their initial assessment. This was to ensure that we captured data from participants who were moderately disabled but excluded those with transient ischemic attacks or very mild strokes that did not require inpatient physical therapy and who were quickly discharged from the unit. Small proportions of people are admitted to the stroke unit for palliation after stroke and were excluded from the study. However those participants who were included in the study, offered rehabilitation, and later deemed to require palliation were included.
Measures
Descriptive data were collected on admission for each participant. This included recording their gender and the side and type of stroke based on information in each participant’s medical record. To provide more information regarding initial walking ability, the MAS item 5 (Walking) was completed per the standard assessment at the study site.16,17
The predictor variables investigated included age, comorbidity, disability level on admission, and cognition. Age was recorded from each participant’s medical record. The Charlson Comorbidity index quantified the extent of each participant’s comorbidity. The version modified for use in ischemic stroke was used.18,19 The participant’s disability level on admission was rated using the modified Rankin Scale (mRS). This 7-point scale reflecting level of disability has been commonly used in the stroke population. 20 The treating physical therapist rated the participant’s cognition. If the therapist perceived that the participant’s cognitive impairment had a negative impact on the assessment or the first therapy session, he or she recorded a cognitive deficit to be present.
Admission walking velocity was measured by the 10-m walk test. The test was measured on a 14-m track with the middle 10 m timed. If the participant required physical assistance, this was specified. If the participant was unable to walk for 10 m, then the velocity was recorded based on the maximal distance he or she was able to walk. If the participant was unable to walk, then the velocity was recorded as zero.
All participants were seen by a physical therapist and prescribed a task-related motor training/exercise program. This study occurred on a comprehensive stroke unit, which provides intense therapy as early as possible after stroke. Most stroke survivors are seen on the day they are admitted to the unit and mobilized as soon as they are medically stable within the first week after their stroke. Their exercise program may include one-on-one training with the physical therapist; exercise supervised by therapists, therapy assistants, and/or family members; and unsupervised exercise in the therapy gymnasium. Stroke survivors able to safely exercise unsupervised were also asked to exercise in their rooms. To ensure that more disabled stroke survivors were also given opportunities to exercise, strategies such as a sliding tilt-table and treadmill with body weight support were used.
The total number of exercise repetitions (excluding upper-limb exercise) quantified the exercise dose in the first week on the stroke unit. Repetitions of each active exercise were counted and documented. In one-to-one sessions, the therapist counted the exercise repetitions. In supervised sessions, the repetitions were counted either by the participant if able or with the assistance of relatives and/or therapy staff. We have previously shown that therapists can identify rehabilitation participants who can accurately quantify exercise repetitions. 21 Exercises completed included training of sitting, sit-to-stand, standing, walking, and strength training in weight-bearing and non-weight-bearing positions. We defined repetitions for each exercise: for example, a sit-to-stand or a single-hip abduction in side lying were counted as 1 repetition each. For ease of data synthesis, each meter of walking (either overground or on a treadmill) was counted as a repetition. Overground distances were calculated by asking the participant to complete laps of a track of known distance and recording the number of laps completed. When not completing the known track—for example, when walking outdoors—a trundle measurement wheel was used by the therapist to accurately record meters walked. All exercises were documented daily on a recording sheet. This sheet listed each exercise, and the therapy staff recorded the number of repetitions immediately after completion.
We defined the first week of admission to be the first 5 days where exercise was possible—for example, weekdays on which the participant was medically stable. A day was counted if therapy was attempted regardless of the amount that occurred. For example, some participants may have attempted active practice in the gym environment but been too drowsy or unable to understand, and little to no exercise repetitions were be performed. Others would be able to complete significant amounts of repetitious practice of exercises supervised or with assistance. This study observed usual practice in this stroke unit; consequently, factors such as medical tests, therapist workload, and sessions with other health professionals did impinge on the time available and dose of exercise that was possible in the first week.
The outcome variables investigated were the participant’s walking velocity on discharge, measured as on admission, and the number of exercise days to achieve the milestone of walking 10 m without hands-on assistance (a walking aid or therapist standing beside the participant was accepted). We dichotomized the outcome of walking speed at 0.8 m/s and predicted either a faster walking velocity of ≥0.8 m/s or a slower walking velocity of <0.8 m/s on discharge from the unit. Previous research has found the average walking speed after stroke rehabilitation to be 0.3 to 0.8 m/s. 22 The value of 0.8 m/s was chosen as the point at which to dichotomize the data because this speed is suggested to be indicative of full community ambulation in the classification system developed by Perry et al. 23 It has been shown that people who can walk at faster speeds (>0.8 m/s) have improved functional ability and quality of life. 24
Discharge from the stroke unit occurs primarily on goal achievement. When the stroke survivor has achieved his or her goals and is no longer making significant improvement, discharge is considered. Discharge goal setting will consider the person’s premorbid level of function, social situation, and support at home. The stroke unit is in a public hospital, and as such, insurance funding did not affect discharge time frames.
Data Analysis
Statistical analysis was completed using PASW (formerly SPSS) V18 and Stata V11 statistical software. Univariable and multivariable logistic regression models were used to investigate predictors of whether participants would achieve a walking speed >0.8 m/s on discharge. We considered achieving an area under the receiver operating characteristic curve (AUC) of 0.80 or higher to indicate a powerful prediction model. 25 AUCs of different models were compared using the “roccomp” command in Stata V11. Survival analysis was used to investigate the predictors of time to achieve walking without assistance during the inpatient stay. We dichotomized exercise dose into high and low for the survival analysis by dividing the sample at the median dose of 703 exercise repetitions. The exercise dose was considered high for those participants completing more than the median 703 repetitions and low for those completing fewer.
Results
Flow of Participants Through the Study
Of the 1013 people admitted to the stroke unit between February 2008 and June 2010, 200 were included in the study (Figure 1). The most common reason for exclusion from the study was diagnosis other than stroke. All predictor data were collected for 199 participants; 7 participants died during their stay on the stroke unit. Discharge data were available for all except 1 (99%) of the survivors—this person was discharged unexpectedly and measurement did not occur.
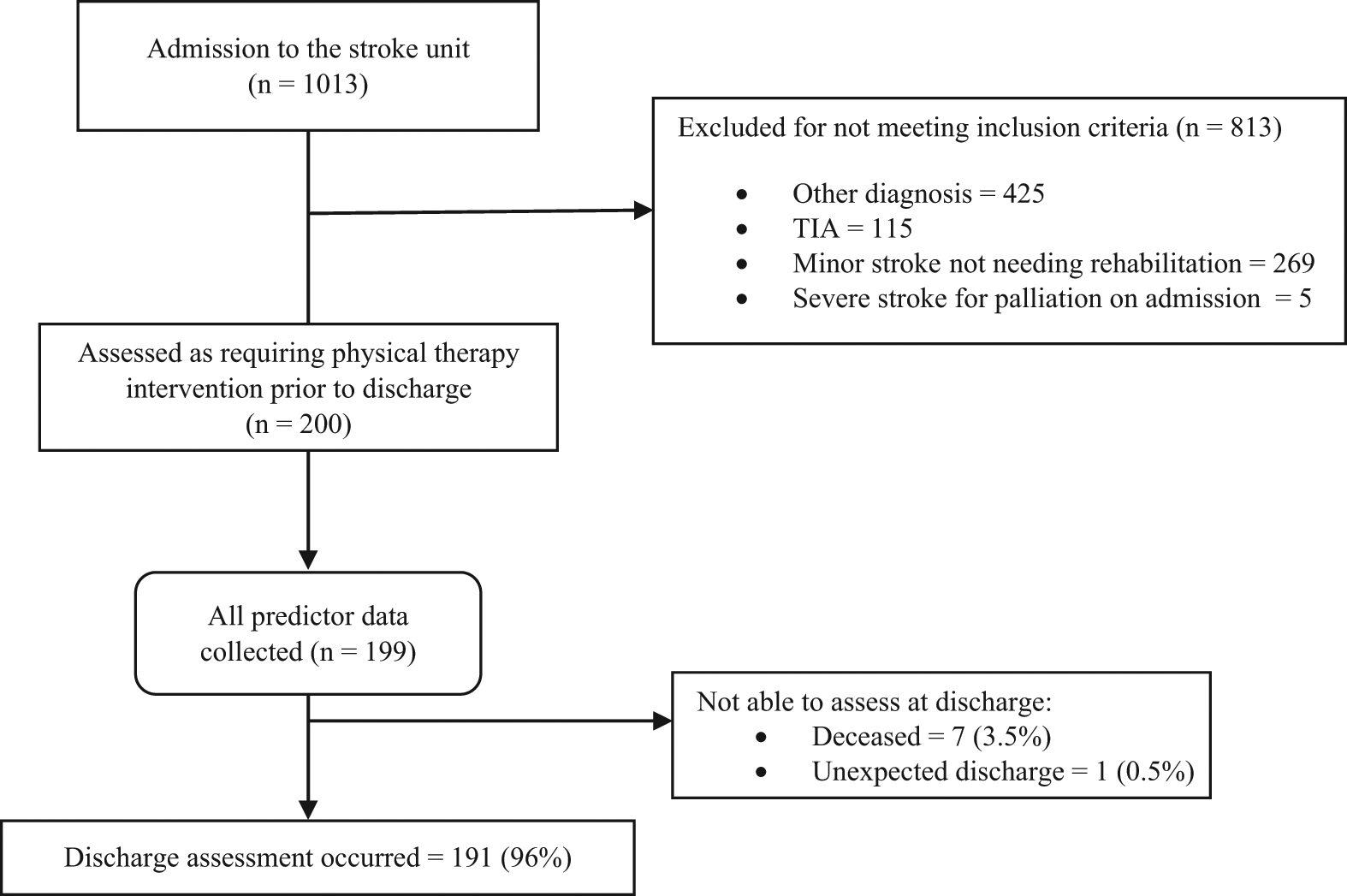
Flow of participants through the study
Characteristics of Participants
The characteristics of the 200 participants are detailed in Table 1. The average age of participants was 76 years (standard deviation [SD] = 12.5; range 19-99). There were 80 participants who had left-sided ischemic strokes and 80 who had right-sided strokes. Also, 2 participants had bilateral strokes. There were 23 participants with hemorrhagic strokes and 15 participants with cerebellar or brainstem strokes. Most participants were significantly disabled on admission. The average mRS score was 4.2 (SD = 0.8). A score of 4 on the mRS indicates the need for assistance to transfer or walk and help with all daily activities. In all, 40% of participants scored 5 for the mRS, meaning that they were bed bound and needed full nursing care. Approximately half of the participants were identified as having cognitive impairments that affected their therapy sessions. During the first week of admission, the number of exercise repetitions achieved ranged from 0 to 5522, and the median number of repetitions was 703.
Demographics of the 200 Study Participants on Admission
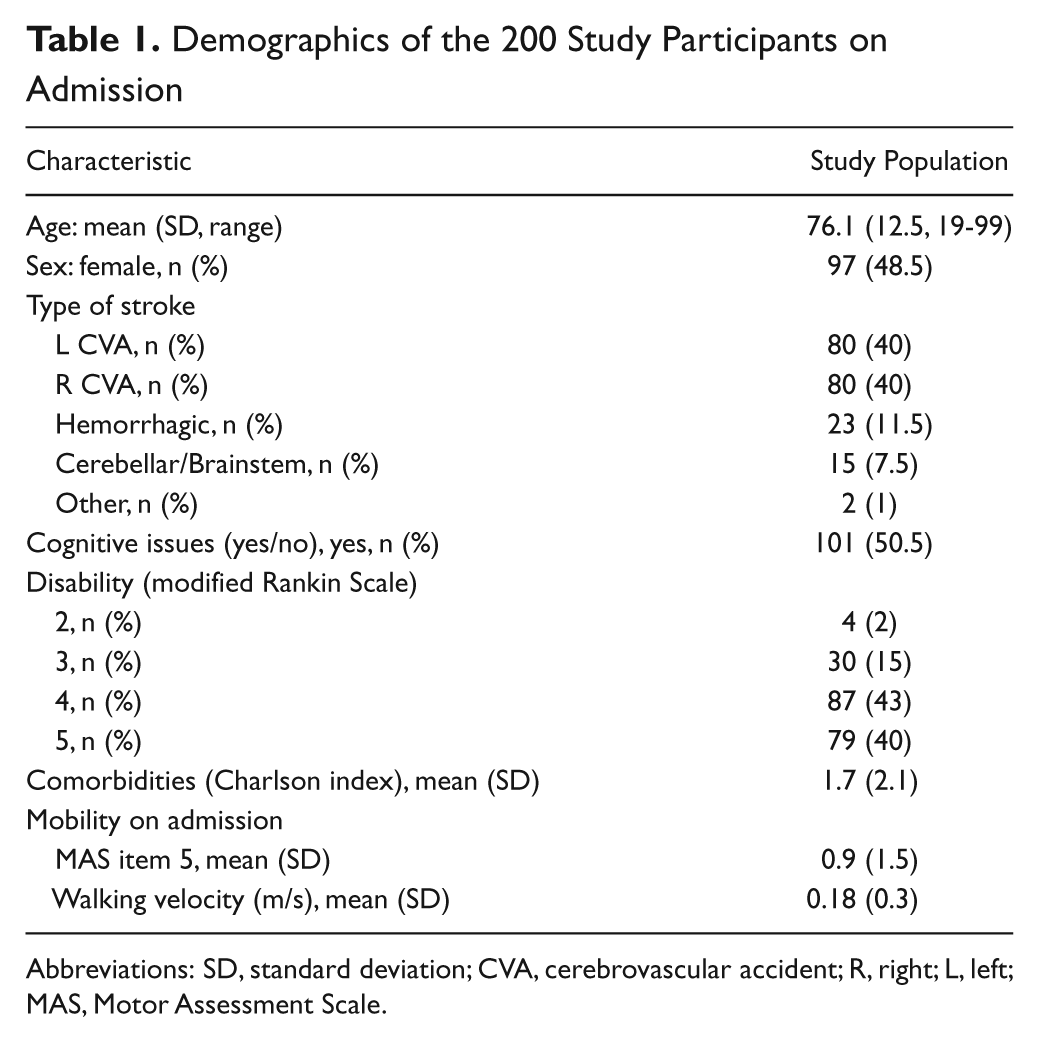
Abbreviations: SD, standard deviation; CVA, cerebrovascular accident; R, right; L, left; MAS, Motor Assessment Scale.
On admission to the stroke unit, 86 stroke survivors were able to walk with or without physical assistance. The average walking velocity for all participants was 0.18 m/s (SD = 0.30; 0 m/s used for participants who were unable to walk). The walking velocity for the ambulatory participants was 0.42 m/s (SD = 0.32).
Seven participants died during their admission. On discharge, 152 survivors were able to walk. The average walking velocity for all survivors was 0.61 m/s (SD = 0.53). The average walking velocity for the ambulatory survivors was 0.77 m/s (SD = 0.39). Of the ambulatory stroke survivors, 94 (62%) could walk independently, 43 (28%) required supervision, and the remaining 15 (10%) needed physical assistance. The treating therapist initiated the use of a walking aid for 20% of the ambulatory stroke survivors; 10% continued to use their prestroke walking aid. The remaining 70% of ambulatory survivors walked unaided.
For 5 survivors, walking velocity actually decreased during the stroke unit stay (range of decrease = 0.08-0.56 m/s). Of these people, 3 had further strokes or an extension of the stroke for which they were admitted. It was noted that the other 2 participants often refused to attend therapy sessions. Data from these participants were included in the analysis.
The number of working days (weekdays) during participants’ stroke unit admissions ranged from 10 to 81 days. The average duration of exercise was 22.2 (SD = 13.1) weekdays or approximately 4 weeks.
Prediction of Discharge Walking Speed
A total of 74 (39%) participants were able to walk at 0.8 m/s or faster on discharge. In univariable analyses, exercise dose was the strongest predictor of having a fast walking velocity (≥0.8 m/s) on discharge from hospital; AUC = 0.82 (95% confidence interval [CI] = 0.75-0.87). This AUC was significantly better than the AUCs for each of the other univariable predictive models (Table 2).
Prediction of Walking Velocity on Discharge Greater Than 0.8 m/s: Comparison Between Exercise Dose and Other Single Predictors
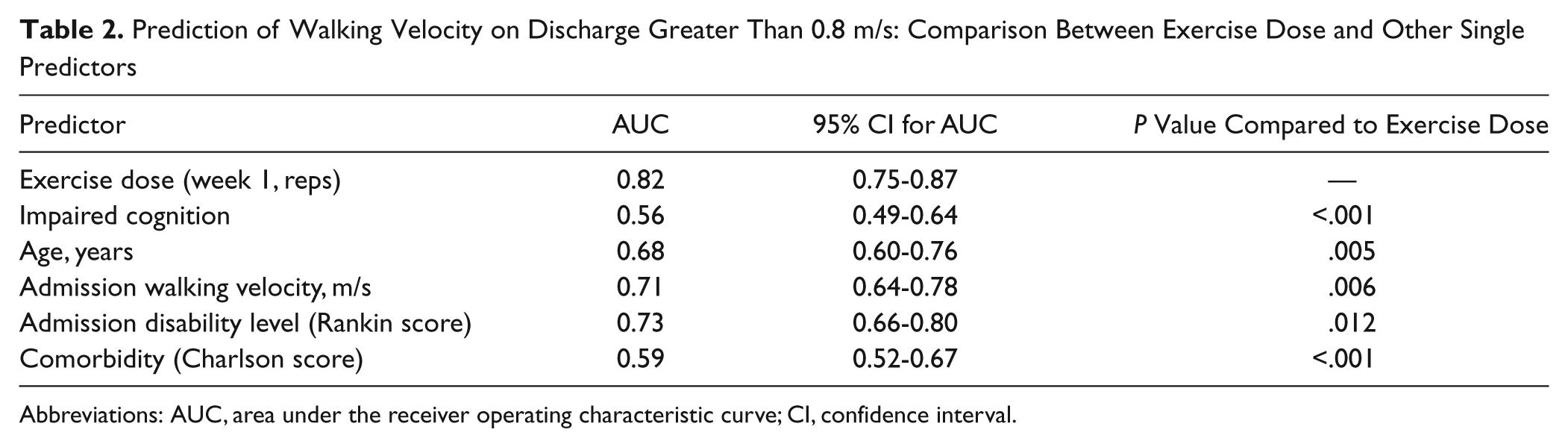
Abbreviations: AUC, area under the receiver operating characteristic curve; CI, confidence interval.
Inclusion of age, level of disability, comorbidities, cognition, and admission walking velocity (in addition to exercise dose) in multivariable analysis increased the model’s predictive ability (AUC = 0.85, 95% CI = 0.80-0.90). However, this increase was relatively small and not statistically significant (P = .12). Within the multivariable model, the variables that made a significant individual contribution to the model were admission walking velocity (continuous variable, odds ratio [OR] = 11.6; 95% CI = 2.0-68.2; P = .007), age (continuous variable, OR = 0.96; 95% CI = 0.93-0.99; P = .005), and exercise dose (continuous variable, OR = 1.0007; 95% CI = 1.0002-1.0010; P = .006). There was no significant difference in the predictive ability of a model that included exercise alone and a model including the 3 variables that made a significant contribution to the multivariable model (admission walking velocity, age, and exercise dose: AUC = 0.84; 96% CI = 0.78-0.89; P = .31).
Time to Achieve Unassisted Walking
On admission, 29 people were able to walk 10 m without physical assistance. During the admission, a further 108 people became able to walk 10 m without physical assistance. Completion of more than the median number of exercise repetitions (703) in the first week of admission was associated with a quicker recovery of unassisted walking (hazard ratio [HR] = 4.1; 95% CI = 2.7-6.1; P < .001). This effect persisted after adjustment for walking velocity on admission, cognition, and comorbidity (HR = 3.5; 95% CI = 2.3-5.4; P < .001). Those who completed 703 or more exercise repetitions in the first week of admission achieved unassisted walking after a median of 9 days of therapy (95% CI = 6-12). Those who completed fewer than 703 exercise repetitions in the first week of admission achieved unassisted walking after a median of 30 days of therapy (95% CI = 23-53; see Figure 2).
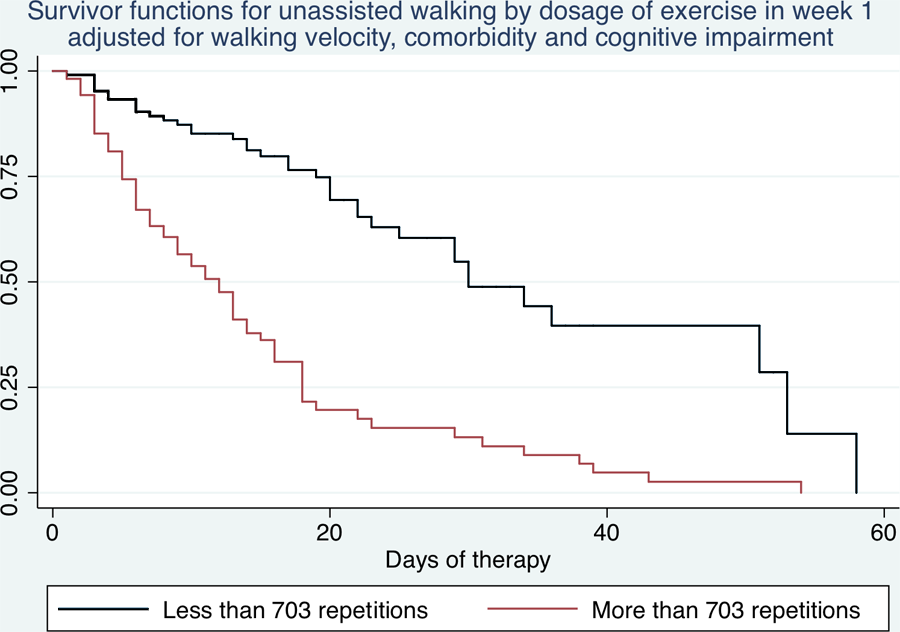
Survival curves showing the proportion of participants who became able to walk 10 m unassisted: separate survival curves are shown for participants completing more or less than the median exercise dose (703 repetitions). Both curves are adjusted for other predictors (walking velocity, comorbidity, and cognitive impairment on admission).
Discussion
This study found that lower-limb exercise dose in the first week on a stroke unit was a strong predictor of walking velocity after stroke rehabilitation. A higher dose of lower-limb exercise repetitions in the first week predicted a faster walking velocity, >0.8 m/s (AUC = 0.82; 95% CI = 0.76-0.87). The inclusion of other known/likely predictors of mobility (age, level of disability, comorbidities, cognition, and admission walking velocity) in a multivariable model did not significantly improve the model’s prediction of walking velocity (AUC = 0.85; 95% CI = 0.80-0.90, P for difference between 2 models = .12). This suggests that the exercise dose is an efficient single predictor of walking velocity after stroke.
This study also found that the completion of more exercise repetitions in the first week of admission was associated with a quicker recovery of unassisted walking (HR = 4.1; 95% CI = 2.7-6.1; P < .001) and that this effect persisted after adjustment for walking velocity on admission, cognition, and comorbidity (HR = 3.5; 95% CI = 2.3-5.4; P < .001).
The exercise dose achieved in the first week of admission will be strongly influenced by the stroke survivor’s ability to participate in repetitive training. Many factors may influence their ability to participate, such as alertness, fatigue, mood, and family support. Future research is required to establish predictors of a stroke survivor’s ability to participate in physical therapy. This study found that regardless of which factors contribute to participation in therapy, the ability to complete repetitions of exercise is a strong predictor of walking velocity and time to unassisted walking after stroke. The lower-limb exercise dose completed in the first week was relevant to daily clinical practice on a stroke unit because we observed usual care and did not adjust for tests and other interruptions to possible therapy time. This indicates that the findings are transferable to clinical practice on acute stroke units.
The strength of this study was the monitoring of 200 stroke survivors throughout their hospital stay, including the acute and rehabilitation phases. There was a minimal loss to follow-up with discharge data available for 99% of surviving participants. The results of this study can only be generalized to stroke patients requiring inpatient stroke unit care and physical therapy intervention. Future studies may investigate predictors of walking outcomes in all people admitted to stroke units or in all stroke survivors.
A limitation of this study was the clinician-rated measure of cognition. This measure was chosen for pragmatic reasons because a simple and efficient measure was needed that could be used by physical therapists. At the time of the study, no routine cognition rating scales were being implemented by any profession on the unit. We believe that the subjective rating used in this study gave an indication of those people who have significant cognitive deficits; however, it probably does not capture those participants with subtle cognitive issues. Another potential limitation is how to define the type and quantity of exercises performed outside of the therapy area. In this study we relied on participants’ report of the amount and type of leg exercises performed. New sensors may be able to more accurately and easily describe repetitions of exercise when a therapist is not present.26,27
Conclusion
The ability to complete more exercise repetitions early after stroke was a useful predictor of walking speed and the number of days of therapy taken to achieve unassisted walking in this sample. After validation in another sample, this simple measure has the potential to assist clinicians to determine likely walking outcomes for individual stroke survivors. This information may be useful to communicate with the stroke survivors, their families, and the stroke unit team to try to increase daily exercise as well as to begin to suggest a prognosis.
Footnotes
Acknowledgements
Dharani Khandasamy and Angela Vratsistas assisted with data collation and entry. The physical therapy staff and students on the stroke unit assisted with data collection.
Authors’ Note
Ethics approval: The Human Research Ethics Committee (Western Zone) of the Sydney South West Area Health Service approved this study on August 13, 2008; Project Number QA2008/049.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an infrastructure grant (number 07-08/007) from the Ingham Health Research Institute. A/Prof Sherrington receives salary funding from the Australian National Health and Medical Research Council.