
Abstract
Background. An understanding of the mechanical effects of botulinum toxin type A (BoNT A) on spastic and voluntary muscle contraction may help predict functional responders. Objective. To compare the effect of BoNT A on the voluntary and stretch reflex–related torques produced by activation of the rectus femoris (RF). Methods. This was a prospective open study where 15 incomplete spinal cord injury patients, impaired by a stiff-knee gait, with RF hyperactivity in mid-swing quantified by formal gait analysis (GA), were assessed before and after RF BoNT A injection (Botox, 200 UI). Main outcome measures included isokinetic peak torque (and angle at peak torque) at 0° (supine) and 90° (seated) during passive stretch (10 deg/s, 90 deg/s, and 150 deg/s), and voluntary contraction (60 deg/s) of the quadriceps. Secondary measures included impairment by Modified Tardieu Scale (MTS), peak knee flexion and spatial-temporal data by GA, activity (6-minute walking test, timed stair climbing), and discomfort (Verbal Rating Scale). Results. Voluntary torque decreased (−16%; P = .0004) but with only a trend toward a decrease in stretch reflex–related torque. The angle at spastic torque increased at 90 deg/s (+5°; P = .03), whereas MTS, peak knee flexion (+4°; P = .01), spatial-temporal data, timed stair climbing test (25%; P = .02), and discomfort were significantly improved. Conclusion. BoNT A appeared to delay the stretch-reflex angle at peak torque, whereas the voluntary torque decreased. After strict patient selection, BoNT A injection into the RF muscle led to improvements in impairment, activity, and discomfort.
Introduction
Spasticity has been defined by Lance 1 as “a motor disorder characterized by a velocity-dependent increase in tonic stretch reflex with exaggerated tendon jerks, resulting from hyperexcitability of the stretch-reflex.” It represents 1 aspect of the upper–motor neuron syndrome. 2 Spasticity can be useful in the presence of paresis but often leads to stiffness and hinders a weakened antagonistic muscle. Botulinum toxin type A (BoNT A) injection reduces resistance to passive movement caused by focal spasticity 3 and decreases spasticity-related muscle contraction4,5 by acting on the neuromuscular junction, but it can also reduce the force of the voluntary contraction, 6 which often must be preserved for the patient to maintain or gain some function. The functional benefit after BoNT A injection has been poorly demonstrated,3,7,8 partly because of methodological difficulties in assessing the multidimensional parameters implicated in function and activity. Furthermore, BoNT A may display a varying effect on spastic and volitional contraction depending on its concurrent action on extrafusal and intrafusal motor end plates.9,10
The precise mechanical impact of BoNT A injections on the stretch reflex and voluntary motor command is poorly understood. The clinical scales used in the literature (Ashworth and Tardieu) are not sensitive enough to quantitatively assess BoNT A’s effect on the stretch reflex. The Medical Research Council Scale (MRCS) also is not sensitive enough to assess the effect of this antispastic treatment on the voluntary motor control of injected muscles. For this reason, the authors evaluate the effect by isokinetic assessment, which is the gold standard tool for the quantified evaluation of the mechanical parameters of voluntary contraction.11,12 Its validity and reliability for spasticity assessment have been established.13-16
Spasticity of the rectus femoris (RF) is one of the main causes of stiff-knee gait (SKG) in patients with upper–motor neuron syndrome and leads to gait disabilities.17,18 SKG treatment with BoNT A has been effective on clinically assessed spasticity as well as certain parameters of the gait cycle (ie, knee flexion during the swing phase and gait velocity).19-21 However, data are lacking on the effect of BoNT A injections on peak voluntary and stretch reflex–related torque at the knee joint. The aim of this study was to assess the effect of BoNT A on peak voluntary and stretch reflex–related torque produced by the activation of knee extensor muscles in persons with incomplete spinal cord injury (SCI).
Methods
This prospective, open-label, single-center pilot study was conducted in a university hospital.
Participants and Inclusion Criteria
A total of 15 participants (14 men) aged 43 ± 15 years, who were “ASIA Impairment Scale-D” incomplete SCI patients with disabling SKG, were included. Injury levels were cervical (n = 7), thoracic (n = 7), and lumbar (n = 1). Posttraumatic delay was 10 years ± 10 months. To be eligible, they had to be able to walk on a treadmill, have no contraindications for BoNT A or previous injection, and have RF spasticity with a positive Ely test 22 , a Modified Tardieu Scale (MTS) grade ≥2 with hip at 0° flexion (and greater than the MTS grade measured in the flexed hip position to ensure the presence of RF spasticity), and RF spasticity > RF contracture (ie, MTS angle V3 < MTS angle V1).23,24 The final inclusion criterion, defined using a 3-dimensional quantified motion analysis, was a peak knee flexion less than 45° in the swing phase, associated with an inappropriate RF discharge in the midswing phase of gait. 20
Procedure and Measures
BoNT A treatment was provided using guided electric stimulation (Multistim sensor, Pajunk, Geisingen, Germany), and 200 units (Botox, Allergan, California) were distributed in 2 points at each site (n = 20 legs; 5 patients had bilateral injections). Patients were assessed before and 4 to 6 weeks after injection. The same physician performed all injections and assessments.
Isokinetic measures (Con-trex, Medimex, Ste-Foy-Les-Lyon, France)
A total of 5 repetitions of active (voluntary torque) and then passive (stretch reflex–related torque and angle at peak torque) extension-flexion movements of the knee were performed. The knee angle range that was tested was the active available amplitude for each patient (expressed in terms of the theoretical 0° extension). Two tests were conducted at a 2-day interval before the injection to increase measure reliability. 15 The maximum peak torque across repetitions was obtained for each leg. Voluntary torque production was recorded at a velocity of 60 deg/s during a concentric exercise with respect to the standard procedures 25 (joint alignment, contention, and position) and with active correction of gravity to avoid limitations because of weakness (minimum threshold torque = 1 N m). Patients were asked to exert a maximal effort across amplitude and repetitions, with verbal encouragement afterward.
The stretch reflex–related torque was recorded during passive movements after 5 minutes of rest. Patients were verbally informed of the start of the passive movements. The knee was held for 0.1 s before moving in the opposite direction. The maximum peak torque was registered at 3 velocities (10 deg/s, 90 deg/s, and 150 deg/s). These were chosen to verify Lance’s definition of spasticity and to differentiate elastic (10 deg/s) and reflex (90 deg/s and 150 deg/s) resistance to passive movement. The “peak spastic torque” was defined as the difference between the peak torques at the high velocities (90 deg/s and 150 deg/s) and at the low velocity (10 deg/s). 16 The role of RF in relation to quadriceps spasticity was tested by 2 hip positions (0°, in supine position, and 90°, sitting). We hypothesized that there would be a strong effect of hip extension (0°), in which the RF is lengthened. RF peak spastic torque was defined as the difference between peak spastic torque values for these 2 hip positions.
Clinical measures
MTS with stretch-reflex grade (0 to 4) and angle (0° to 150°) was recorded for 2 hip positions (extended and flexed). An 11-point Verbal Rating Scale (VRS) was used for the self-assessment of primary and secondary discomfort caused by quadriceps spasticity in a list of daily walking and standing tasks.
The 6-minute walking test was performed at the patients’ preferred velocity. 26 The time taken to ascend and descend thirteen 12-cm-high stairs was called the timed stair climbing test and was recorded in a standardized manner, derived from Wade. 27
Gait Analysis (GA)
Gait was analyzed using a 6-camera optoelectronic motion capture system (Motion Analysis Corporation, California; sampling frequency: 100 Hz). The trajectories of 29 markers placed on anatomic landmarks using the Helen Hayes marker set 28 were collected and filtered using a fourth-order zero-lag Butterworth low-pass filter with a 6-Hz cutoff frequency. The same investigator placed the markers at all sessions. At each session, a minimum of 10 gait cycles were averaged from each limb. GA for participants was obtained at their preferred walking speed along a 15-m stretch of walkway. Surface electromyography (Motion Lab Systems, MA 311; sampling frequency: 1000 Hz) was recorded during kinematic data collection using bipolar electrodes placed on the RF, vastus lateralis, hamstring medial, tibialis anterior, soleus, and gastrocnemius medialis at specific sites (SENIAM recommendations). 29 Electromyographic data were analyzed qualitatively to determine RF activity periods.
Statistical Analyses
Means and standard deviations were calculated for each variable, with n = 15 patients for VRS and functional tests and n = 20 legs for all other data. Differences in quantitative data between conditions (velocity, hip position, and pre/post BoNT A) were analyzed using a Wilcoxon signed-rank test. Statview 5.0 software (SAS Institute Inc,) was used, and P < .05 was considered statistically significant.
This prospective observational study was granted approval by an institutional human research review board (Comité de Protection des Personnes/Ile de France-VIII, 92100 Boulogne-Billancourt).
Results
Verification of Clinical and Methodological Hypotheses
A statistically significant effect for stretch velocity and hip position on peak spastic torque was found, both before and after BoNT A injection, validating the clinical hypothesis (Table 1 for pre-BoNT A).
Effect of Velocity and Hip Positions on Peak Spastic Torque Before BoNT A Treatment
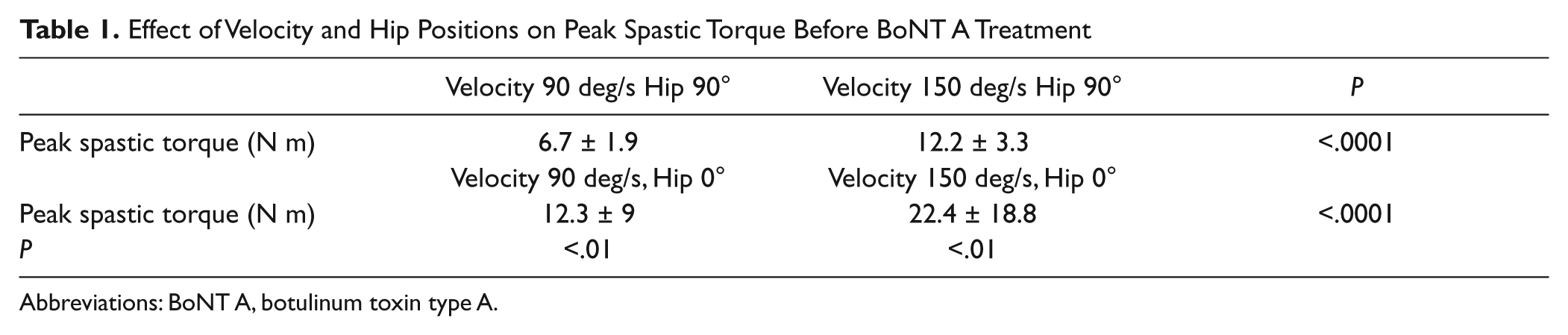
Abbreviations: BoNT A, botulinum toxin type A.
Main Outcome Measures
After BoNT A injection, there was a statistically significant decrease in the peak voluntary torque produced by the quadriceps (−16%, P = .0004; Figure 1), whereas only a tendency toward RF peak spastic torque decrease was found (10.2 vs 6.4 N m at 150 deg/s, P = .47; 5.6 vs 5.5 N m at 90 deg/s, P = .3). A statistically significant increase in the stretch reflex angle at peak torque appeared in hip extended position at 90 deg/s (+5°, P = .03; Figure 2), whereas the angle of peak spastic torque increased not significantly at 150 deg/s (+4°, P = .08). Regardless of the conditions during isokinetic tests, there was no statistical difference related to start angles (29.7° ± 13° to 31° ± 15° in the hip flexed position, P = .3; 30.5° ± 15° to 31.3° ± 16° in the hip extended position, P = .1) and knee range of motion (61° ± 21° to 58° ± 20° in the hip flexed position; 55.1° ± 19° to 54.2° ± 19° in the hip extended position).
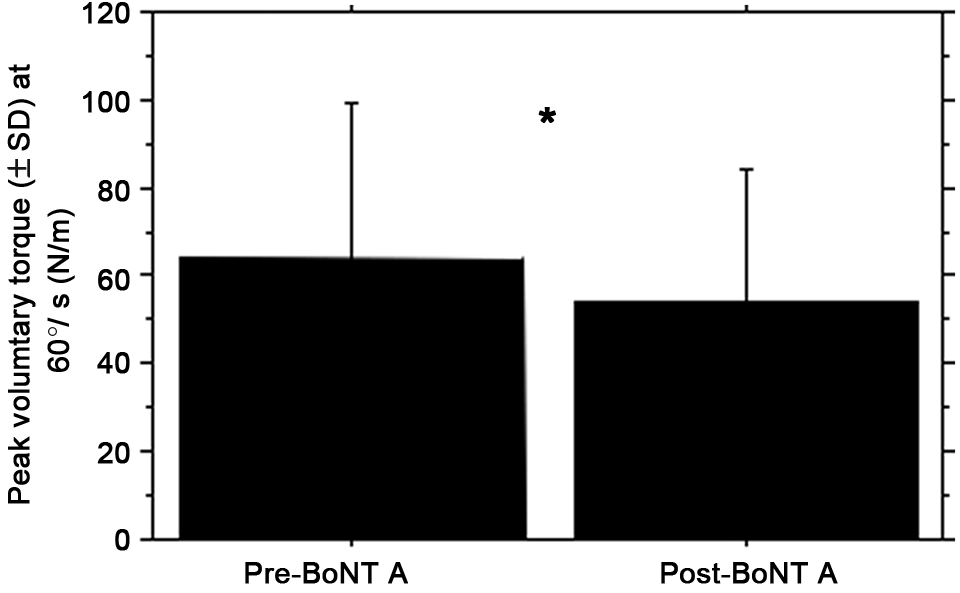
BoNT A effect on peak voluntary torque of the quadriceps. Abbreviations: BoNT A, botulinum toxin type A; SD, standard deviation. *P < .001.
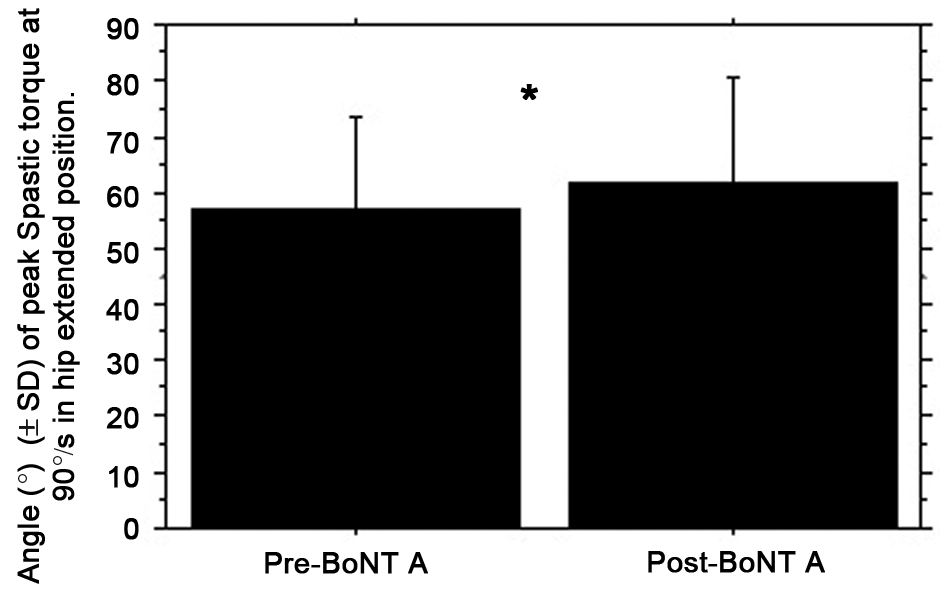
BoNT A effect on stretch-reflex angle at peak spastic torque of the quadriceps. Abbreviations: BoNT A, botulinum toxin type A; SD, standard deviation. *P < .05.
Secondary Outcome Measures
Impairments (Table 2)
Values for clinically or instrumentally assessed impairment parameters improved in the injected leg: MTS grade and angle in the hip-extended position only, peak knee flexion in the swing phase, and knee flexion velocity at toe-off improved. No statistically significant results were found in noninjected legs.
Improvement of Clinically and Instrumentally Assessed Impairments After BoNT A Treatment
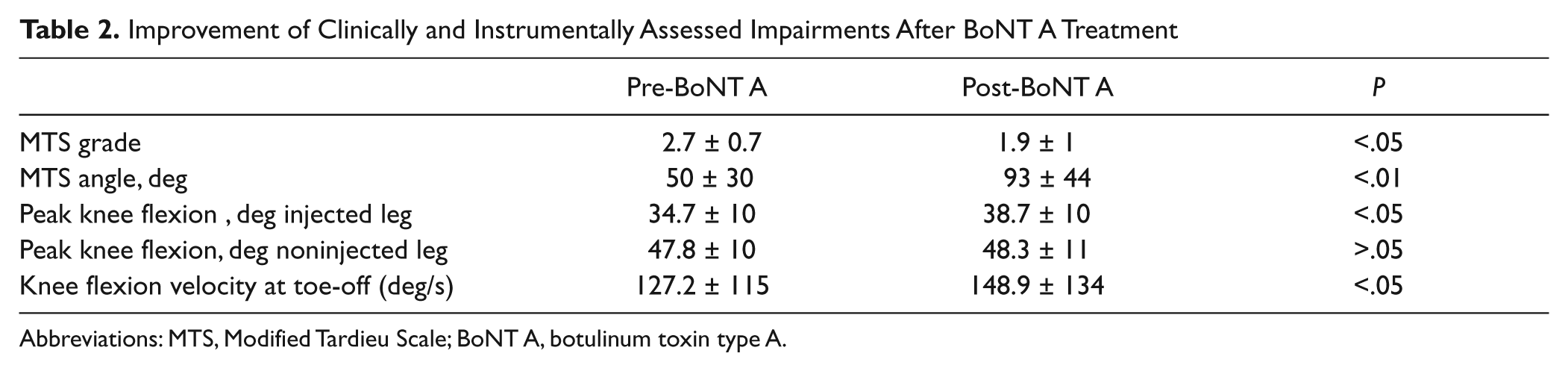
Abbreviations: MTS, Modified Tardieu Scale; BoNT A, botulinum toxin type A.
Activity (Table 3)
Gait spatial-temporal parameters significantly increased (gait velocity, stride and step length, and swing phase proportion). In functional tasks, the timed stair test was significantly improved by 25% without change in the 6-minute walking test.
Improvement of Spatial-Temporal and Functional Gait Abilities After BoNT A Treatment
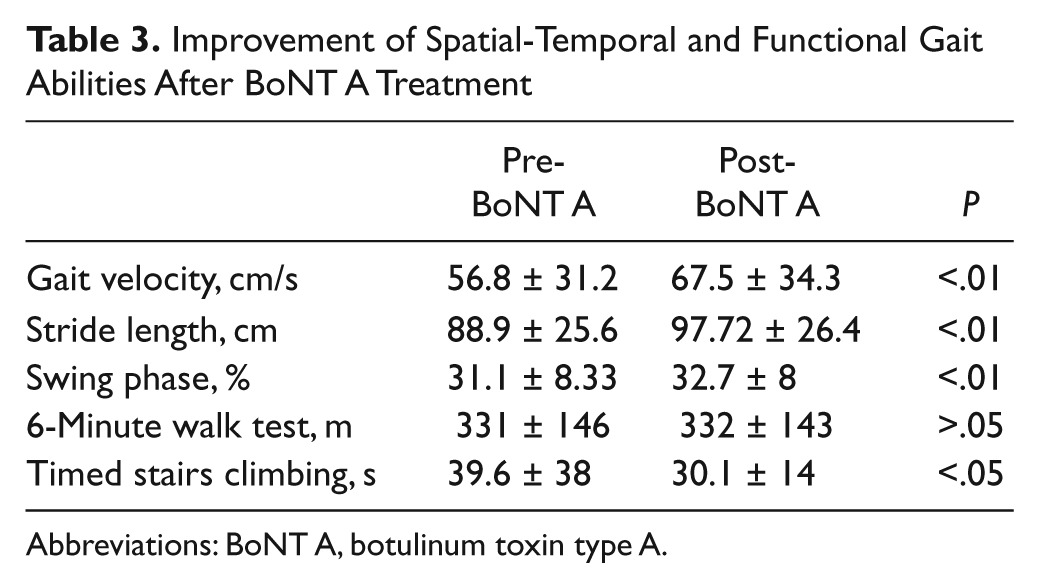
Abbreviations: BoNT A, botulinum toxin type A.
Satisfaction
Patients’ discomfort with daily walking and standing tasks decreased after BoNT A (main discomfort VRS from 6.3 ± 1.2 to 4.1 ± 1.7; P = .001).
Discussion
BoNT A injected into the RF muscle of ambulatory patients with incomplete SCI and SKG led to improvements in impairments, functional aspects of gait, and discomfort. The RF muscle was highly implicated in quadriceps spasticity, doubling the peak spastic torque with the hip extended compared with the hip flexed, at both velocities. Even so, hip sensory afferent feedback from the ipsilateral and contralateral hip is known to adjust the ipsilateral soleus H-reflex, 30 and heteronymous muscle afferents also could have increased quadriceps spasticity in the hip extended position.
The effect of BoNT A was greater on the isokinetic angle at which peak spastic torque occurred in the hip extended position at 90 deg/s (the angle increased) than on the peak spastic torque itself (which only tended to decrease). The increase of angle at peak spastic torque at 150 deg/s (+4°) was similar to the one at 90 deg/s (+5°) and close to statistical significance (P = .08), so that the small sample size could explain this lack of a statistical result. This could indicate that fusimotor synapses became less excitable, with a delayed Ia afferent response, despite a theoretical low tonic Ia discharge at rest. 31 Electrophysiological studies comparing the tonic vibration reflex and M-wave before and after BoNT A injection support the intrafusal effect of BoNT A with afferent modifications.9,10 Other positive effects of modified afferent information after BoNT A on cerebral activity have been found in poststroke patients. 32
The 16% decrease in the voluntary torque produced by activation of the quadriceps is lower than the values found in the literature 6 (−40% in the flexor digitorum of poststroke patients). This can be explained by the fact that RF is only a part of the quadriceps and is probably not the primary portion in terms of strength. Thus, we found a 16% decrease versus an expected maximum 25% (4 heads) decrease in voluntary torque. Furthermore, even at high doses, BoNT A does not block the entire neuromuscular junction. Regardless, no patient had knee extension weakness, whereas 3 patients reported hip flexion weakness. Even if the mean hip flexion velocity at toe-off was significantly increased in this study (not shown), it seems that the hip flexor weakness (≤2/5 MRCS) could be a contraindication to RF BoNT A injection in some cases (ie, responsibility of other quadriceps muscles and other causes of SKG).
It was surprising that peak spastic torque did not decrease significantly, whereas voluntary torque did. If not a result of the small sample size, this could be a result of the fact that Ib/II nerve endings inhibit the spastic contraction, whereas the stretch continues at the same velocity—described as the “clasp knife phenomenon” by Burke. 33 As the Ib/II threshold does not vary, a decrease in available α units should induce a delay to produce the peak at which Ib/II discharge appears, leading to an increase in the angle at peak torque without changing the peak itself. However, the exact distribution of BoNT on α and γ end plates is still underrated, and future studies on the mechanical effect of BoNT A should compare spasticity at rest, both with and without minimal eccentric voluntary contractions, to be able to assess the α-γ coactivation and, thus, the γ effect.
Spasticity, SKG, and Gait Improvement
The statistically significant decrease in MTS grade was less than 1 point, which does not seem to be clinically relevant. In contrast, the MTS angle changed substantially (from 50° onset to 93°) and was correlated with the increase in the isokinetic angle at peak spastic torque in hip extended positions. This angle increased by 5°, which could correspond with the 4° increase in peak knee flexion recorded during the GA. This amount of increase (+4°) in peak knee flexion during the swing phase was not found for the noninjected leg (+0.5°, NS) and is similar to other results found in poststroke patients: +5° for Caty et al 19 and +8° for Robertson et al. 20 The clinical relevance of these small analytical results could be questioned; however, even a small increase in peak knee flexion during the swing phase could lead to a consistent improvement in step clearance (calculated with trigonometric rules, as derived from leg length × sin α), as Gage 34 found after surgery on cerebral palsy patients presenting with SKG. For example, an increase of +5° in peak knee flexion for a man with a leg length of 0.5 m can theoretically increase the step clearance by more than 2 cm. This could explain the functional improvement in the stair-climbing task in the present study, with a 25% decrease in the time taken to ascend and descend stairs. A small improvement in step clearance could provide a functional improvement in stair climbing, whereas the 6-minute walking test results remained unchanged. No strong predictive factors could be found, although the peak voluntary/spastic torque ratio before BoNT A seemed interesting and should be assessed in a larger sample. 35
Study Limitations
The primary limitation of this study is the small sample size. However, the homogeneous population and the strict inclusion criteria for RF spasticity and SKG characteristics give support to the findings. The open-label design of the study could allow bias, but we did not intend to assess the effectiveness of BoNT A in treating spasticity. Regarding the mechanical consequences of the stretch reflex, the use of an isokinetic device has many advantages. The main one is the constant velocity, although parameters must be chosen carefully to reach an isokinetic velocity as soon as possible during the movement, to ensure isokinetic movement with an adequate range of motion in these spastic populations. The first and last 10° of the movement are usually not isokinetic because of acceleration and deceleration onset. This needs to be specified and improved by the manufacturers.
To our knowledge, no other study has assessed the effect of BoNT A on SKG in SCI patients.
Conclusion
BoNT A seemed to delay the angle of peak spastic torque, whereas the voluntary force decreased. This increase of angle at peak spastic torque could be a circumstantial effect of a decrease in α units, whereas the Ib/II inhibition threshold remained constant during isokinetic stretching. In this study, after strict patient selection, BoNT A injection into the RF muscle in incomplete SCI patients led to improvements in impairments, functional aspects of gait, and discomfort.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.