
Abstract
Background and objective. Previous studies suggest that error augmentation may be used as a strategy to achieve longer-term changes in gait deficits after stroke. The purpose of this study was to determine whether longer-term improvements in step length asymmetry could be achieved with repeated split-belt treadmill walking practice using an error augmentation strategy. Methods. 13 persons with chronic stroke (>6 months) participated in testing: (1) prior to 12 sessions of split-belt treadmill training, (2) after the training, and (3) in follow-up testing at 1 and 3 months. Step length asymmetry was the target of training, so belt speeds were set to augment step length asymmetry such that aftereffects resulted in reduced step length asymmetry during overground walking practice. Each individual was classified as a “responder” or “nonresponder” based on whether their reduction in step length asymmetry exceeded day-to-day variability. Results. For the group and for the responders (7 individuals), step length asymmetry improved from baseline to posttesting (P < .05) through an increased step length on both legs but a relatively larger change on the shorter step side (P < .05). Other parameters that were not targeted (eg, stance time asymmetry) did not change over the intervention. Conclusions. This study demonstrates that short-term adaptations can be capitalized on through repetitive practice and can lead to longer-term improvements in gait deficits poststroke. The error augmentation strategy, which promotes stride-by-stride adjustment to reduce asymmetry and results in improved asymmetry during overground walking practice, appears to be critical for obtaining the improvements observed.
Keywords
Introduction
Stroke is a leading cause of disability in the United States, 1 and one of the primary concerns for patients who experience stroke is the ability to regain walking function. 2 Consequently, significant effort is focused on gait retraining during rehabilitation following a stroke, 3 and efforts to develop and improve locomotor retraining programs are a major focus of rehabilitation research. Despite these efforts, many individuals with stroke continue to have residual gait deficits4-9 and never achieve community ambulation status.10,11 Spatiotemporal gait asymmetries are prevalent after stroke and are related to slow walking speed,7,12-14 which is related to reduced participation. 15 In addition, step length asymmetry has consequences relative to other gait deviations. Specifically, a shorter nonparetic step is related to a decreased propulsive force on the paretic leg, 12 which limits forward propulsion of the body and is related to slow gait speed. 4 Thus, recent poststroke gait retraining interventions have targeted step length asymmetry to promote greater recovery of walking.14,16
Many novel rehabilitation interventions for those with stroke have emerged in the past several years.16-18 A recent group of studies utilizing motor adaptation, a form of error-driven motor learning, applied to walking have gained interest in the rehabilitation community because of their unique ability to target specific gait deviations.19-24 Motor adaptation through a split-belt walking paradigm can lead to short-term (ie, within-day) improvements in step length asymmetry in people with chronic stroke.21,22 To see these improvements, a person’s step length asymmetry must be exaggerated while walking on the split-belt treadmill. That is, their error (asymmetry) must be augmented during walking to drive the nervous system to make corrections. For example, a person with stroke who takes a longer step with the paretic leg (short nonparetic step) during regular walking would walk on the split-belt treadmill with the paretic leg on the slow belt. Initially, this will cause the person to take an even longer step with the paretic leg and an even shorter step with the nonparetic leg. However, over time (<15 minutes), through practice, they will correct this by lengthening the nonparetic step and shortening the paretic step. After split-belt walking, when the belts are returned to the same speed, the stroke survivor will continue the adjusted pattern, resulting in step length symmetry.21,22 In contrast to step length, percentage stance time does not adapt during split-belt walking. Rather, the leg on the slow belt immediately adopts a longer stance time, and the leg on the fast belt adopts a shorter stance time, and these times do not change over the period of split-belt walking. Once the belts are returned to the same speed, percentage stance time immediately returns to its normal duration.21,22,25
The improvements in step length asymmetry observed after split-belt walking are found whether the person walks on the treadmill with the belts going at the same speed or over ground. 22 Thus, the improvements transfer to natural situations off of the treadmill. That being said, the improvements in step length asymmetry are short-lived, and the person with stroke returns to their baseline asymmetry after several minutes of overground or treadmill walking. Not surprisingly, this suggests that 1 session of this type of training is not enough to produce long-term changes. Similar effects have been observed in reaching movements of chronic stroke survivors—they show short-term improvements in reaching errors following an error augmentation paradigm that is carried out through a robot manipulandum during reaching practice. 26
The results from studies of split-belt treadmill walking and reaching with a robot have caused investigators to hypothesize that error augmentation can be used as a strategy to achieve longer-term changes in movement abnormalities after stroke. 27 A recent case report showed that 12 sessions of split-belt treadmill training using an error augmentation strategy led to improvements in step length asymmetry, but not stance time asymmetry, in a single chronic stroke survivor. 28 The purpose of this study was to expand on those results in a larger group of chronic stroke survivors to determine whether longer-term improvements in step length asymmetry could be achieved with repeated split-belt treadmill walking practice using an error augmentation strategy. A secondary purpose of the study was to determine if there were differences between individuals in their response to the training. If longer-term improvements in step length asymmetry are observed, this would suggest that error augmentation may be a strategy that can be used to target specific gait deviations during rehabilitation after stroke.
Methods
Participants
Individuals who had sustained a single, unilateral stroke more than 6 months prior to the study were eligible to participate either at the Johns Hopkins School of Medicine/Kennedy Krieger Institute or at the University of Delaware. All participants gave their informed consent prior to participating, and a human subjects committee approved the study. Individuals were excluded if they had other neurological conditions, orthopedic conditions affecting the legs or back, uncontrolled hypertension, pacemaker or automatic defibrillator, active cancer, and radiological and/or physical examination evidence of damage to the cerebellum or were unable to complete the walking task. Participants were also excluded if they did not have at least a 5-cm step length asymmetry as measured during overground walking. This was determined from data gathered from self-selected walking speed trials over an electronic walkway (GAITRite, CIR Systems, Havertown, PA, at the Kennedy Krieger Institute and GaitMat II, EQ, Inc, Chalfont, PA, at the University of Delaware). Those who customarily wore an ankle-foot orthosis were allowed to wear it throughout the study. Those who used an assistive device such as a cane or walker were allowed to use it during all overground walking.
Testing
All individuals participated in double baseline testing, with each session approximately 1 week apart, prior to 4 weeks of split-belt treadmill training. They completed a postintervention testing session and follow-up testing at 1 and 3 months following the completion of the intervention. Each testing session comprised computerized measurement of overground walking and several clinical tests of movement and walking function.
Gait analysis
All gait data were collected during overground walking using 1 of 3 data collection systems. Whichever system was used to test an individual at baseline was used for all subsequent testing. For the first 3 individuals, gait data were measured through computerized gait analysis using OPTOTRAK (Northern Digital, Waterloo, ON, Canada) sensors that recorded 3-dimensional position data at 100 Hz from both sides of the body using methodology described previously. 22 It was quickly determined that the subject burden associated with these data collections was not necessary for the gait parameters targeted for this study, and all subsequent data were collected via an electronic walkway. All participants completed 7 to 10 walking trials at both their self-selected and at their fastest possible speed. Rest breaks were allowed as needed. For the 3 individuals whose data were collected through motion capture, step length was calculated as the anterior-posterior distance between the feet at the time when each foot contacted the ground, as determined by footswitches placed on the heel. Step length was labeled paretic or nonparetic based on the leading leg. The percentage time in double-limb support was the time that both feet were in contact with the floor, expressed as a percentage of the stride time for each leg. The stance time (the time from foot contact to liftoff) was also expressed as a percentage of the stride time.
Functional testing
All participants underwent a clinical examination, including measurement of lower-extremity performance on the Fugl-Meyer test, cutaneous pressure sensitivity and proprioception, and self-selected and fast walking speed. Walking speed was measured as the average of 3 trials along a 10-m walkway at both the self-selected and fastest speeds. 29 Pressure sensitivity of the great toe was tested using graded monofilaments. The lowest gram filament that could correctly be detected on 4/5 trials was recorded. 22 Proprioception was tested at the great toe, ankle, knee, and hip by moving the joint approximately 10° and asking the individual to determine the direction of movement. The number of correct responses out of 5 trials was recorded, and the percentage of trials correct at the great toe was used for subsequent analysis. 22
Training
Participants trained 3 d/wk for 4 weeks. Each session lasted approximately 1 hour, including a warm-up on the treadmill and rest periods between bouts. The training was designed so the participants would walk on the split-belt treadmill in six 5-minute bouts, for a total of 30 minutes of split-belt treadmill walking each day. During each training block, heart rate and the rating of perceived exertion (RPE) 30 were recorded at 2 and 4 minutes during treadmill walking and before and after overground walking. If RPE exceeded 15 or heart rate exceeded 80% of age-predicted heart rate maximum, the participant was given a rest break. During the rest period, heart rate and blood pressure were monitored.
To assess the perceived difficulty of each training session, the average RPE during both the treadmill and overground walking was calculated for each training session. Changes in perceived exertion over training sessions was calculated as the difference in average perceived exertion between session 1 and session 11 for both treadmill and overground walking. Thus, positive values represent reduced perceived exertion from the beginning to end of the training, whereas negative values represent increased exertion.
The leg-belt speed configuration during split-belt walking was chosen so that the participant’s baseline step length asymmetry would be exaggerated by the split-belts. The speed of the fast belt was chosen to be as close as possible to the participant’s fast overground walking speed, and the slow belt speed was half of the fast belt speed. Because the goal of the training was to determine if repeated exposure to split-belt treadmill walking could improve step length asymmetry and not necessarily to improve walking speed or endurance, the belt speeds were not increased during the training period.
During all treadmill walking, participants wore a ceiling-mounted harness for safety. The harness did not support body weight or interfere with the participant’s walking. Participants were allowed to use the front handrail of the treadmill for safety but were encouraged not to use this support. Each day, following completion of all treadmill walking bouts, the participant practiced walking overground for approximately 5 to 10 minutes, with verbal cueing from the physical therapist to reinforce the improved step length asymmetry.
Data Analysis
Step length asymmetry during self-selected speed for overground walking was the primary outcome of interest and was calculated as the normalized step length difference 31 :
where SLparetic and SLnonparetic refer to paretic and nonparetic step lengths, respectively. Larger values mean more asymmetry, and a value of 0 indicates symmetry, regardless of the direction of the asymmetry. Normalization was done so participants who took different-sized steps could be compared. Stance and double-support time asymmetry were calculated as the ratio of paretic leg to nonparetic leg stance or double-support time.21,22
Because of the small sample size, nonparametric statistics were used. The Wilcoxon matched-pair signed-rank test was used to examine differences between the first baseline and posttesting session and between baseline and each follow-up test.
We classified each individual as a “responder” or a “nonresponder” via changes in step length asymmetry after training. First, the difference in step length asymmetry between the 2 baseline testing sessions was calculated for each individual and then averaged across individuals. Then, each person’s change in step length asymmetry from baseline to posttesting was calculated. If the individual’s change exceeded the average baseline day-to-day difference, he or she was considered a responder. To understand whether there were specific characteristics that could be used to identify those who were classified as responders, we examined differences in age and time since stroke, differences in the baseline measures of the lower-extremity Fugl-Meyer, step length asymmetry, walking speed, sensation, and proprioception between the group of responders and nonresponders. We also examined whether perceived exertion during overground walking was different between the 2 groups. These differences between responders and nonresponders were examined with the Mann-Whitney U test. Relationships between changes in step length asymmetry and other parameters were examined using Spearman’s rank correlation.
Results
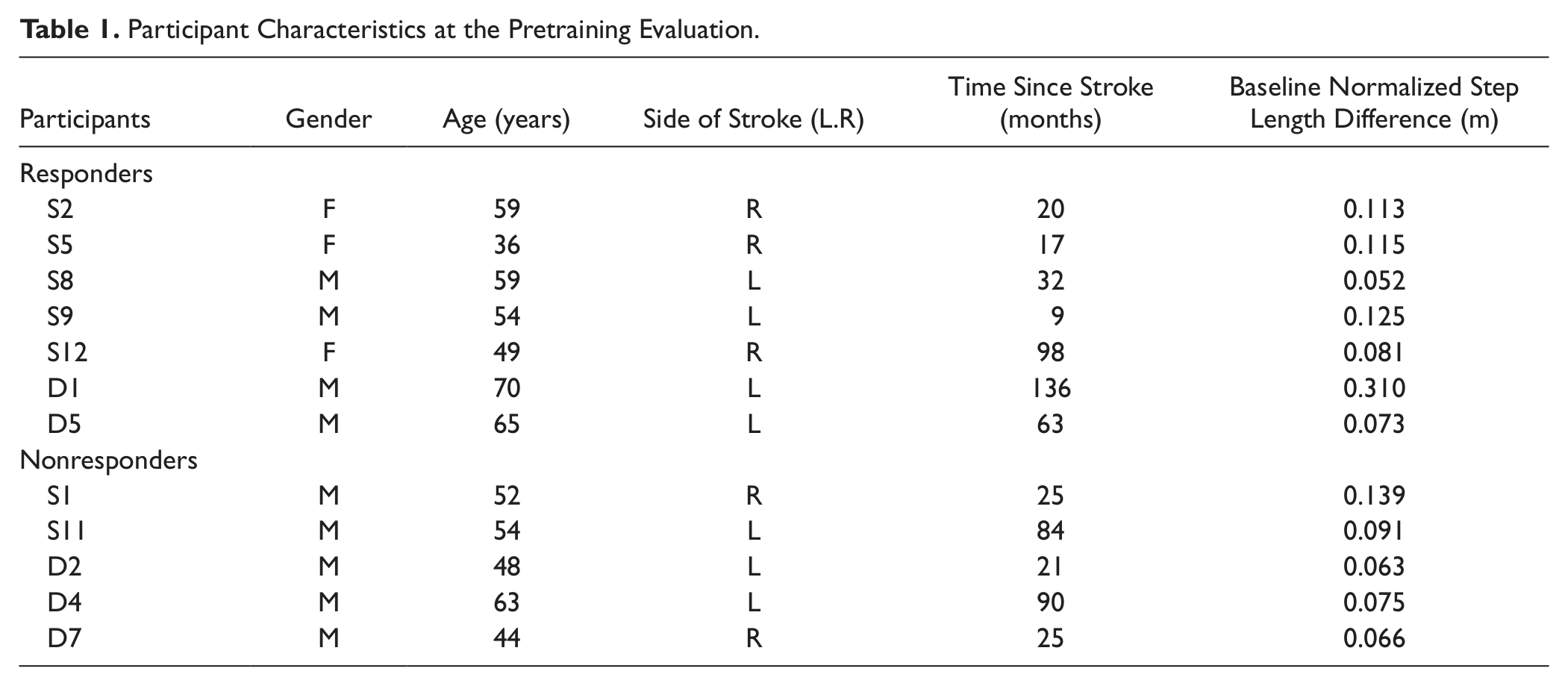
In all, 13 participants were enrolled in the study. Data are presented from 12 because walking data from 1 participant could not be reliably calculated because of foot scuffing during walking. Two participants did not complete the 3-month evaluation—1 person had a new diagnosis of cancer after the 1-month evaluation and 1 was unavailable. Gait data from 1 participant at the 1-month follow-up were unavailable because of equipment malfunction. Participant demographic data can be found in Table 1. The pattern of step length asymmetry was consistent across the group; for 11 of the 12 participants, their step length was longer on the paretic side compared with the nonparetic side.
Participant Characteristics at the Pretraining Evaluation.
Across the entire group of participants, step length asymmetry improved from baseline testing to posttesting (Figure 1A; P < .05). The difference between baseline and the 1- and 3-month follow-up testing approached significance, suggesting that the effects are reasonably durable (Figure 1; P = .062 and P = .059, respectively). The change in step length asymmetry occurred as a result of an increased step length on both legs but a relatively larger change on the side with the shorter step (Figure 1B; P < .05 for all).
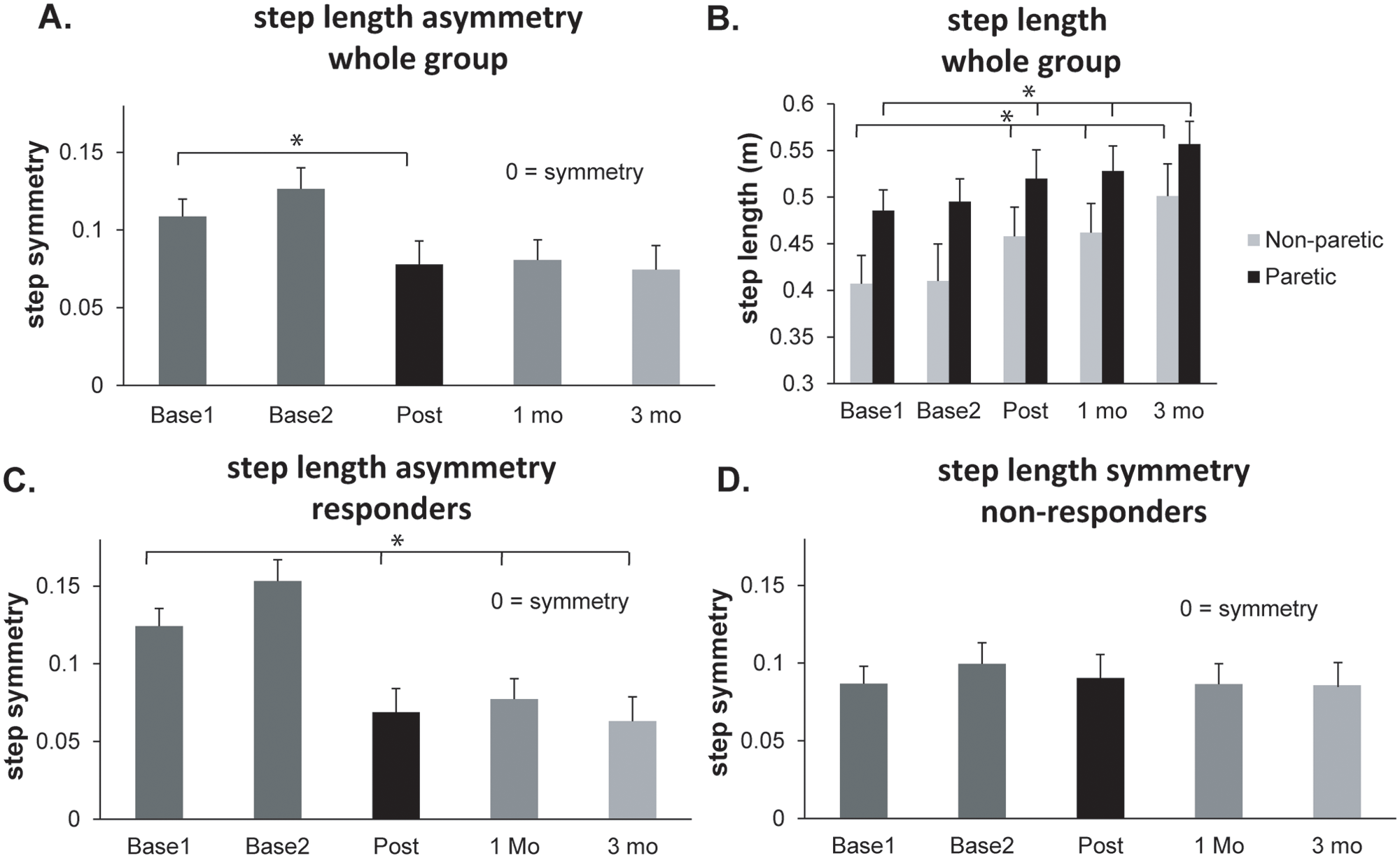
Step length during overground walking measured at each baseline session (Base1, Base2) at posttraining (Post) and at 1 and 3 months (mo) after training: A. Step length asymmetry for the entire group (n = 12). B. step length in meters for the nonparetic (gray bars) and paretic (black bars) leg for the entire group (n = 12). C. step length asymmetry in the group identified as responders based on their pretraining to posttraining change in asymmetry (n = 7). D. step length asymmetry in the group identified as nonresponders based on their pretraining to posttraining change in asymmetry (n = 5)a
The average difference in step length asymmetry between the 2 baseline testing sessions was 0.020. Therefore, to be considered a responder to the intervention, a participant’s change in step length asymmetry from baseline to posttesting needed to exceed 0.020. Based on these criteria, 7 participants’ change in step length asymmetry exceeded this value (responders, indicated in Table 1) and 5 participants’ change did not (nonresponders). Participants in the responder group showed significant improvements in step length asymmetry between the baseline testing session and all other testing points (Figure 1C; P < .05 for all). The participants in the nonresponder group did not show differences between baseline and any other testing session (Figure 1D; P > .05).
Step length asymmetry was targeted by the training, but we also evaluated percentage stance and percentage double-support-time asymmetry. Neither parameter changed from baseline to any of the other testing sessions (Figure 2; P > .05 for all). Self-selected overground walking speed also did not change from baseline to any of the other testing sessions, and this did not differ between the group of responders and nonresponders (P > .05 for all). For example, self-selected overground walking speed at baseline was 0.71 ± 0.21 m/s for the entire group, 0.68 ± 0.23 m/s for the responders, and 0.75 ± 0.20 m/s for the nonresponders. At the end of 4 weeks of training, it was 0.75 ± 0.20, 0.68 ± 0.22, and 0.85 ± 0.20 m/s for these groups, respectively. Finally, cadence decreased for the responders from 98 steps/min at baseline to 89 steps/min at the end of training; this may explain why their walking speed did not change despite their increased step lengths. In the nonresponders, cadence was 91 steps/min at baseline and 95 steps/min at the end of training.
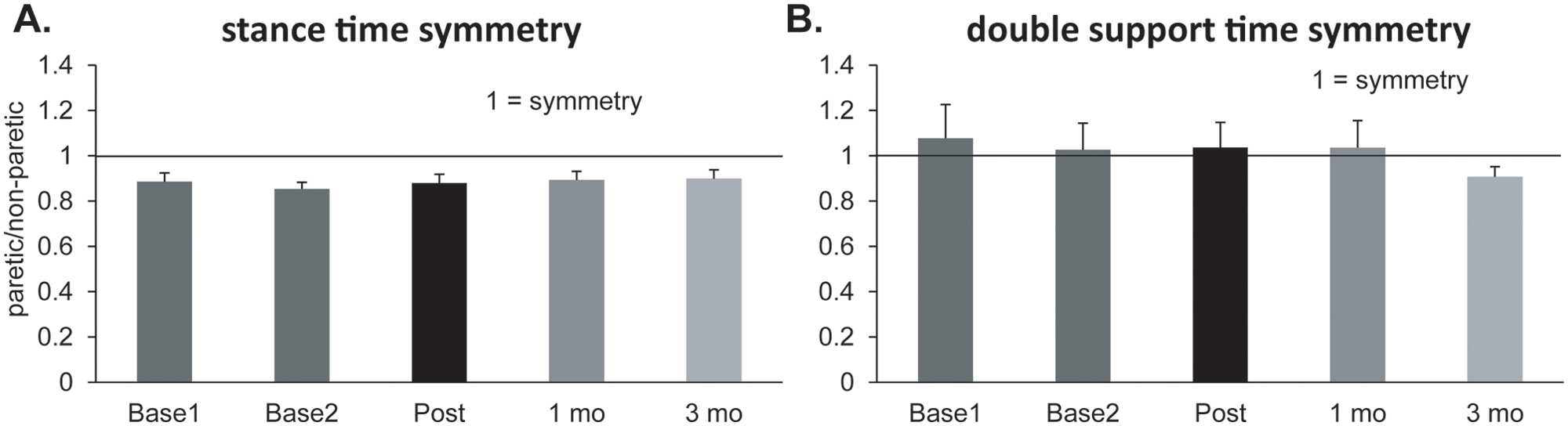
Stance and double-support-time asymmetry during overground walking measured at each baseline session (Base1, Base2), at posttraining (Post) and at 1 and 3 months (mo) after training: A. Percentage stance time asymmetry for the entire group (n = 12). B. Percentage double-support-time asymmetry for the entire group (n = 12)
There were no differences in the baseline lower-extremity Fugl-Meyer, step length asymmetry, walking speed, sensation, or proprioception between the group of responders and nonresponders (P > .05 for all). The only difference between the group of responders and nonresponders was in perceived exertion. The responders had higher perceived exertion scores during overground walking on the first day of training and showed a greater change in perceived exertion during overground walking from the beginning to the end of the training intervention compared with the nonresponders (P < .05, P < .01, respectively; Table 2). Perceived exertion scores during overground walking on the first day of training and the change in perceived exertion from the beginning to the end of the training intervention were highly correlated with the change in step length asymmetry across the entire group (Figure 3; P < .05 and P < .001, respectively). In other words, those who initially felt it was hardest to walk overground and subsequently showed the greatest reduction in perceived exertion after training responded the best in terms of improvements in step length asymmetry.
Differences Between Responder and Nonresponder Groups. a
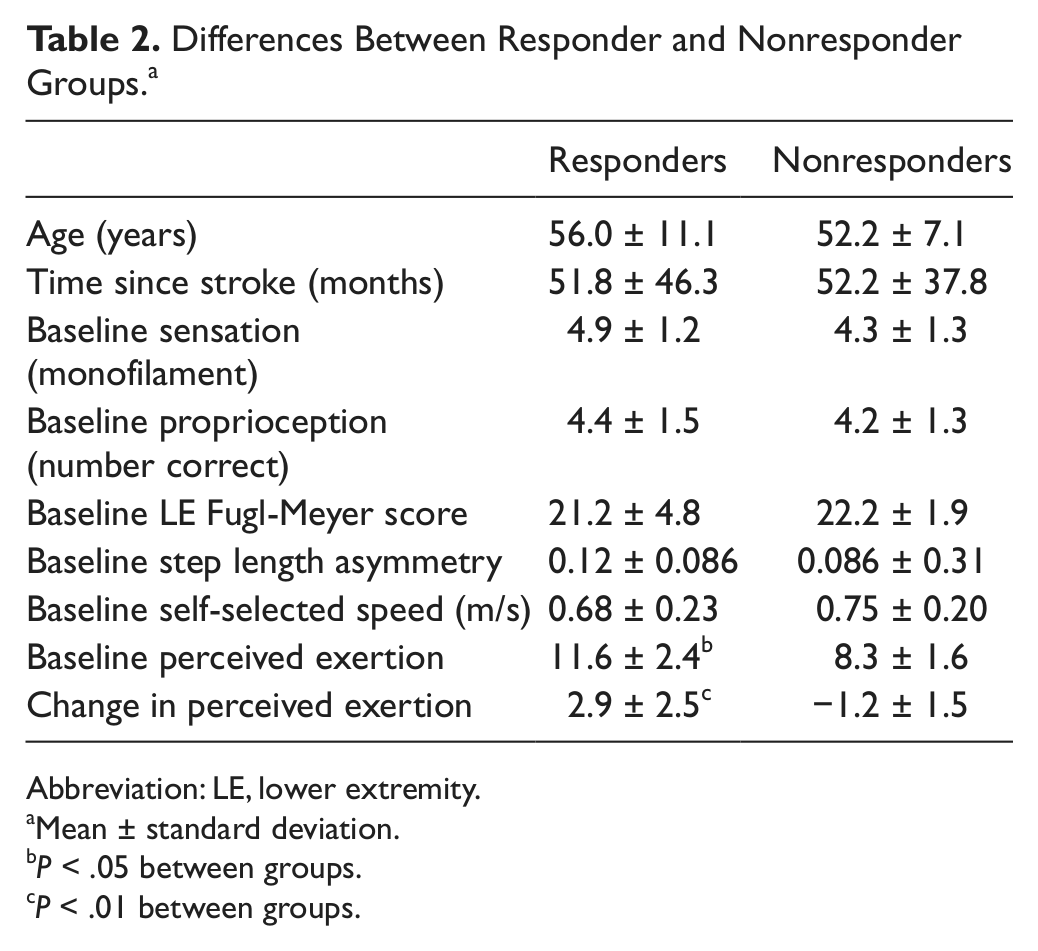
Abbreviation: LE, lower extremity.
Mean ± standard deviation.
P < .05 between groups.
P < .01 between groups.
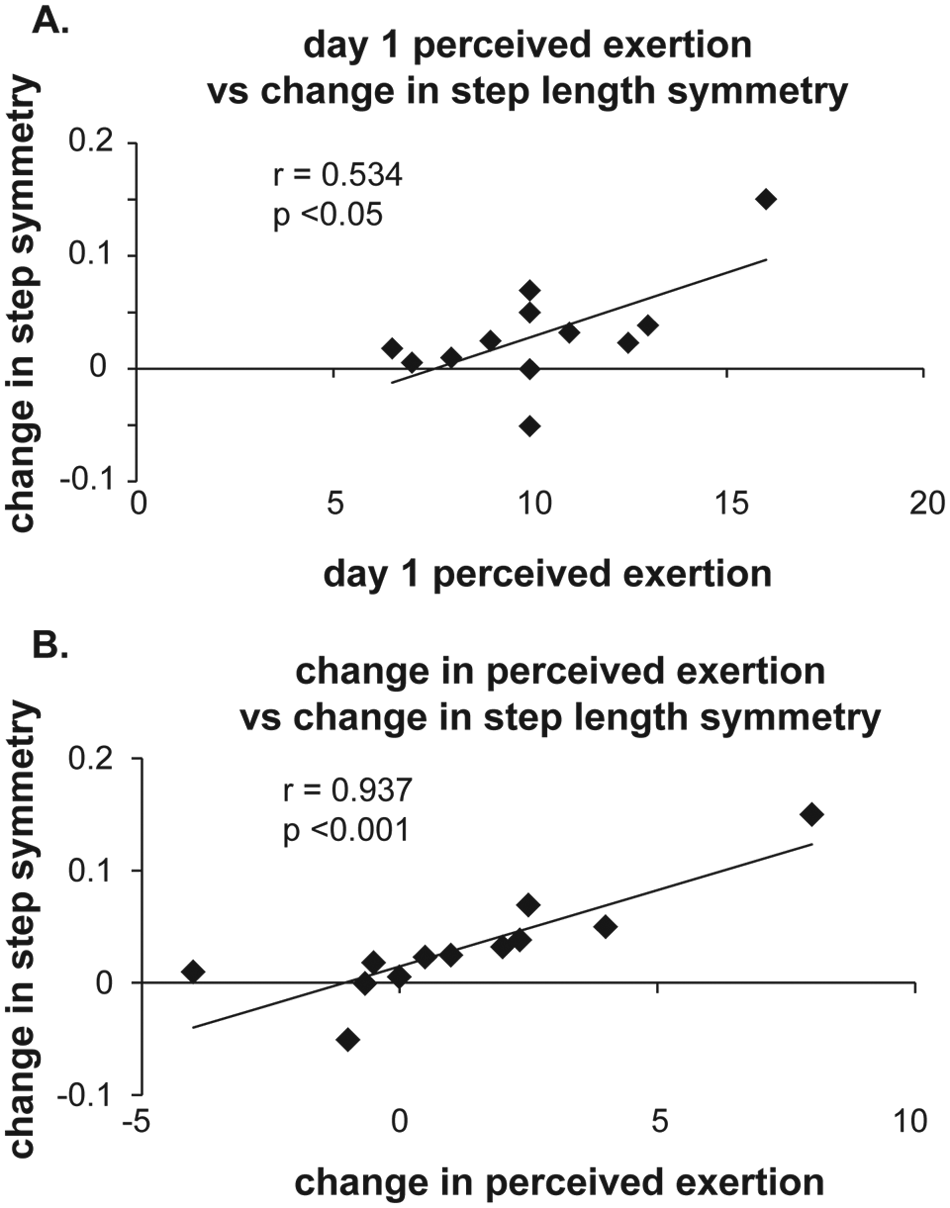
The relationship between perceived exertion and change in step length asymmetry: A. Perceived exertion during overground walking on the first day of training versus the change in step length asymmetry from the beginning to end of training. B. Change in perceived exertion during overground walking from beginning to end of training versus the change in step length asymmetry from the beginning to end of training. Each symbol represents data from 1 individual
Discussion
Since the early reports of short-term improvements in poststroke movement deficits using an error augmentation strategy,21,22,26 it has been questioned whether such a strategy could be used to improve movement deficits over the longer term. 27 This is the first study, to our knowledge, to demonstrate that repetitive practice with error augmentation can result in longer-term improvements in a targeted movement deficit after stroke. Although not statistically significant, the results support a trend for the improvements to be maintained at both 1 and 3 months after the end of training.
Studies of both reaching and walking have shown that persons with chronic stroke retain the ability to adapt their movement patterns to an external perturbation and temporarily store these new movements (evidenced by aftereffects).21,22,26 Moreover, if the perturbation exaggerates the stroke survivor’s movement errors, the aftereffects result in temporary improvement in the movement, demonstrating that the compromised nervous system is still capable of producing a more normal movement pattern.21,22,26 This also allows the individual to experience the “correct” movement pattern and practice using it.
How would practice of walking with improved step length asymmetry over the short term result in longer-term improvements in asymmetry? A recent study demonstrated that after a person undergoes error-driven adaptation, they engage an additional learning system that reinforces the newly adapted pattern. 32 They specifically showed that reinforcement-based learning mechanisms are activated and responsible for retention of the adapted pattern from 1 training session to the next. This finding may explain why we saw repeated adaptation experiences resulting in learning of a new pattern. We reinforced the adapted pattern right after each split-belt treadmill session through verbal feedback and cueing from a physical therapist during a 5- to 10-minute overground walking session. Thus, it is possible that the combination of split-belt treadmill training and reinforcement of the adapted pattern led to the long-term changes that we observed.
It is interesting that only the aspects of walking that we targeted and specifically adapted changed over the long term. Step length asymmetry changed, whereas other parameters, such as percentage stance time, did not. This was the case despite the fact that for 11 out of 12 participants, the paretic leg was on the slow belt and spent considerably more time in stance compared with the leg on the fast belt (~70% vs 55%, respectively).21,22,25,33 Why did this additional practice in stance on the paretic leg not lead to long-term changes? One possibility is that the stride-by-stride step length adaptation was an essential part of the process in producing the long-term change. We have shown repeatedly that stance time does not adapt during split-belt walking and is not stored as an aftereffect.21,22,25,33 It is instead immediately changed using feedback mechanisms to be appropriate for either split-belt walking or normal treadmill or overground walking and, thus, does not undergo error-driven change. Thus, the effect of split-belt walking on stance time is that participants repeatedly produce the same pattern of stance time, without stride-by-stride adjustment. Previous studies have shown that simple performance of a pattern does not appear to be sufficient to change the pattern over the longer term. Studies in both animals and humans indicate that changes in, for example, corticospinal excitability or motor maps occur only with practice of skilled movement and not with mere use.34-36 It is interesting to note that a recent case report in a person with chronic stroke found that feedback targeted at step length asymmetry led to stride-by-stride adjustment of step length and changes in step length asymmetry. Stance asymmetry was unchanged, despite increased time spent in stance on the paretic leg during the training. 14 Taken together, these results suggest that it may be that stride-by-stride adjustment based on feedback, and not mere use, is required to see longer-term, more permanent changes in motor behavior after stroke.
Another critical component of the split-belt training was that the participants’ step length asymmetry was exaggerated with the split-belt treadmill, thereby augmenting their “error” (asymmetry) during split-belt walking. This error augmentation may provide a stronger drive to the nervous system to correct the asymmetry21,22 and suggests an interesting and important concept for rehabilitation: movement error augmentation prompts the nervous system to make a movement correction. This “prompt” could be especially necessary for persons with chronic movement deviations, where the deviation may no longer be perceived by the nervous system as a movement error that requires correction. 20 The results of this study suggest that for chronic stroke survivors with long-standing movement asymmetries, it may be useful to enhance error and allow the patient to correct the movement, thereby facilitating practice and motor learning.
From a functional perspective, it is important that the improvements in step length asymmetry in this study were achieved by an increase in step length on both legs but a relatively greater increase on the leg with the shorter step. This is significant because an improvement in asymmetry could also be achieved by a decrease in step length on the side with the longer step. That type of change in asymmetry would not be as functionally desirable, given that increased step length has been associated with increased walking speed following a walking program in persons poststroke. 37
As a group, there were significant changes in step length asymmetry following the split-belt treadmill training; however, not every participant showed improvements in asymmetry that exceeded day-to-day variability in the measure. Similarly, in a study of neurologically intact individuals learning a simulated pinball game using either an error augmentation strategy or a haptic guidance strategy, only some individuals learned better with error augmentation. 38 In the present study, we examined a number of variables to understand why some participants appeared to learn more with the error augmentation strategy than others. There were no baseline demographic, clinical, or gait characteristics that differed between the groups. What did differ, however, was the participant’s perceived exertion or effort during the overground walking portion of the training. Participants who had the highest perceived exertion scores on day 1 of training and had large changes in perceived exertion over the course of training also had the largest improvements in step length asymmetry, such that improvements in step length asymmetry were associated with a reduced perception of effort during walking. This may indicate that those participants who obtained a perceived benefit (in terms of effort) from walking more symmetrically more readily adopted the pattern over the longer term. Alternatively, it could be that for those who learned to walk more symmetrically, there was some efficiency benefit that reduced the effort of walking. It has been suggested that spatiotemporal asymmetry is a factor in the increased energy cost of walking after stroke, 9 and improvements in gait asymmetry are associated with reduced energy cost of walking in amputees. 39
It is possible that the improvements in step length asymmetry could simply be a result of the fact that the individuals participated in walking training and have nothing to do with the error augmentation strategy used. However, step length asymmetry has been shown to be relatively resistant to change with other treadmill and overground training interventions after stroke, with no improvements in this asymmetry observed following training.17,29,40 Moreover, step length asymmetry was the only spatiotemporal asymmetry that improved; stance and double-support-time asymmetry were unchanged. Finally, overground walking speed did not improve, suggesting that improvements in step length asymmetry were not simply a by-product of faster walking. 41 Thus, it seems unlikely that the walking training alone, without the error augmentation strategy, could account for the improvements observed in step length asymmetry. However, this study cannot rule out this possibility.
Conclusions
Previous single-session studies have suggested that rehabilitation interventions that use an error-augmentation strategy may be effective at targeting specific movement deficits after stroke.21,22,26 This is the first study demonstrating that the short-term adaptations observed in previous studies can be capitalized on through repetitive practice and can lead to longer-term improvements in gait deficits after stroke. The error augmentation strategy, which promotes stride-by-stride adjustment to reduce asymmetry and results in improved asymmetry during overground walking practice, appears critical for obtaining the improvements observed, as evidenced by the differing results for stance time and step length asymmetry. Future, larger studies are necessary to determine characteristics that moderate a person’s response to this intervention after stroke.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Health Shared Instrumentation Grant S10RR022396, the National Institute of Child Health & Human Development Grant K01HD050582, and the National Institute of Child Health & Human Development Grant R01HD048740.