
Abstract
Background. Not all individuals with unilateral vestibular hypofunction (UVH) have fewer subjective complaints and improved function after vestibular rehabilitation. Objective. To identify factors and/or combinations of factors that are strongly associated with rehabilitation outcome in patients with UVH and that ultimately can be used to develop models to predict outcome. Methods. Data from 209 patients with UVH were analyzed. All patients participated in similar vestibular rehabilitation (5 weeks of home exercises and once-weekly clinic visits). Outcome measures included intensity of oscillopsia and dysequilibrium, balance confidence, perceived disability, percentage of time symptoms interfered with activities, gait speed, fall risk, and dynamic visual acuity (DVA). Bivariate correlation and regression analysis were used to determine relationships between baseline (pretherapy) measures and outcome at discharge. Results. No baseline measure of subjective complaints (eg, symptom intensity) predicted improvement of physical function (eg, gait speed). Similarly, no baseline measure of physical function predicted improvement of subjective complaints. Certain patient characteristics, such as gender and time from onset, were not related to any outcomes. Most comorbidities did not affect outcome; however, anxiety and/or depression were associated with lower balance confidence and higher percentage of time for which symptoms interfered with activities at discharge. Baseline DVA and gait speed were associated with DVA and gait speed at discharge, respectively. Dynamic gait index (DGI) at discharge was affected by age, baseline DGI, and history of falls. Conclusion. These results provide insight into recovery of patients with UVH. Therapists can use this information in the development of expectations for patient outcome and treatment priorities.
Introduction
Studies of individuals with unilateral vestibular hypofunction (UVH) suggest that a program of vestibular adaptation and substitution exercises results in decreased subjective complaints and improved function in most but not all patients.1-7 We have some ideas as to what factors affect recovery: for example, patient age and time from onset do not affect the potential for recovery.1,3,8 In contrast, vestibular migraine has been identified as a risk factor for continued anxiety and symptom intensity. 9 Many factors that might influence recovery, such as degree of balance impairment at the initiation of rehabilitation or the presence of comorbidities such as neck pain, have not been examined to determine if or how they affect recovery. Additionally, there is little quantitative evidence about the effect of interactions among factors such as level of impairment, patient demographics, and comorbidities on outcome. The purpose of our study was to identify factors or combinations of factors that are strongly associated with rehabilitation outcomes of patients with vestibular dysfunction in order to develop models that predict outcome.
Methods
Participants
Informed consent was obtained in compliance with the University of Miami or Emory University Institutional Review Board protocols. Patients were entered into a database by a vestibular technician. A total of 323 patients who met the inclusion criteria of a documented peripheral UVH and referral for vestibular rehabilitation were identified and cross-checked by one of the investigators (SJH). Of these patients, 209 had multiple sessions of vestibular rehabilitation and were included in the final analyses. Diagnosis of UVH was based on a ≥25% difference in slow-phase eye velocity between right and left sides on caloric or rotary chair testing and by a time constant of less than 10 s on step rotary chair testing at 60° per second.
Three certified, vestibular physical therapists collected the data and treated the patients (one from 1997 to 2006 and two after 2003). Every 6 months, interrater reliability testing was performed to ensure consistency of measurements. At the initial visit, patients filled out questionnaires regarding date of onset, symptoms, depression and anxiety, medications, and medical history. These data were confirmed during the interview by the health care provider. Depression and anxiety were identified from medical history, medication, and physician interview based on DSM-IV criteria. Migraine was diagnosed by the neurologist based on International Headache Society (IHS) criteria. Age and gender were obtained from patients’ charts. Degree of deficit was the asymmetry in response to caloric irrigation or to rotations at 240° per second. An assumption was made that the status of those patients after surgical intervention (eg, schwannoma resection or vestibular labyrinthectomy or neurectomy) was of 100% asymmetry. Duration of treatment was obtained from physical therapy notes.
Vestibular Exercises
Patients were seen by the therapist once a week to review and modify their home exercise program. All patients performed a combination of vestibular adaptation and substitution exercises 3 to 5 times daily.3,10 The general sequence of exercises was the same for all patients, except that the rate of exercise progression differed across individuals. All patients also performed balance and gait exercises and a walking program daily. 10 The total duration for all exercises was 60 to 70 minutes daily. Patients performed the exercises until recovery plateaued, based on repeated outcome measures. Typically, patients were seen for 4 to 6 weeks as is standard. 3
Outcome Measures
Outcome measures included (1) subjective complaints (intensity of symptoms, balance confidence, perceived disability, and percentage of time symptoms interfered with activities) and (2) functional activities (gait speed, dynamic gait index score, and visual acuity during head movement—dynamic visual acuity [DVA]). Only outcome measures that were initially abnormal (with the exception of DVA and gait speed) were included in analyses. Not all patients had all outcome measures repeated at discharge.
Measurement of Subjective Complaints
Intensity of symptoms
Visual analogue scales were used to assess the degree of perceived visual blurring (OVAS) and of perceived dysequilibrium (DYSVAS). 11 Test–retest reliability for these measurements is moderate. 11 For both visual analogue scales, patients rated the intensity of their symptoms on a featureless, vertical 10-cm line. One end of the line was anchored with the statement “I see perfectly clearly (normal for me before the problem)” or “I feel perfectly steady” and the other end by “as bad as it can be.” Measurements were taken first while the patient was sitting and then while the patient was walking. Separate handouts were used for each of the measures. OVAS and DYSVAS represent the difference in scores between sitting and walking. Only baseline scores >0.2 cm were considered abnormal and included in the analysis. We chose 0.2 cm as the cutoff for normal because many patients drew a line hastily near the bottom of the 10-cm line but verbally indicated no symptoms. There are no data on what constitutes a significant or clinically meaningful change in VAS score.
Balance confidence
The Activities-Specific Balance Confidence Scale (ABC) assesses balance confidence across a continuum of progressively more challenging situations from mobility in the home to walking on icy sidewalks.12,13 The ABC scale demonstrates good test–retest reliability (r = 0.92) and convergent and criterion validity. 13 Total scores range from 0% to 100%, with baseline scores of <80% considered abnormal. A significant change in the ABC score was either a return to a score of at least 80% or a change of more than 10 points.13,14
Quality of life
Quality of life was assessed using the Disability Scale 15 and the percentage of time symptoms interfere with life (PSIL). The Disability Scale has excellent test–retest reliability (r = 0.98) and is sensitive to change. 16 Possible scores range from 0 to 5, with 0 indicating negligible symptoms and 5 indicating permanent disability or not being able to work for more than 1 year. Baseline scores of 1 or greater were considered abnormal and included in the analysis. A change in score of 1 point was considered a meaningful change based on the normal variability of the score. 16
Percentage of time symptoms interfere with life
Patients answered the question, “What percentage of the time has dizziness interfered with your activities?” by drawing a vertical line across a 10-cm line with 20% increments. The outcome measure was the distance from 0 to the patient’s mark and ranged from 0% to 100%. 17 Test–retest reliability for this tool is excellent (r = 1.00). 16 Significant change was based on a change of at least 4.1% (mean plus 2 standard deviations [SDs] of test–retest variability). 16 There are no available data on what constitutes a clinically meaningful change in score.
Measurement of Functional Activities
Gait speed
The time taken to walk the middle 6-m of a 9-m course was measured with a stopwatch, and then, gait speed was calculated. Only 1 trial was used because test–retest reliability for a single trial is excellent (r = 0.85). 16 A meaningful change in gait speed was defined as a return to normal gait speed for age and gender based on data from Bohannon. 18
Dynamic gait index (DGI)
Scoring of the DGI is based on a 4-point scale from 0 (severe impairment) to 3 (normal ability). A maximum total score of 24 is possible, and scores less than 20 indicate fall risk.19-21 The DGI has validity and excellent reliability in patients with vestibular deficits (r = 0.96-0.98).19,20,22 Meaningful change was defined as a change in score by at least 3 points or a return to a score of ≥20 points. 16
Falls
Falls were defined as falls to the ground or floor. Falls that occurred prior to the initiation of vestibular exercises were identified by patient history.
Dynamic visual acuity (DVA)
Visual acuity during head movement was measured using a computerized system in which the optotype is displayed only when the patient’s head velocity is between 120° and 180° per second. 23 Test–retest reliability of computerized DVA is excellent (r = 0.92) in patients with vestibular hypofunction. 23 Normal values by age (mean plus 1 SD) have been established using this test. 23 A significant change in results was defined as either a return to normal DVA for age or a change in score that was at least 0.069 logMAR (minimum angle of resolution). 3
Statistical Analyses
SPSS v17.0 software (SPSS Inc, Chicago, IL) was used for data analyses. We calculated effect size as a measure of the magnitude of difference between baseline and discharge means for each outcome measure. Using Cohen’s convention, a medium effect size was defined as the difference between the means of 50% of the group SD, and a large effect size was defined as a difference between the means of 80% of the group SD. 24
Group characteristics were summarized using descriptive statistics. Student’s t tests for paired comparisons were performed to determine significant changes (P < .006 to control for multiple comparisons25,26) from baseline to discharge. Paired data were included only if the baseline value was abnormal. Confidence intervals were calculated to provide an estimate of normal population values for each measure.
The strength of the relationship between the independent variables and each of the outcome measures at discharge was determined using bivariate correlations. Independent variables were age, gender, time from onset, degree of deficit, specific comorbidities, number of comorbidities and baseline measures of subjective complaints, balance confidence, perceived disability, PSIL, gait speed, fall risk, and visual acuity during head movement (Tables 1 and 2). Only abnormal baseline measures were included in the analysis, except for normal DVA and gait speed. Missing data were left as blank values. Correlations were determined for raw data, significant change (yes or no), and return to normal (yes or no). Level of significance was set at P < .001 to control for the large number of variables examined. Relative strengths of the correlations were defined as follows: 0.00 to 0.25, little or no relationship; 025 to 0.50, fair relationship; 0.50 to 0.75, good; and >0.75, good to excellent relationship.
Relationships Between Baseline Measures and Subjective Outcome Measures at Discharge (Only Significant Relationships Are Shown)
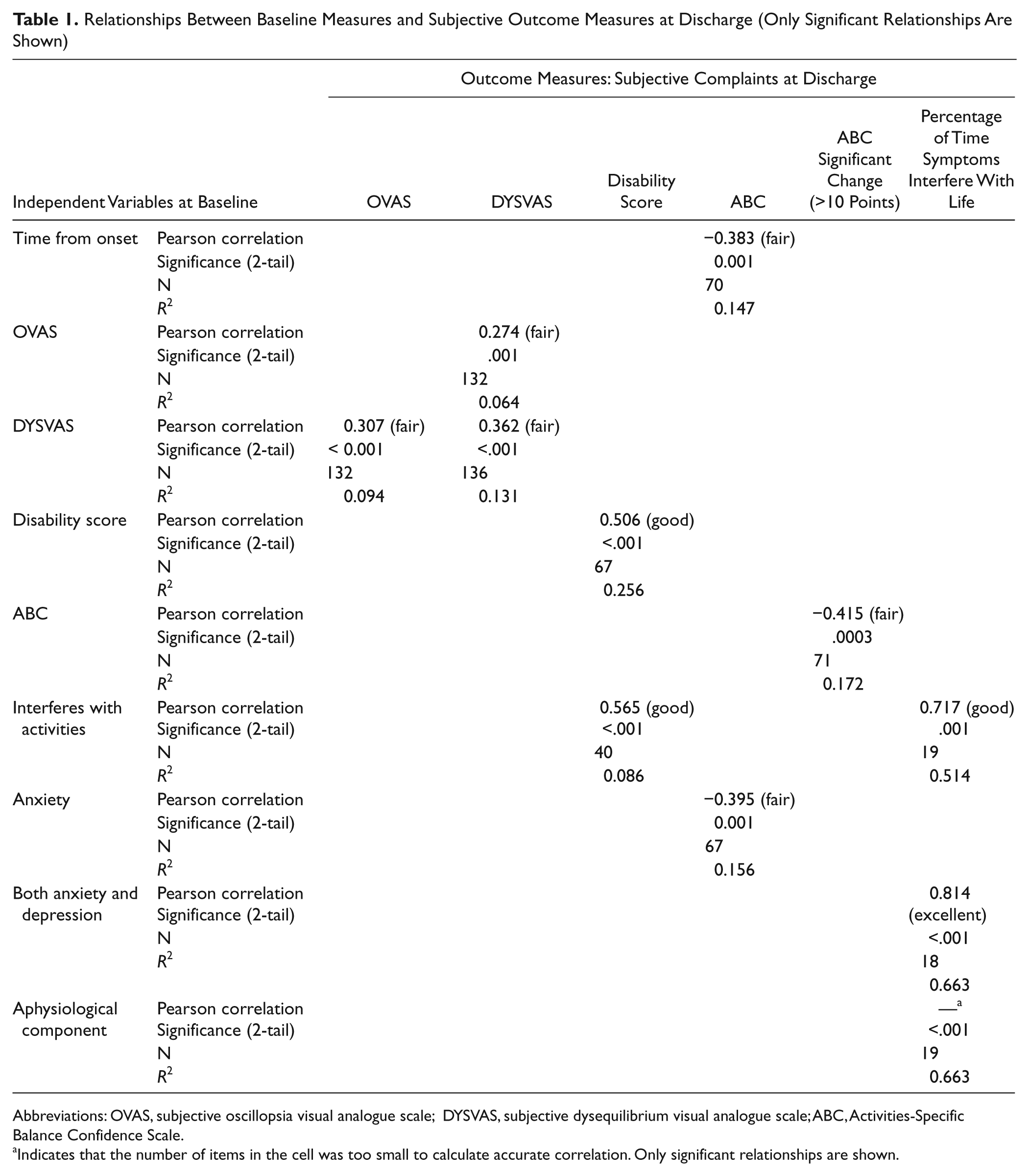
Abbreviations: OVAS, subjective oscillopsia visual analogue scale; DYSVAS, subjective dysequilibrium visual analogue scale; ABC, Activities-Specific Balance Confidence Scale.
Indicates that the number of items in the cell was too small to calculate accurate correlation. Only significant relationships are shown.
Relationships Between Baseline Measures and Measures of Function at Discharge
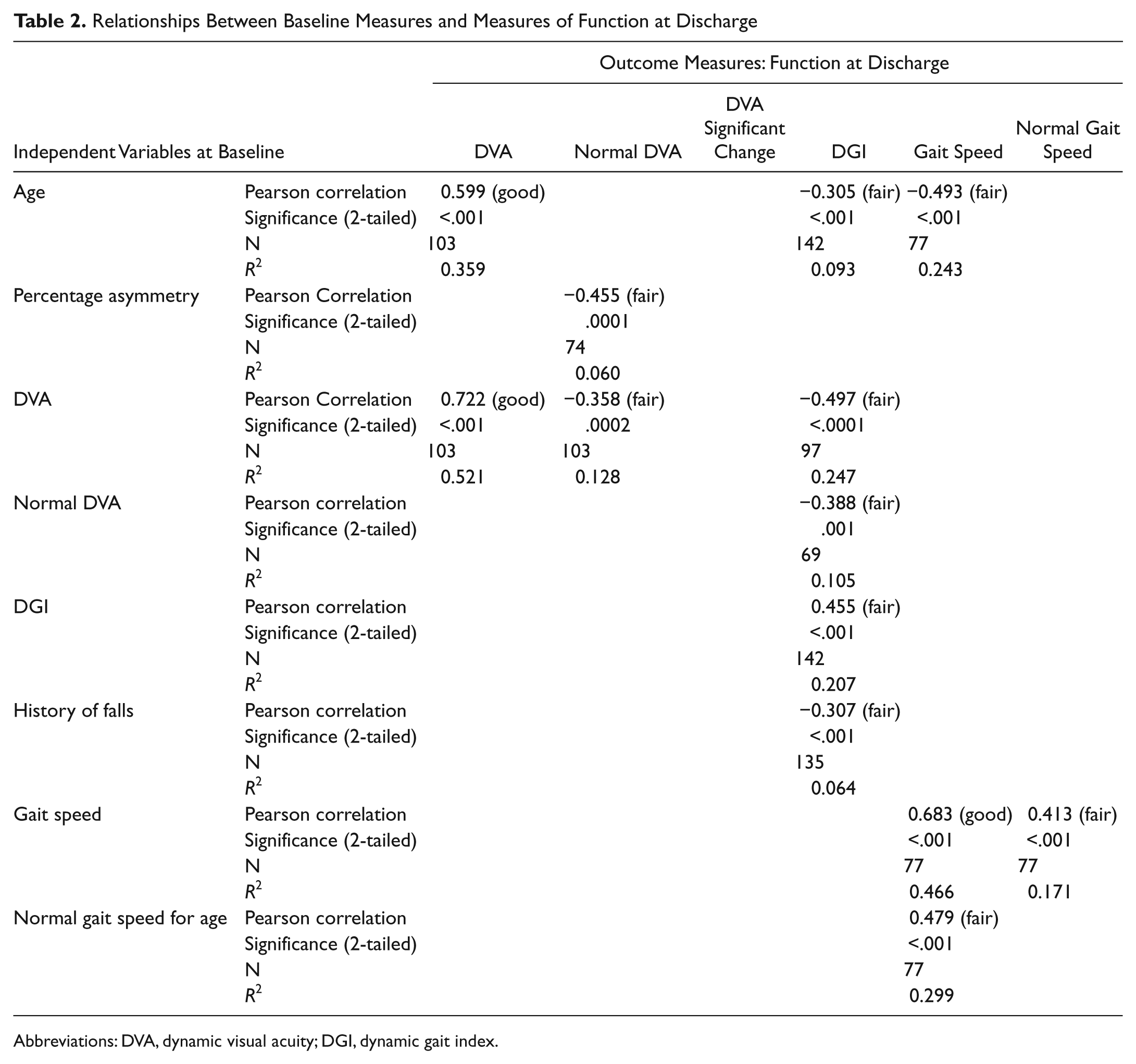
Abbreviations: DVA, dynamic visual acuity; DGI, dynamic gait index.
Multiple stepwise regression analyses were performed to identify factors or combinations of factors that explained rehabilitation outcomes. Independent variables that were statistically significant based on bivariate correlations were included in multiple stepwise regression analyses to control for interactions among the independent variables. A probability of F of .05 was used to enter variables and .10 to remain within the model. R2 values for the whole model and standardized β weights and β2 values for individual factors were used to identify meaningful associations between the independent variables at baseline and the discharge measures. We used Cohen conventions for R2 values, with 0.01, 0.09, and 0.25 indicating small, medium, and large effects, respectively.
Results
Participant Characteristics
In all, 209 patients with UVH met the inclusion criteria (women, n = 106; men, n = 103). The average age was 59.3 years ± 14.9 years (range, 14-88 years). Of the 209 patients, 76.1% (n = 159) had vestibular neuronitis or labyrinthitis; 8.1% (n = 17) were status postresection of vestibular schwannoma, 2.4% (n = 5) status postlabyrinthectomy, 1.9% (n = 4) status postvestibular nerve section, and 1.5% (n = 3) status postcholesteoma, meningioma resection, or chemical ablation; and 10% (n = 21) had no specific diagnoses. The mean asymmetry was 71% ± 26%, and the mean time from onset was 14.5 months ± 33.6 months (range, 1 week to 12 years; median, 5.0 months). The average duration of rehabilitation was 5.7 ± 3.3 weeks. Among the participants, 25 (12%) had a history of migraine, and 8.6% had a history of Ménière’s disease (Table 3); 77 (36.8%) of the participants had none of the comorbidities we examined, 44 (21.1%) had 1, 34 (16.3%) had 2, and 54 (25.8%) had 3 or more comorbidities.
Number (Percentage) of Individuals With Specific Comorbidities Present
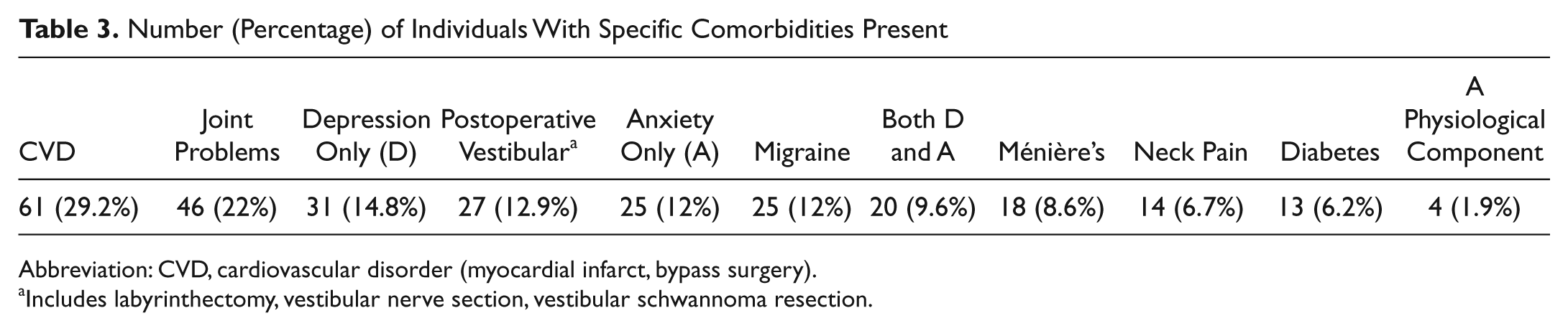
Abbreviation: CVD, cardiovascular disorder (myocardial infarct, bypass surgery).
Includes labyrinthectomy, vestibular nerve section, vestibular schwannoma resection.
All patients had repeat testing; however, some data were missing from almost every participant. Missing data at discharge were in part a result of time constraints. Furthermore, not all patients had abnormal test results at initial assessment (Table 4).
Mean (SD) in Outcome Measures for the Group at Baseline and Discharge
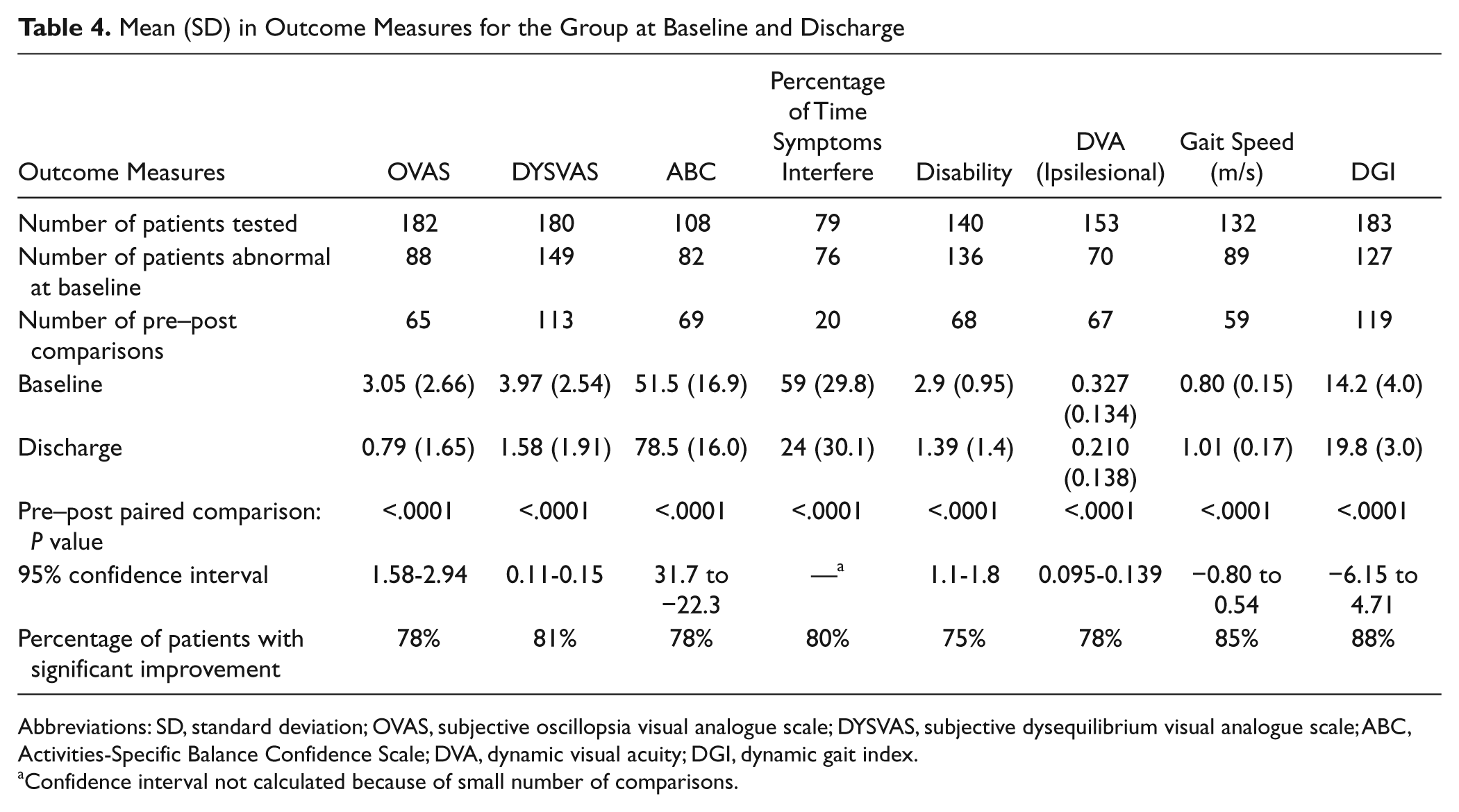
Abbreviations: SD, standard deviation; OVAS, subjective oscillopsia visual analogue scale; DYSVAS, subjective dysequilibrium visual analogue scale; ABC, Activities-Specific Balance Confidence Scale; DVA, dynamic visual acuity; DGI, dynamic gait index.
Confidence interval not calculated because of small number of comparisons.
Change in Outcome Measures With Intervention
There was a significant improvement for the group as a whole for each outcome measure (P < .006; Table 4). For each outcome measure, a majority of patients, but not all, improved. The percentage of patients who improved varied from 75% to 88% depending on the specific measurement (Figures 1 and 2; Table 4).

Change in subjective complaints in individual participants with vestibular rehabilitation: change in the subjective complaint of visual blurring (OVAS; A), the perception of dysequilibrium (DYSVAS; B), balance confidence (C), and perceived disability (D) show that while the majority of patients improve over the course of rehabilitation, there are some patients who either do not improve or become worse. For all figures, the initial measurement is indicated by the light gray bars and the final measurement by the dark gray bars. The number of participants is on the x-axis, and the scale for each measure is on the y-axis for each. The arrows point to the groups of participants who returned to normal, improved, did not change, or became worse

Change in physical function in individual participants with vestibular rehabilitation: change in the dynamic visual acuity (A), preferred gait speed (B), and risk for falling (C) show that whereas the majority of patients improve over the course of rehabilitation, there are some patients who either do not improve or become worse. For all figures, the initial measurement is indicated by the light gray bars and the final measurement by the dark gray bars. The number of participants is on the x-axis, and the scale for each measure is on the y-axis for each. The arrows point to the groups of participants who returned to normal, improved, did not change, or became worse
Strength of Associations Between Baseline and Outcome Measures at Discharge: General Findings
Some independent variables did not show a significant relationship with any outcome measure at discharge. These include gender, initial subjective complaint of oscillopsia, the presence of a functional component (a rare occurrence seen in only 4 patients), and the presence of depression.
Age and percentage caloric/rotary chair asymmetry showed a strong relationship with certain measures of function at discharge but not with subjective complaints at discharge.
None of the independent variables showed a significant relationship with return to normal ABC at discharge or the occurrence of falls during treatment.
The presence of Ménière’s disease, joint problems, cervical problems, cardiovascular disorders, diabetes, surgical etiology, and the total number of comorbidities were not related to outcome.
Regression Models of Outcome Measures: Specific Findings (Table 5)
Oscillopsia
Intensity of oscillopsia and of dysequilibrium at baseline were significantly correlated with oscillopsia at discharge. Only the intensity of the patient’s baseline perception of dysequilibrium had a significant relationship to oscillopsia at discharge, such that the greater the intensity of dysequilibrium initially, the greater the intensity of oscillopsia at discharge.
Independent Variables Affecting Outcome at Discharge Based on Regression Analysis
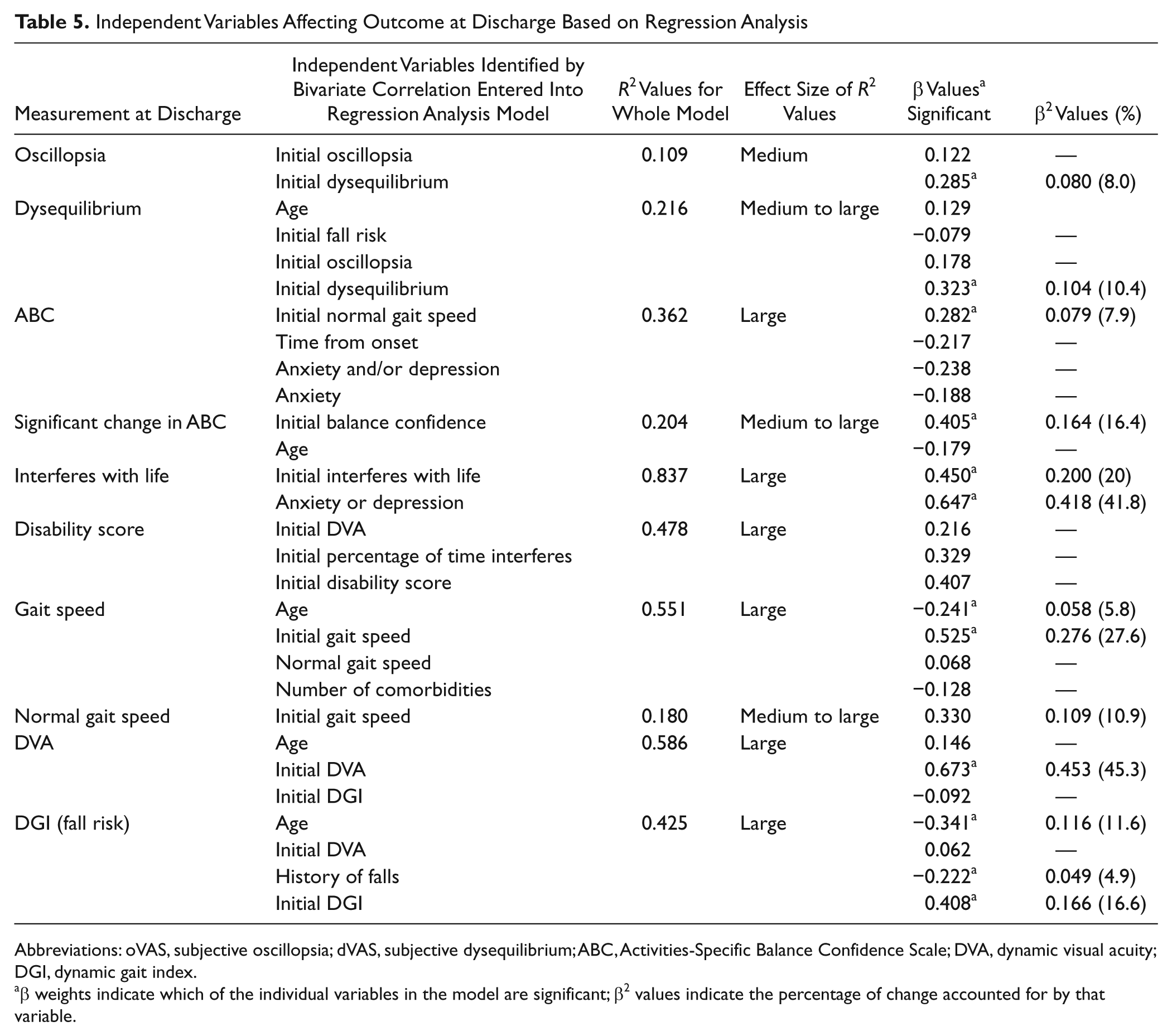
Abbreviations: oVAS, subjective oscillopsia; dVAS, subjective dysequilibrium; ABC, Activities-Specific Balance Confidence Scale; DVA, dynamic visual acuity; DGI, dynamic gait index.
β weights indicate which of the individual variables in the model are significant; β2 values indicate the percentage of change accounted for by that variable.
Dysequilibrium
Initial DGI (fall risk), oscillopsia, and dysequilibrium scores were significantly correlated with dys-equilibrium at discharge. Only initial dysequilibrium was a significant factor explaining dysequilibrium at discharge. Patients with greater intensity of dysequilibrium initially had a greater intensity of dysequilibrium at discharge.
Balance confidence
Normal gait speed initially, time from onset, the presence of a psychological problem (anxiety and/or depression), and the presence of anxiety alone were entered into multiple regression analysis. Patients with normal gait speed at baseline were more likely to have increased balance confidence at discharge. Time from onset and the presence of anxiety and/or depression had near-significant associations. For significant change in the balance confidence score (ie, at least a 10-point change), age and initial balance confidence scores were entered into the model. Only the initial balance confidence had a significant relationship to change in balance confidence score.
Percentage of time symptoms interfere with life
PSIL at baseline and the presence of anxiety or depression were entered into the regression analysis. Greater initial symptom interference and the presence of anxiety and/or depression were associated with a higher score after rehabilitation.
Disability score
Initial DVA, initial PSIL, and initial disability score were entered into the regression analysis. No single independent variable explained disability at discharge. Multicollinearity explains this finding and does not affect the goodness of prediction.
Gait speed
Age, initial gait speed, normal initial gait speed, and number of comorbidities were entered into the analysis. Only the initial gait speed and age explained gait speed at discharge. Patients with faster gait speed initially, even though abnormal for age and gender, were more likely to have faster gait speed and were more likely to return to normal gait speed for age and gender after intervention. As expected, the older the individual, the slower the gait speed, even after intervention.
Visual acuity during head movements
Age, initial DVA, and initial DGI were entered into the model. Only initial DVA explained significant improvements in DVA. The higher the DVA score initially (indicative of greater impairment), the greater the likelihood of significant change in DVA at discharge. Initial DVA and degree of asymmetry of vestibular function were entered into the model for return to normal DVA. Patients with smaller asymmetries in vestibular function were more likely to return to normal DVA for age.
DGI score
Initial DVA, history of falls, initial DGI score, and age were entered into the model. Age, initial DGI score, and history of falls explained DGI score (fall risk) at discharge. Older patients were more likely to remain at risk for falling even though their DGI scores improved. Baseline DGI scores and presence of history of falls were associated with lower DGI scores at discharge.
Discussion
Although studies such as this one, with no control group, cannot provide definitive evidence that exercise intervention results in improvement in outcome in patients with vestibular hypofunction, 75% to 88% of our patients showed significant improvement in the outcome measures used in the study. At least 1 randomized controlled trial has demonstrated 100% of patients showing improvement in DVA and subjective complaints; however, these studies were on a relatively small number of patients and therefore may have not have included a wide enough sample of patients. 3
Patients improved on at least some outcome measures, but not all. The characteristics associated with improvement depended on the specific measure. More detailed identification of factors, such as the patient’s coping mechanism, personality traits, and family support, may help characterize those patients who are unlikely to improve and may lead to the development of better interventions.
Age and Gender
Results from numerous studies suggest that age is not a factor in achieving improvement in subjective complaints, visual acuity during head movement, gait speed, and DGI scores in patients following a course of vestibular exercises.3,8,27,28 We found that age did not affect whether improvement in function would occur. However, at discharge, older patients walked more slowly than younger individuals and were more likely to remain at risk for falling.
Less is known about the role of gender in recovery. One study showed that at 3 months following resection of vestibular schwannoma, male patients reported a greater perception of handicap than did female patients; however, there was no effect of gender at 1 year. 29 We did not find a relationship between gender and any outcome measures studied. Most of our patients, however, had vestibular hypofunction from problems other than resection of vestibular schwannoma.
Time From Onset
The longer the time from onset to initiation of exercises, the poorer the balance confidence after rehabilitation. However, time from onset accounted for only 4.9% of balance confidence at discharge, which is a relatively small effect. We did not find any relationship between time from onset and any other outcome measure. Although other studies have similarly suggested that time from onset is not a factor in recovery in patients with chronic problems, Bamiou et al 30 found that patients who started the rehabilitation process within 6 months of onset had a greater improvement in disability scores than those who started at a later time. 3
Degree of Deficit
The greater the degree of deficit (percentage asymmetry), the less likely that DVA was normal at discharge. Degree of deficit, however, was not related to improvement in other outcome measures. This is in contrast to another study that reported that for patients status postresection of vestibular schwannoma, degree of preoperative canal paresis was a significant factor in the patients’ perception of handicap postoperatively. 29 Because we did not examine etiology as a factor that might influence outcome, we may have missed some significant relationships.
Comorbidities
Relatively little is known about the effect of comorbidities on outcome in patients with vestibular hypofunction. Several studies have suggested that patients with migraine improve equally in physical activities but have greater perceived handicap than patients without migraine.9,15,31 In our study, no specific comorbidity was related to outcome measures at discharge. However, we found that the presence of migraine had a strong relationship with the presence of depression and/or anxiety. This finding is similar to that of Best et al 9 who found that patients with vestibular migraine continued to have high levels of anxiety even 1 year after onset. We were surprised that no other comorbidity demonstrated a strong relationship to outcomes. Possible factors influencing the results may be the low numbers of patients with specific comorbidities as well as the lack of disease-specific information; for example, pain associated with arthritis might have been more important than the presence or absence of arthritis itself.
There was a trend for more than 3 comorbidities to be associated with slower gait speed at discharge. This relationship, although not statistically significant, is in agreement with another study that suggested that patients with multiple comorbidities do not show as great an improvement as those with only 1 comorbidity. 32
Quality of Life and Psychiatric and Psychological Factors
We expected that the presence of psychological problems would be negatively related to subjective complaints and functional measures. Krebs et al 33 noted that some patients with bilateral vestibular hypofunction developed depression that prevented participation in vestibular rehabilitation, thus affecting outcome. Other studies have identified somatization, negative mood, dissatisfaction with social support, poor self-esteem, and anxiety as factors that contribute to perceived disability in patients with dizziness.34-36 The only relationship we found, however, was the patient’s perception of how much symptoms interfered with activities before rehabilitation, and the presence of either depression or anxiety were independently related to the patient’s perception of the PSIL at discharge. This relationship was very strong, and these 2 baseline measures together accounted for almost 62% of the variance. In these patients, a recommendation for counseling may be beneficial.
Study Weaknesses
Inherent in all retrospective studies is the problem of missing data. In our study, data were missing for several reasons. Although we had been using most of the scales as outcome measures since 1990, we added gait speed and PSIL as outcome measures in 1999 and 2003, respectively. We performed the final (discharge) assessments over 2 visits because of time constraints, and some patients did not return for the final visit. Individual therapists at times did not obtain all the discharge measurements. We did not use a specific measurement to assess the patients’ perceptions of overall improvement, which would have been of considerable interest. However, the measures used cover the primary impairments and functional problems for people with UVH (perception of oscillopsia and dysequilibrium with head movement, risk for falling, poor visual acuity during head movement, and low confidence in balance). Our criterion for improvement in gait speed was based on a return to normal gait speed for age and gender. It would have been interesting to use meaningful change in gait speed as a criterion. 37 Using a small meaningful change of 0.05 m/s and a substantial change of 0.10 m/s for gait speed, all our participants (Figure 2B) were correctly classified as either having or not having a meaningful change in gait speed. Finally, there were several measures that, in hindsight, would have been of interest to include in the analyses, including the effect of etiology on outcome and whether or not depression and anxiety changed over the course of the rehabilitation process.
Conclusion
Although most patients with UVH show excellent improvement after a course of vestibular exercises, a number of patients do not improve or improve only in some areas. Some factors examined, for example, gender, were not related to any outcome measure. There were a number of relationships in which single factors measured at baseline were related to an outcome measure at discharge. For example, the greater the time from onset before rehabilitation was initiated, the worse the patient’s balance confidence at discharge, suggesting that earlier referral for vestibular rehabilitation would be beneficial. Patients with greater loss of vestibular function were less likely to return to normal DVA following a course of vestibular exercises, although they still showed significant improvement. Similarly, older patients had poorer DGI scores at the end of the rehabilitation process than younger patients, although they still improved. Several models are offered in which multiple factors measured at baseline are related to outcome measures at discharge. The strongest of these models was the following: the greater the percentage of time symptoms interfere with activities initially plus anxiety or depression, the greater the time symptoms will interfere after vestibular rehabilitation. Second, gait speed at discharge was explained by patient age and initial gait speed. Third, DGI score at discharge was related to age, fall history, and initial DGI score. Fourth, disability at discharge was related to the combined effect of initial DVA, PSIL, and initial disability score. At initial evaluation, therapists can use this information to temper their expectations and to initiate specific treatments—for example, introducing the use of an appropriate assistive device earlier in treatment. Future studies should examine referral of patients to a psychologist as potentially improving the outcome in vestibular rehabilitation of patients with UVH.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.