
Abstract
Background. Bell’s palsy (BP) is the most frequent form of peripheral palsy of the facial nerve. Prognosis for recovery is good for most patients; in the remaining cases, different grades of residual impairment persist. Physical therapy, in association with drug administration, aims to improve outcomes. Objective. To assess the efficacy of early physical therapy in association with standard drug administration versus pharmacological therapy only, in terms of time to maximum gains and grade of recovery of function, and to examine who will most benefit from rehabilitation. Methods. From June 2008 to May 2010, 232 individuals were evaluated. The 87 patients meeting the eligibility criteria were randomly assigned to the experimental group (prednisone and valacyclovir plus physical therapy, n = 39) or the control group (pharmacological therapy, n = 48) within 10 days of onset. Intention-to-treat analyses were done. Results. The physical therapy had a significant effect on grade (P = .038) and time (P = .044) to recovery only in patients presenting with severe facial palsy (House-Brackmann [HB] grade V/VI). No significant differences were found between the study and control groups for outcome of synkinesis. Conclusion. Physical therapy appears to be effective only in the more severe BP (baseline HB grade V/VI), whereas less severe BP (baseline HB grade IV) results in complete spontaneous recovery, regardless of physical therapy.
Keywords
Introduction
Bell’s palsy (BP) is the most frequent form of peripheral palsy of the facial nerve and represents about 50% to 60% of all etiologies, with a diversely reported annual incidence of between 8 and 52.8 new cases per 100 000 individuals.1-7 From 69% to 85% have a complete spontaneous recovery, whereas partial motor recovery, synkinesis, hemifacial spasm, contractures, salivation, and lacrimation alterations may persist in remaining cases.5,8,9 These residual symptoms have a significant impact on the quality of life because they cause esthetic (asymmetry of the face at rest, during movements, speech, and alterations in smiling) and functional problems (difficulty in eating, drinking, and speech).
The sequelae may trigger severe psychological problems10-13 because facial harmony and symmetry influence the person’s own mental picture of themselves and how others perceive them 14 and are determinant factors of facial attractiveness, markers of good health, and a vehicle of expression of feelings.15,16 In an attempt to prevent or reduce these residual deficits, continuous efforts have been made to identify the most effective therapeutic approaches, including medications, 17 physical therapy, 18 or a combination of both.19-21
The main problem concerning the efficacy of medications such as steroids is the uncertain etiology of BP and the timing of intervention. Pharmacological treatment starts when the patient is assessed the first time: the time lapse between paresis/paralysis and treatment may vary considerably. Although therapy appears to reduce edema and secondary inflammation damage, it does not influence the amount of damage already present when the patient presents for medical attention and starts steroid intake. At present, efficacy has been shown for the use of corticosteroids alone, 17 with a better outcome if administered within 48 hours of onset of palsy. 22
Physical therapy has been initially experimented with in an attempt to avoid, or at least minimize, the sequelae associated with drug administration. The first attempts were made using electrostimulation, thermal methods, massage, and gross-motor facial exercises, with and without biofeedback. Over the past few years, methods have changed in favor of tailored and patient-centered approaches, based on exercises more suitable for the particular physiology and function of facial muscles and the management of psychological distress.
Efficacy of physical therapy, as the only alternative to no treatment, has been shown in patients with stabilized sequelae (long-standing paralysis) by several observational studies.23-26 Beurskens and Heymans 27 confirmed these findings through a randomized trial, showing a significant effect of mime therapy in an experimental group as opposed to a control group who received no treatment while on a waiting list. Benefits of physical therapy were stable 1 year later. 28 As shown by Pereira and colleagues 29 in a recent systematic review on the effect of facial exercise on facial palsy, the above-mentioned trial presents sufficient data to perform a meta-analysis and to provide evidence that physical therapy is effective in this typology of patients.
In contrast, the evaluation of physical therapy efficacy in the acute clinical phase is more complex because of the high rate of spontaneous recovery. 5 In the literature, there are only a few experimental or quasiexperimental studies, most of which compare different physical techniques.30-33 Only 1 randomized trial has been designed to compare patients who did and did not receive physical therapy during the acute phase of BP. 19 As shown by Teixeira and colleagues 18 in a recent systematic review, this study is at high risk of bias mainly because there is no description of random allocation, an unclear definition of blinded status of the assessors, and the short period of follow-up.
The present study was implemented to assess the efficacy of early physical therapy compared with only drug administration, in terms of time to improvement and grade of recovery of function. We tested 2 main hypotheses: first, that physical therapy procedures do not influence the rate of recovery or improve the grade of recovery but can be of help to the patient with a poor prognosis to better cope with paralysis; second, not all patients need physical therapy because it is possible to identify which of them have a favorable prognoses.
Methods
Study Design
The study was designed as a 6-month, independent, single-blinded, randomized controlled trial and implemented according to the rules of the CONSORT statement. 34 The protocol was approved by the local ethics committee; each patient gave written informed consent before commencing any study-related procedure. The eligibility criteria were age 15 to 70 years; unilateral “pure” BP diagnosed by clinical and neurologicl assessment; facial palsy severity, assessed by the House-Brackmann (HB) scale, ranging from grade IV to VI on the 10th day after the onset of palsy; onset of steroid treatment within 48 hours after the initial symptoms of BP as oral administration of prednisone 1 mg/kg for 10 days plus valacyclovir 500 mg 3 times a day for 6 days; not pregnant; no metabolic, neurologicl, infective, neoplastic, toxic, or iatrogenic disease; and no traumatic injury to the seventh nerve.
Study Groups and Randomization
Eligible patients were randomly assigned, in a 1:1.2 ratio, to 2 experimental groups: (1) a treatment group that received the standardized pharmacological treatment plus the intervention with physical therapy (group B) and (2) a control group that received only the standardized pharmacological treatment but not physical therapy (group A). This ratio was set, assuming drop-out rates, during the 6-month follow-up period, of 10% and 30%, respectively, for groups B and A. According to previous studies,5,9 we also expected complete recovery proportions of 0.85 in group B and of 0.58 in group A (as estimated by the 1-sided Fisher’s exact test). Consequently, we needed 45 individuals in group B and 54 in group A to achieve a power of 80% (type II error), with a 2-sided significance level of 5% (type I error).
Furthermore, to ensure a more reliable and accurate comparison of the 2 groups, the randomization procedure included stratification according to the HB grades at enrolment, 10 days after palsy onset (IV, V, or VI). Therefore, each stratum comprised 15 and 18 patients in groups B and A, respectively. The randomization schedule, one for each stratum, was arranged using the random number tables (ie, aleatory or dependent on chance) created in 1959 by the Institute of Statistics of “Sapienza” University in Rome. 35 The random number tables were derived using the unit digit of the first extract numbers of each national lottery wheel from 1862 to March 1955. Therefore, these numbers were uniformly distributed and truly random and not computer-generated pseudorandom numbers.
Study Procedures
Assessment of patients was carried out using 2 of the routinely used systems in clinical practice19,27,30,36,37: the HB facial grading system 38 (see Supplementary Table 1 at http://nnr.sagepub.com/content/by/supplemental-data) and the Sunnybrook facial (SB) grading system 39 (see Supplementary Figure 1 at http://nnr.sagepub.com/content/by/supplemental-data).
The first system was selected to measure the global degree of paresis/paralysis for its simplicity of administration, most frequent use, and its robustness, as assessed by Smith et al, 40 who estimated an internal consistency of 0.75, and Evans et al, 41 who found an interobserver reliability of 93%.
As HB lacks in delivering satisfactory information in regional facial function, 42 the SB was added to obtain detailed data on symmetry—at rest and during motion—and synkinesis. It was selected for its psychometric characteristics; as described by Ross et al, 39 it has a good sensitivity to clinical changes (P = .0000), and as assessed by Pavese et al, 43 it has a high internal consistency (Cronbach α of .91) and an elevated repeatability (interrater reliability = 0.96; intrarater reliability = 0.98). The overall agreement between the SB and HB facial grading systems showed a weighted k value ranging from 0.56 (for days 1 to 14) to 0.71 (for days 61 to 180). 44
Each patient was videotaped on his or her first visit to the clinic, 10 days thereafter, and then monthly until the end of follow-up (sixth month), for a total of 8 evaluation sessions. Video recordings were evaluated by an experienced and trained ear, nose, and throat physician blinded to the group assignment.
Interventions in the experimental group were conducted by a physiotherapist and speech therapist, trained according to the neuromuscular retraining principles.14,23,31,45,46 Each patient was treated in the outpatient clinic by means of individual sessions lasting 45 minutes each, twice a week for the first 3 months and once a week thereafter, until the follow-up was completed. Patients were instructed to follow a daily program of exercise implemented during the individual sessions, which are detailed below.
They were educated on facial muscle physiology and functions and changes induced by paralysis. Education was imparted regarding face massages to improve circulation, 10 minutes twice a day. Active motion exercises with and without mirror feedback were used to promote motor control and to avoid altered patterns of movements and overactivity of the unaffected side. The aim was to train patients to produce symmetric, isolated, small movements with a slow execution; to avoid the activation of abnormal motor patterns; and to reinforce a normal physiological response and offer better control and the opportunity to learn new patterns of movements. Patients were instructed to practice at home daily, 4 times/d, for no more than 10 minutes. Daily management of drinking, eating, and smiling problems were addressed with strategies identified during the individual sessions. Daily management of speech was addressed, training the patient with modified patterns of motion to produce vowels, and bilabial, labial-dental, and affricate consonants to allow more symmetric movements. Stretching of face muscles and relaxation activities were implemented when signs of spasm or synkinesis were present.
In the case of complete recovery, rehabilitation was no longer performed, although assessment continued until the sixth month.
Outcomes Definition
The primary outcome was the proportion of patients to reach a HB grade of II or less at the end of the 6-month follow-up period.
The secondary outcomes were the time to reach a HB grade of II or less, the differences over time in the mean SB total score, and the proportion of patients having a synkinesis subscore of 0 (ie, no synkinesis) at the end of the 6-month follow-up period.
Statistical Analysis
Analyses were carried-out according to the intention-to-treat (ITT) principle.47,48 All randomized patients were analyzed for primary and secondary outcomes, regardless of whether they dropped out of the study. Missing values were replaced according to the last observation carried forward approach; therefore, final values of the outcome variables are replaced by the last known value before the participant was lost to follow-up.
Values are expressed as means (±standard deviation) for continuous variables and proportion for categorical variables, as appropriate. Demographic and clinical data considered at baseline included the following: sex (female or male), age, HB grade, and SB score. Differences between the 2 treatment arms (ie, A and B groups) in baseline characteristics were tested using Fisher exact test, the χ2 test, or the Mann-Whitney U test, as appropriate. The differences in proportions of patients between groups (A vs B) who experienced recovery of function and disappearance of synkinesis were investigated by logistic regression analyses adjusted for age and sex, with the prespecified outcome measure as the dependent variable and group assignment as the independent variable.
The time taken to reach the recovery of function (as defined above) was investigated using a Cox proportional hazard regression model, adjusted for age and sex. We considered the length of follow-up (in months) between baseline and the last 6-month visit or outcome reach as the main time variable, whichever came first. Survival curves, showing the time-to-event unadjusted analysis, were also provided and the differences between the 2 groups analyzed by the log-rank test.
Changes over time in SB scores were investigated by means of an analysis of variance (ANOVA), with time (T0, T1, T2, T3, T4, T5 and T6 monthly visits) and treatment group (A vs B) as the between-subjects factors. A time-treatment interaction analysis was run to evaluate the treatment effect on the SB score over time, after adjusting for age and sex. Simple contrasts were conducted for each significant time main effect to determine the source of the significant difference, where necessary.
All 3 outcomes were investigated in the entire study population as well as after stratifying patients according to their baseline HB grades (IV and V/VI). P values less than .05 (2-sided) were considered as significant. Analyses were carried out using the Statistical Package for Social Sciences, version 16.0 (SPSS Inc, Chicago, Illinois).
Results
Participants
A total of 232 individuals affected by BP from June 2008 to May 2010 were invited to take part in the study. All patients were recruited at the University Hospital “Umberto I” of Rome, referred by the neurologists of the emergency department, where they arrived soon after onset of symptoms and having started pharmacological treatment as outlined above. According to the randomization tables described above, 87 patients who met all the eligibility criteria were assigned to the 2 arms (48 in group A and 39 in group B). Their baseline characteristics are summarized in Table 1. The 2 groups were comparable in terms of baseline demographics and clinical characteristics.
Baseline Characteristics of the Per-Protocol Population (n = 73), According to Treatment Groups. a
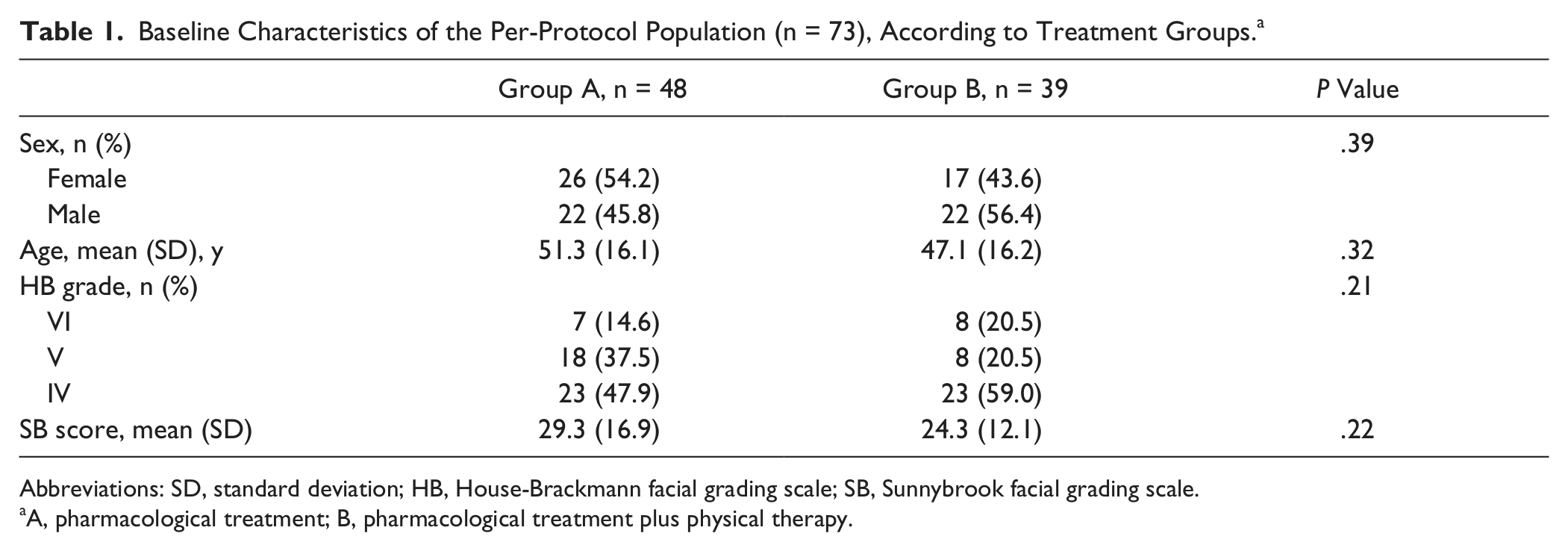
Abbreviations: SD, standard deviation; HB, House-Brackmann facial grading scale; SB, Sunnybrook facial grading scale.
A, pharmacological treatment; B, pharmacological treatment plus physical therapy.
Figure 1 shows the flowchart of the study. The number of dropouts after randomization in group A was high (n = 11), especially among those patients presenting with higher HB grades because of the desire to get rehabilitation. Therefore, a total of 76 patients (37 in group A, 39 in group B) concluded the follow-up according to the study protocol before reaching the preplanned sample size.
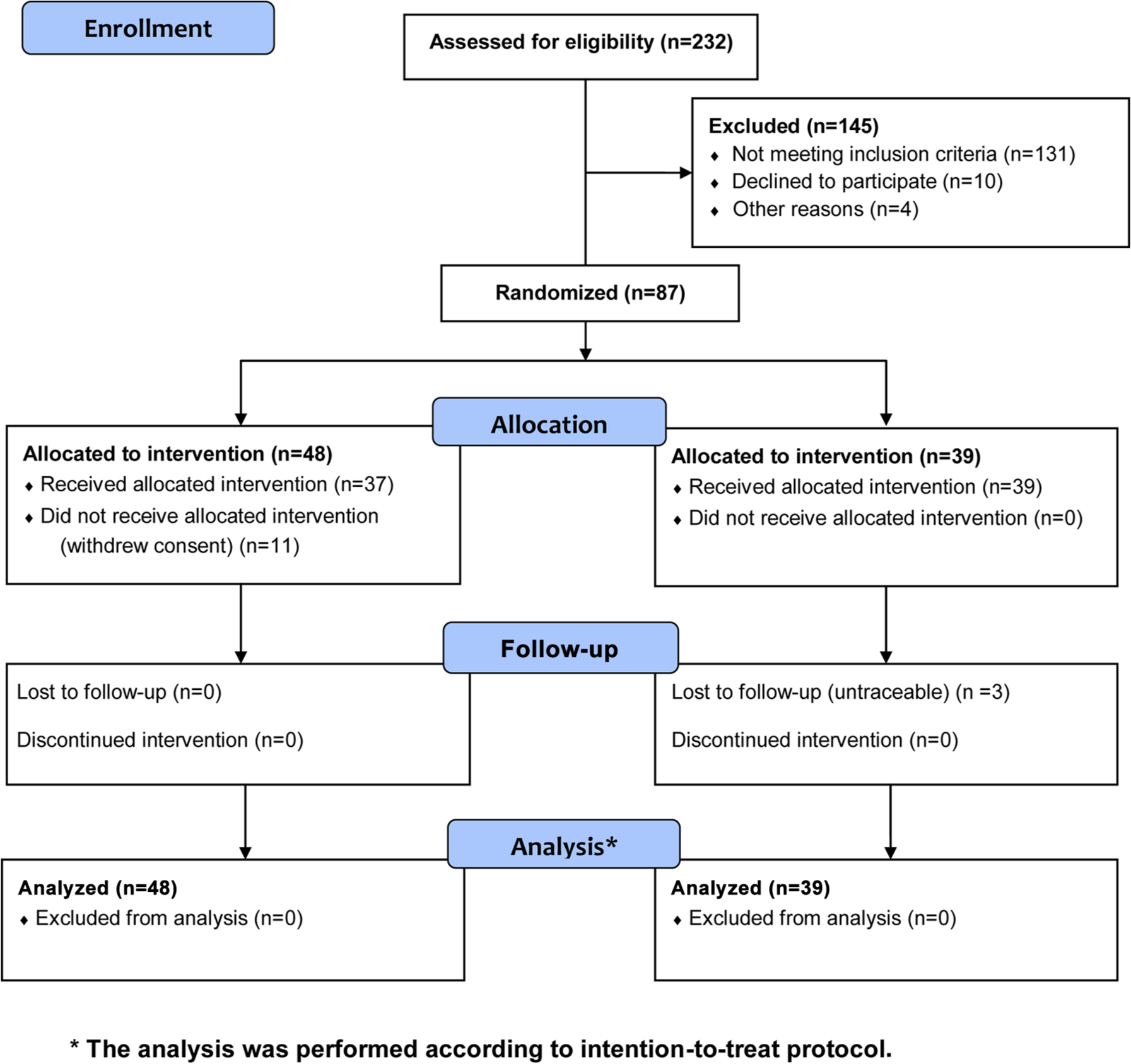
Study flowchart.
Primary Outcome
No significant effect of physical therapy treatment on the primary outcome was found when the entire study sample was taken into consideration. As shown in Table 2, at the end of the 6-month follow-up period, 36 (75%) patients in group A and 33 (86%) in group B experienced recovery of function (P = .27), as defined in the outcome definition section. In contrast, when stratification was considered, the physical therapy treatment had a significant effect (P = .038) on patients with HB grade V/VI (see also Table 3). All the patients with HB grade IV reached the primary outcome (final HB grade I or II), regardless of the treatment group assignment.
Differences in Proportion of Patients Reaching HB Grade II at the End of the 6-Month Follow-up Between the 2 Treatment Groups A and B, as Calculated by Propensity Score Inverse-Weighting-Adjusted Multivariate Logistic Regression Analyses. a
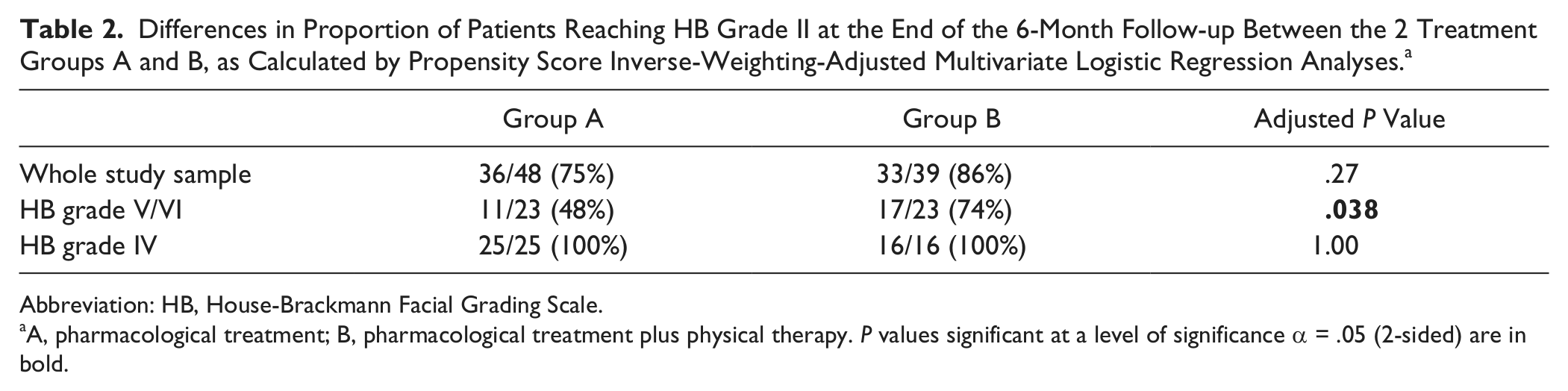
Abbreviation: HB, House-Brackmann Facial Grading Scale.
A, pharmacological treatment; B, pharmacological treatment plus physical therapy. P values significant at a level of significance α = .05 (2-sided) are in bold.
Sex-and Age-Adjusted Cox Regression Models to Reach HB Grade II or I at the End of the 6-Month Follow-up. a
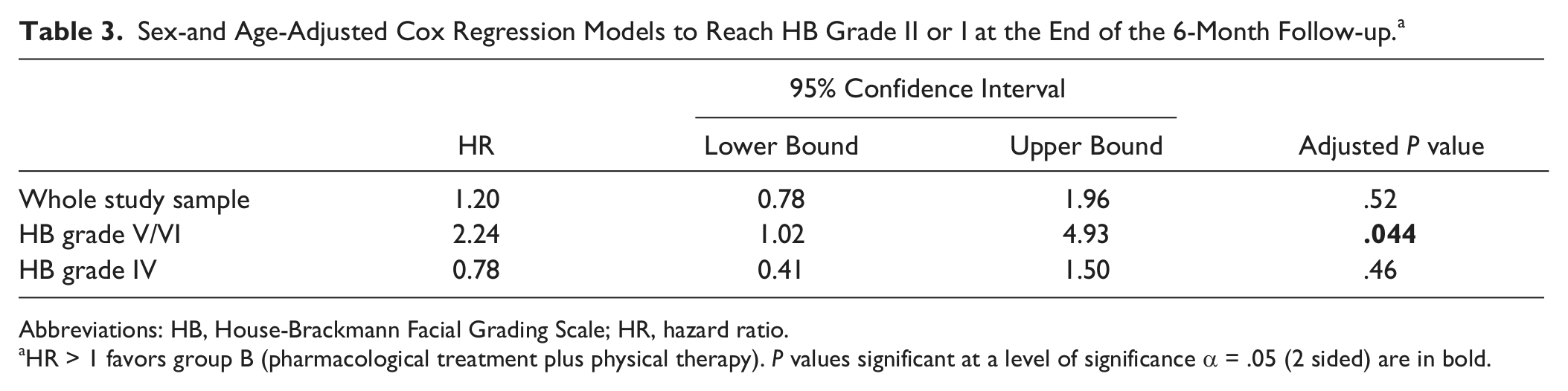
Abbreviations: HB, House-Brackmann Facial Grading Scale; HR, hazard ratio.
HR > 1 favors group B (pharmacological treatment plus physical therapy). P values significant at a level of significance α = .05 (2 sided) are in bold.
Secondary Outcomes
There were no differences in the time taken to reach the primary outcome between the 2 groups (hazard ratio [HR] = 1.20, 95% confidence interval [CI] = 0.78-1.96; P = .52). In the entire study sample, the only variable able to predict a shorter time to reach the outcome was the baseline HB grade (HR = 5.05, 95% CI = 3.02-8.45; P < .001). The Kaplan-Meier curve shows that 50% of the study sample reached the outcome within the second month of follow- up when the HB grade at baseline was IV and within the fourth month when the HB grade at baseline was V or VI (Figure 2).
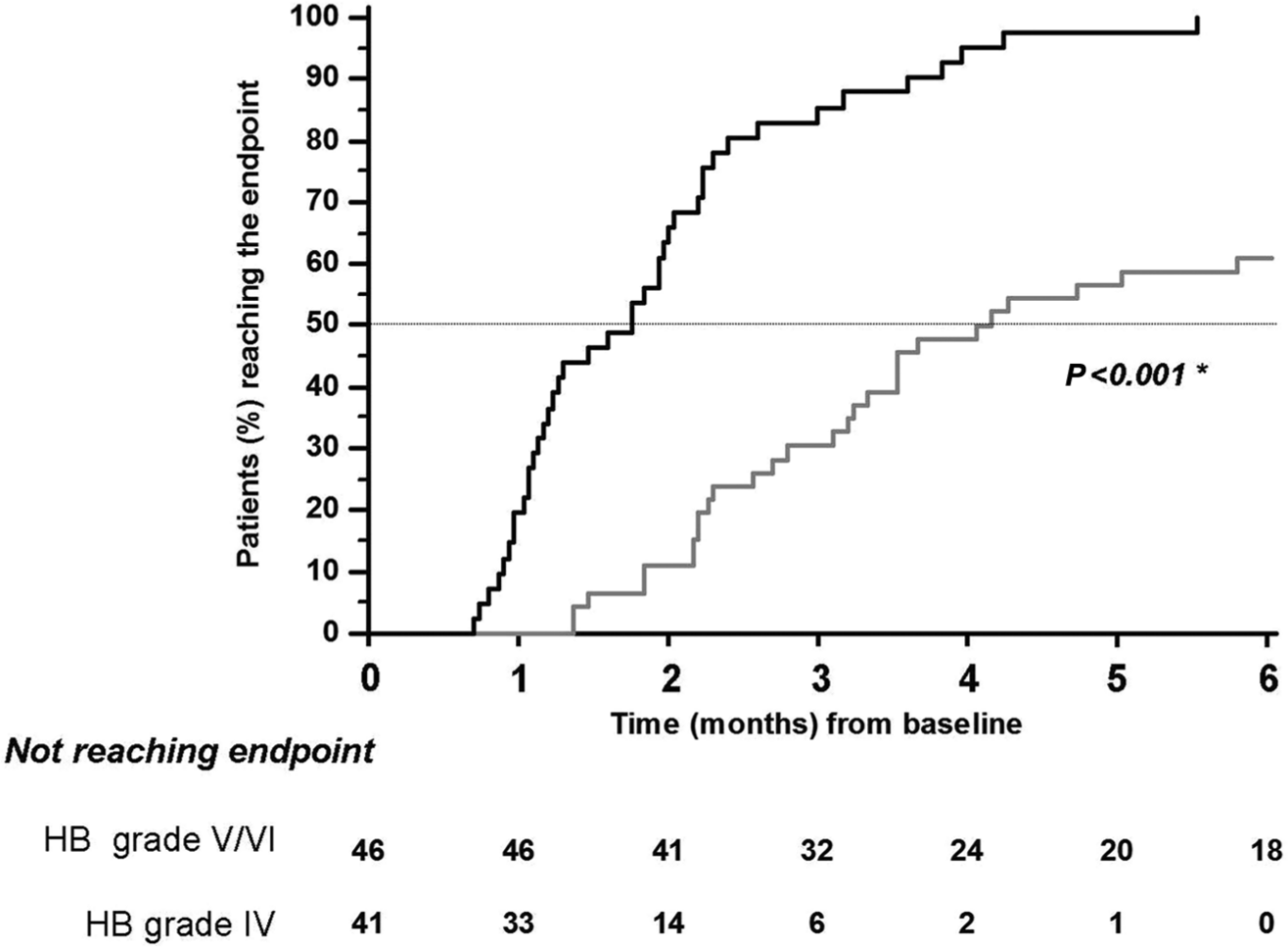
Kaplan-Meier curves showing time taken to reach primary outcome (ie, House-Brackmann [HB] grade II) according to HB grade at baseline. Black line, HB grade IV; gray line, HB grades V/VI. *P value by log-rank test.
In contrast, when taking into consideration only the subgroup of patients with a baseline HB grade V/VI, it was found that group B reached the primary outcome faster than group A (HR = 2.24, 95% CI = 1.02-4.93; P = .044), as also shown in the Kaplan-Meier curve (P = .048 by the log-rank test; Figure 3). This finding was not replicated in the subgroup of patients with a baseline HB grade IV (HR = 0.78, 95% CI = 0.41-1.50; P = .46).
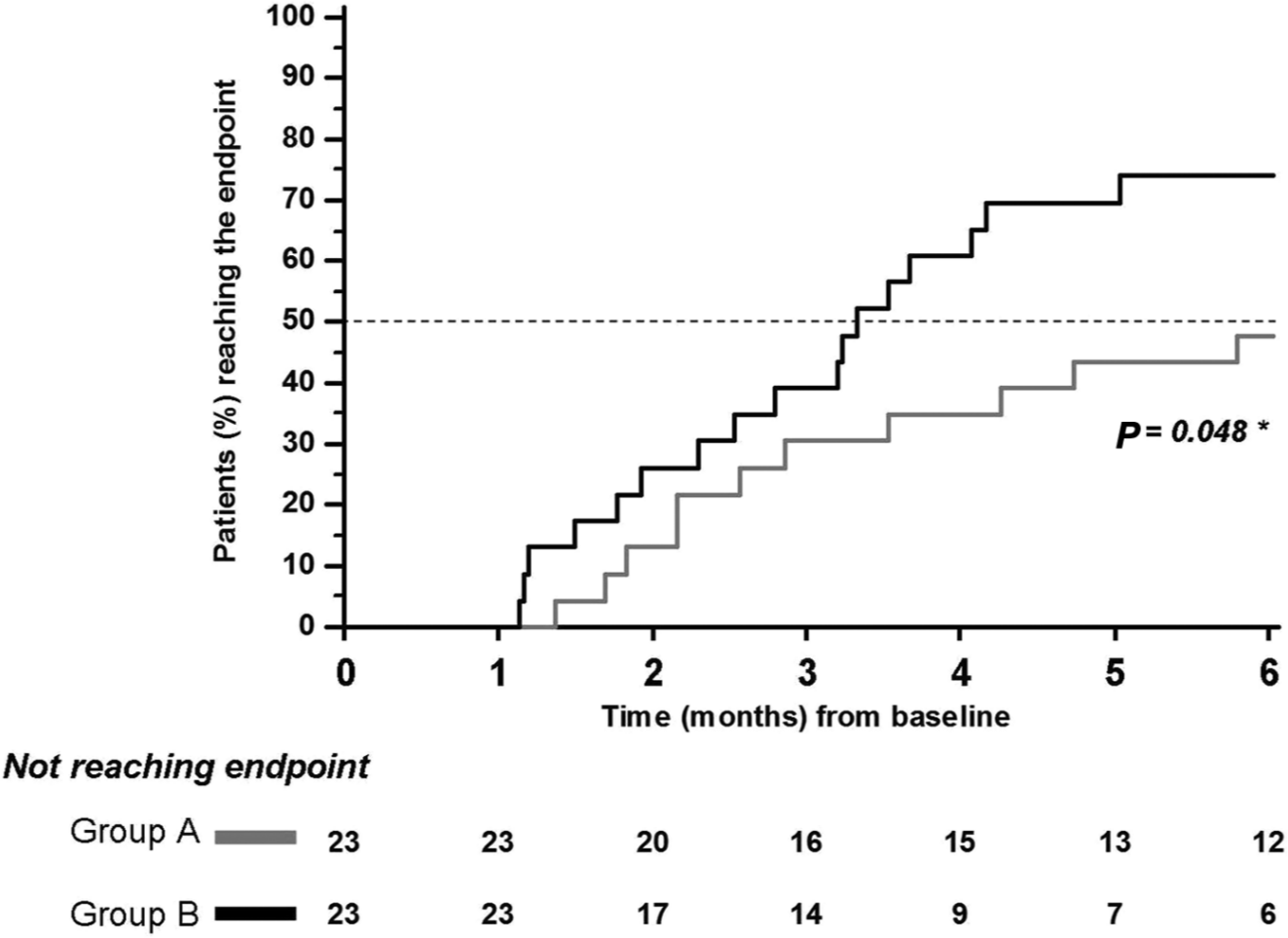
Subgroup of patients with House-Brackmann (HB) grade V or VI at study entry (n = 38): Kaplan-Meier curves showing time to reach primary outcome (ie, HB grade II) according to treatment group. Group A, pharmacological treatment; group B, pharmacological treatment plus physical therapy. *P value by log-rank test.
At the end of the 6-month follow-up period, SB scores were 80 (28) and 86 (23) for the A and B groups, respectively (P = .67 by the Mann-Whitney U test). A significant effect of time was observed, indicating that SB scores increased over time in both groups (F = 8.29; P < .001). Moreover, there was also a significant Time × Treatment effect (F = 2.58; P = .025), suggesting that the rehabilitation treatment could have led to a greater increase in the SB scores at specific time points. This was demonstrated by a simple contrast analysis that revealed significant differences between the 2 groups at T4 (F = 5.09; P = .018), T5 (F = 7.86; P = .006), and T6 (F = 7.39; P = .008) examinations (when compared with the previous examination; Figure 4).
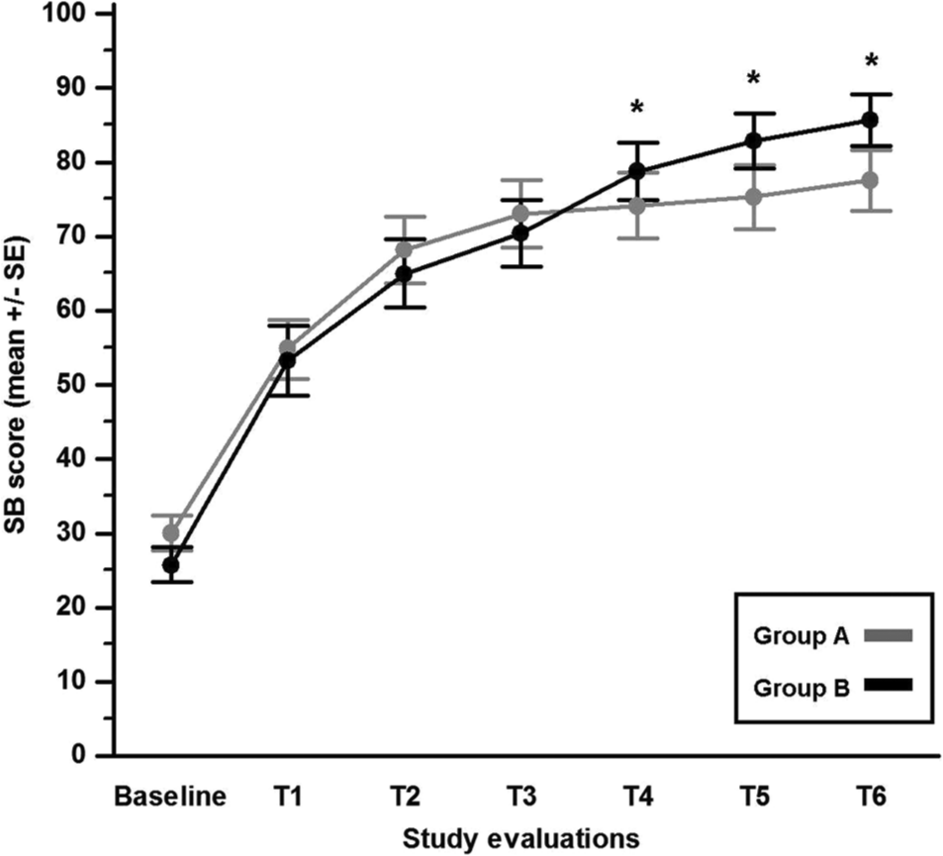
Changes (expressed as mean ± standard error [SE]) in Sunnybrook (SB) scores over the 6-month study period, according to treatment group. Group A, pharmacological treatment; group B, pharmacological treatment plus physical therapy. *P < .05.
When only those patients presenting with a HB grade of V or VI were taken into consideration, a significant difference was observed between the 2 groups for final SB scores: 60 (29) and 79 (27), for the A and B groups, respectively (P = .021 by the Mann-Whitney U test). In contrast, when we considered only patients presenting with a HB grade of IV, the final SB scores did not significantly differ for the A and B groups: 98 (7) versus 97 (7); P = .71 by the Mann-Whitney U test.
Nevertheless, considering the rate of recovery, SB scores increased over time, regardless of the physical therapy treatment, even after dividing the entire study population according to baseline HB grades (IV and V/VI; Table 4).
Summary of Sunnybrook Facial Grading Scores Over Time, According to HB Grade at Baseline. a
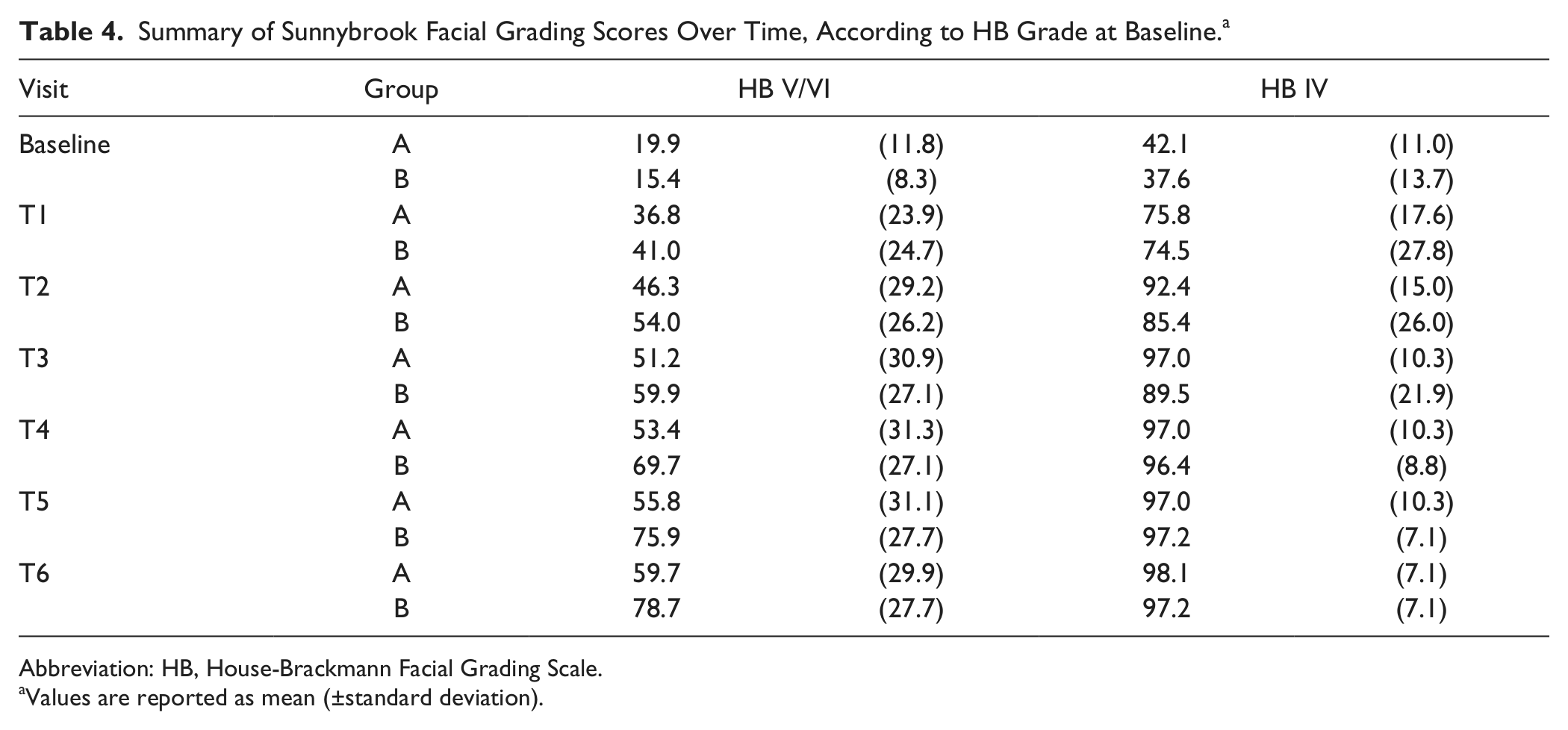
Abbreviation: HB, House-Brackmann Facial Grading Scale.
Values are reported as mean (±standard deviation).
Synkinesis was found in 25 (29%) patients, and in the majority of cases, it started after the fourth month of follow-up and persisted even at the end of the study. Only one 61-year-old woman had the synkinesis started at the second month of follow-up; at the end of the study, this patient also had the highest synkinesis subscore, equal to 7. As far as the proportion of patients with a synkinesis subscore of 0 at the end of the study period was concerned, no differences were found between the 2 treatment groups (Table 5). Finally, a logistic regression analysis showed that the only baseline clinical variable useful in predicting which patients might develop synkinesis during follow-up was the presence of a HB grade of V (odds ratio [OR] = 4.32, 95% CI = 1.33-14.03; P = .015) or VI (OR = 9.60, 95% CI = 2.34-39.42; P = .002), irrespective of age and sex.
Differences in Proportion of Patients Having No Synkinesis (ie, a Score of 0 in the Corresponding Scale) at the End of the 6-Month Follow-up Period Between the 2 Treatment Groups a as Calculated by a Propensity Score Inverse-Weighting Logistic Regression Analysis.
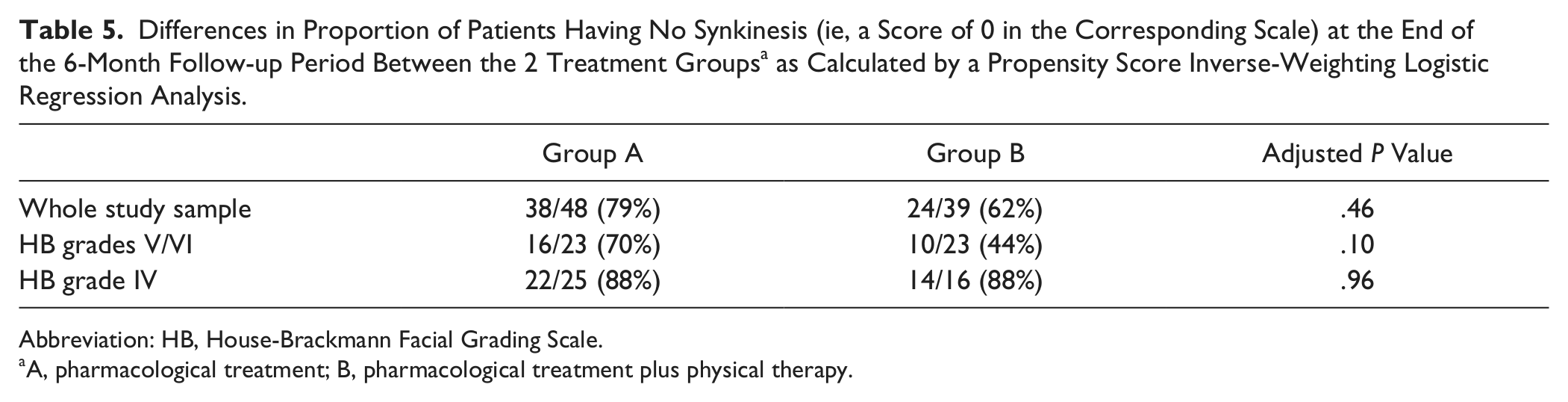
Abbreviation: HB, House-Brackmann Facial Grading Scale.
A, pharmacological treatment; B, pharmacological treatment plus physical therapy.
Discussion
Physical therapy has played an important role in the treatment of BP. Over the years, approaches have focused more and more on the specificity and peculiarity of facial nerve physiology and on permanent sequelae related to the recovery processes during nerve regeneration. These procedures and strategies, implemented for long-standing facial palsy, have been developed to help the patient control the symmetry of the face, through slow movements and voluntary control of synkinesis. The patient is encouraged to experiment with different modes of movement and to practice and automatize them in daily activities and expression of emotions.10,26 Treatment often includes botulinum toxin, massage, and stretching to reduce synkinesis and hypertonus.20,21 Specific exercises and compensation strategies are implemented also for the correct management of problems occurring when drinking, speaking (eg. slowing speech), eating, and smiling.24,26,49 These approaches may improve health status and quality of life, 14 as supported by the experimental results of Beurskens and colleagues.27,28 Two randomized clinical studies designed to assess the efficacy of mime therapy have shown how significant improvements can be obtained both rapidly 27 and 1 year after rehabilitation. 28 Rehabilitation seemed to be effective in regaining facial symmetry, in reducing the severity of paresis by 0.6 grades on the HB scale, and in controlling synkinesis. Functional improvements were reflected in the patient’s perception of disability, measured using the Facial Disability Index 50 : patients in the experimental group continued to show an improvement even 1 year after the end of rehabilitation. 28
Diels and Combs 14 and Coulson et al 26 have shown similar results on facial palsy sequelae using neuromuscular retraining and video self-modeling. Unfortunately, these outcomes are characterized by low levels of evidence, 18 mainly related to lack of experimental protocol design or to an excess of potential bias because of small sample size, short follow-up period, or absence of randomization of treatment. The lack of significant data is more evident when intervention is considered in the early phase of palsy, when the high rate of spontaneous recovery complicates the assessment of the effect of any intervention.
The present study was originally planned to control and reduce bias (selection, allocation, and attrition) through accurate sample size count, randomization of treatment, and blind assessment. Therefore, its main limit is the failure to achieve the calculated sample size. In our study, a significant number of V and VI HB grade patients dropped out after being assigned to the control group when they did not observe any spontaneous improvement because they wanted to get physical therapy. To overcome these limitations, an ITT analysis was carried out, and missing values were replaced according to the last-observation-carried-forward approach. 48 Although it has been reported that this method may introduce bias, 47 this approach is simple and does not require statistical sophistication. 51 Moreover, it is likely that in our study patients enrolled in the control group were those who did not spontaneously recover from BP. Therefore, replacing missing final outcome values by the last known values should not have strongly affected the analyses.
Despite the limits discussed above, to our knowledge, the present study is the largest clinical trial, with the longest follow-up, focusing on the effect of physical therapy in the early phase of BP compared with only drug administration. Moreover, the present study is the first in which patients have been stratified according to the severity of paresis and where the patients’ assessment was initiated at the same point of time, 10 days after the onset of palsy, considered as the most effective time to evaluate the degree of damage. 52
As expected, almost all patients showed spontaneous recovery. The differences between treated and control patients did not reach statistical significance, although results showed a positive trend for treated patients in terms of grade and time of recovery.
A different result was found on analysis of participants presenting with IV and V/VI HB grades at the time of enrolment. The rehabilitation treatment had a significant effect on grade (P = .039) and time (P = .04) of recovery. Results on efficacy of physical therapy are in agreement with those of Barbara et al. 19 However, comparison with this study is limited by differences in the characteristics of the patients enrolled (HB grade III-VI vs IV-VI), physical therapy procedures (Kabat vs NMR), and length of follow-up (15 days vs 6 months).
When only those patients with HB grade IV were taken into consideration, we found that all reached the primary outcome (final HB grade of I-II), regardless of the treatment. This finding can be compared with those reported by Peitersen, 5 who, in his study on the spontaneous course of 2500 peripheral facial nerve palsies, reported a complete recovery of 94% in those patients with an initial incomplete palsy; 6% of the differences between our findings and Peitersen’s can be related to the different grading systems used (House-Brackman vs Peitersen Grading System): Peitersen grade III (severe but incomplete) includes HB grades IV and V, whereas we considered grade V separately. Complete spontaneous recovery in the HB IV group could be explained by the presence of neuropraxis in these patients, 53 although we do not have electromyography and electroneurography data to support this hypothesis.
Less severe paresis (II-IV) would appear to have a positive spontaneous prognosis and not benefit from physical therapy. This is an important aspect from the viewpoints of clinical practice and cost-effectiveness. The speed of recovery experienced by these patients is such that improvements can become evident within the first weeks: this in turn has a positive impact on self-perception and allows them to trust the clinicians in a “wait and scan” condition.
In our trial, 23 (31%) patients developed persistent synkinesis, as assessed at the end of the study, regardless of the group assignment. Hence early rehabilitation does not appear to prevent or reduce synkinesis, although the number of patients with this finding may have been too low or the follow-up time too short; the usual onset is at the fourth to sixth month and continues to evolve throughout the twelfth month after the onset of palsy.
Conclusions
This study is the largest randomized clinical trial to focus on the effect of physical therapy in patients in the early phase of BP. Overall results and ITT statistical analysis strongly indicate that physical therapy in BP is effective in the more severe (V-VI) grades only, whereas HB grades II to IV result in complete spontaneous recovery. Also, at the 6-month follow-up, early physical therapy did not appear to prevent or reduce the occurrence of synkinesis. These findings might help in clinical practice for counseling of patients and facilitate decision making regarding who may most benefit from physical therapy, to optimize the use of health care resources.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.