
Abstract
Background and Objective. Unilateral neglect due to parieto-temporo-frontal lesions has a negative impact on the success of rehabilitation, and prism adaptation (PA) enhances recovery from neglect. However, it is unclear if this effect holds also in severely impaired patients and/or in the postacute phase of rehabilitation. Moreover, it is not known whether PA affects all aspects of neglect recovery or ego-centered spatial orientation only. Methods. Sixteen patients in a postacute stage (on average 36 days after a large right cerebrovascular stroke) were entered into a series of single case design studies with 4 measurements: 2 before and 2 after 1 week of PA treatment. All patients had severe neglect (showing trunk, head, and eye deviation; canceling less than 20% of targets in a visual cancellation test). Lesions were transferred to a standard brain to analyze size and location. Results. Patients improved in cued body orientation and in the cancellation task, that is, in ego-centered neglect. However, none of the measures used to evaluate neglect of left side of objects irrespective of their position on the right or left side of the patient (allocentric neglect) showed an improvement. Treatment effects were not influenced by total lesion size, but lesions including the postcentral cortex were related to smaller recovery gains. Conclusion. PA is helpful in treating severely impaired patients in the postacute phase, but the effect is restricted to ego-centered neglect. Lesions in the postcentral cortex (middle occipito-temporal, middle temporal, and posterior parietal areas) seem to limit the effect of PA.
Introduction
Neglect has been defined as an inability to orient and to respond to stimuli located in space of the contralateral side to the brain injury. 1 It is a frequent consequence of stroke or other brain disorders associated with lesions in the (right) parietal, temporal, and frontal cortex. Neglect is, in case of no spontaneous recovery during the first weeks of the illness, related to longer treatment time in rehabilitation units, less profit from physiotherapy, and less independence in activities of daily living. 2 During the past decades neglect has been the subject of a considerable number of well-designed treatment studies, and according to many reviews on cognitive rehabilitation, it is the domain with the highest evidence of effective intervention. 3 Although intensive cognitive rehabilitation of neglect seems to be effective,4,5 treatment options reducing a usually large number of individual sessions would be welcome for their cost-effectiveness. Prism adaptation (PA) is one of several add-on therapies that have been studied to hasten recovery from neglect, and it has been shown in controlled studies that even a small number of sessions seem to be effective in reducing the attentional bias of neglect patients.6-11 A recent randomized controlled study 8 analyzed the impact of PA on functional outcome measured by the Functional Independence Measure (FIM). 12 While PA improved neglect symptoms in patients with weak to moderate neglect, a positive influence could not be found in severe cases. Moreover, most studies dealing with PA in neglect patients so far have focused on the chronic phase. Only one study analyzed the impact of PA on the outcome of the early recovery period after a stroke. 13 In that study, PA only had transient and no enduring positive effects on neglect. Aside from these issues, neglect is a syndrome encompassing different aspects of visuospatial inattention. 14 For example, neglect may concern unilateral inattention to spatial coordinates around the patients (equivalent to a rotation of the patient’s body axes and therefore a shift of perception of their environment toward the ipsilesional side). 1 It may also concern inattention to the contralesional side of perceptual objects—regardless of where these objects are positioned in the environment of the patients. 15 To the best of our knowledge, none of the previous studies on neglect analyzed whether PA improves ego-centered and/or allocentric neglect alone or together. To answer 3 questions—(a) is PA suitable to improve neglect in postacute and severely impaired patients, (b) does PA improve ego-centered and allocentric neglect, and (c) do lesions in specific brain areas modulate the degree of improvement after PA—we included 16 patients with large unilateral infarcts or hemorrhages within the territory of the right middle cerebral artery and treated them with 4 sessions of PA for neglect therapy.
Methods
Patients
All patients included in the study suffered from left-sided visual neglect as a consequence of a cerebrovascular disease (stroke, intracerebral bleeding, or nontraumatic subarachnoidal bleeding) and were admitted to our early rehabilitation unit.
Eighteen patients were screened and 16 individuals were treated. The 2 patients who were excluded were in a minimal responsive state and therefore unable to follow the treatment schedule. The included patients were judged as left visual neglect by their spontaneous body deviation and the tests described below.
After rotating the MRIcron 16 template into the same direction as the axial cCT scans of the patients (slice gap of 6 mm), their lesions were transferred manually to the corresponding template slices and the lesion volume (in mm3) for each patient was calculated (see Groh-Bordin et al 17 for a more detailed description of the method). We also generated overlap and subtraction images for patients with high and low impact of PA (see the following).
The study was approved by the ethical committee of the University of Oldenburg.
Procedure
Patients were examined 4 times: 2 times before and 2 times after PA. The assessments were separated by 5 to 6 days. Each assessment consisted of a clinical evaluation of the sitting position in the wheelchair (eye, head, and trunk orientation spontaneously and after asking the patients a number of defined questions, ie, after cueing, from a left-sided position; normal position = 0 points, some deviation toward the right = 1 point, strong deviation = 2 points; maximal neglect score = 6 points), the apples test, 18 line bisection, clock drawing, and reading. The apples test is a cancellation task where patients are supposed to cross out complete apples among incomplete apples, drawn with a gap on either side. It is assumed that ignoring full apples reflects ego-centered neglect, whereas incorrectly canceling apples with left-sided gaps assesses allocentric neglect. The line bisection test was composed of 3 lines, each 21 cm long. The starting points of the lines were shifted progressively toward the left to distinguish between ego-centered and allocentric neglect. Improvement in allocentric neglect would imply a reduction of the difference between the upper line with the outmost right starting point and the lower line with the outmost left starting point. Improvement in ego-centered neglect should not influence the difference score of the deviations in the upper and lower lines. We measured the deviation from the center of the lines and the marks of the patients in centimeters. In the clock drawing test, patients were supposed to fill in the numbers in a marked circle. Clocks not having any number drawn on the left side were counted as maximal distorted and scored with a “2,” clocks showing numbers on both sides but without symmetrical positioning were counted as minimally distorted (“1”), and clocks without spatial distortions as correct (“0”). We used 4 different reading texts of similar length (60 words), randomly varied in their sequence, to prevent influences of knowledge of the text on reading behavior. The number of missed words was counted. Patients were scored weekly with the FIM 19 and the Early Rehabilitation Barthel Index 20 (ERBI).
During therapy, the patients got 4 training sessions of 30 minutes’ duration each. Within each session, the training task was repeated multiple times. To increase compliance in our group of patients with severe impairments of visual and sustained attention, we combined the treatment with a goal. The patient sat in front of a Solitaire board while the investigator sat on the ipsilesional side. The patient wore prism goggles and the right visual field was restricted with an eye patch to prevent seeing the right hand moving from its starting position to the Solitaire board. The prism goggles had wedge-shaped glasses with a shift of 10° to the right-handed side. The task was to grasp for a wooden rod, which was placed randomly at different positions in front of the patient by the investigator, and to put the rod into one of the holes of the Solitaire board. After each grasp, the patient was told to take back his arm beside the wheelchair, to prevent seeing the hand just before reaching for the next rod and to retain the effect of the prism goggles. When all positions were filled, the patient was asked to remove the staffs one by one and to put them back into the basket, placed on the contralesional side on his own. In case the patient was unable to locate the basket on the contralesional side, the investigator helped to reach it.
As already noted, all participants were inpatients of an early rehabilitation unit. As obligatory in German early rehabilitation units, all patients received 5 hours treatment per day to improve transfer into a wheelchair, dressing, swallowing, orientation, and so on (additionally to the PA treatment).
Predictions for Statistical Evaluation
We predicted an increase of correctly canceled apples in the apples test, a decrease of missed words in reading, and an improvement in body positioning in the wheelchair in the case of treating ego-centered neglect effectively.
Improvements in allocentric neglect were defined as a decrease of wrongly canceled apples, a decrease of the difference in the ipsilesional deviation in the line bisection task, and an improvement in clock drawing.
Statistical Evaluation
We used Wilcoxon signed rank tests to evaluate the influence of age, sex, lesion size, and the treatment effect. Specifically, we compared the results of the first and second evaluations for spontaneous recovery or retest effects, between the second and third evaluation sessions for short-term treatment effects, and between the second and fourth assessments for the stability of the treatment effect.
Results
The clinical characteristics of the patients are summarized in Table 1.
Clinical Characteristics of Patients.
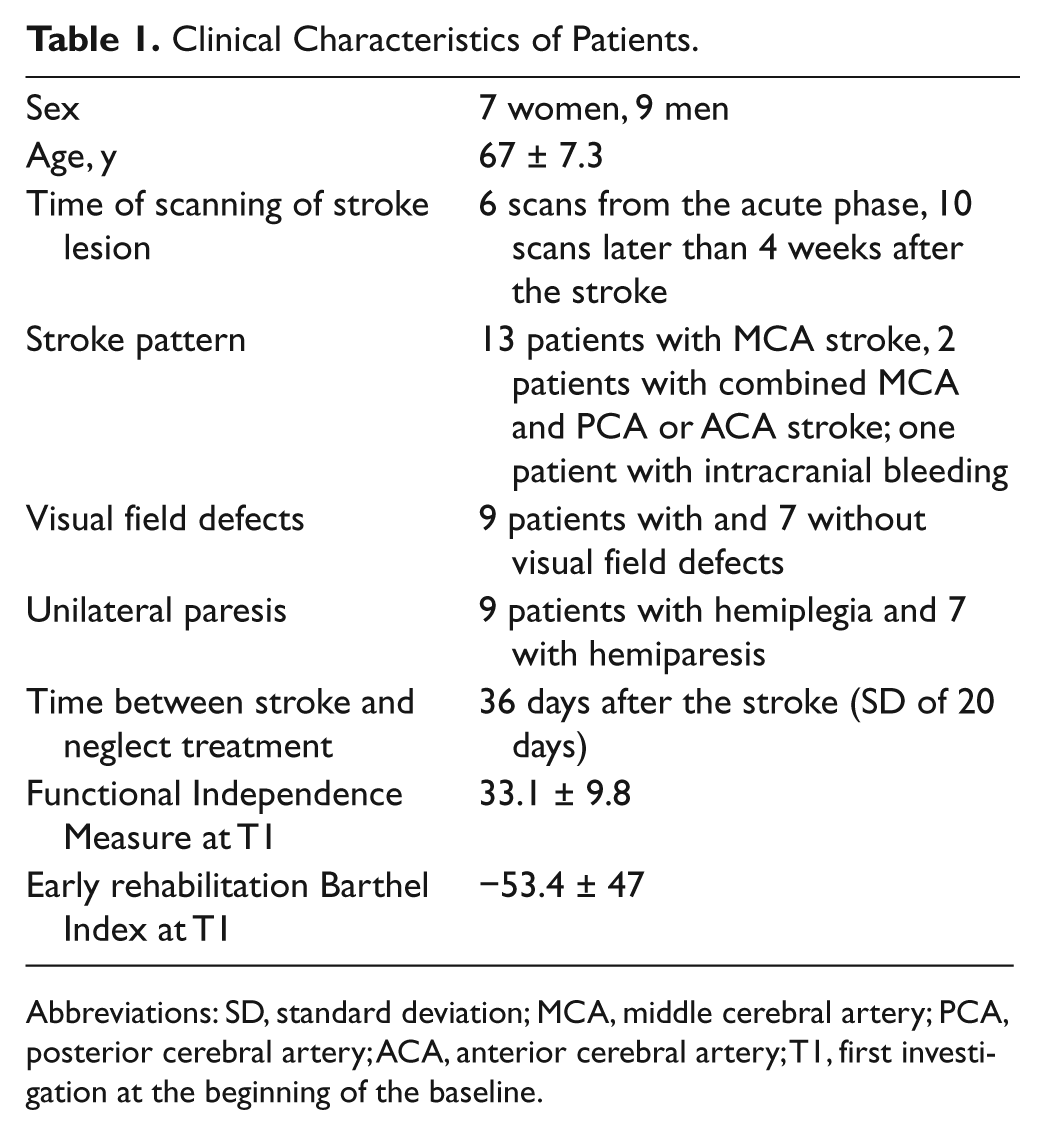
Abbreviations: SD, standard deviation; MCA, middle cerebral artery; PCA, posterior cerebral artery; ACA, anterior cerebral artery; T1, first investigation at the beginning of the baseline.
Notably, all patients suffered from severe neglect—showing body deviation toward the right, ignoring at least half of the paper sheet of the apples test and/or being unable to draw a clock and/or being unable to read the text (Table 2 shows the results of neglect testing at T1).
Neuropsychological Test Results at the 4 Time Points (T1, T2, T3, and T4).
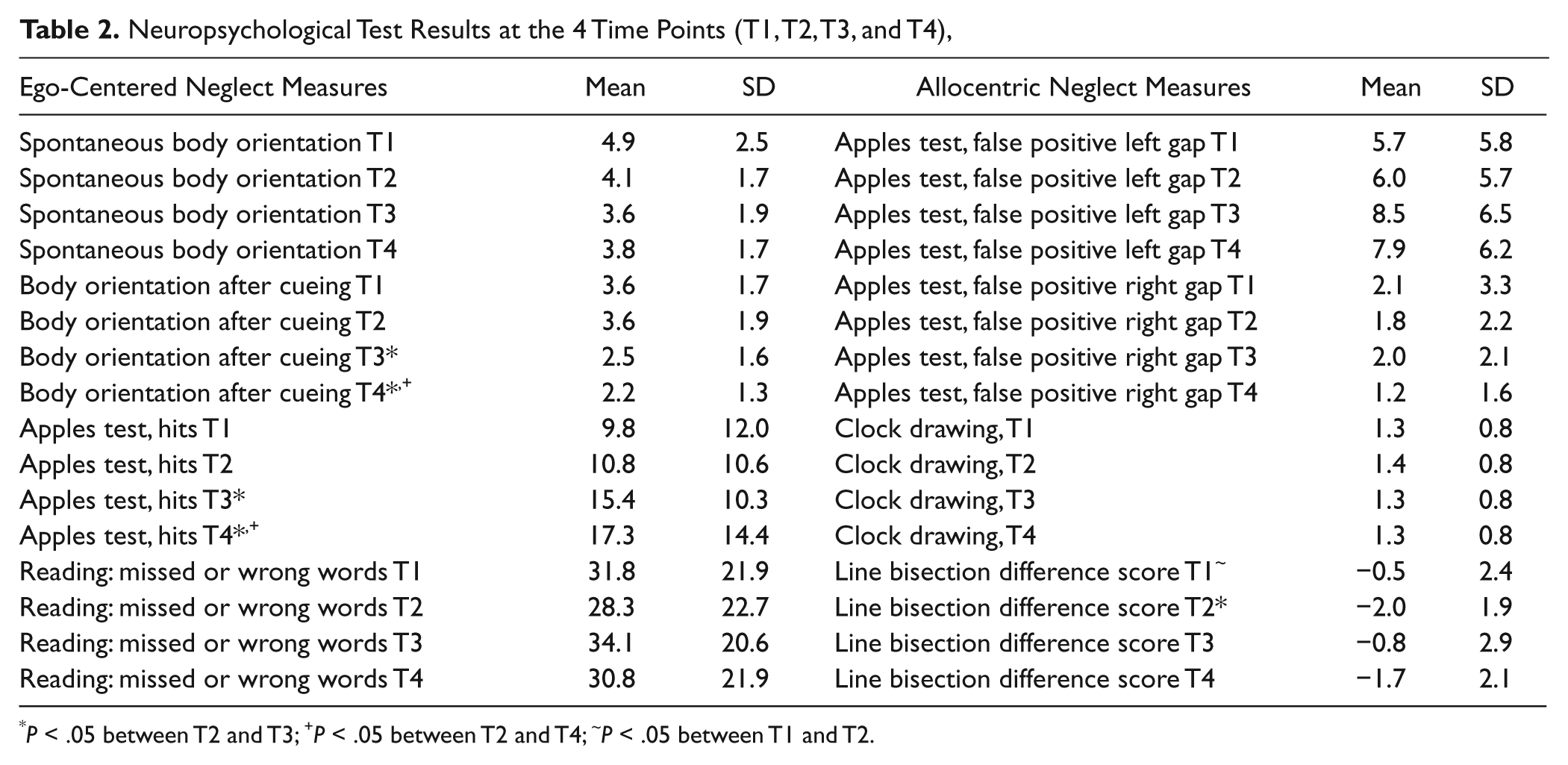
P < .05 between T2 and T3;
P < .05 between T2 and T4;
P < .05 between T1 and T2.
After treatment with PA, patients improved in cancellation of full apples in the apples test (Z = −2.045, P = .041; Table 2, Figure 1). The effect remained significant in the follow-up testing (Z = −2.743, P = .006). Moreover, patients improved in body orientation regarding their sitting position in the wheelchair after being asked the set of standard questions (Z = −2.263, P = .024, and Z = −2.203, P = .028, for the follow-up; Figure 2). This treatment effect was not significant in their spontaneous orientation. No other difference in test results was significant.
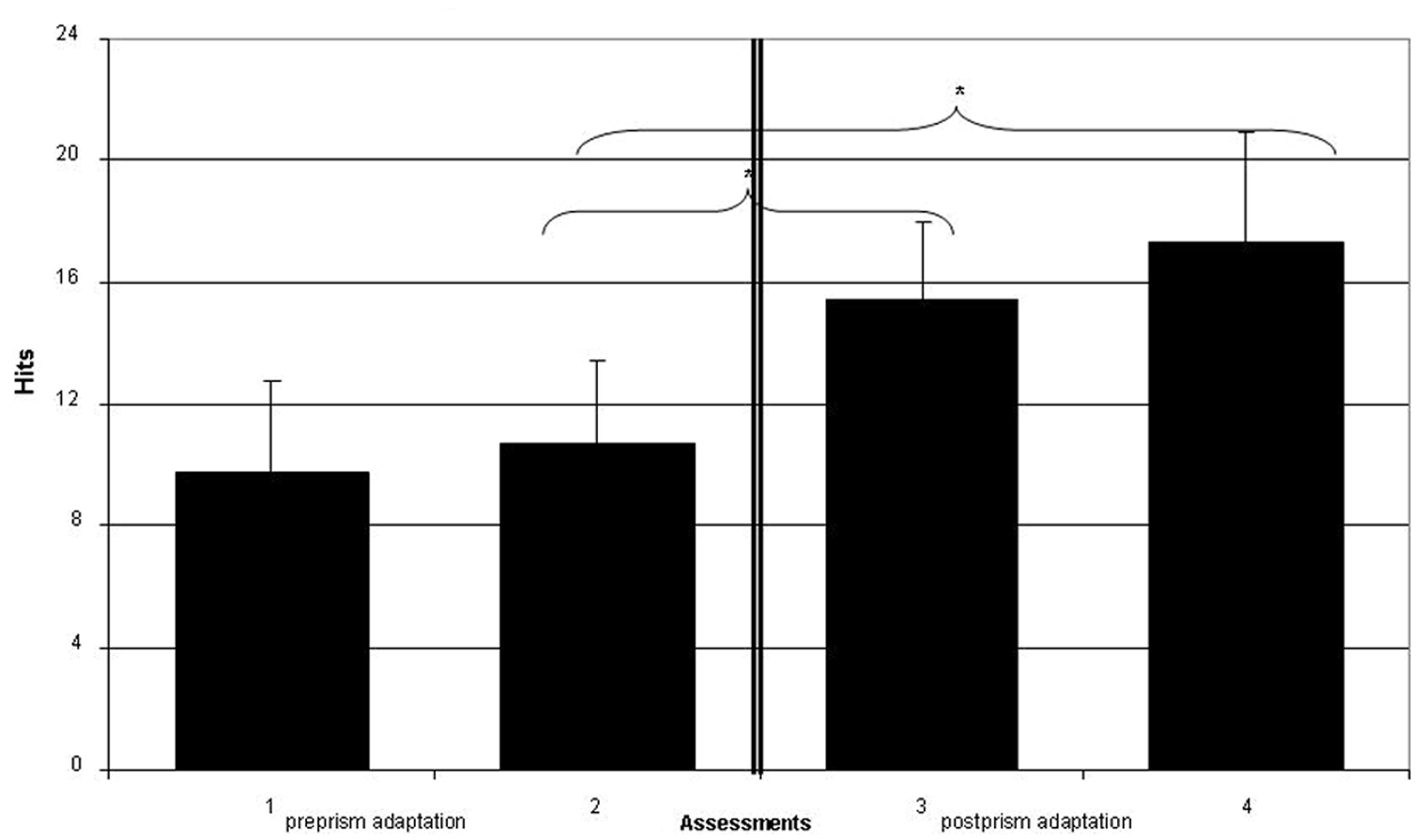
Hits (cancelled full apples) for each of the 4 assessments. Error bars represent standard error of mean. *Indicates significant differences.
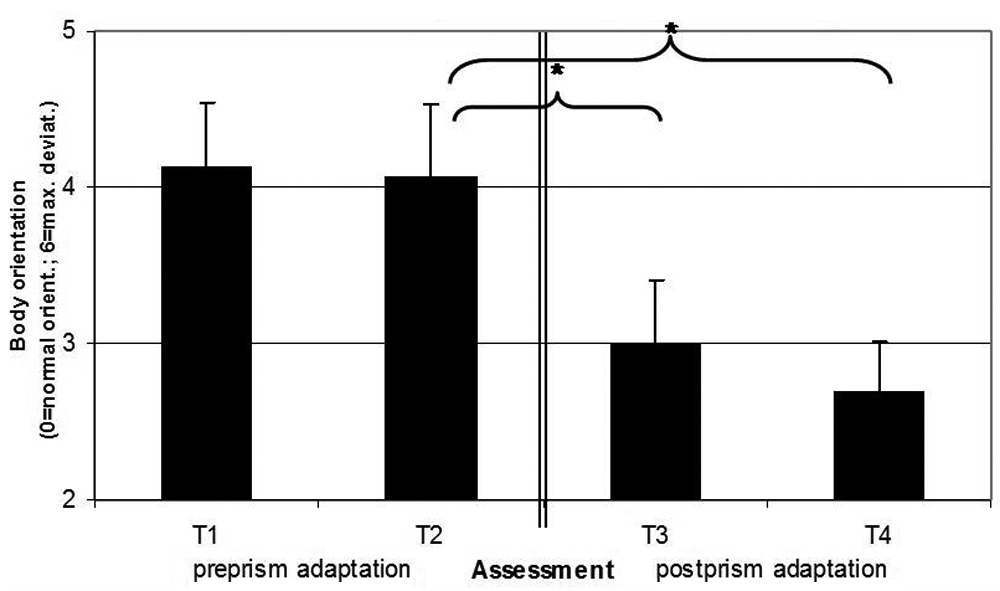
Trunk, head, and eye rotation of the neglect patients after being cued by questioning with a series of standard questions (0 = normal orientation, 6 = maximal ipsilesional rotation of trunk, head, and eyes). Error bars represent standard error of mean. Prism adaptation (PA) decreased ipsilesional shifts of the patient’s body rotation, but only after being cued by questions, whereas the spontaneous body orientation did not change (data not shown).
For allocentric neglect, the difference score in line bisection changed significantly between T2 and T3 (Z = −2.017, P = .044) and also between T1 and T2 (Z = −2.449, P = .014). Because of this shift of the baseline, no effect of PA on allocentric neglect can be postulated. In the apples test, the number of falsely crossed items with a left-sided gap increased (nonsignificantly) after PA, contrary to what would have been expected after a successful treatment (Figure 3).
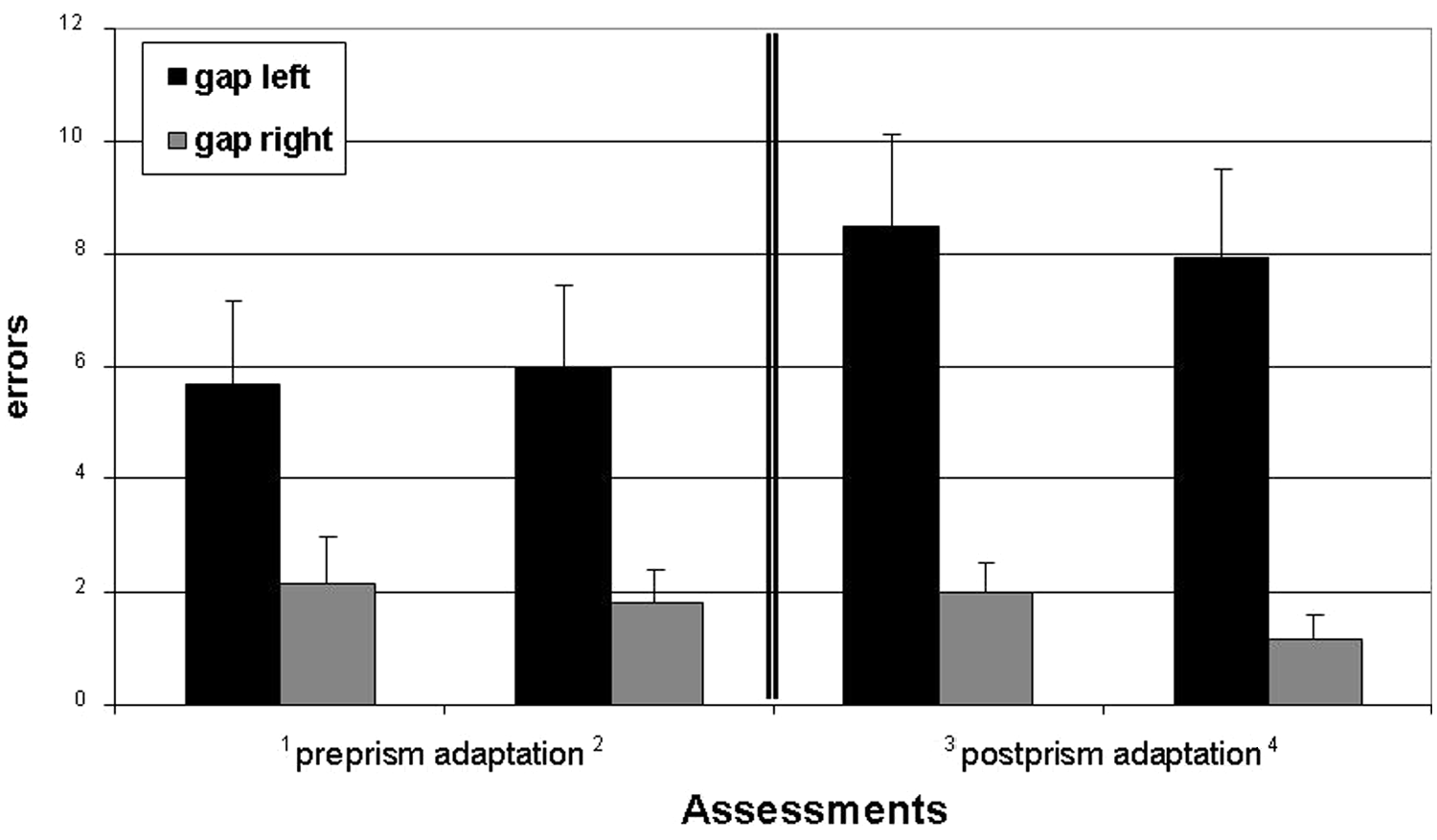
Errors (cancelled apples with left or right gaps) for each of the 4 assessments. Error bars represent standard error of mean. The figure shows that the patients canceled more apples with left-sided gaps, but not with right-sided gaps. Therefore, the patients improved in ego-centric (Figure 1), but not in allocentric, neglect.
The mean FIM was 33.1 at T1 and 35.3 at T4 (not significant). The ERBI was negative at T1 (−53.4) and improved to −48.5 at T2, to −37.2 at T3, and to −26.7 at T4. The negative values of the ERBI document an increased need of nursing compared with patients without any behavioral, vegetative, and swallowing risks. The statistical comparison of the ERBI scores showed a significant increase between T2 and T4 (Z = −2.366, P = .018), but not for the comparison of T1 and T2 and, more important, neither for the comparison of T2 and T3.
To analyze the relation between age, lesion size, lesion location, and treatment size, we divided the patients into 2 groups with large versus small or absent improvement in body orientation after cueing (using a median split), because this measure produced the highest significant change directly after the treatment with PA. Both groups did not differ in age (68 vs 65 years, P = .49) and lesion sizes (22.4 vs 38.1 mm3, P = .22), but strongly improving patients scored after PA at 2.3 (directly before PA with 3.7), whereas patients improving only slightly scored after PA at 3.0 (directly before PA with 3.8). It is noteworthy that maximal body disorientation (concerning orientation of trunk, head, and eye direction) was set to a score of 6, whereas normal body orientation was set to a score of 0. Actually, none of the patients reached a score of 0 at t3, excluding floor effects.
Figure 4 shows the lesion localization for the patients who strongly profited from PA with respect to body orientation and of those patients who showed limited or no profit. Patients who profited from PA tended to have more frontally and subcortically located infarcts, whereas those with minimal or no profit from PA tended to have more middle occipito-temporally, middle temporally, and posterior parietally located lesions.
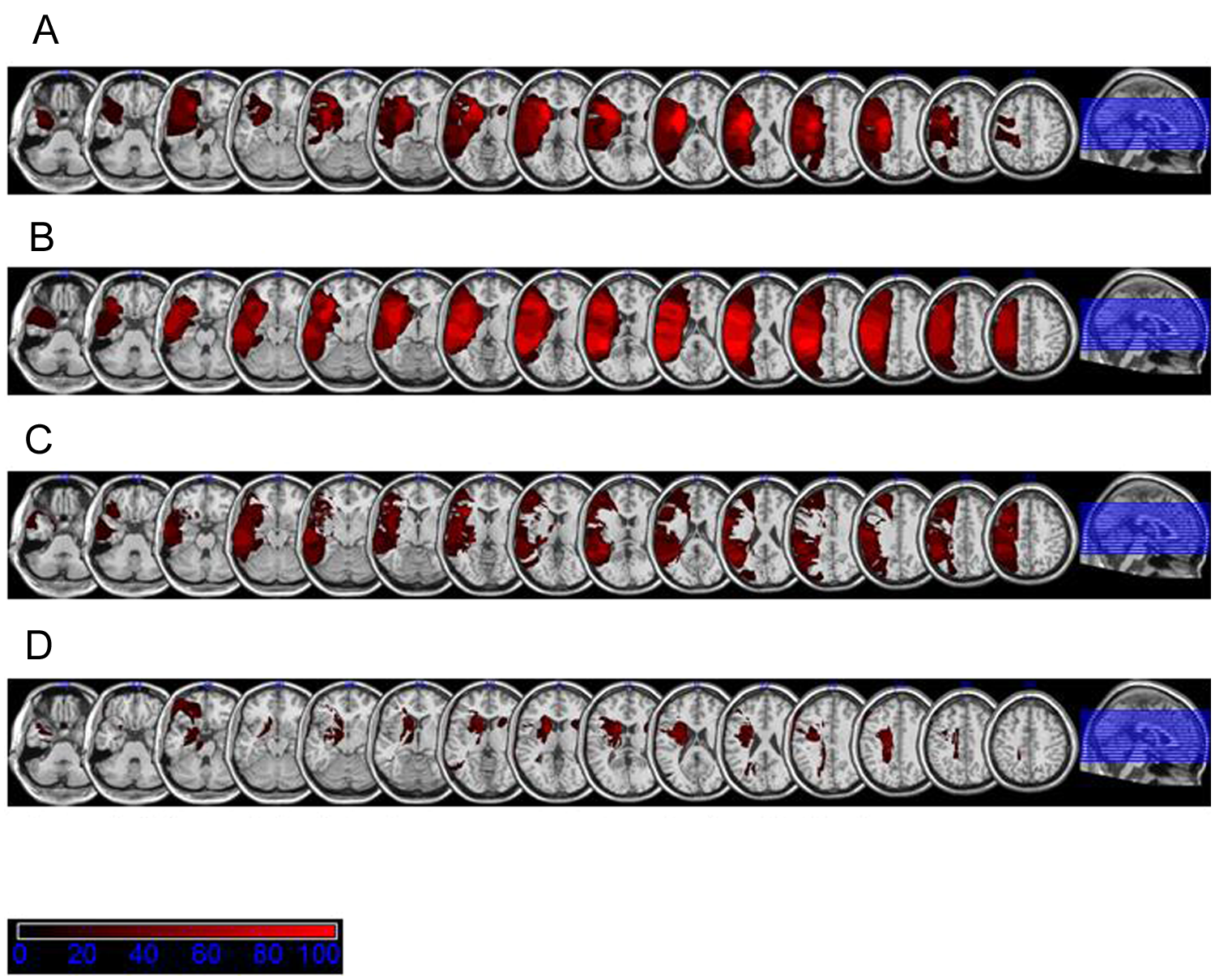
Localization of lesion according to improvement after prism adaptation (PA). (A) Overlap of lesions for patients with strong effect of PA. (B) Overlap of lesions for patients with small or no effect of PA. (C) Subtraction of (A) from (B). (D) Subtraction of (B) from (A).
Discussion
The present study shows that a short intervention with PA is effective in improving ego-centered neglect in patients with severe unilateral neglect in the postacute phase. This improvement persisted for at least 1 week. In contrast to previous studies, which showed short-term but no long-term effects in the acute phase or no effect at all in severely impaired patients,8,11 our results indicate that PA is a valuable treatment option also for patients in the early rehabilitation period.
The positive effects of PA only applied to the ego- centered aspects of neglect, whereas allocentric neglect was not affected by PA. This was evident in all tasks used to measure allocentric neglect in the current study. As an interesting auxiliary finding, allocentric neglect seemed to increase (albeit nonsignificantly) in parallel to the decrease of ego-centered neglect in the apples cancellation test. As far as we know, this is the first study on the effect of PA on allocentric neglect compared with ego-centered neglect. However, some previous studies21,22 yielded similar results in comparing the short-term experimental effects of PA on chimerical faces and objects, arguing that performance in such tasks cannot be improved by wearing prism glasses (for a discussion of this topic see Newport and Schenk 14 ).
One alternative interpretation of our results is that the assessments of ego-centered neglect were more sensitive than the assessments of allocentric neglect. In that case a comparatively small impact of PA would only show improvements in sensitive tests, mimicking a dissociated effect on ego-centered versus allocentric neglect. While this explanation cannot be excluded entirely, the significant differences in line bisection indicate that this test was sensitive enough to detect even small improvements. Moreover, the apples test documented increases of positive cancellations of items with left-sided but not with right-sided gaps. This strongly supports the notion that allocentric neglect was not positively influenced by PA and therefore the dissociated results are not just a consequence of different test loads.
The main models to explain the effect of PA on neglect rehabilitation argue for a bottom-up mechanism, which processes information of a systematic mismatch between motor coordinates and visual coordinates of space representation to the cortex and leads to short- and long-term recalibration of both these levels of spatial representation.14,23 This recalibration endorses a partial compensation of neglect. A more refined model argues for a role of the colliculi superior in neglect recovery through PA, because of the matching spatial position between visual, acoustic, and body position senses in the different layers of the superior colliculi. 24 Irrespective of the physiological basis for the positive effect of PA on neglect recovery, it has been postulated 14 that primarily the dorsal pathway of visual information processing is involved, and not the ventral pathway. This hypothesis is supported by our findings in comparing the lesion localization of patients with high and low profit from PA. Figure 4A-D shows that the parietal cortex and the posterior temporal cortex were spared in patients with high profit. In these latter patients the center of the lesion was in the medial frontal white matter and the basal ganglia. In patients highly profiting from PA, the dorsal pathway seems to be intact, whereas in patients with low profit, this pathway appears to be damaged. In a recent study, the improvement of neglect by PA was related to frontal lesions sparing the right temporal lobe. 25 Our results add to these findings that lesions in a parieto-temporal-frontal cortical network (affecting the “dorsal pathway”) seem to limit the effect of PA, whereas neglect caused by subcortical frontal lesions seems to respond positively to PA. Unfortunately, Chen et al 25 did not distinguish between frontal cortical and subcortical lesions (actually their nonfrontal group shows subcortical frontal lesions, eg, in the corona radiate, dorsal putamen, and caudate nucleus; see their Figure 3B), and therefore it is not possible to compare their results with ours in this respect.
On the neuroanatomic basis of ego-centered and allocentric neglect, some authors26-29 recently argued that allocentric neglect seems to be associated with lesions in inferior occipito-temporal areas, middle temporal, and in more postcentral parietal areas (angular gyrus). In this respect, it seems to be plausible that a pure visuospatial shift toward the right does not affect the representation of objects, as allocentric neglect does not covary with motor coordinates. In general, PA affects visuomotor recovery more than visuoperceptual recovery, 14 which is in good agreement with our results. Actually, the subtraction image of patients with small improvements in PA compared with those with high improvements (Figure 4C) seems to indicate that patients with small improvements have a more posteriorly localized lesion (in middle occipito-temporal, middle temporal, and parietal areas) than patients with high profit. Another more structural explanation for the smaller improvement of this patient group might be that having a lesion in postcentral areas, that is, in regions that are related to allocentric neglect, restricts the efficacy of PA. On the other hand, the finding that ego-centered neglect but not allocentric neglect can be treated with PA endorses the postulated dissociation between these different kinds of impairment. Allocentric measures of neglect therefore should be integrated into further treatment studies since currently no neglect treatment is able to reduce this component of neglect. 2 A relevant question of future research could be whether other bottom-up add-on treatments such as neck vibration, optokinetic stimulation, and vestibular stimulation are also restricted to ego-centered aspects of neglect rehabilitation.
The effect of our intervention on ego-centered neglect was clearly limited. We neither improved the ability of self-care (the increase of the ERBI concerned the comparison of T2 and T4, not the comparison of T2 and T3) nor reading as 2 major clinical endpoints for stroke rehabilitation. The patients still missed about two thirds of the critical targets in the apple-cancellation test. Improvements in body rotation were found only after cueing by asking questions from the left side of the patient and not for the spontaneous positioning. The reason for this limited effect might be the very short treatment schedule with only 4 sessions of PA. It is also possible that the add-on effect on neglect rehabilitation of procedures in such severely impaired patients as in our study does not exceed a specific threshold and that further improvements can only be reached by extended training schedules, a question that should be dealt with in future research. On the other hand, the raw score values of spontaneous body orientation also pointed in the direction of improvement. Thus, only reading did not show the expected result. For assessing the ability to read, we presented 4 stories encompassing 7 lines and counted omissions and errors. This might have influenced our results, because improvement in ego-centered neglect (starting more on the left) may have been accompanied by more errors in allocentric neglect (omitting or confusing characters from the left side of a word) as the performance in the apples test would suggest (Figure 3).
Further limitations of this study include the relatively small number of patients and a missing control group. However, the lack of a control group was partially overcome by using 2 measure points before starting the actual treatment to exclude spontaneous remission as an explanation for our results.
Also it should be mentioned that the effect of our treatment may be due to one of the components of our treatment (PA and restricted lateral right visual field by eye patching or repetitive visuomotor grasping) or its combination. From a therapeutic viewpoint, it should be emphasized that lesion volume did not differ between the 2 groups with high and with low improvement after PA. Although this might be due to the small number of included patients, it also shows that even severely impaired patients can be treated at least in some respects.
In summary, treatment with PA is effective even in severely impaired patients and should be used to speed-up neglect rehabilitation in postacute early rehabilitation of stroke patients, but its impact might be restricted to ego-centered neglect and not valid for allocentric neglect.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.