
Abstract
Background. In line with patient-centered health care, it is necessary to understand patients’ perceptions of health. How stroke survivors perceive their health at different time points after stroke and which factors are associated with these feelings provide important information about relevant rehabilitation targets. Objective. This study aimed to identify the independent factors of health-related quality of life (HRQoL) from a biopsychosocial perspective using the methods of multivariate regression at 3 different time points poststroke. Methods. Included in the study were 99 patients from stroke units with diagnosed first-ever stroke. At admission and at 6 weeks, 3 months, and 1 year poststroke, HRQoL was assessed using the EuroQoL-5D Visual Analogue Scale (EQ-5D VAS). Consequences in Body Functions and Activities and Participation, and Environmental Factors were documented using 155 categories of the International Classification of Functioning, Disability and Health (ICF) Core Set for Stroke. Results. For a period of 1 year, problems with recreation and leisure, personality functions, energy and drive functions, and gait pattern functions were repeatedly associated with worse HRQoL. Whereas Body Functions and Activities and Participation explained more than three-fourths of the variances of HRQoL at 6 weeks and 3 months (R2 = 0.80-0.93), the variation at 1 year was best explained by either Body Functions or Environmental Factors (R2 = 0.51). Conclusions. The results indicate the importance of Body Functions and Activities and Participation (mainly personality functions and recreation and leisure) on HRQoL within 3 months poststroke, but increased impact of Environmental Factors on HRQoL at 1 year.
Introduction
An important outcome of rehabilitation, in particular in rehabilitation of health conditions with chronic course such as stroke, is health-related quality of life (HRQoL). 1 HRQoL is the health-related subset of quality of life (QoL) that is defined as “individual’s perception of their position in life in the context of the culture and value system in which they live and in relation to their goals, expectations, standards and concerns” (p.153).2,3 In line with patient-centered health care, it is necessary to understand patients’ perceptions of health and their individual concepts of disability.1,4 How stroke survivors perceive their health at different time points after stroke and which factors are associated with these feelings provide important information about relevant rehabilitation targets. With this knowledge, stroke recovery may be increased by delivering patient-centered care and service adapted to the different stages of the lifelong rehabilitation course. 1
Recent years have seen a growing number of articles on HRQoL in stroke literature. 5 Trying to identify factors and predictors of HRQoL, many studies consider either disease-specific and demographic characteristics or use total scores of functional status. However, to be able to identify relevant intervention targets, it is important to have information about the single factors associated with HRQoL. 6 A review on determinants of HRQoL after stroke by Carod-Artal and Egido 5 showed that there is a complex network of factors influencing an individual’s adjustment to life—for example, social background, neurological impairment, disability, cognition, mood, coping styles, social support, and so on. Without doubt, HRQoL is a complex concept with many dimensions. Instead of summarizing the results of different studies, we were interested in considering all those various biopsychosocial dimensions of health simultaneously with the possibility of adjusting for the different aspects.
A comprehensive framework that can be useful to describe the many single factors of functioning and disability is the International Classification of Functioning, Disability and Health (ICF) from the World Health Organization. 7 It provides a common terminology of health and functioning that is understandable for different health professionals and aims to be more complete than tools used at present.8,9 The ICF, more specifically the ICF Core Set for Stroke, contains a number of 166 ICF categories potentially relevant for persons with stroke comprising body functions, structures, activities and participation, and environmental factors.10,11 With this ICF Core Set it becomes possible to account for the multidimensional complexity of HRQoL in a novel comprehensive way.
The objective of this study was to use the ICF Core Set for Stroke to identify the factors of HRQoL from a comprehensive biopsychosocial perspective and to study whether those factors are different at 6 weeks, 3 months, and 1 year poststroke. The specific aims were (1) to identify relevant Body Functions, Activities and Participation, and Environmental Factors that positively or negatively influence HRQoL at the different time points and (2) to identify independent factors of HRQoL at each time point considering the biopsychosocial factors of disability together.
Methods
Participants
The study was designed as a cohort study with 120 participants. The inclusion criteria were a diagnosed first-ever stroke, age of at least 18 years, and written informed consent. Patients with a diagnosis of first-ever stroke (International Classification of Diseases [ICD]-10 codes I60-I67) 12 were recruited within the first week after admission to 4 stroke units of 1 hospital in western Sweden from February to July 2006. Stroke was clinically determined by specialists according to the World Health Organization (WHO) criteria 13 and was confirmed using computed tomography. Demographic and clinical-specific information—among others the grade of global disability with the modified Rankin Scale (mRS) 14 —were recorded at recruitment. Participants were followed up at 6 weeks, 3 months, and 1 year poststroke with repeated assessments.
The study was conducted in conformity with the ethical principles of the Declaration of Helsinki 15 and approved by the Ethics Committee of the University of Gothenburg (Dnr: 390-05). At recruitment, patients were provided with a written description of the study, and in the case of participation, written informed consent was obtained.
Outcome Measures
Dependent variable
Generally, HRQoL is considered a complex concept with several dimensions, including physical, occupational, psychological, emotional, social, and so on.1,16 In the literature, one can also find the description of person-reported outcomes or self-reported health in the context of HRQoL research. It can be assessed with multi-item and single-item instruments, both of which have strengths and weaknesses.1,17 In the present study, the single-item approach was chosen, and HRQoL was assessed using the Visual Analogue Scale (VAS) from the EuroQol-5D (EQ-5D) questionnaire. The EQ-5D questionnaire is a generic self-administered HRQoL instrument that is considered a valid measure of HRQoL after stroke.18,19 Additionally, the validity, reliability, and responsiveness of the VAS in particular as an instrument for measuring global quality of life is supported by the literature.20,21 The EQ-5D VAS is a thermometer ranging from 0 (worst imaginable health state) to 100 (best imaginable health state). Study participants were shown a demonstration of this thermometer, received verbal explanations, and were asked to either verbally or mechanically indicate their perceived health, which was noted by the interviewer. The reasons for choosing to measure HRQoL in this study with a single-item question were many. HRQoL is inherently an attribute of people’s perceptions and represents individuals’ feelings about their health. 22 Whereas it has been found that responding to multi-item questionnaires is difficult,23,24 single-item questions are easy to administer and less burdensome to patients.20,25 Furthermore, the rating of a single global question about overall health allows the individuals themselves to combine the various dimensions of HRQoL individually.
Independent variables
The extended version of the ICF Core Set for Stroke8-10 was used to document the biopsychosocial aspects of disability after stroke. The Core Set and its development are described elsewhere. 26 Altogether, 59 categories of Body Functions, 59 of Activities and Participation, and 37 of Environmental Factors were applied in this study. To evaluate the extent of a person’s problems in each ICF category, the qualifier scale proposed by the WHO was used. 7 This scale has 5 response categories for Body Functions and Activities and Participation ranging from 0 to 4: 0 = no; 1 = mild; 2 = moderate; 3 = severe; 4 = complete (4). For Environmental Factors, the qualifier scale has 9 response categories: 0 (no barrier or facilitator), 1 to 4 (mild/moderate/severe/complete barrier), and +1 to +4 (mild/moderate/severe/complete facilitator). In addition, there are the response options 8 (not specified) and 9 (not applicable). Response option 9 was used when a category was not applicable in a determinate patient or situation, and option 8 was used when the information available was not sufficient to quantify the severity of the problem and/or was deemed unreliable.
Information was gathered by means of a standardized interview that consisted of a battery of questions based on the 155 categories from the Stroke ICF Core Set named above (excluding the 11 categories of Structures). Information on health care and social services utilization, spouse support, medication, and observation at the different time points included in a home visit and interview situation gave additional insight into the participants’ problems. If available, additional information from caregivers and health professionals was gathered. The examination could last between half an hour and 2 hours, depending on a participant’s health state. The ratings of the 59 ICF categories of Body Functions, the 59 categories of Activities and Participation, and the 37 categories of Environmental Factors were based on all information obtained during the interview, including also information from observation of the interviewee’s functioning. The integration of information from interview and observation was done to rate correctly participants’ actual functioning, that is, what they can and cannot do in their individual environments. For example, if a participant answered that he has no problem using his walking frame but he struggled several times with it during the home visit, this ICF category was rated as a problem. All interviews and ratings were done by the first author who was trained in stroke rehabilitation and ICF as a member of the ICF Research Branch in Munich that coordinates the international development and validation of ICF Core Sets. 27
Data Analysis
Univariate statistics were used to describe the sample characteristics. When the variables were not distributed normally (Kolmogorov-Smirnov test 28 ), medians were reported. Independent relationships between HRQoL (EQ-5D VAS) and impairments (ICF categories of Body Functions), limitations and restrictions (ICF categories of Activities and Participation), and environmental factors (ICF categories of Environmental Factors) were analyzed by means of backward linear regression analysis at each time point. The ICF categories entered in the regression models were identified by means of bivariate analysis (Spearman correlation). In cases of multicollinearity (correlation coefficient > .5), the category with the stronger correlation with the EQ VAS score was chosen. For each ICF component—namely, Body Functions, Activities and Participation, and Environmental Factors—linear regression analyses were performed independently. To account for the multivarious biopsychosocial factors of disability, a regression model considering categories of all 3 components simultaneously were calculated. Therefore, the identified categories within each ICF component from the previous regression analyses were used. This stepwise approach is shown in Figure 1. For the multivariate analyses, the degrees of the qualifier scale of the ICF categories were dichotomized into a yes/no problem as follows: the qualifier 0 (no problem) was maintained, the qualifiers 1 to 4 were recoded to 1 (problem), the response option 8 (not specified) was treated as missing, and the response option 9 (not applicable) was recoded to 0 (no problem). Age and number of comorbidities were incorporated into each model as independent variables for HRQoL. The level of significance was set at 5% for all tests (2-sided). Statistical analyses were performed using SPSS (version 17.0; SPSS Inc, Chicago, Illinois).
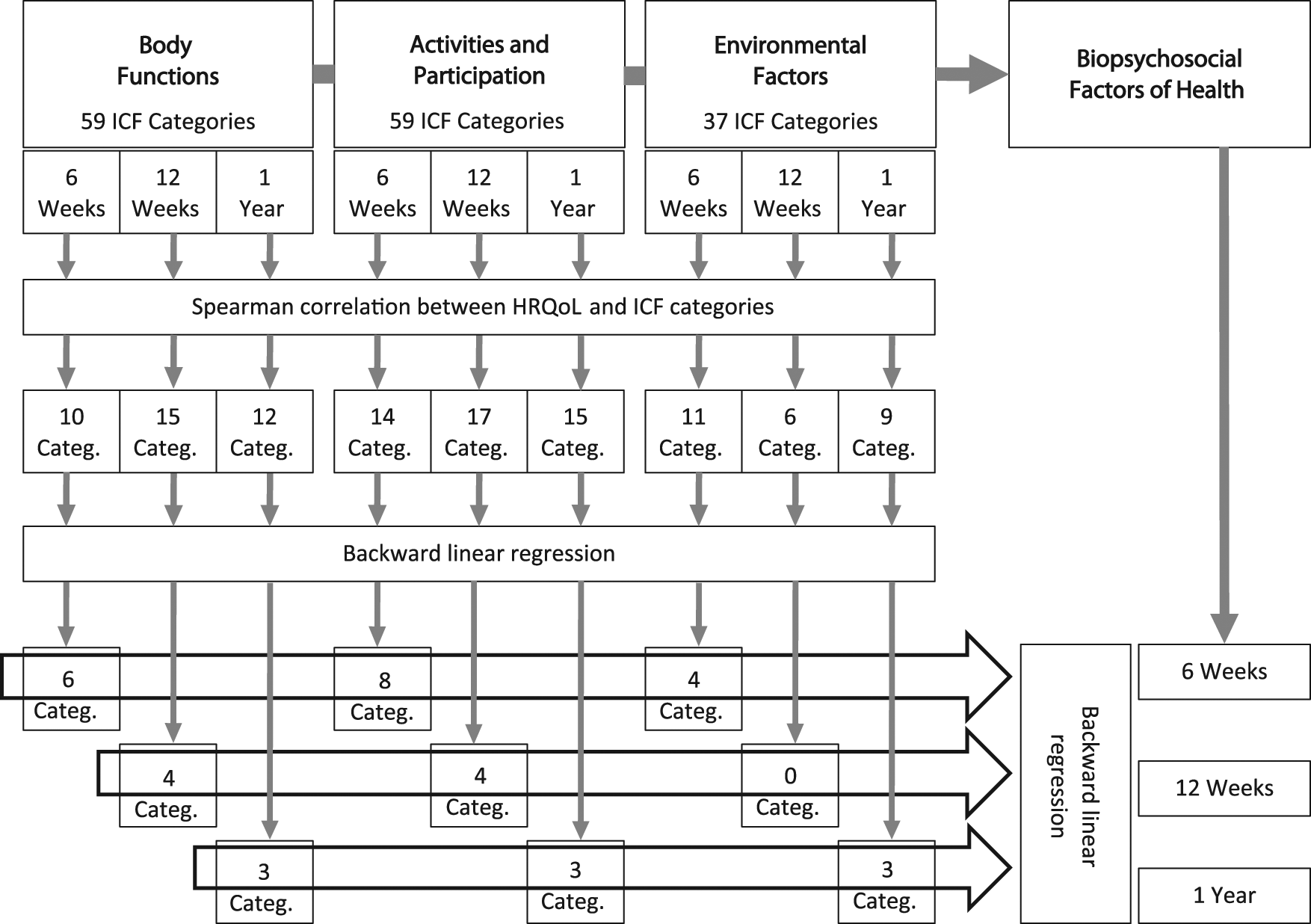
The stepwise approach to identify factors of HRQoL at 3 different time points poststroke. Abbreviations: HRQoL, health-related quality of life; ICF, International Classification of Functioning, Disability and Health.
Results
Participants
A total of 120 patients with stroke were recruited and assessed at admission. After a diagnosis check, 14 participants were deemed ineligible to participate because their preliminary diagnosis of a first-ever stroke had been revised. Of the 106 patients included, 3 died, 2 moved, and 2 declined to participate. The remaining 99 participants were followed up, and 80 of them were assessed for HRQoL at 6 weeks, 76 at 3 months (1 had died), and 85 at 1 year (2 had died). Reasons for losses to follow-up were either that they were not contactable, had died, or had no opinion about their HRQoL. There were no significant differences in diagnosis, gender, and age between those who were assessed and those who were lost to follow-up. Ischemic stroke was the main diagnosis (82%). At inclusion, the mean age of participants (55% women) was 72 years, time after diagnosed stroke was an average of 4 days (with a standard deviation of 2 to 4 days), and stroke severity was an average of 3 on the mRS. At 1 year, global disability was less severe, and the median score on the mRS was 2. Baseline and disease-specific characteristics of the study sample are shown in Table 1.
Study and Disease-Specific Characteristics of Stroke Survivors
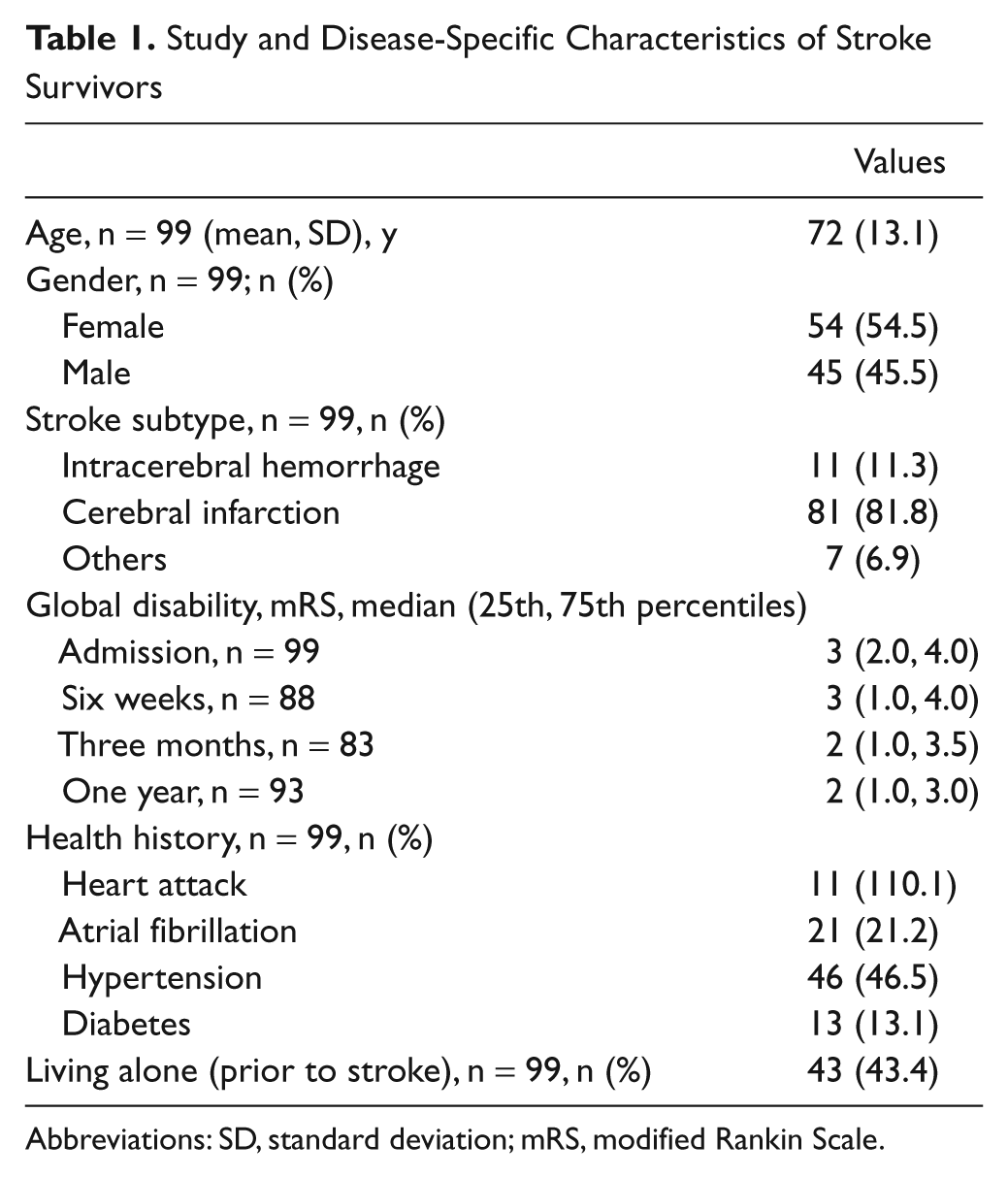
Abbreviations: SD, standard deviation; mRS, modified Rankin Scale.
Whereas participants’ HRQoL scored a median of 50 on the EQ VAS at inclusion, it improved, and the median score on the VAS was 75 at 1 year. Most of the participants (53%) improved between admission and at 6 weeks poststroke (see Figure 2). The number of participants’ impairments, limitations, restrictions, and environmental facilitators changed minimally during 1 year. Detailed information about participants’ problems and facilitators during the first 3 months was given in 2 previous articles.29,30 HRQoL and consequences for participants are presented in Table 2.
Health-Related Quality of Life and Number of Problems Within Each ICF Component, n = 99
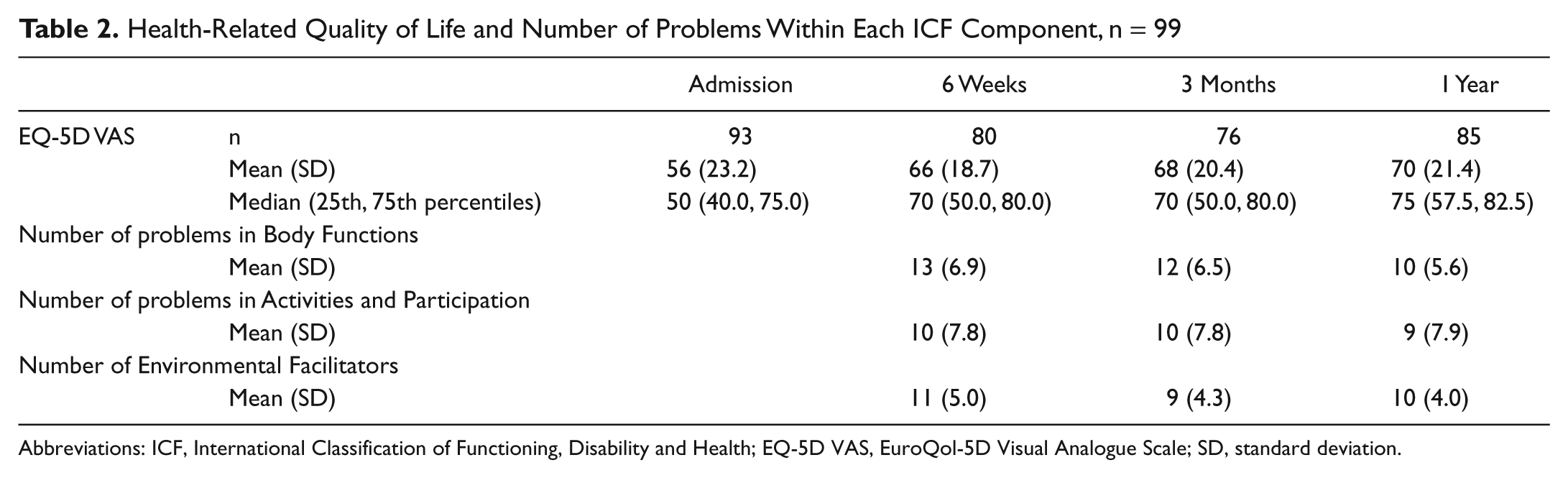
Abbreviations: ICF, International Classification of Functioning, Disability and Health; EQ-5D VAS, EuroQol-5D Visual Analogue Scale; SD, standard deviation.
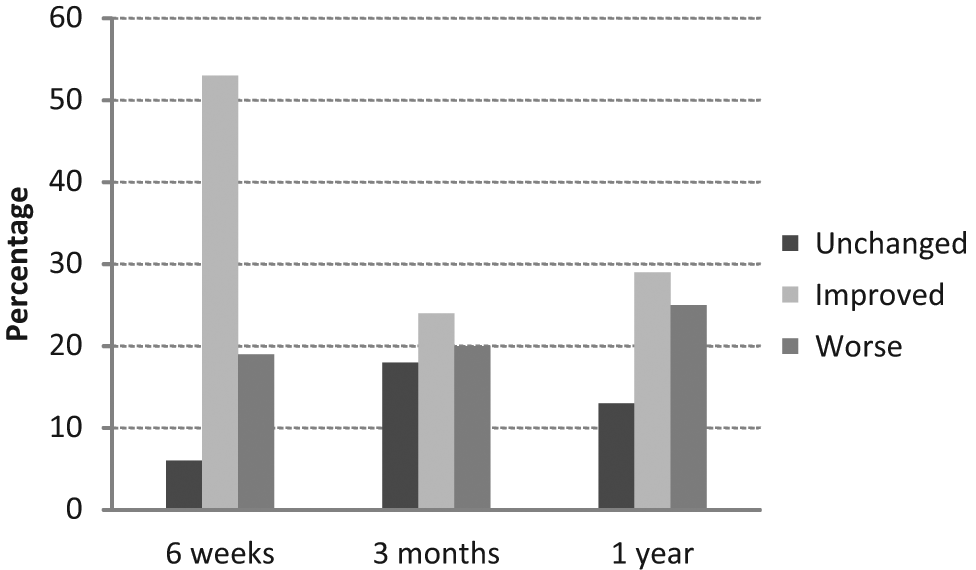
The percentage of stroke survivors with unchanged, improved, or worse health-related quality of life rated on the EuroQol-5D Visual Analogue Scale at each time point.
Bivariate Analyses
Of 59 ICF categories of Body Functions, there were 10 at 6 weeks, 15 at 3 months, and 12 at 1 year that were significantly (P < .05) related to HRQoL. Coefficients (Spearman) ranged from 0.22 (b160 Thought functions) to 0.58 (b455 Exercise tolerance functions). Of the 59 categories of Activities and Participation, there were 14 at 6 weeks, 17 at 3 months, and 15 at 1 year with a significant relationship to HRQoL. Coefficients ranged from 0.23 (d170 Writing) to 0.63 (d920 Recreation and leisure). Of the 39 ICF categories of Environmental Factors, there were 11 facilitators at 6 weeks, 6 at 3 months, and 9 at 1 year that were significantly associated with HRQoL. Coefficients ranged from 0.23 (e355 Health professionals) to 0.44 (e575 Social security services, systems and policies). No barrier was significantly correlated with HRQoL. The table of the correlations between the initial 155 ICF categories and the EQ-5D VAS can be obtained from the authors on request.
Multivariate Analyses Within Each ICF Component
Results of the linear regression models are shown in Table 3. Problems in Body Functions and Activities and Participation were constantly associated with worse HRQoL, except for problems in d325 (Communicating with-receiving-written messages) and d360 (Using communication devices and techniques) that were related to better HRQoL. Almost all the variance in HRQoL was explained by Body Functions as well as Activities and Participation at 6 weeks and 3 months (93% and 89%, and 80% and 84%, respectively). Whereas at 1 year Activities and Participation could explain only one fourth (22%), Body Functions still explained half of the variance (51%). Environmental facilitators explained half of the variance at 1 year, but nothing and little (10%) at 3 months and 6 weeks, respectively.
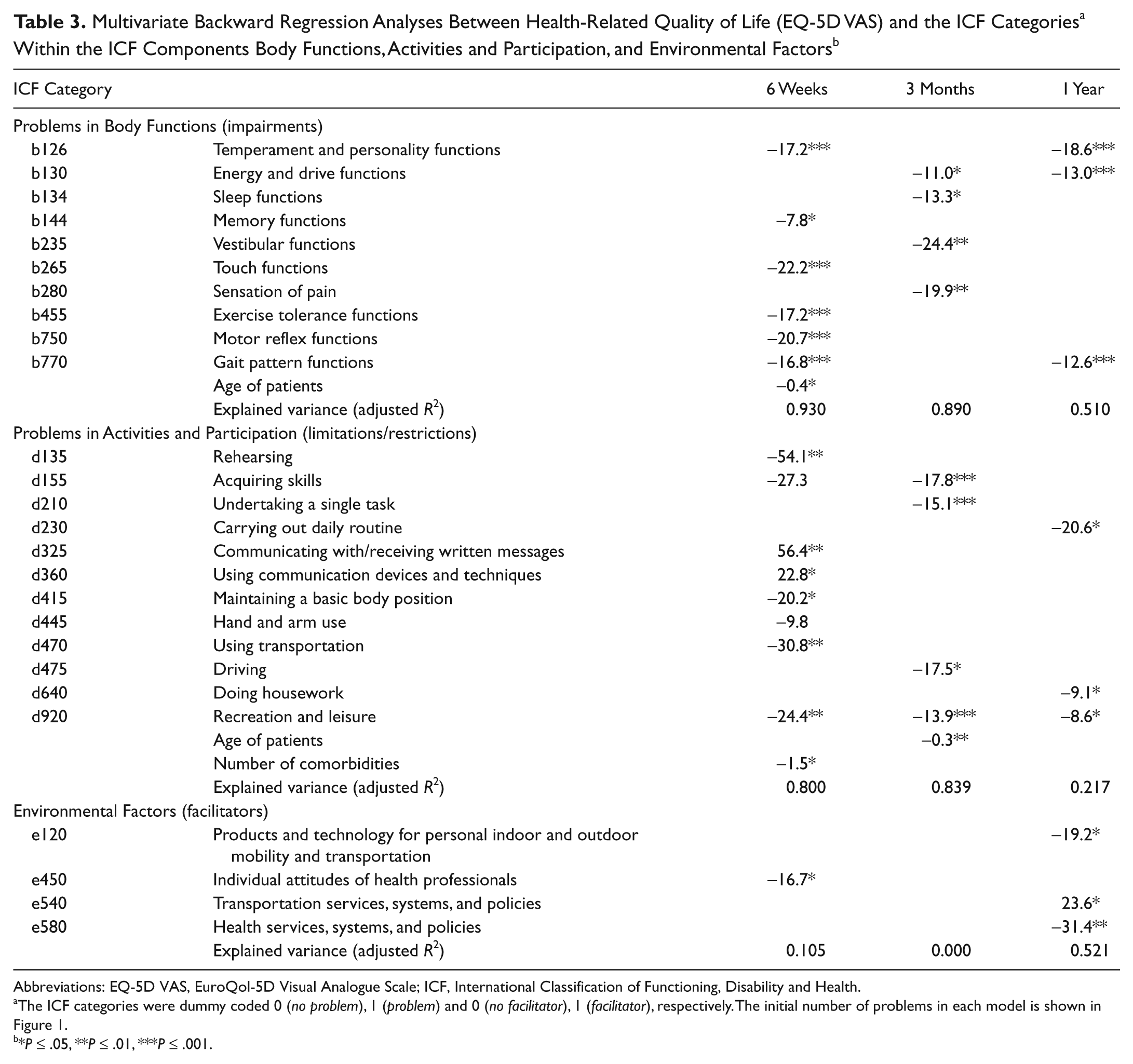
Abbreviations: EQ-5D VAS, EuroQol-5D Visual Analogue Scale; ICF, International Classification of Functioning, Disability and Health.
The ICF categories were dummy coded 0 (no problem), 1 (problem) and 0 (no facilitator), 1 (facilitator), respectively. The initial number of problems in each model is shown in Figure 1.
*P ≤ .05, **P ≤ .01, ***P ≤ .001.
Multivariate Analyses of All ICF Components
The results of the final regression model that considered ICF categories of Body Functions, Activities and Participation, and Environmental Factors together are displayed in Table 4. At all time points, problems in Body Functions and Activities and Participation were associated with lower HRQoL and likewise e450 (Individual attitudes of health professionals) at 6 weeks, although this was perceived as a facilitator. The ICF categories b126 (Temperament and personality functions), b120 (Energy and drive functions), b770 (Gait pattern functions), and d640 (Doing housework) could explain half of the variance in HRQoL (49%) at 1 year. At 6 weeks and 3 months, less variance was explained (29% and 38%).
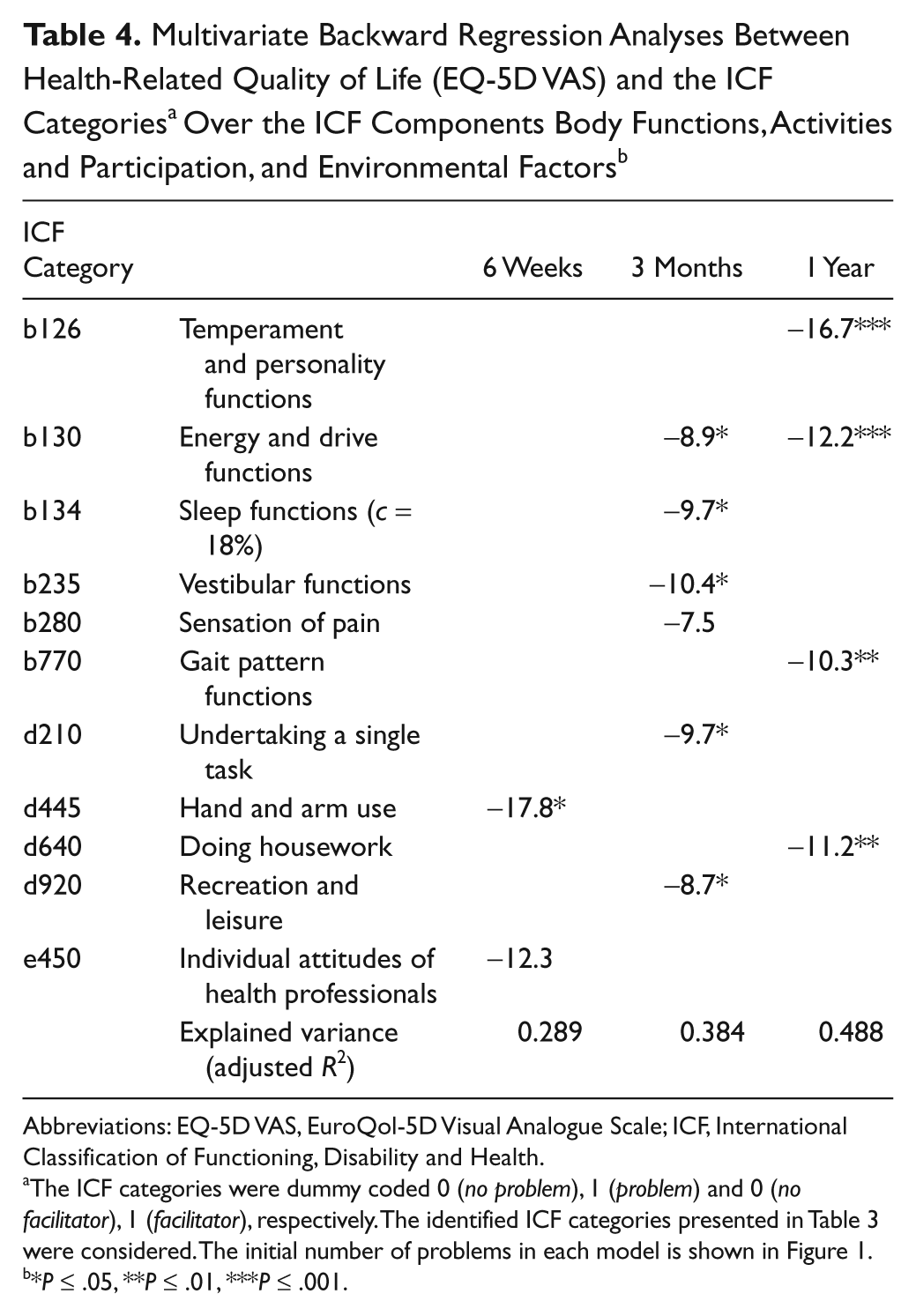
Abbreviations: EQ-5D VAS, EuroQol-5D Visual Analogue Scale; ICF, International Classification of Functioning, Disability and Health.
The ICF categories were dummy coded 0 (no problem), 1 (problem) and 0 (no facilitator), 1 (facilitator), respectively. The identified ICF categories presented in Table 3 were considered. The initial number of problems in each model is shown in Figure 1.
*P ≤ .05, **P ≤ .01, ***P ≤ .001.
Discussion
The association between HRQoL and the biopsychosocial factors of functioning and disability over the course of 1 year poststroke was examined. Factors of HRQoL after stroke varied over time. Whereas in the first 3 months Body Functions and Activities and Participation were the constitutive parameters and could explain almost all variance in HRQoL, at 1 year, only half of the variance could be explained, and then by either Body Functions or Environmental Factors. Accounting for the complexity of functioning and considering the various biopsychosocial factors all together, only a minor part of the variance was explained in the first 3 months but about half was explained at 1 year. Limited recreation and leisure, energy and drive functions (e.g. fatigue), impaired gait patterns, and personality functions were independent factors repeatedly associated with lower HRQoL during a period of 1 year poststroke.
Considering the categories within Body Functions and Activities and Participation themselves explained excellently the deviation in HRQoL under the first 3 months poststroke. For example, impaired energy and drive functions (e.g. fatigue), sleep problems, impaired vestibular functions (e.g. balance problems), and pain were very important for HRQoL at 3 months and explained almost all the variance. Regarding Activities and Participation, limited learning capacity, problems in undertaking a single task, problems with driving, and limited and restricted recreational activities were central factors in HRQoL at 3 months and explained four fifths of the variation. However, at 1 year, HRQoL was no longer influenced as powerfully by Activities and Participation and much less by Body Functions, but environmental facilitators attached meaningfulness to HRQoL. Determinants of HRQoL might be more obscure in the chronic phase because only half of the variation in HRQoL could be explained at 1 year, whereas almost all variation was explained in the first 3 months. At 1 year, then, other dimensions of HRQoL may not be detected by categories of the Core Set, such as personal factors included in the ICF framework but not classified. For example, coping strategies were shown to be a powerful determinant of HRQoL later in the chronic phase by Darlington et al. 31 In our study, HRQoL was repeatedly influenced by temperament and personality functions that are closely related to personal factors.
Products and technology for personal indoor and outdoor mobility (eg, wheelchair and walking frame), facilitating transportation services, and facilitating health services and systems were important for HRQoL. Their positive effect has been shown in other studies but has not been directly associated with HRQoL.32,33 Surprisingly, facilitators were not consistently related to better but instead to worse HRQoL, except for transportation services. One explanation for this might be that quality of life is strongly related to global disability, and the patients who were more disabled easily had more contact points with those factors and thus reported them as facilitators.
An analogous phenomenon was seen within Activities and Participation. All problems were related to worse HRQoL except for those in communication involving receiving written messages and problems with telephone use, which were associated with better HRQoL. It is generally accepted that social contact and support are essential to quality of life.34,35 It was only the patients who experienced problems in using the telephone and reading the newspaper who had this important social contact, and this fact might explain the positive relationship.
Taking into account that health originates in the complexity of the various biopsychosocial factors and their interaction, it could be expected that considering categories of Body Functions, Activities and Participation, Environmental Factors, and Personal Factors (e.g. age and number of comorbidities) all together can explain most variation in HRQoL. However, this was not true. It was only at 1 year that the various factors together could explain as much variance as Body Functions or Environmental Factors. Then, the substantial factors of HRQoL were again personality and energy functions but also gait pattern functions and housework activities. Mechanisms that cause the individual to move toward satisfying specific needs and goals are defined as energy and drive functions in the ICF framework. 7 Furthermore, an individual’s perception and establishment of goals and expectations are undoubtedly influenced by personal characteristics such as optimism, psychic stability, and confidence. 36 Not only were mental and personality functions identified as powerful determinants of HRQoL already in previous studies,37-39 but the relationship between HRQoL and gait as well as activities of daily living (ADL), including housework, were also identified as determinants.40,41 This association was in the chronic phase after stroke. At 1 year, participants might have changed their internal values and standards as expectations of returning to a normal life grew more realistic. Many activities are dependent on ambulatory capacity. The importance of housework activities might be explained by the fact that participants were elderly. A younger study group might have had other primary expectations and values, such as returning to work.
Limitations to this study include the relatively small sample size, which leads to a lack of statistical power. Because this study was explorative, testing a less-common approach to looking at factors of global HRQoL, further research with larger study samples is needed to validate the findings. A sample size of about 200 participants might be more appropriate because the number of identified independent variables for the multivariate analyses ranged in this study between 8 and 18, and most authors recommend at least 10 times as many observations as one has independent variables to ensure the reliability of the regression estimates. 42 Another limitation is a possible selection bias during the data collection process. If information was inadequate or ambiguous, the ICF-qualifier “8—not specified” was used, as in participants with communication difficulties. They were excluded from analysis. A further limitation might be that information about the extent of problems with respective facilitators were not considered since the ratings on the 5-point ICF rating scale were dichotomized for the analysis into problem yes/no respective facilitator/barrier/neither-nor. However, this was done in order to increase reliability as there is little evidence for the psychometric applicability of the 5-point ICF rating scale.
Conclusion
Factors of HRQoL vary with time after stroke and reflect the individual’s changes of internal standards, values, and expectations influenced by the recovery process. For clinical implications, the results of this study suggest that rehabilitation programs should address primarily Body Functions and Activities and Participation within the first 3 months (such as problems with balance, fatigue, sleep, pain, hand and arm use, undertaking single tasks, and recreation). At 1 year, adjusted Environmental Factors can contribute considerably to improving HRQoL. Specifically, an initial focus on patients’ personality and energy drive functions as well as on their recreational activities and walking capacities might have a great impact on HRQoL.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Norrbacka-Eugenia Foundation, the Swedish Association of Persons with Neurological Disabilities, the Swedish Stroke Association, FoU Göteborg and Södra Bohuslän, Västra Götalands Handicap Committee, the Wilhelm and Martina Lundgren Foundation, and the Felix Neubergh Foundation.