
Abstract
Background. Quantitative posturography has been reported as a reliable tool to measure balance in people with multiple sclerosis (MS). However, data on its diagnostic accuracy in predicting the occurrence of falls are lacking. Objective. To determine sensitivity, specificity, predictive values, and accuracy of posturography in detecting falls in MS subjects over a 3-month follow-up period. Methods. One hundred consecutive patients with MS were tested by the Berg Balance Scale (BBS) and by static posturography on a monoaxial platform. Participants recorded the occurrence of accidental falls for the next 3 months. Abnormal cutoff values for static standing balance measures were set at 2 standard deviations above the mean values obtained from 50 healthy controls (HC). The diagnostic accuracy of the BBS and static posturography was analyzed with respect to the prospectively collected data on the occurrence of falls. Results. Posturometric measures in participants with MS were significantly worse than in HC (all P values <.0001); however, only the center of pressure (COP) path with open eyes condition had substantial test–retest reliability. Static posturography was more sensitive (88% vs 37%) and accurate (75% vs 63%), but slightly less specific (67% vs 81%), than the BBS in predicting accidental falls. A logistic regression analysis revealed that the worse the COP path, the greater the risk for accidental falls (odds ratio = 1.08; P < .0001), even after adjusting for sex, age, disease duration, body mass index, MS subtype, Expanded Disability Status Scale, and BBS score. Conclusion. The COP path measurement in static position is a sensitive and accurate tool to identify people with MS who are at risk of accidental falls.
Introduction
Lack of balance is among the most disabling symptoms of multiple sclerosis (MS) and may affect about 75% over the course of the disease. 1 One major concern is their high incidence of accidental falls, which ranges from 52% to 63% over 2 to 6 months.2-5 Accidental falls are associated with considerable morbidity, including trauma, immobilization, and fractures, especially in patients suffering from osteoporosis. 6
Falls and fear of falling may also restrict the patients in performing daily living activities and negatively affect quality of life. 3 The consequences of activity curtailment driven by the fear of falling and subsequent deconditioning may be significant. 7 Therefore, identifying the patients who are at risk of accidental falls from those who are not is necessary to establish intervention and rehabilitation programs.
Clinical scales are hampered by their variable execution and subjective scoring systems 8 and have also been reported as having poor or moderate sensitivity (from 40% to 65%) in discriminating between fallers and nonfallers with MS. 9 By contrast, instrumental measures of balance may be more sensitive than common clinical tests for documenting both deficits10,11 and improvements12,13 in balance, even in minimally impaired persons with MS14-17 or in patients affected by a clinically isolated syndrome suggestive of MS. 18 Therefore, quantitative measures as provided by posturography might provide a reliable tool to identify MS subjects at risk of falls, but data on the diagnostic accuracy (ie, the extent to which a measurement is close to the true value) of static posturography in identifying patients at risk of falls are still lacking.
The aims of this study were (a) to test the reliability of static standing balance measures (SSBMs) as provided by static posturography and (b) to calculate its sensitivity, specificity, predictive values, and accuracy for detecting patients at risk of falls.
Methods
Participants
People diagnosed as affected by MS as per McDonald criteria 19 and regularly attending the outpatient MS Centre of S. Andrea Hospital in Rome were consecutively recruited for the present study. Eligibility included age from 18 to 55 years, an Expanded Disability Status Scale (EDSS) 20 score from 0 to 5.5, and clinical stability for at least 6 months. Exclusion criteria included pregnancy, severely blurred vision, disease-modifying or symptomatic treatments that began or dose regimen that changed in the previous 3 months, concomitant otological or vestibular disease (non-MS related), psychiatric disorders, severe cognitive impairment, and cardiovascular and respiratory diseases.
To obtain normative values for SSBMs, sex- and age-matched healthy volunteers were also recruited among the students in physiotherapy, residents, nurses, and doctors working on the Neurology Unit of S. Andrea Hospital. This study was approved by the ethics committee of our institution; informed consents were obtained from each participant.
Study Procedures
The assessment protocol consisted of a neurological evaluation, including the EDSS, Berg Balance Scale (BBS), 21 and static posturography. Patients were then instructed to report the occurrence of their falls (defined as an unexpected contact of any part of the body with the ground) over 3 months by means of a daily diary. They were also asked to report the circumstances in which they fell. The physiotherapist (DF) phoned patients monthly to remind them to record the occurrence of falls in the diary, which was returned at the end of the 3-month follow-up.
The BBS is a 14-item scale exploring the ability to sit, stand, lean, turn, and maintain the upright position on one leg; a cutoff score of 45 is an established criterion to identify elderly subjects with high risk of fall. 22 A sensitivity of 40% and a specificity of 90% in predicting fall status has been reported for the BBS in an Italian MS population. 9
Static posturography was carried out by a trained physical therapist (DF) unaware of clinical data by a monoaxial force-platform (ProKin, Tecnobody, Dalmine, Italy), 23 consisting of 3 strain gauges set in a triangular position under a surface of 55 cm diameter, with a 20-Hz sampling rate and a sensitivity of 0.1°. Static posturography was performed according to a standardized procedure as follows: Each subject was asked to stand barefoot on the ground, in upright static condition, double-leg stance, and with arms resting at their sides. The position of the feet on the force-platform was standardized using a V-shaped frame, keeping on a 3-cm distance between the 2 medial malleoli and an extra rotation of 12° with respect to the sagittal axis. 10
Stance conditions were tested with open eyes (OE) and closed eyes (CE); each test lasted 30 seconds. The instant positions of the center of pressure (COP) on the ground (this is estimated as compatible with the center of gravity at about 97%) 24 was used to calculate the following time domain measures: the velocity of the COP on the anteroposterior (AP) or mediolateral (ML) axes (COP vel; mm/s), the sum of the displacements of COP on force-measuring platform (COP path; mm), and the 95% confidence ellipse area (COP area; mm2).
Statistical Analyses
The target condition was the occurrence of one or more falls. The index test was static posturography. The reference test was the BBS; according to a previous study on patients with MS, a score ≥44 was considered as abnormal. 9
Data are presented as mean (SD), median (range), or proportion, as appropriate. Differences between groups were tested using the χ2 test with Yate continuity correction and Mann–Whitney U tests for continuous and dichotomous variables, respectively. Relationships between variables were tested using the Spearman rank coefficient. The normal distribution of the SSBMs was assessed by the Shapiro–Wilk test. Test–retest reliability for SSBMs in MS patients was assessed as concordance correlation coefficient (CCC), and its relative 95% confidence intervals (CIs), by comparing the average measures of 3 consecutive trials from 2 different evaluations separated by a 30-minute interval.
To test the diagnostic accuracy of static posturography, we applied criteria according to the STARD initiative. 25 Sensitivity, specificity, positive and negative predictive values (PPV and NPV, respectively), accuracy, and their 95% CIs were measured for the presence of the target condition (ie, being a faller or a nonfaller in the 3-month follow-up). Sensitivity was calculated as true-positive/(true-positive + false-negative), specificity as true-negative/(true-negative + false-positive), PPV as true positive/(true-positive + false-positive), NPV as true-negative/(true-negative + false-negative), accuracy as true-positive + true negative/(true-positive + false-negative + true-negative + false-positive). Estimates of variability of diagnostic accuracy between subgroups of patients were tested after binning the whole MS population according to EDSS tertiles.
We evaluated the potential predictors for the fall status (ie, the dependent variable) computing the odds ratio (OR), with their relative 95% CIs, by a stepwise logistic regression analysis (forward stepwise selection) including as covariates: sex (female or male), age, body mass index (BMI), disease duration, MS subtype (relapsing–remitting or secondary progressive), EDSS and BBS scores, and SSBMs. In each subsequent step, the regression equations comprised those variables reaching specific thresholds of F and P values (for variable inclusion, F ≥ 1 and P ≤ .05; for exclusion, F < 1 and P > .05); interactions terms were also tested, where appropriate. All P values less than .05 (2-sided) were considered as significant. Analyses were carried out using a PC version of Statistical Package for Social Sciences 16.0 (IBM SPSS, Chicago, Illinois).
Results
Participants
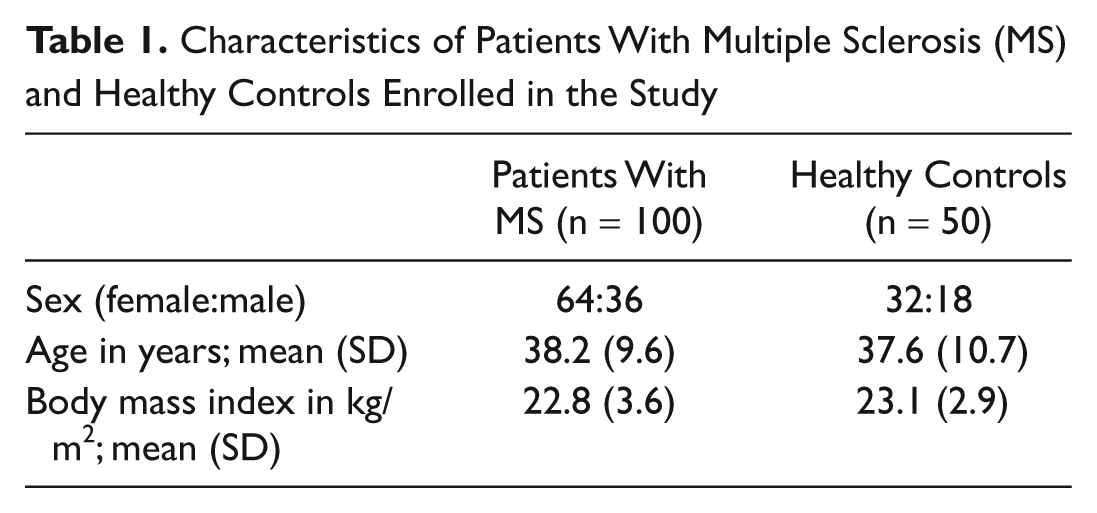
From September 2010 until April 2011, we consecutively enrolled 100 MS patients (64 women, 36 men) and 50 sex and age-matched healthy subjects (32 women, 18 men). Patients had a mean age of 38.0 (9.9) years, mean disease duration of 9.5 (6.4) years, and median EDSS score of 3.2 (1.0-5.0). There were no differences regarding sex, age, and BMI between patients and controls (Table 1). Table 2 shows the normative values for SSBMs obtained by the sample of the healthy controls. SSBMs of healthy controls were normally distributed (P = .25), whereas those of MS patients did not satisfy the normality assumption (P < .0001).
Characteristics of Patients With Multiple Sclerosis (MS) and Healthy Controls Enrolled in the Study
Normative Values for Static Standing Balance Measures From a Sample of 50 Healthy Subjects
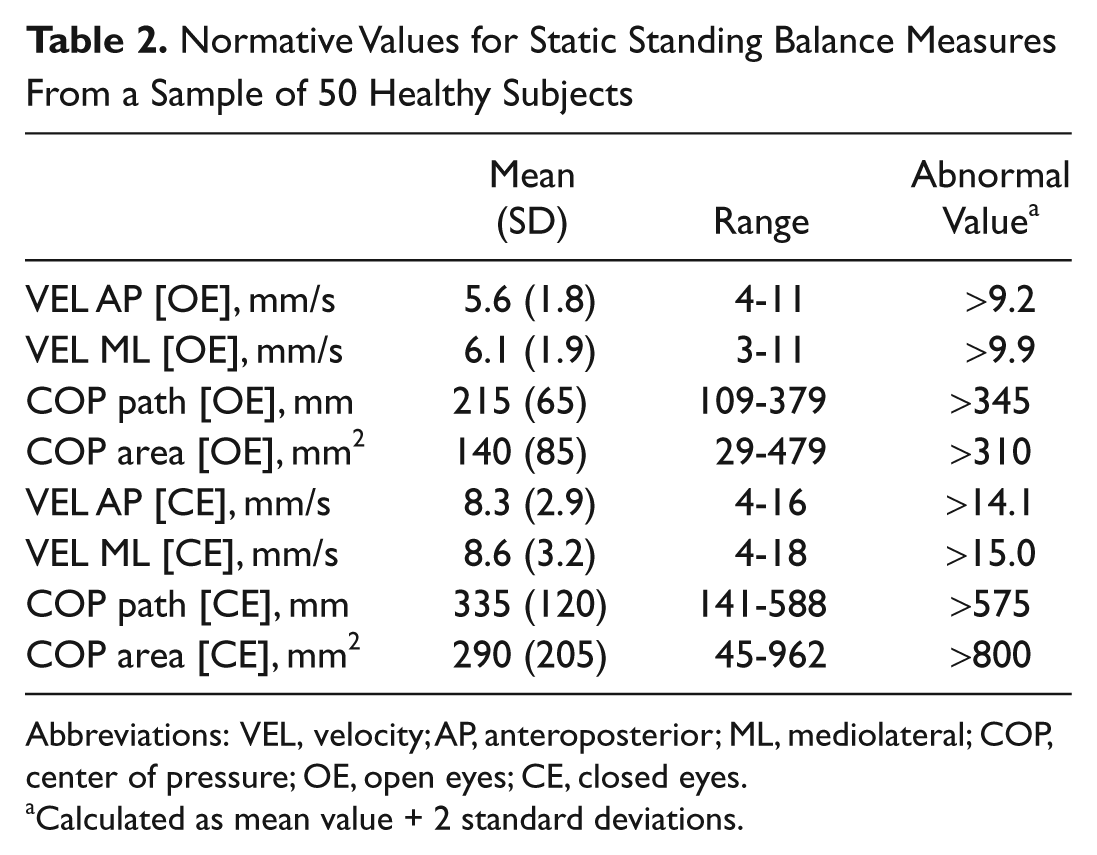
Abbreviations: VEL, velocity; AP, anteroposterior; ML, mediolateral; COP, center of pressure; OE, open eyes; CE, closed eyes.
Calculated as mean value + 2 standard deviations.
Follow-up Data
At 3 months, 41 (41%) of the participants reported 1 or more falls; 22 had 1 fall, 11 had 2 falls, and 8 had ≥3 falls. Two falls resulted in an injury: A 45-year-old woman with an EDSS score of 3.5 had a hip fracture during her daily living activities and a 37-year-old man with an EDSS score of 3.0 had a minor head trauma (without loss of consciousness) while walking in the dark.
Table 3 shows baseline demographic and clinical characteristics of MS participants according to the occurrence of their falls. Fallers had a longer disease duration (P = .02) and worse EDSS and BBS scores than nonfallers (P = .001 and P < .0001, respectively). During the static stance trials, the fallers moved faster in the AP and ML directions and had wider displacement of COP path than nonfallers, in both OE and CE conditions (all P values <.0001). Interestingly, several parameters, especially when measured in CE condition, had mean values larger than the abnormal cut-points not only in fallers but also in the nonfaller group.
Demographic, Clinical, and Posturometric Characteristics of Patients With Multiple Sclerosis (n = 100) According to Fall Status at the End of the 3-Month Observational Period a
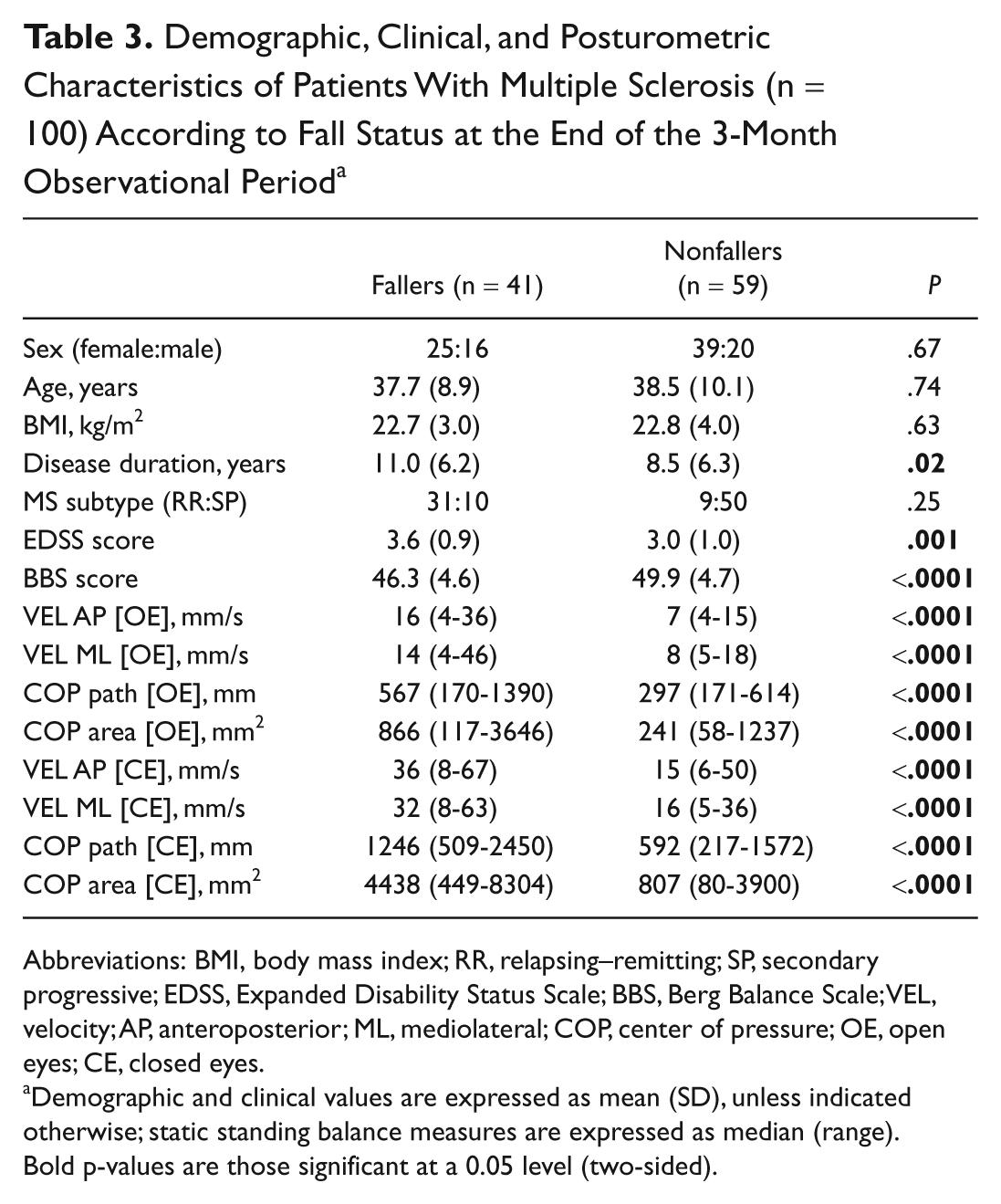
Abbreviations: BMI, body mass index; RR, relapsing–remitting; SP, secondary progressive; EDSS, Expanded Disability Status Scale; BBS, Berg Balance Scale; VEL, velocity; AP, anteroposterior; ML, mediolateral; COP, center of pressure; OE, open eyes; CE, closed eyes.
Demographic and clinical values are expressed as mean (SD), unless indicated otherwise; static standing balance measures are expressed as median (range). Bold p-values are those significant at a 0.05 level (two-sided).
Moreover, patients who reported multiple falls over the study period had worse BBS and EDSS scores, as well as SSBMs than those who reported only 1 fall over the 3-month study period (P values ≤.005; data not shown).
Figure 1 shows the differences in the SSBMs among patients who reported at least 1 fall over the 3-month follow-up period (n = 41), those who did not (n = 59), and the healthy control group (n = 50). As expected, we observed a gradient for worse SSBMs in the 3 groups (fallers > nonfallers > healthy controls with P < .0001 for all between-group comparisons).
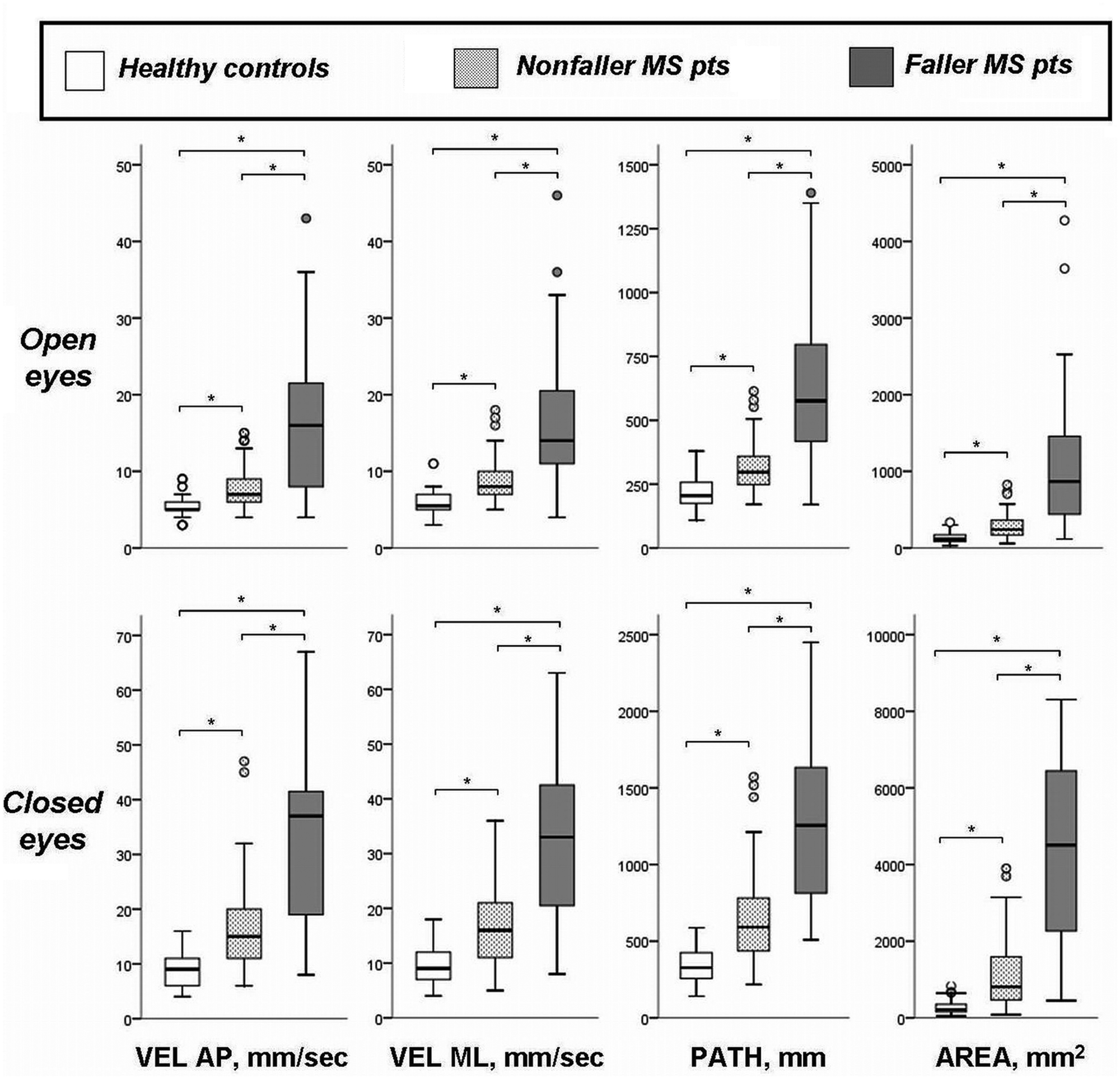
Static standing balance measures of healthy controls, nonfallers, and faller patients with multiple sclerosis. Abbreviations: MS, multiple sclerosis; VEL, velocity; AP, anteroposterior; ML, mediolateral. P < .0001 by the Mann–Whitney U test.
Reliability of Static Posturography
Table 4 shows the test–retest reliability of SSBMs. A better test–retest reliability was observed for the measures recorded in the open rather than the closed eye condition. However, the unique SSBM having a substantial CCC (ie ≥95% 26 ) was the COP path [OE]; hence, we selected this single measure for the diagnostic accuracy analyses. We also observed that all the SSBMs were related to one another, with correlation coefficient ranging from 0.61 to 0.86 (all P values <.0001 by the Spearman rank correlation coefficient).
Test–Retest Reliability for Static Standing Balance Measures, as Assessed in Patients With Multiple Sclerosis (n = 100), Expressed as Concordant Correlation Coefficients, and Their Relative 95% Confidence Intervals
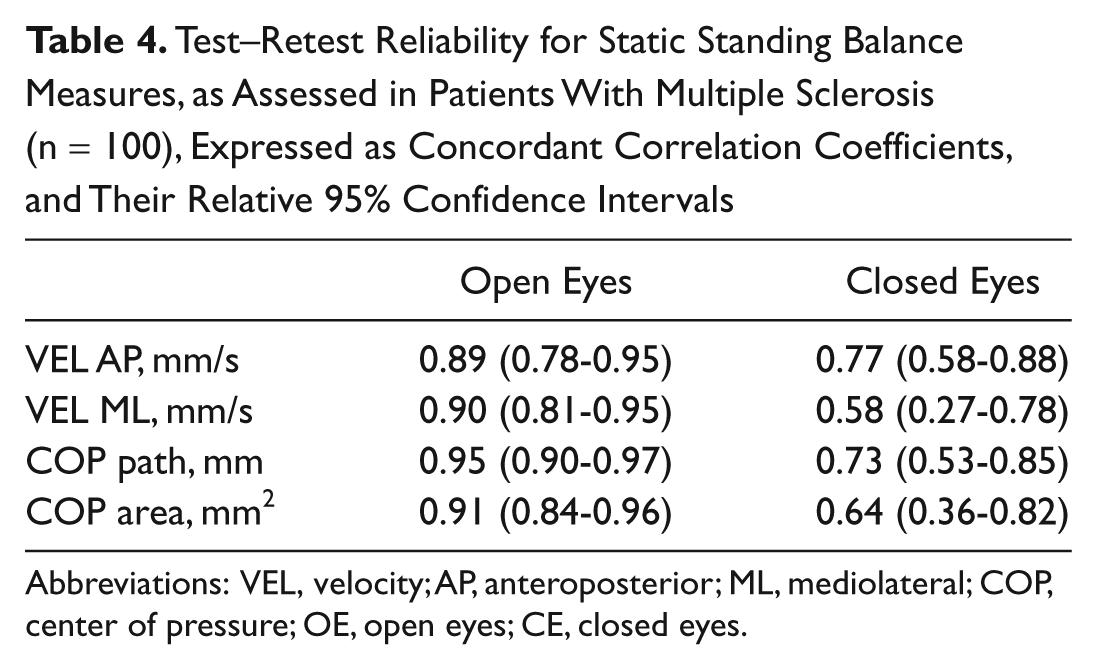
Abbreviations: VEL, velocity; AP, anteroposterior; ML, mediolateral; COP, center of pressure; OE, open eyes; CE, closed eyes.
Diagnostic Accuracy
Figure 2 shows the flow diagram regarding the diagnostic accuracy of BBS and the COP path in OE condition. The overall diagnostic accuracy of static posturography in detecting the target condition was better than BBS (75% vs 64%): Static posturography had better sensitivity and NPV, similar PPV, and slightly worse specificity than BBS (Table 5). Moreover, we observed a certain degree of variability in the diagnostic accuracy of static posturography according to the disability level (Figure 3). After binning the whole MS population according to EDSS tertiles (≤2.0, 2.5-3.5, ≥4.0), we found that the worse the disability level, the greater the sensitivity. By contrast, static posturography lost specificity in patients with higher EDSS scores. However, the overall accuracy of static posturography ranged from good to very good (from 71% to 80%). For the COP path in the OE condition, the EDSS and BBS scores were significantly related (Table 6)—the multivariate analysis further confirms that static posturography provided the best predictor of the risk for the occurrence of accidental falls. According to the stepwise logistic regression, only the COP path [OE] predicted the risk of accidental falls, whereas the other variables included in the model as covariates (sex, age, BMI, disease duration, MS subtype, EDSS and BBS scores) were excluded from the final model. In particular, we found that the risk of accidental falls increased by 8% for each 10-mm increase in COP path [OE] (OR = 1.08, 95% CI = 1.04-1.12; P < .0001; Table 7). This model explains a quite considerable amount of the variance (43%, Nagelkerke pseudo R2 = .43) in predicting the fall status.
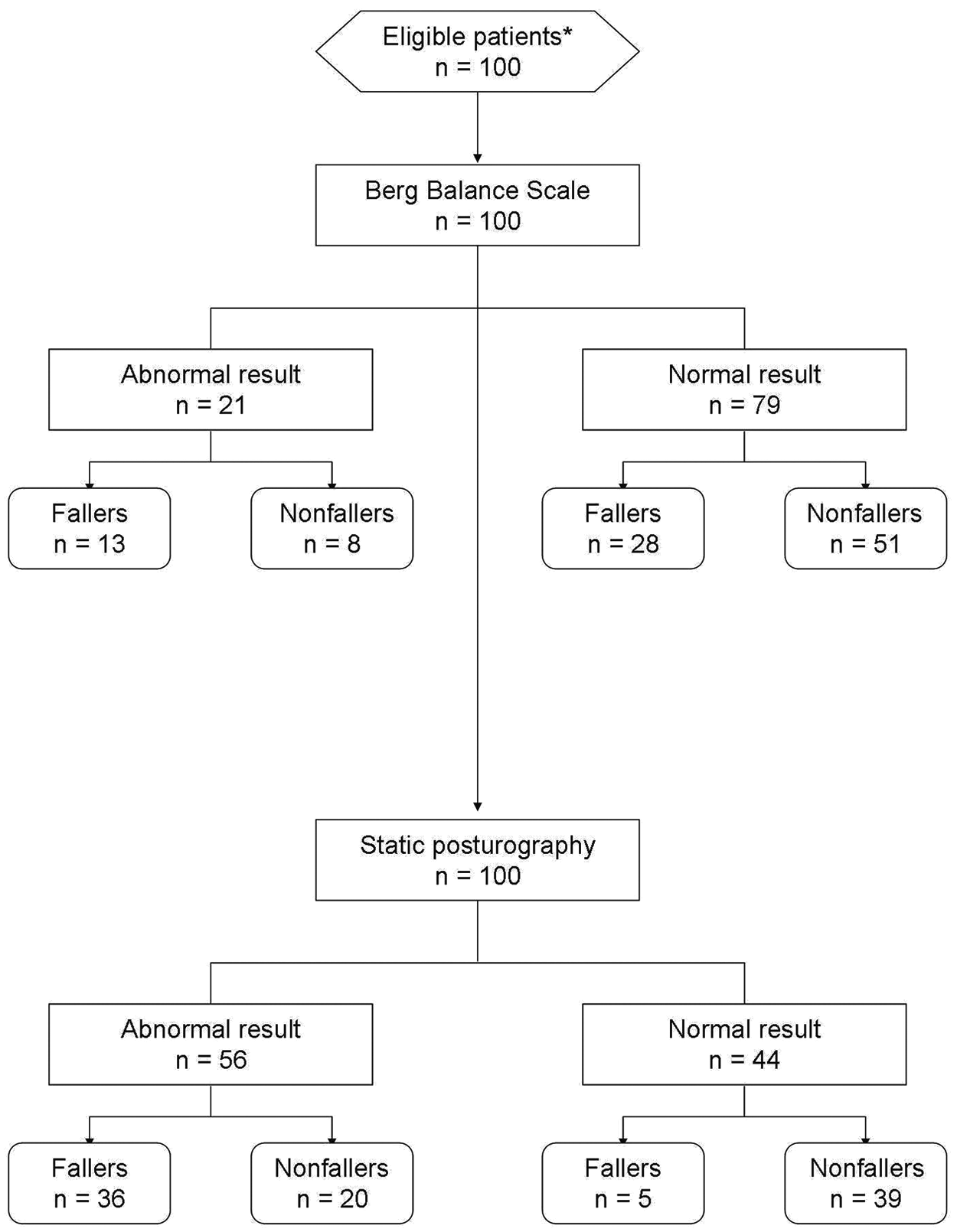
Flow diagram (as recommended by the STARD criteria) showing the number of patients undergoing the index test (ie, the static posturography), the reference test (ie, the Berg Balance Scale), and their relative diagnosis. *In this study, the patients were recruited consecutively.
Diagnostic Values and Their Relative 95% Confidence Intervals, of Index Test (ie, the Static Posturography) and Reference Test (ie, the Berg Balance Scale), as Assessed in Patients With Multiple Sclerosis (n = 100)
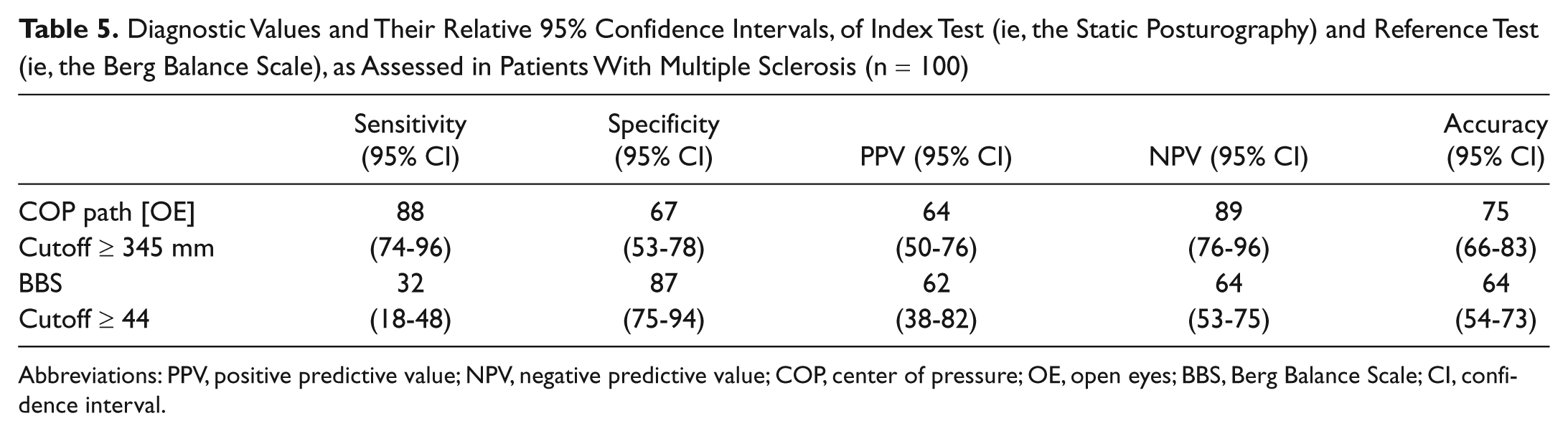
Abbreviations: PPV, positive predictive value; NPV, negative predictive value; COP, center of pressure; OE, open eyes; BBS, Berg Balance Scale; CI, confidence interval.
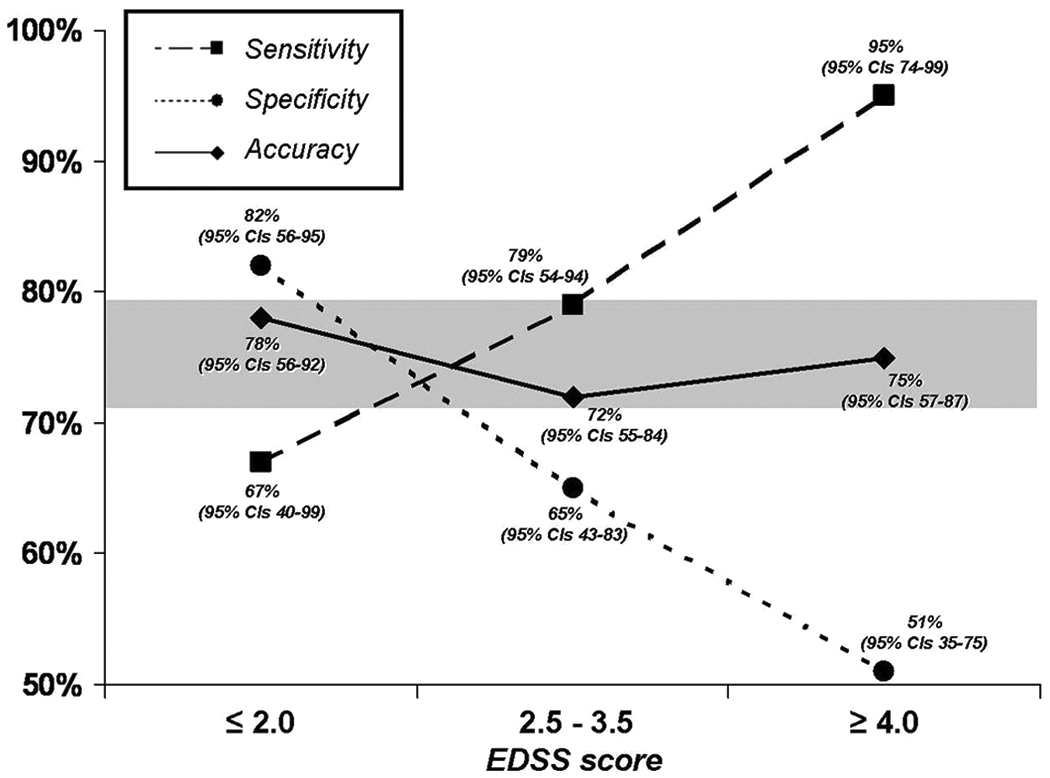
Sensitivity, specificity, and accuracy (with their relative 95% confidence intervals) of static posturography according to disability level (after splitting the population in EDSS tertiles). Abbreviations: CI, confidence interval; EDSS, Expanded Disability Status Scale.
Results of the Bivariate Correlation Analyses in Patients With Multiple Sclerosis (n = 100), Expressed as Spearman Rank Correlation Coefficient a
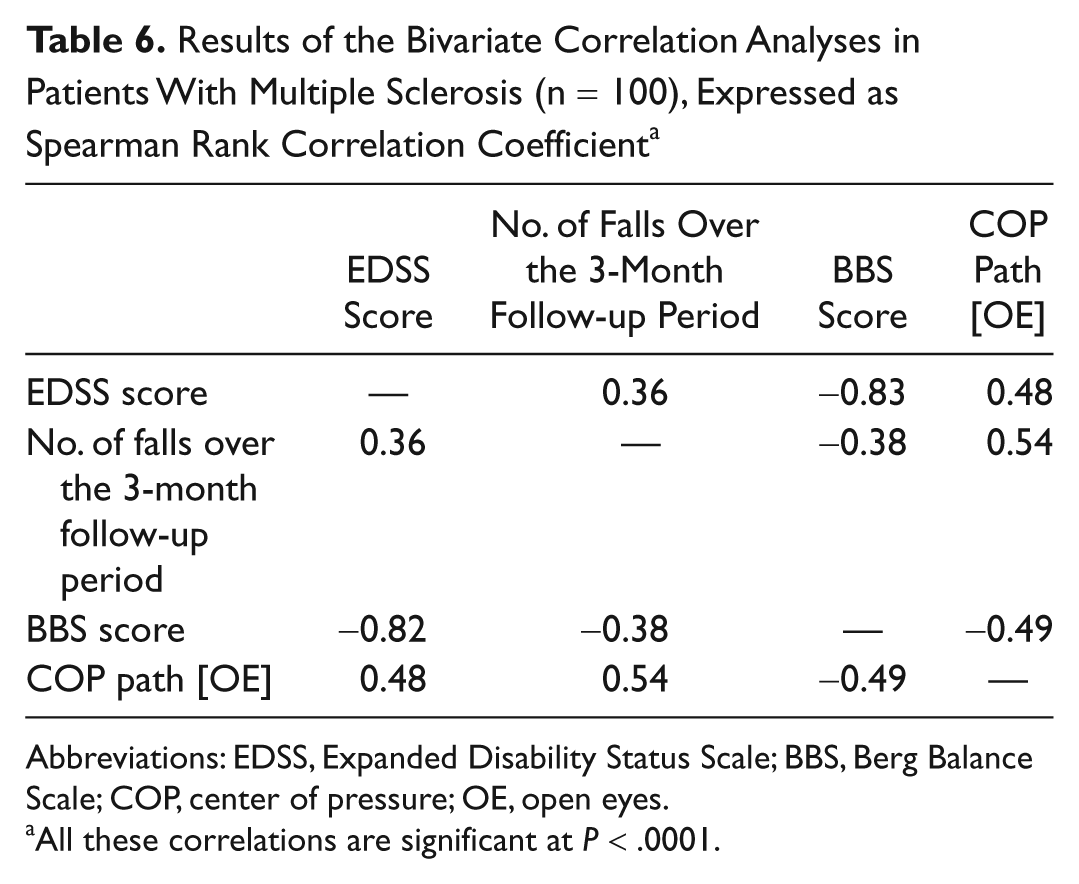
Abbreviations: EDSS, Expanded Disability Status Scale; BBS, Berg Balance Scale; COP, center of pressure; OE, open eyes.
All these correlations are significant at P < .0001.
Statistical Score and Partial Correlation for Each Variable Included in the Logistic Regression Model That Was Built to Predict the Fall Status Over the 3-Month Follow-up Period a
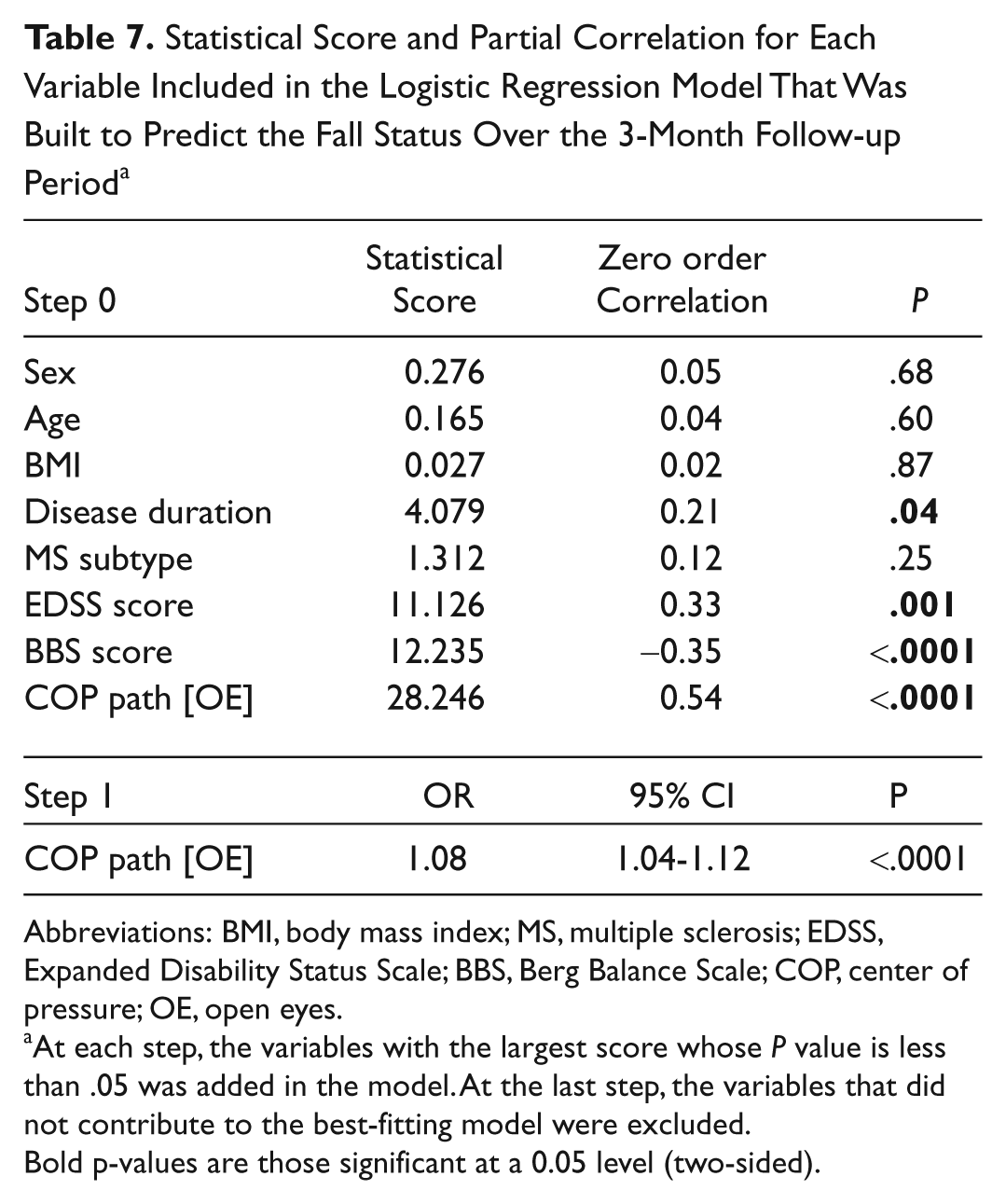
Abbreviations: BMI, body mass index; MS, multiple sclerosis; EDSS, Expanded Disability Status Scale; BBS, Berg Balance Scale; COP, center of pressure; OE, open eyes.
At each step, the variables with the largest score whose P value is less than .05 was added in the model. At the last step, the variables that did not contribute to the best-fitting model were excluded.
Bold p-values are those significant at a 0.05 level (two-sided).
Discussion
In the present prospective study, we demonstrated the high diagnostic reliability and accuracy of static posturography to detect risk of accidental falls over a short interval in people with MS. The COP path in the OE condition had the best test–restest reliability, but generally, all the measures recorded with OE had CCC values better than those in the CE condition. One possible explanation encompasses a greater variability of SSBMs as a source of a major intrasubject variability, especially when the visual input is not available.10,13,15,27
There were significant differences between patients with MS and healthy control subjects regarding the SSBMs, even considering that about one third of our population had only a minimal or no disability as measured by an EDSS lower than 2.5. Accordingly, a recent study demonstrated that about 40% of patients with clinically isolated syndrome had poor or very poor scores in COP sway rate (ie, 2-4 or ≥4 SD higher than the mean value of healthy controls, respectively) in OE condition. 18 Other studies also demonstrated balance deficit in minimally impaired MS patients,14-17 even in patients with normal clinical balance test, thus suggesting that MS patients may have a subclinical balance disorder unrevealed by conventional balance tests. 17
Our study also showed that static posturography was more accurate than BBS, a well-established clinical tool for measuring balance in MS and other neurological diseases. We found that BBS had poor sensitivity although slightly higher specificity than the COP path in OE condition, with more than 10% difference in accuracy in favor of static posturography. We adopted a cutoff score of 44 for the BBS, since it had been previously determined in the MS setting. 9 Accordingly, we found sensitivity and specificity (37% and 83%, respectively) 9 similar to those reported (40% and 90%, respectively). 9 In contrast, in another MS sample, a sensitivity of 94% and a specificity of 32% were found by using a cutoff point between 55 and 56 points (the maximum score). The authors concluded that a ceiling effect on the BBS may have caused an artifact. 4 In our opinion, these 2 conflicting results further strengthen the a priori hypothesis that computer-based SSBMs are better than clinical scales.
It can be argued that the major limitation of static posturography is represented by an overestimation of patients prone to accidental falls (34% false-positives in our study, especially among those patients with mild disability). However, in a clinical context, it may be better to identify a greater proportion of patients with false-positive than false-negative risk. Moreover, one could speculate that the false-positive group included patients having an activity curtailment driven by the fear of falling. 7 Although sensitivity and specificity in our study were influenced by level of disability (Figure 3), measuring the COP path in the OE condition may ensure an acceptable accuracy regardless of EDSS score. Lastly, the multivariate analysis clearly indicated that the risk of falls was increased in direct proportion to the extent of the COP path in the OE condition, irrespective of the other demographic and clinical variables.
Limitations
Limitations of the present study mainly concern the small sample size and the reliance on self-reported data; however, the prospective design and the collection of patient diaries should have improved the validity of our findings. 4 Although SSBMs of healthy controls in our study are comparable with those found in a previous report that used the same protocol, 10 the cutoff values for the SSBMs have not been established in the MS population. Furthermore, static posturography instruments may differ, thus precluding the possibility to generalize our results. Up to now, it is not well defined as to which time domain parameters of balance (eg, velocity, path, area) should be evaluated by static posturography. 28 A possible solution to standardize the static posturography assessment could be the Wii Balance Board (Nintendo, Kyoto, Japan). It has characteristics similar to the currently used force-platform, possesses very good test–retest reliability for the COP path, and has concurrent validity with a laboratory-grade force-platform. 29
Lastly, falls may be due to the sum of multiple impairments, which may not be detected by static posturography alone. 30 Indeed, falls are a common consequence of any neurological disease that induces a wide range of impairments.31-33
Conclusions
We suggest that static posturography may be used as a useful tool to select MS patients for rehabilitation interventions, such as traditional 34 and novel exercise-based training with torso weighting 12 or visuoproprioceptive training, 13 that may improve balance-related activities and reduce the risk of accidental falls.
Footnotes
Authors’ Note
This research was carried out using information collected during normal patient care, and extra time spent in data analyses and interpretation was part of the educational programs within the university.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.