
Abstract
Background. Gait impairments after stroke arise from dysfunction of one or several features of the walking pattern. Traditional rehabilitation practice focuses on improving one component at a time, which may leave certain features unaddressed or prolong rehabilitation time. Recent work shows that neurologically intact adults can learn multiple movement components simultaneously. Objective. To determine whether a dual-learning paradigm, incorporating 2 distinct motor tasks, can simultaneously improve 2 impaired components of the gait pattern in people posttroke. Methods. Twelve individuals with stroke participated. Participants completed 2 sessions during which they received visual feedback reflecting paretic knee flexion during walking. During the learning phase of the experiment, an unseen offset was applied to this feedback, promoting increased paretic knee flexion. During the first session, this task was performed while walking on a split-belt treadmill intended to improve step length asymmetry. During the second session, it was performed during tied-belt walking. Results. The dual-learning task simultaneously increased paretic knee flexion and decreased step length asymmetry in the majority of people post-stroke. Split-belt treadmill walking did not significantly interfere with joint-angle learning: participants had similar rates and magnitudes of joint-angle learning during both single and dual-learning conditions. Participants also had significant changes in the amount of paretic hip flexion in both single and dual-learning conditions. Conclusions. People with stroke can perform a dual-learning paradigm and change 2 clinically relevant gait impairments in a single session. Long-term studies are needed to determine if this strategy can be used to efficiently and permanently alter multiple gait impairments.
Introduction
Reduced walking function after stroke limits independence, increases long-term disability, and reduces quality of life.1-4 Impaired walking post-stroke often has many components rather than a single abnormality. Two common deficits in people with hemiparetic stroke are stiff-knee gait and step length asymmetry. Stiff-knee gait is characterized by decreased paretic-leg knee flexion during the swing phase of the gait cycle,5,6 and is particularly debilitating because it compromises foot clearance, which can decrease stability and increase the risk of falling. 7 To advance their paretic leg during walking, people with stiff-knee gait often develop compensatory movement patterns such as circumduction, vaulting, or pelvic tilt,8,9 which further increase energy expenditure and instability. 10 Many individuals post-stroke also demonstrate step length asymmetry where one leg advances further than the other leg. 11 Step length asymmetry is a significant predictor of walking performance because it strongly correlates with reduced walking speed, increased energy expenditure, decreased activity levels, and falls.11-13 Moreover, there is evidence that gait asymmetry persists, and may even worsen, long after the stroke event. 14
Recovery from these motor deficits requires motor learning, either for relearning premorbid movement patterns or learning compensatory strategies to overcome persistent deficits.15,16 Therefore, a number of novel rehabilitation interventions that leverage different forms of motor learning principles have been used to address motor impairments post-stroke. For instance, a form of motor learning called adaptation can alter step asymmetry in walking. Specifically, we and others have used a split-belt treadmill adaptation protocol, where separate treadmill belts drive the legs at different speeds during walking, to improve step length asymmetry after stroke. 17 In this case, a person’s baseline step length asymmetry is initially exaggerated by placing the leg that takes the shorter step on the faster treadmill belt. This mechanical perturbation provides a salient stimulus for people to recalibrate their walking pattern and reduce the exaggerated asymmetry. When the belts are returned to the same speeds after adaptation, the resulting motor aftereffect can leave people with more symmetrical step lengths. 17 Moreover, repeated split-belt treadmill training can lead to lasting improvements in step length asymmetry in people with stroke. 18
Providing real-time biofeedback during gait may be another useful strategy to improve motor performance in people post-stroke. 19 A number of studies have shown that instantaneous visual or auditory feedback of biological signals can lead to improved gait speed, spatiotemporal symmetry, stride length, stride width, genu recurvatum, and push-off force in people with stroke.20-23 Moreover, in a single stroke subject case study, performing a target-tracking task using real-time kinematic information (ie, paretic ankle trajectory) elicited lasting improvements in kinematic control and clinical measures of walking distance, walking speed, and balance. 24
These types of interventions have shown promise for improving walking, yet current neurorehabilitation techniques are often unable to restore prestroke gait. 25 One potential drawback of traditional rehabilitation practice is they often address a single deficit at a time. For instance, a therapist may work on increasing paretic knee flexion, and once that is accomplished move to interventions targeting step length asymmetry. Given that the current median length of stay in an inpatient rehabilitation facility is only 16 days, 26 this serial approach challenges therapists and patients to prioritize certain deficits, leaving some untreated. 27 A protocol that involves simultaneously confronting multiple faulty movement components may be a more efficient use of rehabilitation time and ultimately result in superior patient outcomes. Recent work demonstrated that neurologically intact adults can learn multiple components of the walking pattern simultaneously and without interference. 28 Specifically, participants learned to increase peak knee flexion using biofeedback while simultaneously adapting step length symmetry on a split-belt treadmill. This type of approach could prove useful for stroke rehabilitation to simultaneously improve multiple, distinct deficits of the walking pattern.
Here we aim to determine whether a dual-learning paradigm, incorporating 2 distinct motor learning tasks, can simultaneously improve paretic knee flexion and step length asymmetry in people post-stroke. We hypothesized that the dual-learning paradigm would lead to improvements in peak paretic knee flexion and step length asymmetry in people post-stroke.
Methods
Participants
Twelve adults with chronic stroke (8 male; 61.3 ± 8.3 years old) participated in this study. All participants met inclusion and exclusion criteria (Table 1). The study protocol was approved by the Johns Hopkins Medicine Institutional Review Board and was conducted in compliance with the Declaration of Helsinki. All participants provided written informed consent prior to beginning the study and were compensated for their time.
Inclusion and Exclusion Criteria a .
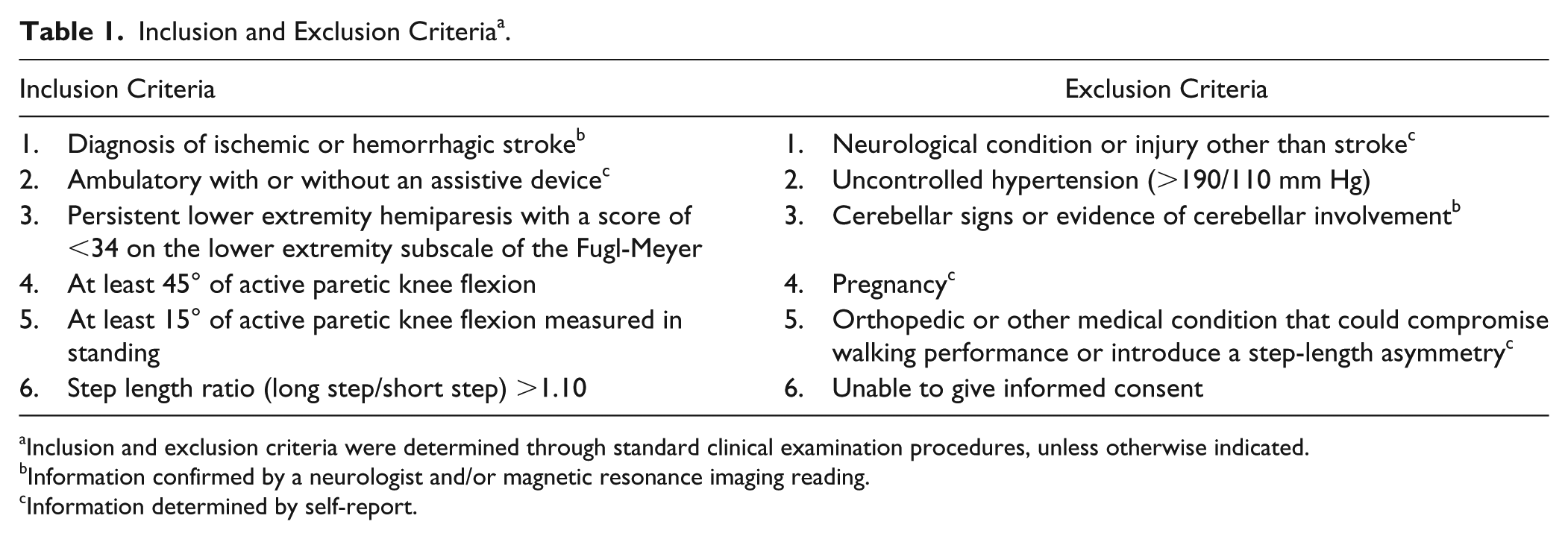
Inclusion and exclusion criteria were determined through standard clinical examination procedures, unless otherwise indicated.
Information confirmed by a neurologist and/or magnetic resonance imaging reading.
Information determined by self-report.
Clinical Assessment
Motor impairment was quantified using the lower extremity subscale of the Fugl-Meyer test (FM-LE). This test includes 17 items scored on an ordinal scale (0-2) with 34 possible points and higher scores representing less impairment. 29 Self-selected and fast over-ground walking speeds were measured by having participants walk 2 passes at each speed across a 6-meter electronic walkway (Zeno Walkway, ProtoKinetics, Havertown, PA). Baseline differences in step length were determined by the electronic walkway during the self-selected walking speed assessment. Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), 30 and participants who scored >26/30 possible points were considered to have normal cognitive function. Active and passive range of motion of lower extremity joints were measured using standard clinical procedures. For proprioception testing, participants were supine with their eyes closed. The examiner stabilized the proximal joint segment and passively moved the distal segment to a position above or below the neutral starting position (neutral position was midway through the joint’s range of motion). The participant reported whether the position of the specified joint was above or below the starting position. Paretic hip, knee, and ankle joints were each tested at 6 different positions (18 total probes). Participants who customarily wore an ankle-foot orthosis wore it throughout the study.
Experimental Design
The study included 2 sessions separated by 3 or more days (Figure 1). During Session 1, participants performed a Dual-learning condition, which consisted of performing a joint-angle learning task with concurrent split-belt treadmill walking. During Session 2, participants performed the Joint-angle learning condition while walking with tied treadmill belts. As our primary goal was to investigate whether people with stroke can successfully learn 2 features of the walking pattern at once, participants always performed sessions in this order to ensure they were naïve to both tasks during the Dual-learning condition.
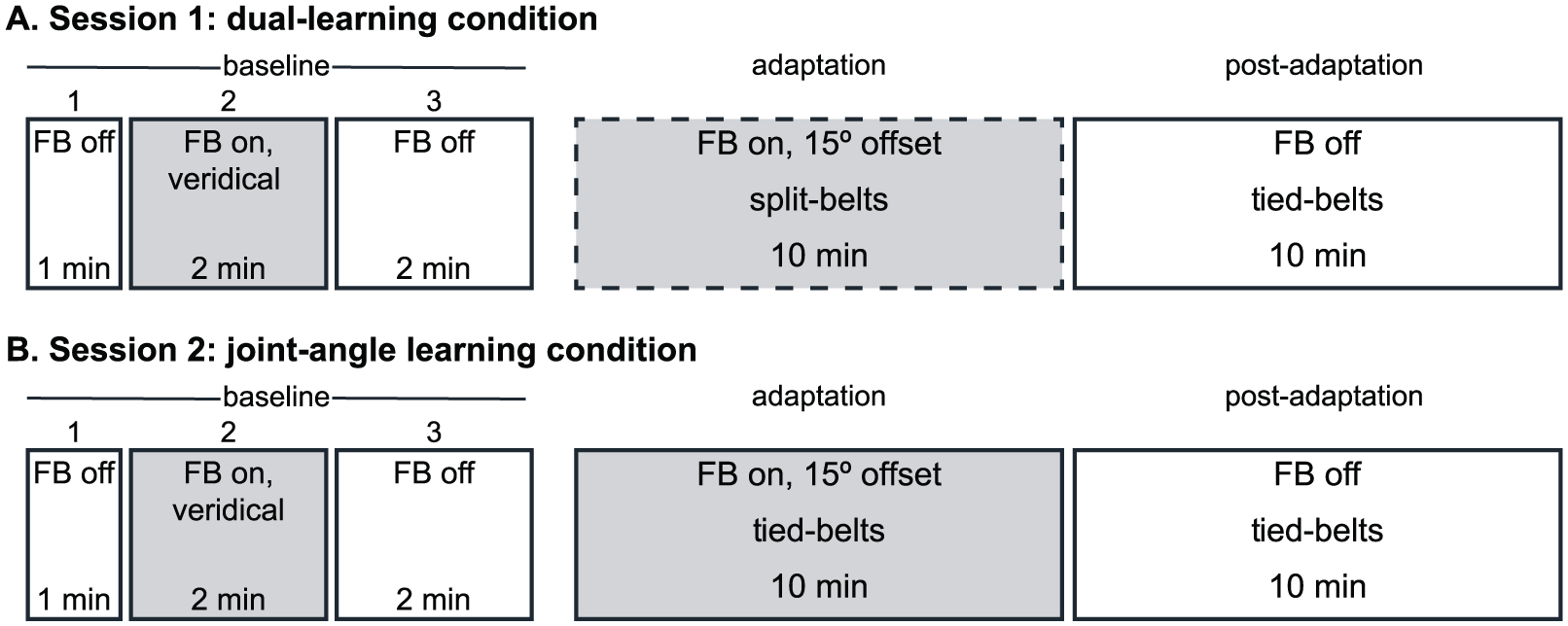
Experimental paradigm for Session 1 (A) and Session 2 (B). Visual feedback (FB) of paretic knee flexion was provided during Baseline 2 and Adaptation phases, shown in gray. No feedback was provided during all other phases, shown in white. In Session 1 (dual-learning condition), participants walked with split-belts during Adaptation, shown in dashed lines, and with tied-belts for all other phases of the experiment. The paradigm for the Session 2 differed only in that participants walked with tied belts throughout the experiment. Sitting rest breaks were given halfway through adaptation and postadaptation blocks during both sessions.
Joint-Angle Learning Task
We explored the effects of a joint-angle learning task 28 to teach people with stroke to increase their paretic knee flexion during walking. Participants were given real-time visual feedback of their paretic knee flexion angles during walking using a custom Python program that was synchronized with Optotrak software to sample marker position simultaneously. Knee flexion angle was calculated as the angle between the vector from the hip to the knee and the vector from the knee to the ankle; increasing positive values indicated increased flexion. Visual feedback was provided as a green bar on a screen that changed in height based on real-time changes in paretic knee flexion angle. Participants were told that the height of this green bar reflected the amount of bend in the paretic knee. Participants were also shown a “target” line and were instructed to walk such that the peak height of the green bar landed as close to the target line as possible. Although participants were not specifically instructed to reach the target during the swing phase, this point of peak sagittal knee flexion occurs during the swing phase. During adaptation, we introduced a 15° offset to the target line so that participants had to increase their knee flexion angle to succeed at the task.
Split-Belt Treadmill Walking
Participants walked on a custom split-belt treadmill (Woodway USA, Waukesha, WI), which has separate treadmill belts, driven by independent motors, for each leg. During Dual-learning, participants walked with periods of “split-belts,” where right and left belts moved at different speeds. All other walking periods occurred with “tied-belts,” where both belts moved at the same speed. The treadmill was controlled with a custom Python program in the Vizard (WorldViz) development environment. Participants wore a safety harness and held onto a handrail in front of the treadmill for all phases of the experiments.
Treadmill belt speeds were based on each individual’s over-ground walking speed. During split-belt walking, the fast belt was set to the participant’s fast over-ground walking speed and the slow belt was set to half of that speed. During tied-belt walking, both belts moved at the slow speed. Consistent with previous studies, 17 the leg that took the shorter step during over-ground walking was placed on the fast belt during split-belt walking. For some participants, this was the paretic leg and for others it was the nonparetic leg.
Optotrak Motion Analysis
Kinematic data were collected during walking at 100 Hz using Optotrak (Northern Digital, Waterloo, Ontario, Canada). Bilateral infrared-emitting markers were placed over the fifth metatarsal head, lateral malleolus, lateral femoral epicondyle, greater trochanter, iliac crest, and acromion process. Heel strike events were approximated as the maximum (positive) angle of the limb, and toe-off events were approximated as the minimum (negative) limb angle. 31
Experimental Paradigm
The experimental paradigm consisted of 5 walking phases. Baseline 1: 1 minute of walking with tied-belts and no visual feedback. Baseline 2: 2 minutes of walking with tied-belts and unbiased (ie, veridical) feedback such that the target line represented the mean peak paretic knee flexion measured during Baseline 1. Baseline 3: 2 minutes of walking with tied-belts and no visual feedback. Adaptation: 10 minutes of walking with either split-belts (Dual-learning) or tied-belts (Joint-angle learning). During this phase, feedback was offset −15° while the target line remained in the same location seen in Baseline 2. Successfully performing the task thus required participants to flex the paretic knee 15° more than at baseline. Postadaptation: 10 minutes of walking with tied-belts and no visual feedback to assess any aftereffects of the Adaptation phase. To mitigate fatigue, participants had 2-minute sitting rest breaks at the midpoint of adaptation and postadaptation.
Data Analysis
Kinematic data were analyzed stride-by-stride to calculate the peak paretic knee flexion angle during each stride cycle. In addition to paretic knee flexion, we were interested in step asymmetry, as it is known to adapt robustly to split-belt treadmill walking in healthy adults32,33 and those post-stroke. 17 Step asymmetry was defined as the normalized difference between the step lengths (SL) of the “fast” and “slow” leg, or:
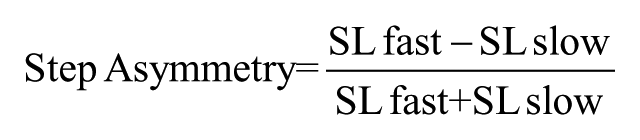
A step asymmetry of 0 indicates symmetric walking, while positive values indicate the fast step was larger than the slow step and vice versa for negative values. Note, however, that in Session 2 (joint-angle learning condition) we assigned any step asymmetry at baseline as a positive value, no matter if the paretic leg took a longer step or the nonparetic leg took a longer step. That way subjects with different direction asymmetries would not artificially collapse group averages.
We have previously shown that when neurologically intact adults perform a knee joint-angle learning task, they also increase hip flexion due to the mechanical coupling of hip and knee joints during gait. 28 Therefore, although participants only received feedback of paretic knee flexion, we analyzed peak paretic hip flexion. Hip flexion angle was calculated as the angle between a vertical reference passing from the hip to the floor and the vector from the hip to the knee; increasing positive values indicated increased flexion.
As in our previous work, 28 we characterized learning/unlearning patterns of all 3 outcome measures by averaging values in 5 epochs: baseline (mean of Baseline 3), early adaptation (first 5 strides of Adaptation), adaptation plateau (last 100 strides of Adaptation), early postadaptation (first 5 strides of Postadaptation), and postadaptation plateau (last 100 strides of Postadaptation). Additionally, the time-courses of learning/unlearning were quantified as the number of strides from the beginning of adaptation and post-adaptation until the respective parameter remained within the plateau range (mean ± 2 SDs of plateau) for 30 strides. 28
Statistics
We first used independent-samples t tests to confirm that there were no significant differences in baseline epoch (mean of baseline 3) between the dual-learning and joint-angle learning conditions. Once this was confirmed, all subsequent statistical analyses were performed on baseline-subtracted values, allowing us to account for the wide range of starting values found in this heterogeneous stroke population. To best visualize the results in figures, data were smoothed with a moving average and binned by 3 strides; statistics were performed on the unsmoothed data.
Our primary objective was to determine whether the Dual-learning condition produced changes in paretic knee flexion, step asymmetry, and paretic hip flexion. We then performed separate repeated-measures ANOVAs for each walking parameter to assess changes across epoch (early adaptation, adaptation plateau, early postadaptation, postadaptation plateau). This analysis was repeated for the Joint-angle learning condition as well. If the assumption of sphericity was violated (Mauchly’s test P < .05), Greenhouse-Geisser corrections were applied. If the repeated-measures ANOVA revealed a significant main effect of epoch, we observed pairwise comparisons to determine which epochs differed, as well as 1-sample t tests (test value = 0) to determine differences from baseline.
Finally, we sought to determine whether split-belt treadmill walking interfered with joint-angle learning. We used a 2-by-4 repeated-measures ANOVA to determine changes in paretic knee flexion between conditions (Dual-learning, Joint-angle learning) across epochs. We also used a 1-way ANOVA to compare rates (# strides-to-plateau) of learning and unlearning of peak paretic knee flexion. In all cases, post hoc analyses were performed using the Bonferroni correction when applicable, and we report corrected P values.
Results
Demographics
Twelve participants with chronic stroke and mild-to-moderate lower extremity motor deficits (Table 2) were included in this study. One additional participant met inclusion criteria but was subsequently excluded from analyses because he could not perform the task on which learning was being assessed (ie, he could not modulate paretic knee flexion while walking).
Demographic Data a .
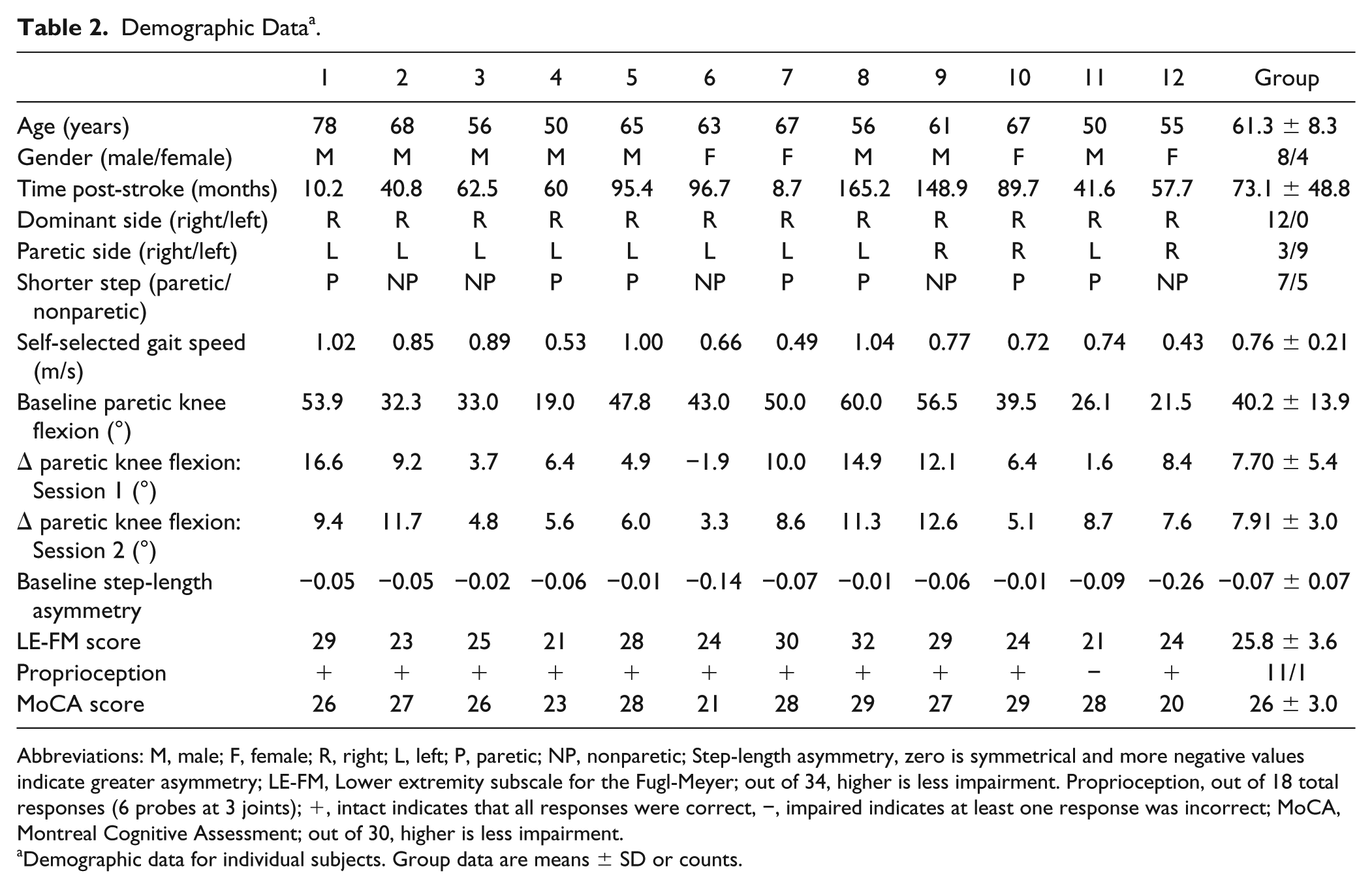
Abbreviations: M, male; F, female; R, right; L, left; P, paretic; NP, nonparetic; Step-length asymmetry, zero is symmetrical and more negative values indicate greater asymmetry; LE-FM, Lower extremity subscale for the Fugl-Meyer; out of 34, higher is less impairment. Proprioception, out of 18 total responses (6 probes at 3 joints); +, intact indicates that all responses were correct, −, impaired indicates at least one response was incorrect; MoCA, Montreal Cognitive Assessment; out of 30, higher is less impairment.
Demographic data for individual subjects. Group data are means ± SD or counts.
Dual-Learning Condition
Participants performed the joint-angle learning task while walking on a split-belt treadmill. We found that simultaneously performing these 2 tasks led to increased peak paretic knee flexion (Figure 2A and B) and adaptation of step asymmetry (Figure 2C and D). The group was able to immediately increase knee flexion by roughly 5°, and then slowly increase it another 5° during adaptation, peaking at approximately 10°. During postadaptation, the group appears to show a small after-effect, though this varied greatly between subjects. Subjects returned to baseline by the end of postadaptation. Repeated-measures ANOVA demonstrated a significant effect of epoch for Δ paretic knee flexion (F[3, 33] = 5.961, P = .002). That is, there were significant changes in adaptation and postadaptation measures. Post hoc tests showed a significant change in peak paretic knee flexion at adaptation plateau (7.698 ± 5.35°, P < .001). However, this increase was not significantly retained in postadaptation (early postadaptation: 3.363 ± 7.96°, P = .171).
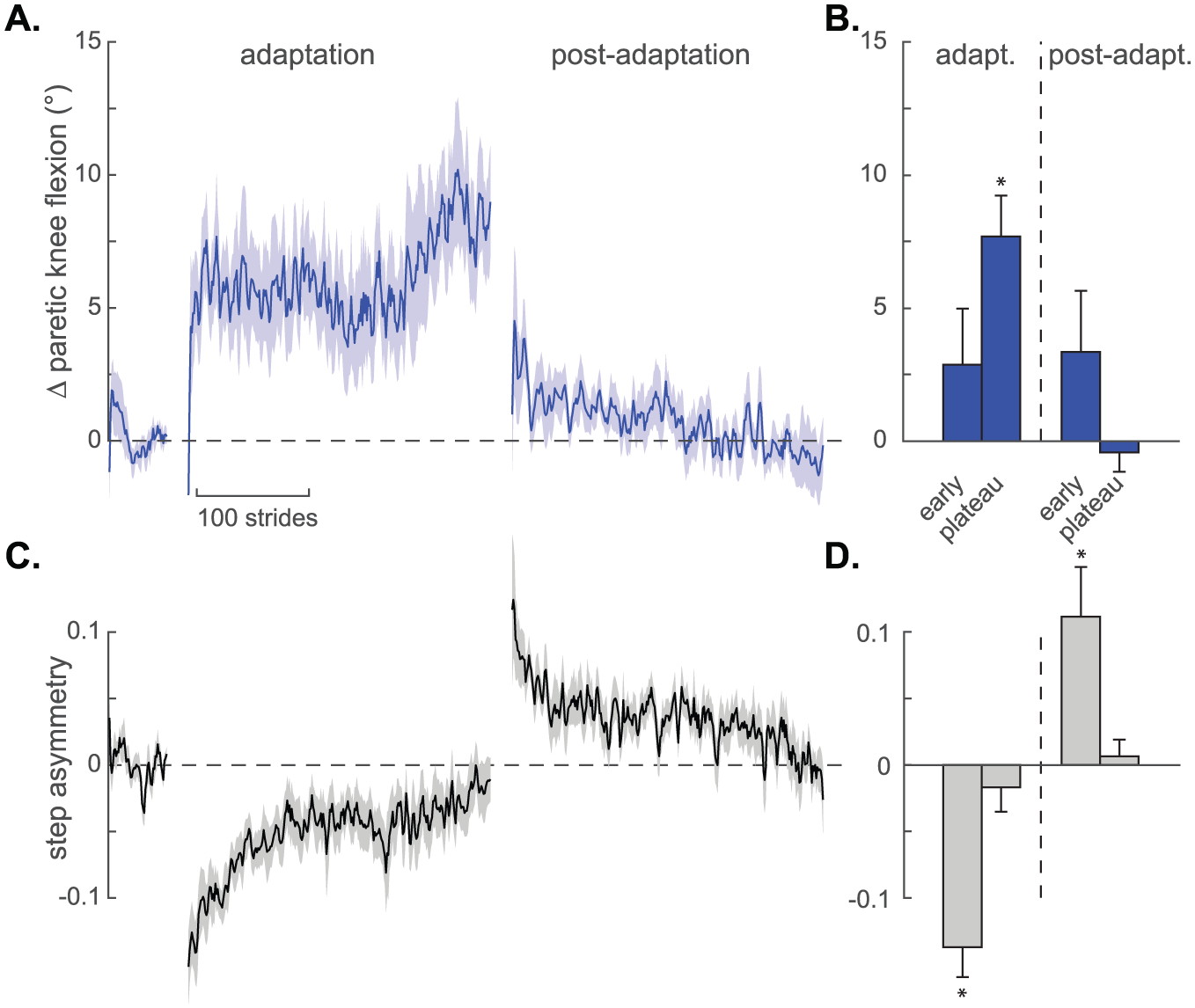
Results from the dual-learning condition. (A) Time series for change in paretic knee flexion angle plotted stride-by-stride during Baseline 3, Adaptation, and Postadaptation epochs. Data are smoothed with a running average by 3 strides and expressed relative to baseline (values >0 indicate increased paretic knee flexion compared to baseline). Shaded areas around each line represent SE. (B) Group average change in paretic knee flexion angle during early and plateau phases of Adaptation and Postadaptation. Data shown as means ± SE. (C) Time series for step length asymmetry plotted stride-by-stride. Positive values indicate that the fast step was larger than the slow step and vice versa for negative values. Data are smoothed with a running average by 3 strides and expressed relative to baseline. Shaded areas around each line represent SE. (D) Group average step asymmetry during early and plateau phases of Adaptation and Postadaptation. Data shown as means ± SE. *Significant change compared with baseline, P < .05.
Step asymmetry results indicated that performing the dual-learning task did not preclude participants with stroke from adapting to split-belt treadmill walking. On initial exposure to the split-belt treadmill, the group experienced an immediate perturbation such that step asymmetry decreased from baseline. Over time, the group adapted their walking pattern such that step asymmetry returned to near-baseline levels by adaptation plateau. Returning to tied-belt walking during postadaptation caused an initial motor aftereffect such that step asymmetry was greater than baseline levels. This aftereffect rapidly decayed, as subjects resumed walking with their baseline gait pattern. Repeated-measures ANOVA demonstrated a significant effect of epoch (F[1.816, 18.164] = 26.711, P < .001). Post hoc tests showed that step asymmetry was different from baseline early in adaptation and postadaptation (adaptation: −0.137 ± 0.07, P < .001; postadaptation: 0.111 ± 0.12, P = .014), but not at plateaus (adaptation: −0.017 ± 0.06, P = .382; postadaptation: 0.006 ± 0.04, P = .625). Together, these results demonstrate that paretic knee flexion and step asymmetry can be learned simultaneously, in a single session, using a dual-learning paradigm.
Joint-Angle Learning Condition
During the joint-angle learning task alone, we saw that the biased knee angle feedback increased peak paretic knee flexion. Figure 3A shows the time series of group data for paretic knee flexion while participants performed the joint-angle task during tied-belt walking. During adaptation, the group was able to immediately increase knee flexion, peaking at roughly 10°. Removal of visual feedback during postadaptation led to a rapid return to baseline levels of paretic knee flexion. Figure 3B shows group average data for specific epochs during adaptation and postadaptation. Repeated-measures ANOVA demonstrated a significant effect of epoch for paretic knee flexion (F[1.855, 20.409] = 7.749, P = .004). Post hoc tests revealed a significant change in paretic knee flexion between baseline and both early adaptation (5.007 ± 3.97°, P = .001) and adaptation plateau (7.906 ± 2.99°, P < .001), but not postadaptation (early: 2.389 ± 8.17°, P = .333; plateau: −0.037 ± 3.24°, P = .698).
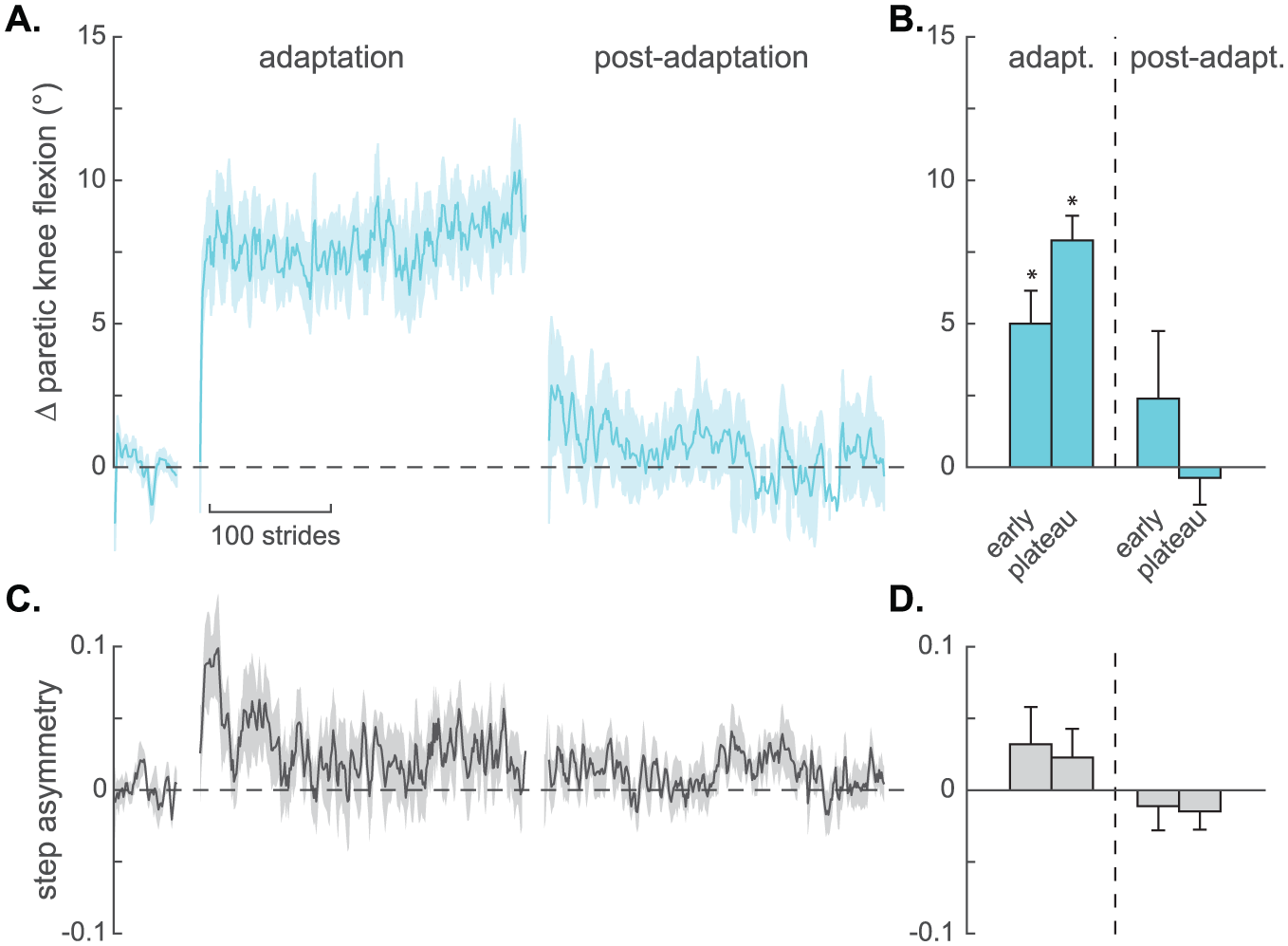
Results from the joint-angle learning condition. (A) Time series for change in paretic knee flexion angle plotted stride-by-stride during Baseline 3, Adaptation, and Postadaptation phases. Data are smoothed with a running average by 3 strides and expressed relative to baseline (values >0 indicate increased paretic knee flexion compared with baseline). Shaded areas around each line represent SE. (B) Group average change in paretic knee flexion angle during early and plateau phases of Adaptation and Postadaptation. Data shown as means ± SE. (C) Time series for step length asymmetry plotted stride-by-stride. Baseline step asymmetry is indicated by 0, while positive values indicate that the fast step was larger than the slow step and vice versa for negative values. Data are smoothed with a running average by 3 strides and expressed relative to baseline. Shaded areas around each line represent SE. (D) Group step asymmetry during early and plateau phases of Adaptation and Postadaptation. Data shown as means ± SE. *Significant change compared to baseline, P < .05.
Recall that during the joint-angle learning condition, participants walked with tied treadmill belts throughout the experiment. Therefore, we would not expect a significant change in step length asymmetry from baseline. Figure 3C shows the time series of group data for step length asymmetry. Although there appears to be a brief increase in step asymmetry at the beginning of adaptation, this was not statistically significant and step length asymmetry returned to baseline where it remained throughout the rest of adaptation and during all of postadaptation. Figure 3D shows the group average of step length asymmetry during adaptation and postadaptation epochs. Repeated-measures ANOVA showed no effect of epoch (F[3, 30] = 1.727, P = .182), indicating that performing the joint-angle learning task had no appreciable effect on step symmetry.
Influence of Split-Belt Walking on Joint-Angle Learning
To test whether walking on the split-belt treadmill interfered with performing the knee joint-angle learning task, we compared the change in paretic knee flexion between the Dual-learning condition (Figure 2A and B) and the Joint-angle learning condition (Figure 3A and B). We found that simultaneously performing the joint-angle learning task while adapting to the split-belt treadmill did not interfere with joint-angle learning. A 2-by-4 repeated-measures ANOVA of paretic knee flexion showed no main effect of condition (P = .831), and no condition-by-epoch interaction (P = .650). Plots of these data, however, suggested that there may be a difference in learning in the first portion of adaptation between conditions. However, additional paired t tests of the early adaptation epoch (2.88 ± 7.3 vs 5.01 ± 4.0, P = .303) and of an additional epoch encompassing strides 6 to 30 (5.93 ± 4.8 vs 7.90 ± 4.8, P = .086) were also nonsignificant. Participants also learned and unlearned the joint-angle pattern at similar rates in both conditions, as evidenced by comparing the number of strides-to-plateau for adaptation (142.3 ± 129.4 vs 110.3 ± 107.7 strides, P = .517) and postadaptation (121.2 ± 89.4 vs 132.8 ± 92.1 strides, P = .756).
Changes in Paretic Hip Flexion
As expected, in both the Dual-learning condition and the Joint-angle learning condition, there were significant changes in the amount of paretic hip flexion across time. Figure 4A and C shows the time series of group data for peak paretic hip flexion for dual-learning and joint-angle learning conditions, respectively. In both conditions, adaptation traces show that the group immediately increased hip flexion by approximately 15°, then fluctuated during the adaptation phase; remaining between 10° and 15° above baseline throughout adaptation. In both conditions, the group appears to show an aftereffect of approximately 5° during early postadaptation before returning to baseline values. Figure 4B and D shows group average data for paretic hip flexion during specific epochs of adaptation and postadaptation. Repeated-measures ANOVA demonstrated significant effects of epoch for both the Dual-learning condition (F[3, 33] = 11.918, P < .001) and the Joint-angle learning condition (F[3, 33] = 7.726, P < .001). Post hoc tests showed that for both conditions, paretic hip flexion increased compared with baseline at early adaptation (Dual-learning: 8.416 ± 5.35°, P < .001; Joint-angle learning: 9.347 ± 6.29°, P < .001) and at the adaptation plateau (Dual-learning: 11.436 ± 8.70°, P = .001; Joint-angle learning: 11.821 ± 6.79°, P < .001). In contrast to paretic knee flexion, changes in paretic hip flexion were retained postadaptation. Specifically, paretic hip flexion was significantly different from baseline (Dual-learning: 4.954 ± 6.58°, P = .024) or trended toward significance (Joint-angle learning: 6.054 ± 10.85°, P = .079) during early postadaptation.
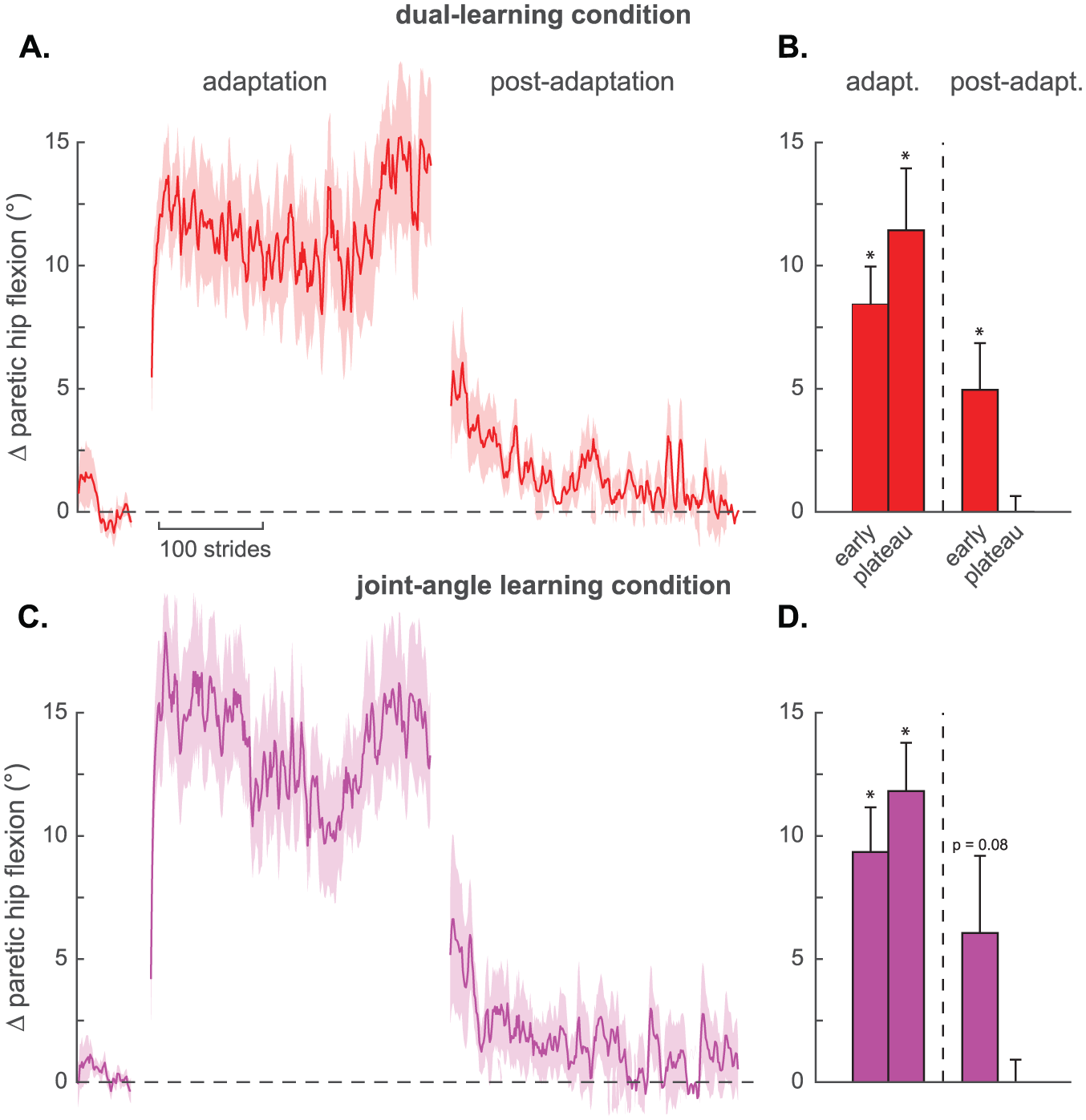
Change in paretic hip flexion for both conditions. (A, C) Time series for change in paretic hip flexion angle during the dual-learning and joint-angle learning conditions, respectively. Data are plotted stride-by-stride during Baseline 3, Adaptation, and Postadaptation phases, smoothed with a running average by 3 strides, and expressed relative to baseline (values >0 indicate increased paretic hip flexion compared to baseline). Shaded areas around each line represent SE. (B, D) Group average change in paretic hip flexion angle for early and plateau phases of Adaptation and Postadaptation during the dual-learning and joint-angle learning conditions, respectively. Data shown as means ± SE. *Significant change compared to baseline, P < .05.
Discussion
Here, we investigated whether individuals with stroke can use a dual-learning paradigm to simultaneously learn 2 distinct components of the walking pattern. We found that most of the people that we tested with stroke (ie, 10 of 12) could perform a joint-angle learning task concurrently with split-belt treadmill walking to simultaneously improve the amount of paretic knee flexion and step length asymmetry. Additionally, as previously seen in a similar study of healthy individuals, the joint-angle learning task targeting the knee joint also increased the amount of paretic hip flexion; likely due to the dynamic coupling between hip and knee joints.
In our previous study of dual-learning in neurologically intact participants, the patterns of learning and unlearning suggest that changes in joint angles occurred via implicit motor adaption processes rather than conscious adjustments of movement. 28 Specifically, following the removal of biased visual feedback, participants exhibited significant motor aftereffects, which are a hallmark of locomotor adaptation. 34 In the present study, however, participants with stroke did not show motor aftereffects in knee flexion during postadaptation. This may demonstrate that, in contrast to healthy individuals, participants with post-stroke motor impairments may be unable to rely exclusively on implicit adaptation processes to adjust paretic knee flexion. Rather, they may need to supplement implicit adaptation processes with conscious strategies in order to meet the joint-angle learning task goal. It has previously been shown that explicit awareness of movement errors is associated with a reduction of motor aftereffects.35,36 As such, while our participants with stroke successfully increased their paretic knee flexion in response to biased visual feedback, those adjustments were not retained in the manner previously seen in healthy people.
Though we suspect that the paradigm used here may require some degree of explicit strategy in people post-stroke, this type of dual-learning task—combining 2 motor learning tasks—is different from traditional “dual-task” paradigms that generally combine a motor and a cognitive task.35,37,38 This distinction is important, as motor-cognitive dual-task studies frequently demonstrate interference in the amount 38 or rate 35 of motor learning. Cognitive-motor interference has been attributed to competing demands for attentional resources 39 and may reflect compromised executive control.40,41 Given that the joint-angle learning task may be more physically and cognitively demanding for people with stroke compared with healthy participants, it is plausible that people with stroke would experience similar interference in performance of the dual-learning task. However, split-belt treadmill walking did not significantly interfere with joint-angle learning: participants with stroke had similar rates and magnitudes of joint-angle learning during the adaptation phases of both single and dual-learning conditions. Given that the current study design did not include a split-belt walking only condition, we cannot draw conclusions as to whether the joint-angle learning task interfered with split-belt treadmill adaptation. However, the magnitude and rate of step asymmetry adaptation in dual-learning was similar to previously published work 31 of split-belt adaptation—hinting that interference effects may be minimal. In either case, our results give credence to the idea that simultaneous learning of 2 movement components, whether through implicit adaptation or explicit strategy, can occur even as task demands increase.
Though this type of dual-learning protocol may be beneficial for some people post-stroke, there are likely subsets of people for whom it is ineffective. For instance, 2 participants increased paretic knee flexion in the joint-angle learning only condition but showed no improvements (Δ paretic knee flexion < mean − 1 SD) during the dual-learning task. One distinguishing feature of these 2 participants was they had very pronounced baseline deficits (eg, step length asymmetries of −0.14 and −0.09). It is plausible that because of their high degree of motor impairments, these individuals prioritized overcoming the destabilizing mechanical perturbation of the split-belt treadmill over engaging in the joint-angle learning task. Further supporting this hypothesis is the finding that there was a correlation between an individual’s lower extremity Fugl-Meyer score and change in paretic knee flexion during the Dual-learning (Pearson correlation: r = 0.671, n = 12, P = .017) but not the Joint-angle learning (Pearson correlation: r = 0.435, n = 12, P = .158) condition. Such participants who are particularly impaired in one specific domain may instead benefit from either a more traditional staged approach to gait rehabilitation or a dual-learning protocol that targets less prominent deficits. Although this study included a sample of only 12 people with chronic stroke, the presentations of these individuals were fairly heterogeneous (eg, baseline paretic knee flexion (19° to 60°), step length asymmetry (−0.01 to −0.14), and gait speed (0.43 to 1.04 m/s). Therefore, we believe that our finding that many, but not all, people with chronic stroke may benefit from this dual-learning intervention will likely hold true for the larger population of people with mild-moderate chronic stroke.
In addition to identifying which participants are most likely to respond to a dual-learning protocol, it is also important to consider which pairings of motor tasks may be successful. In this study, we selected tasks directed at 2 common and detrimental post-stroke gait deficits. There are, however, many faulty walking components that could potentially be addressed in combination. We suspect that in order to avoid motor task interference during future applications, it is important that each task in a dual-learning paradigm involve different kinematic parameters and use different sources of perturbation.28,42,43
One interesting observation from our data is the shape of the adaptation curves of paretic knee and hip flexion in the dual-learning condition. In our previous work, 28 healthy participants exhibited smooth learning curves and plateaus. In contrast, the learning curves expressed by our participants during the dual-learning condition seem to show 2 phases: an early increase in paretic joint flexion with plateau near the midpoint, then a second increase in paretic joint flexion from in the middle into-end of adaptation. One possible interpretation is that engaging in split-belt treadmill walking caused a distraction to learning the joint-angles task such that participants may have waited to fully adapt their joint angles until they reached a stable state of step length asymmetry. A second possible explanation relates to the fact that all participants took a sitting rest break half way through the adaptation period to mitigate fatigue. It is possible that the initial plateau in joint-angle learning resulted from participant fatigue, and after a period of rest, participants were able to continue learning the joint-angle task. Given the close proximity of the rest break to the second increase and plateau of joint angles, we favor the later possibility.
This study is an important first step in demonstrating that people with stroke have the capacity to walk with greater paretic knee and hip flexion than they exhibit in their normal walking patterns. In the realm of stroke rehabilitation, a discussion is emerging about the disconnect between motor capacity (eg, what a person can do) and motor performance (eg, what a person actually does in daily life). 44 For example, Waddell et al found that improved motor capacity resulting from an intensive upper limb intervention did not translate to increased upper limb performance in people with chronic stroke. 45 Here, we revealed that people with stroke have the capacity to walk with more paretic hip and knee flexion than they normally exhibit. Real-time biofeedback may facilitate a more explicit awareness of the relationship between a motor command and motor output allowing a person to exhibit more control over his/her movements. As we advance this dual-learning protocol down the translational pipeline toward clinical implementation, it will be important to develop an understanding of how to capitalize on this uncovered motor capacity to improve walking performance in daily life.
We have shown that a joint-angle learning task (providing biased visual feedback) can be used to increase paretic knee flexion during walking in people with chronic stroke. Moreover, people with stroke can perform this task simultaneously with split-belt treadmill adaptation, changing 2 clinically relevant impairments in walking in a single session. Long-term studies are needed to determine if this strategy can be used to efficiently and permanently alter multiple gait impairments.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NIH 2R37NS090610 awarded to Bastian.