
Abstract
Background. Sitting balance and the ability to perform selective truncal movements are important predictors of functional outcome after stroke. However, few clinical trials have evaluated the effect of truncal exercises. Objective. The authors assessed the effect of additional truncal exercises on truncal function, standing balance, and mobility. Methods. An assessor-blinded randomized controlled trial was carried out at a stroke rehabilitation hospital. A total of 33 participants (mean 35 days post onset) were randomly assigned to an experimental group (n = 18) or a control group (n = 15). In addition to conventional therapy, the experimental group received 16 hours of truncal exercises. The control group received 16 hours of sham treatment. Truncal function was evaluated by the Trunk Impairment Scale (TIS) and standing balance and mobility by the Tinetti Test. The Romberg with eyes open and eyes closed, Four Test Balance Scale (FTBS), Berg Balance Scale (BBS), Rivermead Motor Assessment Battery (RMAB), Functional Ambulation Categories, and Dynamic Gait Index (DGI) were performed to elucidate the findings of the primary outcome measures. Results. A treatment effect was found for the experimental group on the TIS (P < .001), Tinetti Test (P < .001), FTBS (P = .014), BBS (P = .007), RMAB (P < .001), and DGI (P = .006). Conclusions. In addition to conventional therapy, truncal exercises have a beneficial effect on truncal function, standing balance, and mobility in people after stroke.
Introduction
Postural disturbances in patients with hemiplegia are common and limit the recovery of gait and functional independence.1,2 Many approaches include balance training using visual feedback,3,4 task-oriented exercises, 5 and treadmill training 6 to retrain postural control because a key to successful rehabilitation includes regaining adaptive truncal stability. 7 Verheyden et al 8 showed a relationship between trunk performance and measures of balance, gait, and functional ability after stroke. Muscles of the trunk have a supportive role both during bilateral stance and when seated. They stabilize proximal body segments during voluntary movements of the extremities. 8 Furthermore, trunk muscle strength was related to the score on the Berg Balance Scale (BBS) at discharge. 9 Truncal function may predict functional outcome in people recovering from stroke. 10 Indeed, the Trunk Impairment Scale (TIS) on patient admission and its static sitting balance subscale were stronger predictors of the Barthel Index score at 6 months than the Barthel Index score itself on admission. 10 These findings suggest that if trunk performance could be improved early in the rehabilitation process, better functional improvement after stroke might be expected.
Studies that investigated truncal function after stroke and in matched control participants using either a hand-held dynamometer11-13 or electromyograph14,15 found that trunk muscle strength was impaired after stroke during activities such as lateral flexion, rotation, and flexion-extension. Furthermore, the cross-sectional diameter of paravertebral muscles differed significantly between the hemiplegic and the nonhemiplegic side. 16 Trunk impairments were reflected by the reduced activity level of the lateral trunk muscles, in delayed onset of and in reduced synchronization between activation of pertinent muscular pairs. 17 In addition to these impairments, altered trunk position sense has been demonstrated. 18
Only a few rehabilitation studies have been reported. Dean et al 19 showed a beneficial effect of practicing reaching tasks beyond arms’ length on sitting ability, reaching, and standing up. Indeed, 6 months after stroke, participants in the experimental group treated early after stroke significantly increased their maximum reach distance and peak vertical force through the affected foot when standing up. In contrast, no effect was observed on ambulation measured with the 10-m Walk Test. Dursun et al 20 investigated the effect of an angular biofeedback device in patients with impaired sitting balance after stroke. The average mean period to achieve sitting balance was significantly shorter than in patients receiving conventional therapy. Further promising results were found when retraining voluntary trunk movement was coupled to the execution of exploratory tasks. 21 Verheyden et al 22 investigated the effect of additional exercises on truncal function after stroke. These exercises improved the performance of the dynamic sitting balance subscale of the TIS, indicative for selective lateral flexion initiated both from the upper and lower part of the trunk, in the experimental group when compared with the control group. To the best of our knowledge, no transfer effect of truncal exercises has been described on standing balance and mobility.
We assessed the effect of additional trunk exercises on truncal function. In addition, we investigate whether these truncal exercises result in improved standing balance and mobility.
Methods
Patients
Patients were recruited from the stroke population of the rehabilitation hospital Hof Ter Schelde between November 2008 and May 2009. All patients with a history of first stroke attending a rehabilitation program were eligible for inclusion. Exclusion criteria were age 85 years and older, more than 4 months postonset, acute low back pain, and orthopedic and neurological disorders that could influence postural control. Furthermore, patients suffering from communication disorders that interfered with the protocol were excluded. Patients included suffered a single, hemispheric lesion. Patients suffering from brainstem, cerebellar, and multiple lesions were excluded. After confirming the definite diagnosis of stroke based on computed tomography and/or magnetic resonance imaging scans, information on patients’ age, days poststroke, and side and location of the lesion were collected. Patients had to have completed at least 75% of training sessions to be included in the analysis. Participants were asked to sign an informed consent before participation. Approval was given by the ethics committee.
Design
This study was an assessor-blinded, randomized, controlled trial. The number of patients required for this study was calculated a priori to ensure sufficient statistical power. This revealed that a sample size of 19 patients in each group was necessary to achieve an 80% chance (power = 0.80) of detecting a 10% difference in improvement between the 2 groups on the TIS. Furthermore, 20 patients in each group were required for the Tinetti Test. Patients were randomly allocated to either an experimental group or a control group. Because the duration of the study was limited in time as a result of funding limits, only 33 patients were included. For assigning patients to one of both groups, the authors made use of 40 concealed envelopes (20 envelopes for each group), which were randomized by an independent person.
Both groups received multidisciplinary conventional physical and occupational therapy as provided by the rehabilitation staff, mainly focused on neurodevelopmental treatments. This treatment concept is a problem-solving approach in which the trunk is an essential component.7,23 In clinical practice, activities of the trunk are integrated in postural control and task-directed movement. In addition to conventional therapy, patients received training to improve truncal function (experimental group) or exercises for the upper limb (control group). Both groups received 16 hours of additional training over 8 weeks (30 minutes, 4 times a week). This amount of additional therapy is based on a meta-analysis about augmented exercises training to improve ADLs or gait. 24
Intervention
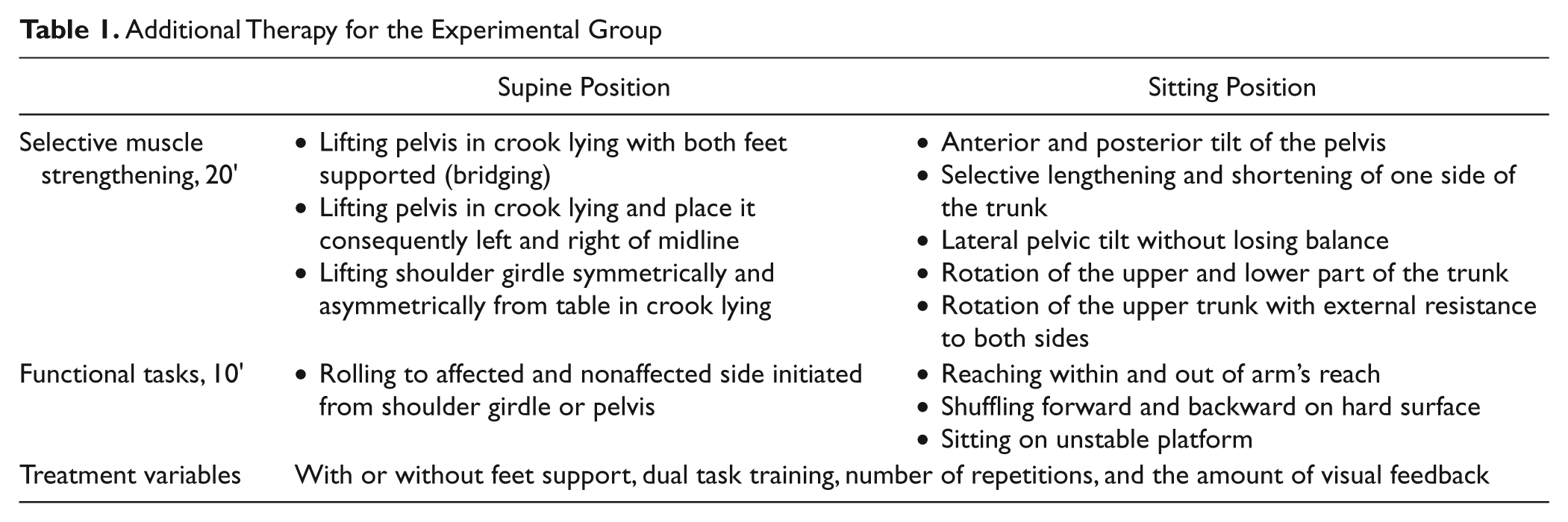
The additional training for the experimental group focused on trunk muscle strength, coordination, and selective movements of the trunk (Table 1). Patients of the control group received passive mobilization of the upper limb and transcutaneous electrical nerve stimulation of the hemiplegic shoulder while supine. A small group of trained therapists delivered the same protocol in order to reduce variability in treatment. All therapists were randomly assigned to a patient. The conventional therapist for that patient was blinded for the experimental intervention. Progression was based on the patients’ level of performance.
Additional Therapy for the Experimental Group
Outcome Measures
Patient characteristics such as age, sex, side of lesion, type and onset of stroke, and comorbidities were registered. The patients were evaluated before and after the intervention. Clinical evaluations were performed by an independent assessor who was blinded to group assignment and not involved in treatment. The TIS and Tinetti Test, with their subscales, were primary outcome measures to assess the effect of the truncal exercises on truncal function, standing balance, and mobility. Secondary outcome measures were introduced to elucidate the results of the primary outcome measures.
The TIS consists of 3 subscales of static and dynamic sitting balance and trunk coordination, scored up to 7, 10, and 6 points, respectively. 25 The static sitting balance subscale assesses whether a person can sit independently and remain seated when the legs are either passively or actively crossed. The dynamic sitting balance subscale evaluates the ability to actively shorten each side of the trunk, first initiated from the shoulder and subsequently initiated from the pelvic girdle. Trunk coordination tests the ability to independently rotate the shoulder girdle and pelvic girdle. The total TIS scores range between 0 and 23 points, where a higher score indicates better truncal function. Reliability, validity, measurement error, and internal consistency of the TIS for stroke patients have been reported.8,10,25 The Tinetti Test measures gait and balance on a 3-point ordinal scale ranging from 0 (impaired) to 2 (independent). 26 The maximum score for the gait and balance components are 12 and 16 points, or a maximum of 28 points.
For the Romberg test, participants were instructed to stand for a maximum of 30 s with their feet together, first with eyes open, followed by the same exercise with closed eyes. 27 The Four Test Balance Scale (FTBS) includes 4 timed static balance tasks of increasing difficulty without the use of assistive devices, 28 parallel stance, semitandem stance, tandem stance, and single-leg stance. Each position must be held for 10 s before the person progresses to the next. Timing is stopped if the person moves the feet from the proper position or the assessor provides contact to prevent a fall. The BBS includes14 tasks that require balance, such as sitting, standing, leaning over, and stepping. 29 Overall scores range from 0 (severely impaired balance) to 56 (excellent balance). The Dynamic Gait Index (DGI) includes 8 gait tasks, including walking on a level surface, walking at different speeds, performing head turns in the pitch and yaw planes while walking, stepping over and around objects, and stair climbing. 30 The test items are scored on a 4-point scale, from 0 to 3. The maximum score of 24 indicates normal performance. The Functional Ambulation Categories (FACs) range from 0 (unable to walk) to 5 (independent indoor and outdoor walking). 31 The Rivermead Motor Assessment Battery (RMAB) includes the Leg and Trunk subscale with 10 items, such as flexing the knee in a weight-bearing position. 32 Each item is coded 0 (fail) or 1 (pass), depending on whether the participant completes the activity according to specific instructions.
Statistical Analysis
Descriptive data analysis was performed for the collected variables of the participants. Patients’ characteristics measured on a continuous scale were examined by the Kolmogorov-Smirnov test to evaluate normal data distribution.
To examine the effect of our randomization procedure, differences between all variables for the experimental and control groups were evaluated by means of an independent t test or χ2 test for continuous or dichotomous data, respectively. Parametric statistics were used to analyze the normally distributed data.
To analyze the results, a general linear repeated-measures model was used. The pretreatment and posttreatment results were entered as within-subjects variable “time,” and the experimental and control groups were included as between-subjects factor “condition.” Probability values for the variable time would indicate whether there is a significant change between pretreatment and posttreatment assessment. A significant interaction of Time × Condition would mean that the change between pretreatment and posttreatment evaluation is significantly different between both groups. Probability values for the TIS and the Tinetti with their subscales were Bonferroni corrected. The significance level, then, was set at P < .007 for the primary outcome measures shown in Table 2. Secondary outcome measures were not corrected for multiple testing with a significance level of P < .05. A post hoc power calculation was performed together with the determination of the effect size and numbers needed to treat based on the assumption of 10% improvement. SPSS 15.0 and Sigmastat 12.0 were used for the statistical analysis.
Outcome Measures in the Experimental and Control Group a
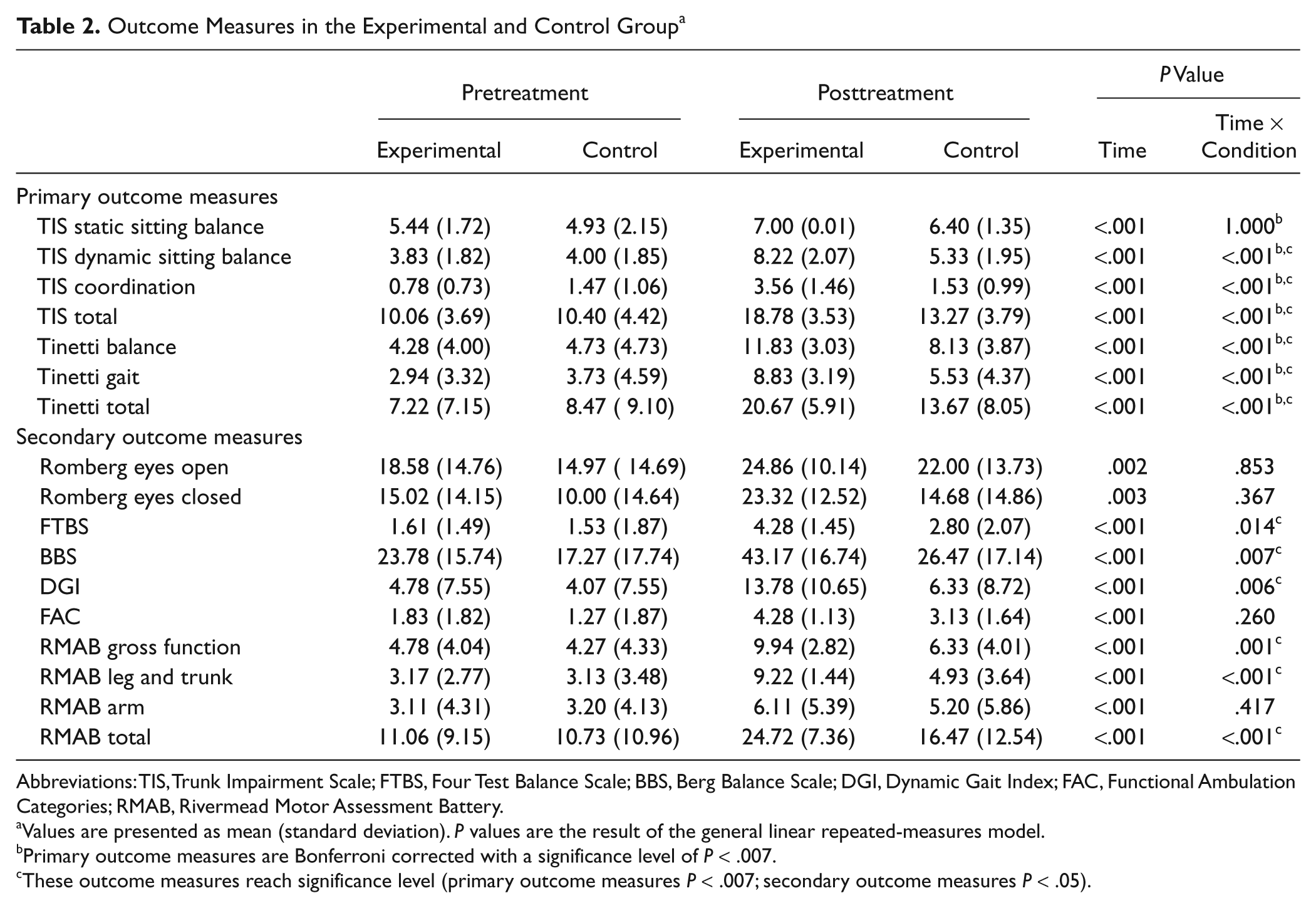
Abbreviations: TIS, Trunk Impairment Scale; FTBS, Four Test Balance Scale; BBS, Berg Balance Scale; DGI, Dynamic Gait Index; FAC, Functional Ambulation Categories; RMAB, Rivermead Motor Assessment Battery.
Values are presented as mean (standard deviation). P values are the result of the general linear repeated-measures model.
Primary outcome measures are Bonferroni corrected with a significance level of P < .007.
These outcome measures reach significance level (primary outcome measures P < .007; secondary outcome measures P < .05).
Results
A total of 15 control group and 18 experimental group participants were included in the analysis. One patient in the experimental group was discharged after completing 24 of 32 training sessions but was still included in the analysis. In Figure 1, we show the flow diagram for the study.
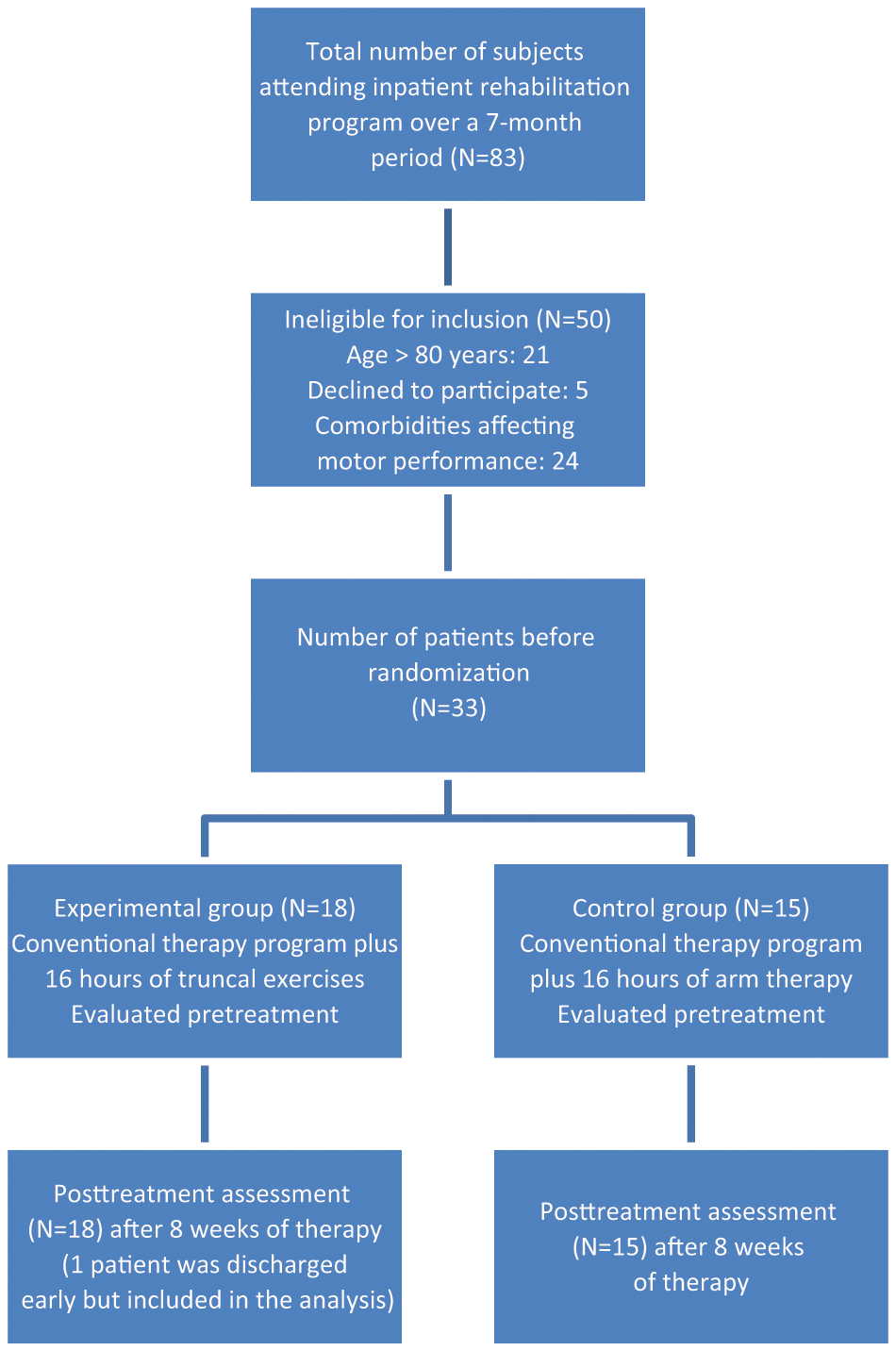
Flow diagram for participant assignment in this study.
Characteristics of both groups are presented in Table 3. No differences were found between the 2 groups for the collected demographic variables, stroke-related parameters, and pretreatment outcome measures.
Characteristics of Both Groups a
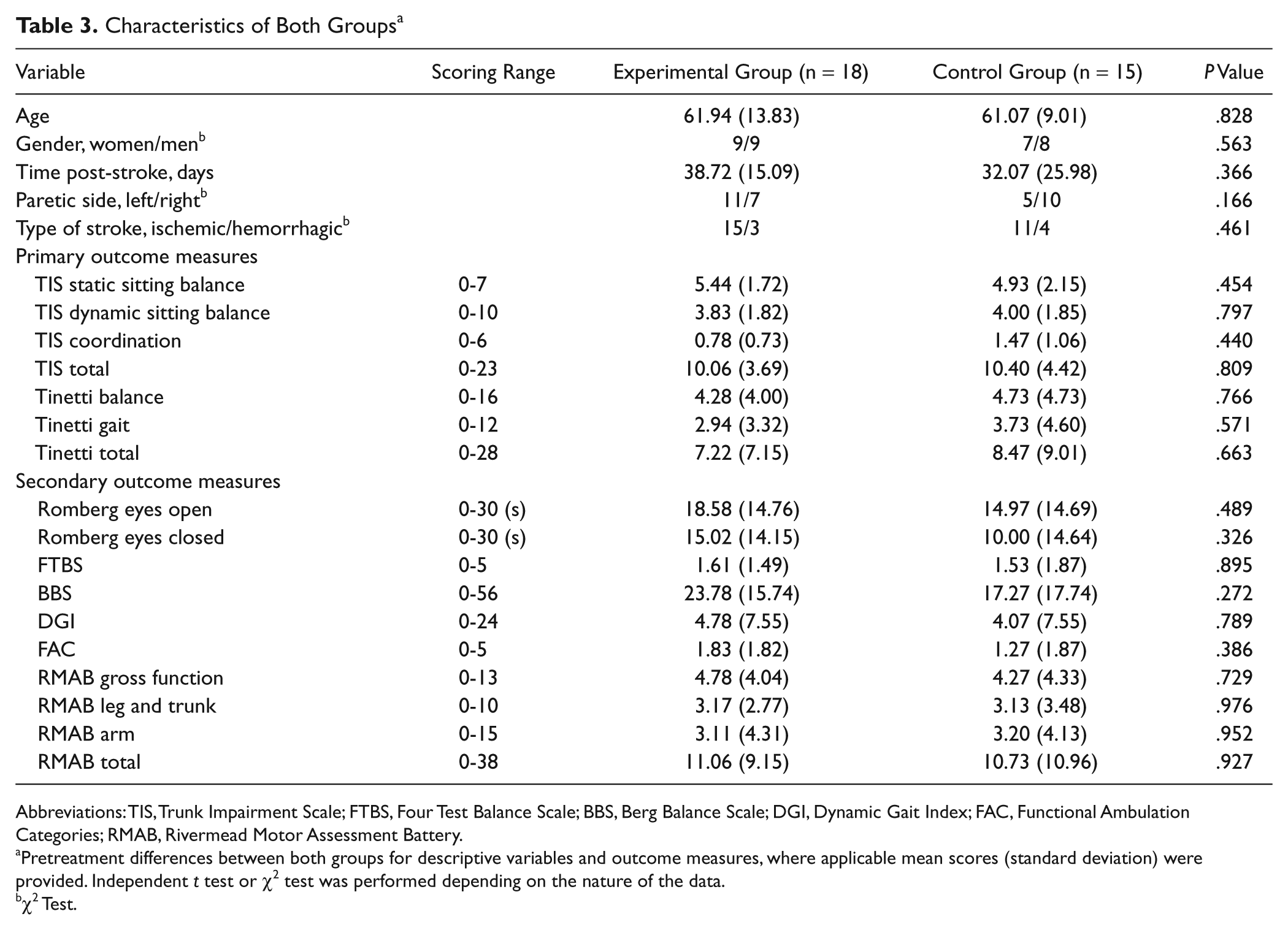
Abbreviations: TIS, Trunk Impairment Scale; FTBS, Four Test Balance Scale; BBS, Berg Balance Scale; DGI, Dynamic Gait Index; FAC, Functional Ambulation Categories; RMAB, Rivermead Motor Assessment Battery.
Pretreatment differences between both groups for descriptive variables and outcome measures, where applicable mean scores (standard deviation) were provided. Independent t test or χ2 test was performed depending on the nature of the data.
χ2 Test.
Both groups improved significantly on all outcome measures during the 8 weeks between pretreatment and posttreatment assessment. The Time × Condition effect was significant for all outcome measures and subscores, with the exception of the Romberg with eyes open and eyes closed (P = .853 and P = .367, respectively), the FAC (P = .260), the arm section of the RMAB (P = .417), and the static sitting balance subscale of the TIS (P = .869). These results are summarized in Table 2. A significant Time × Condition effect was observed each time a strong effect size (>0.80) 33 and a power above 0.80 was shown, except on the FTBS (Power = 0.72). The numbers needed to treat were small, ranging from 1.48 to 4.74, for all outcome measures with a significant Time × Condition effect (Table 4).
Post hoc Calculations
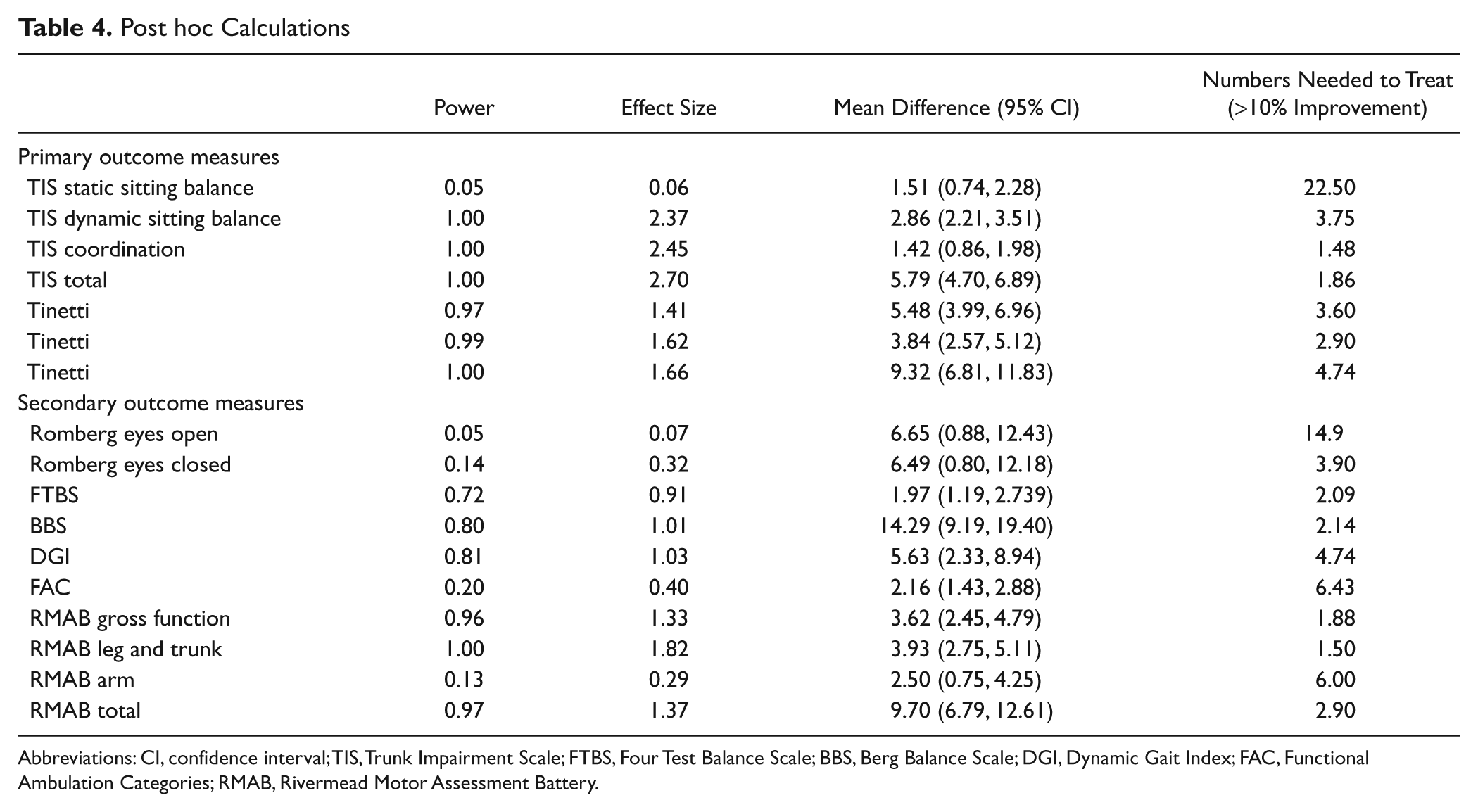
Abbreviations: CI, confidence interval; TIS, Trunk Impairment Scale; FTBS, Four Test Balance Scale; BBS, Berg Balance Scale; DGI, Dynamic Gait Index; FAC, Functional Ambulation Categories; RMAB, Rivermead Motor Assessment Battery.
Discussion
We found that 16 hours of additional exercises aiming to improve truncal function increased dynamic sitting balance and improved truncal coordination. Furthermore, this study shows that truncal function augments postural control during standing balance and mobility. This indicates the importance of truncal exercises in the rehabilitation of stroke patients.
Our results are consistent with other studies showing that therapy primarily induces treatment effects on the abilities at which training is specifically aimed.22,34 When compared with the study of Verheyden et al, 22 our findings demonstrate a therapeutic effect on the dynamic subscale as well as the more complex items of the coordination subscale of the TIS. This higher level of truncal function may be explained by the 16 hours instead of 10 hours of exercises and the type of exercises provided in our study. 24
Additional truncal exercises also transferred to improved standing balance and ambulation. This finding may be explained by exercise implemented as soon as possible in functional tasks such as rolling and reaching (Table 1). Newly gained functions must be incorporated in functional exercises to enable an efficient motor strategy. 35 Furthermore, all patients received conventional treatment. Therapists involved in the implementation of individualized conventional treatment, unaware of patient allocation, immediately implemented gains in truncal activity into a broader functional context. The experimental group, which improved faster in truncal function, could start earlier with complex gait and balance tasks. In addition, truncal stability is an essential core component of balance and coordinated extremity use in daily functional activities and the performance of higher level motor tasks.7,10 Evidence supports the provision of a restraining support to the trunk, which allows for a greater excursion of upper-limb movement and improves interjoint coordination, because of the stabilization of truncal components.36-39 A large portion of the additional therapy focused on selective muscle strengthening, such as lifting the pelvis or the shoulder girdle and rotating the upper trunk with external resistance; all improve strength of both abdominal and back muscles. Another key component of truncal stability is trunk position sense40-42 and feed-forward anticipatory postural adjustments, which the exercises helped enable.43-46
Limitations
The tests that assessed the ability to perform the more demanding tasks, such as the Tinetti, BBS, DGI, RMAB, and FTBS, were the only outcome variables that discriminated between both groups. The number of participants was rather small, although the post hoc analyses showed enough power for all outcome measures that had a significant Time × Condition effect. Additionally, the present study did not investigate long-term effects of the truncal exercises.
Conclusion
It was found that 16 hours of specific truncal exercises, in addition to conventional therapy, can benefit truncal function in people with stroke. In addition, these exercises have a transfer effect on standing balance and ambulation. Further development of task-specific and well-defined interventions should be encouraged.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.