
Abstract
Background. Sensory loss is common after stroke, with negative impact on exploration of the immediate environment, hand function, and return to daily activities. Objective. To compare the effectiveness of a perceptual-learning based sensory discrimination program versus non-specific exposure to sensory stimuli via passive movements and grasping of common objects. Methods. The authors conducted a randomized parallel-group controlled trial, with blinding of subjects, clinical assessors, and data analysts. Fifty subjects with impaired texture discrimination, limb position sense, and/or tactile object recognition (>6 weeks, median 48 weeks poststroke) were randomized to receive somatosensory discrimination training (n = 25) or repeated exposure to sensory stimuli (n = 25) in 60-minute sessions for a total of 10 hours. The primary outcome was change in a composite standardized somatosensory deficit (SSD) index following intervention. Follow-up was at 6 weeks and 6 months posttraining. Results. Between-group comparisons revealed a significantly greater improvement in sensory capacity following sensory discrimination training, t(47) = 2.75, P = .004, 1-tailed; mean between-group change = 11.1 SSD; confidence interval 3.0 to 19.2. Improvements were maintained at 6 weeks and 6 months. Conclusion. Sensory discrimination training can achieve significant improvements in functional sensory discrimination capacity after stroke. The clinically oriented training achieved transfer of training effects to novel stimuli. Our findings provide support for introducing SENSe discrimination training in rehabilitation of sensory deficits after stroke.
Introduction
Loss of body sensations, such as touch discrimination occurs in 50% to 85% of stroke patients. 1,2 This loss impairs the person’s ability to explore the immediate environment 1 and execute everyday tasks such as grasping and manipulating objects. 3,4 It negatively affects quality of life and personal safety, and prolongs hospital stay. 1,5,6 Yet sensory loss is often neglected in the clinic. 1,7 Clinicians either do not treat the problem or employ methods lacking a sound theoretical or empirical basis. 8
Currently, we do not have high level evidence for the effectiveness of sensory retraining on improving sensory discrimination in the hand after stroke. 1,5,8-10 Although somatosensory stimulation protocols have been systematically reviewed, mostly in regard to motor recovery and transient effects, 10 there are a limited number of retraining approaches that focus on sensory discrimination and sustained improvement. 11 The need for high-quality research in the “. . . treatment of ‘neglected’ impairments such as . . . sensory loss” 12 has been recently highlighted. 9-11
We systematically developed an approach to training sensory discrimination of the hand, 13,14 in line with the Framework for Development of Complex Interventions. 15,16 Our novel approach is based on perceptual learning, consistent with “learning-dependent” neural plasticity 8 and is designed to facilitate transfer of training effects to novel stimuli. 14 It requires the individual to calibrate his or her impaired touch sensation internally by reference to a more normal touch sensation experienced through the “unaffected” hand (intramodal calibration) and via vision (cross-modal calibration), given cross-modal plasticity. 17 Deliberate use of anticipation, attentive exploration with vision occluded, and feedback are also employed to enhance salience of important sensory attributes. 8 To date we have demonstrated clinically and statistically significant effects for task specific training of texture discrimination (z = −8.6, P < .0001) and limb position sense (z = −4.3, P < .001) and for transfer of training effects to novel texture stimuli (z = −5.7, P < .001) based on meta-analyses across a total series of 30 controlled single-case experiments. 8
The objective of the current study was to compare the effectiveness of our approach to sensory discrimination training of the upper limb with the control intervention of repeated exposure to sensory stimuli in stroke patients with sensory impairment using a randomized controlled trial. We selected the most optimal approach to training investigated by us, that is, generalization enhanced sensory training, 14 and applied it to training of texture discrimination, limb position sense, and recognition of everyday objects through the sense of touch in a clinical training package. We hypothesized that stroke survivors receiving the discrimination training would demonstrate significantly greater improvement in sensory discrimination capacity in comparison with the control intervention, with maintenance at follow-up.
Methods
Participants
Stroke survivors with impaired texture discrimination, limb position sense, and/or tactile object recognition, identified clinically and by standardized tests below, were recruited at least 6 weeks poststroke. They were eligible to participate if they were medically stable, had adequate comprehension of instructions 18 and perceptual ability for assessment, and were able to commit time to participate in the rehabilitation program. They were excluded if they had evidence of unilateral spatial neglect, based on standard neuropsychological assessments, 19,20 or prior history of other central nervous system dysfunction or peripheral neuropathy. They were recruited from 6 participating hospitals in metropolitan Melbourne. This included rehabilitation and long-term community-based facilities associated with the hospitals. Patients were recruited to the study after they had completed their inpatient and outpatient therapy or community-based follow-up, to minimize any confound with co-therapies. Most were living at home or in supported accommodation at the time of the study. Potential participants, referred by hospital clinicians, were screened by research therapists for eligibility. They were recruited consecutively as they became available. All participants gave voluntary informed consent and procedures were approved by Human Ethics Committees of participating hospitals and La Trobe University.
Sample Size
Power estimates were based on our prior study investigating generalized training effects. 14 Outcome data were extracted at phase transitions to mimic the proposed design. The very large standardized effect sizes indicated by that analysis (Cohen’s d >5) yielded powers in excess of 99% for even quite small samples (eg, n = 20). Inclusion of 50 allowed for some attrition and investigation of therapeutic effects on a larger sample.
Study Design
A randomized prospective parallel-group controlled trial was conducted that employed between-group and within-subject experimental controls. The primary outcome was the between-group difference in sensory discrimination capacity at the end of phase 1 following sensory discrimination training. In phase 2, the control group received the sensory discrimination training in a cross-over arm whereas the experimental group received a second period of sensory training. This approach is resource efficient, permits investigation of the additional benefits of sensory training beyond the current exposure only approach with the person acting as their own control, and permits investigation of treatment dosage. Stroke survivors, assessors, and data analysts were blinded to group assignment. Trial conduct and reporting followed the Consolidated Standards of Reporting Trials (CONSORT) statement for Randomized Trials. 21,22 The study was registered with the Australian New Zealand Clinical Trials Registry (ACTRN012605000609651).
Randomization
Randomization was computer generated, with proportional sampling to control for side of lesion (and gender). Allocation to intervention was concealed from recruiting therapists. Independent assignment was managed centrally by a researcher who did not have any contact with stroke survivors and had only remote contact with treating therapists to inform them of allocation via sealed opaque envelopes or electronic mail just prior to commencement of intervention, thus the sequence of allocation was concealed from recruiting and treating therapists. Consecutive assignment occurred by randomly allocating the first arriving right-sided lesion subject to the experimental or control group, with the next right-sided lesion subject (of the same gender) going to the other group. The process was repeated for each consecutive pair of right-sided or left-sided lesion subjects, the first member always being allocated at random. The person assigning subjects was different to the executors of the assignment.
Masking
Both experimental and control protocols were presented to stroke survivors as therapeutic activities, to control placebo effects. As both involved presentation of sensory stimuli and manipulation of objects, it was expected that stroke survivors would not be aware that exposure was a control condition, in accord with our previous observations. Exposure to sensory stimuli is sometimes used as a clinical treatment, and therapists were not informed as to which condition was expected to yield the major improvement. However, intervention double-blinding cannot be guaranteed, as the treating therapist may have understood the difference between protocols. An independent therapist conducted outcome assessments and was blind to group membership. Outcomes were scored, entered, and analyzed by independent researchers blind to group allocation and having no contact with participants.
Intervention and outcomes schedule
A phase consisted of 10 intervention sessions, each of approximately 60-minute duration, conducted 3 times a week. Assessment of outcome was conducted as follows: just before commencement of phase 1 (A0), at the end of phase 1 following experimental or control intervention (A1), at the end of phase 2 following experimental intervention for both immediate and delayed intervention groups (A2), and at 6 weeks (A3) and 6 months (A4) postintervention. A treatment log was kept for each individual. During the study, participants were not permitted to be involved in any other sensory retraining and were asked not to deviate from their normal pattern of exposure to sensory stimuli. Most participants received the experimental or control intervention at their place of residence.
Baseline information
Age, gender, hand dominance using the Annett Questionnaire, 23 side and site of lesion from report of computed tomography or magnetic resonance imaging scan, stroke type, severity of neurological impairment using the National Institutes of Health Stroke Scale, 18 and severity of global disability using the Barthel Index were ascertained. 24 Background information on somatosensory impairment was obtained for touch detection using WEST-hand monofilaments, 25 texture discrimination using the Tactile Discrimination Test 26 and Fabric Matching Test (FMT), 1 limb position sense using the Wrist Position Sense Test (WPST) 27 and Finger Position Sense Test, 1 temperature discrimination using Roylan hot and cold discrimination kit, A629-1, and tactile object recognition using the functional Tactile Object Recognition Test (fTORT). 28 Baseline information on hand function, using the Sequential Occupational Dexterity Assessment 29 and the Motor Activity Log, 30 was also obtained.
Primary Outcome
The primary outcome measure was a composite index of functional somatosensory discrimination capacity, derived from standardized indexes of texture discrimination, limb position sense, and tactile object recognition. A composite measure was selected a priori as the training program was designed to improve sensation across 3 modalities. Texture discrimination was assessed using the FMT, 1 limb position sense using the WPST, 27 and tactile object recognition using the fTORT. 28 Each measure has age-adjusted normative standards, high reliability (r = .85 to .92), and good discriminative test properties. Assessors were trained in test administration by a skilled practitioner (LC) using a standard protocol.
To derive the composite index, scores on each of the component capacities were first standardized. Principal components factor analysis of preintervention scores was then used to verify that somatosensory deficit could be adequately represented by a unidimensional scale comprising the pooled results of the standardized FMT, WPST, and fTORT scores. Our analysis of the baseline data indicated that all 3 measures loaded strongly on 1 common underlying component (this factor by itself accounted for 71% of the total variance, and subsequent eigenvalues were substantially less than 1). The component matrix showed that each of the 3 measures contributed 0.79 or better to the underlying “somatosensory performance” variable. Thus a simple average of the 3 was computed for the composite measure. It is preferable that the standardized score permit interpretation in relation to performance of age-matched healthy controls and the range of severity of deficit experienced after stroke. The Standardized Somatosensory Deficit (SSD) scale was therefore calibrated so that zero equaled the 5th percentile of healthy performance and negative 100 equaled the 90th percentile of most severely impaired stroke performance, thus minimizing the influence of outliers. Thus, the composite index can be interpreted relative to expected performance.
Interventions
Experimental intervention
The experimental intervention (EI) applied the principles of generalized sensory discrimination training 14 to 3 sensory tasks: texture discrimination, limb position sense, and tactile object recognition. Training employed a variety of stimuli within each sensory dimension trained, graded progression of discriminations from easy to difficult, attentive exploration with vision occluded, anticipation trials, cross-modal calibration via vision, feedback on sensation and method of exploration, intermittent feedback and self-checking of accuracy, feedback on ability to identify distinctive features in novel stimuli, tuition of training principles, and summary feedback and intensive training. 14 During each EI session, subjects were trained on each sensory task, in random sequence, for 15 to 20 minutes at a time. Texture discrimination training used graded stimuli with varying surface characteristics. 14 Limb position sense was trained across a wide range of limb positions of the upper limb. Tactile object recognition training focused on discrimination of shape, size, weight, texture, hardness, and temperature using a range of multidimensional, graded objects.
Control intervention
The control intervention (CI) consisted of non-specific repeated exposure to stimuli varying in texture, shape, size, weight, hardness, and temperature, via grasping of common objects, and passive movements of the upper limb. Exposure was selected as the CI because it is comparable with experience in daily activities and in therapy, the current characteristic experience, and previous studies indicated that most stroke survivors do not show improvement with repeated exposure alone. 13,14 Because exposure can be presented as treatment, it allowed control for nonspecific intervention effects, reactivity to repeated testing, and natural recovery.
Data Analysis
Hypotheses were investigated with planned comparisons contrasting: (a) the reduction in SSD during phase 1 obtained with EI versus with CI (independent groups t test after Levene’s test for homogeneity of variances) and (b) the reduction in SSD obtained for the delayed intervention group during phase 2 (EI) versus phase 1 (CI; paired samples t test). One-tailed tests were used as our hypotheses were directional based on positive findings from our original studies and the fact that “lack of an improvement,” whether because of an inconclusive result or an apparent deterioration in performance, would not be considered a significant result. Confidence intervals (95%) for these mean differences were obtained to estimate typical effect magnitudes. They were also used to quantify the typical gains retained at follow-up. Individual effects of intervention and gains retained were investigated with scatterplots. Data were managed and analyzed using the Statistical Package for Social Sciences (version 17.0; SPSS Inc, Chicago, Illinois).
Results
Study Population
A total of 50 stroke survivors were recruited, as outlined in Figure 1. Of these, 25 were randomized to the EI and 25 to the CI. All received interventions as allocated. Three individuals were lost to follow-up. Patients were recruited from 2003 to 2007, with 6-month follow-up.
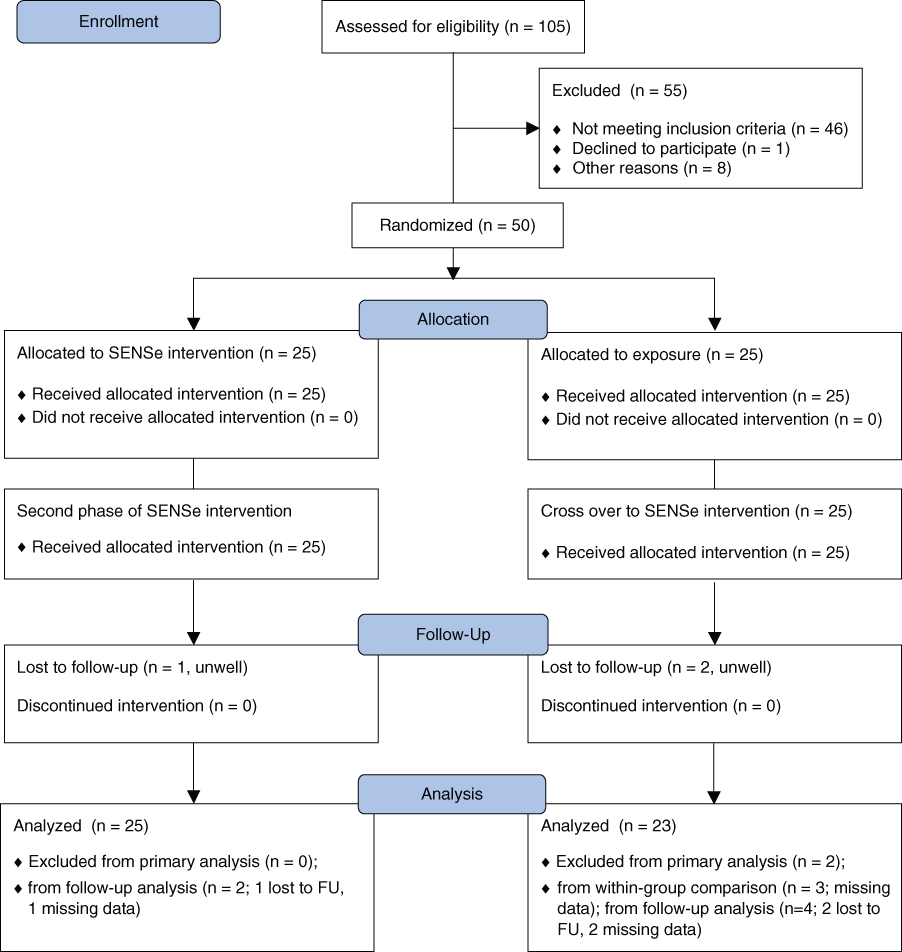
Flow diagram of study profile comparing sensory discrimination training with repeated exposure to sensory stimuli
Demographics and Clinical Characteristics
Baseline demographic and clinical characteristics of the groups were similar at baseline (Table 1). The combined mean age was 61.02 years. In all, 29 had left and 21 had right hemispheric lesions. There were no between-group differences in side of lesion, National Institutes of Health Stroke Scale score, time poststroke, or SSD score at baseline. The median time poststroke at commencement of intervention was 48.14 weeks. Sensory performance on the primary outcome is reported for each group at change of phase and for component sensory abilities at baseline (Table 2).
Demographics and Background Clinical and Somatosensory Details
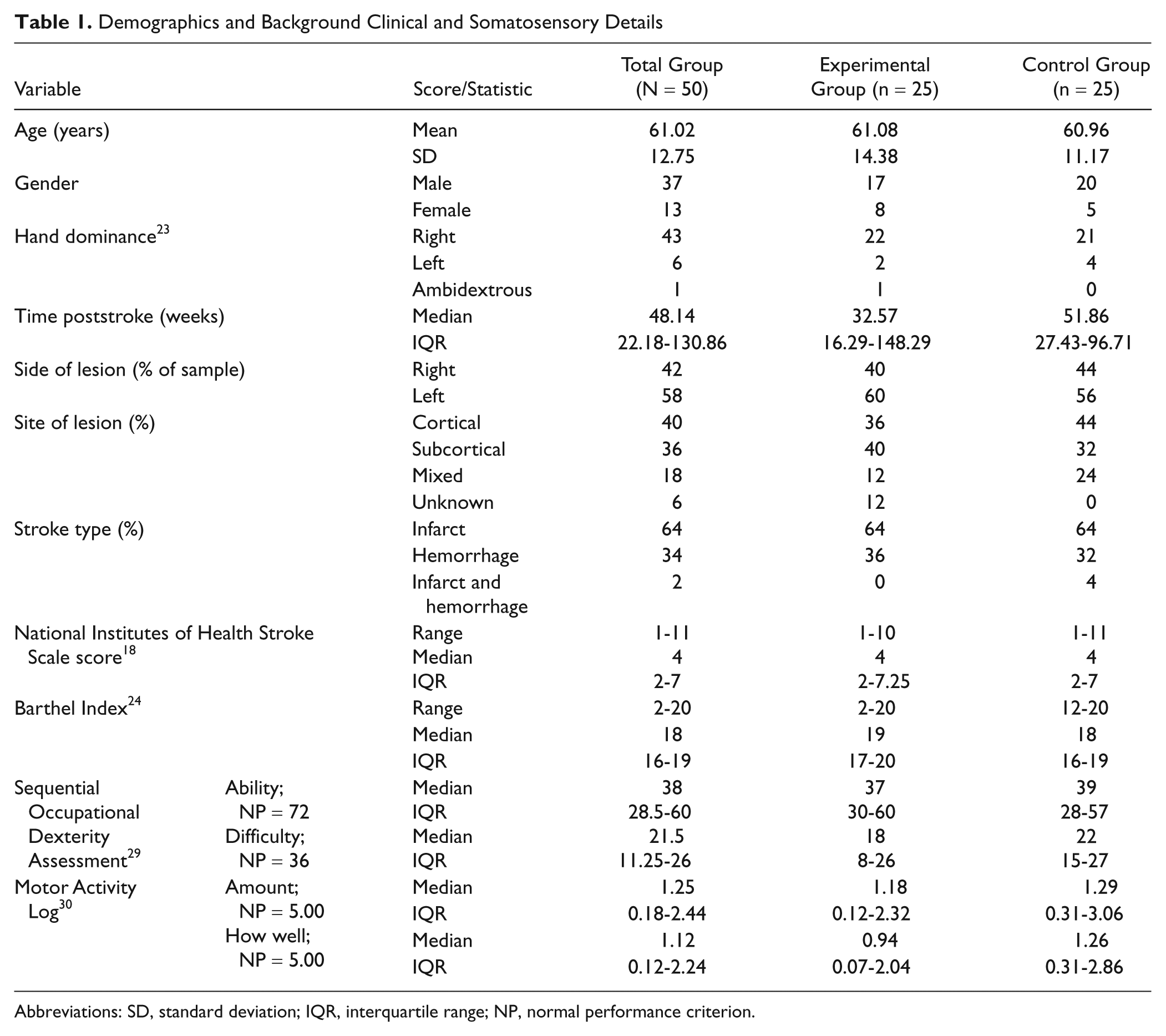
Abbreviations: SD, standard deviation; IQR, interquartile range; NP, normal performance criterion.
Somatosensory Performance at Baseline and Over Time
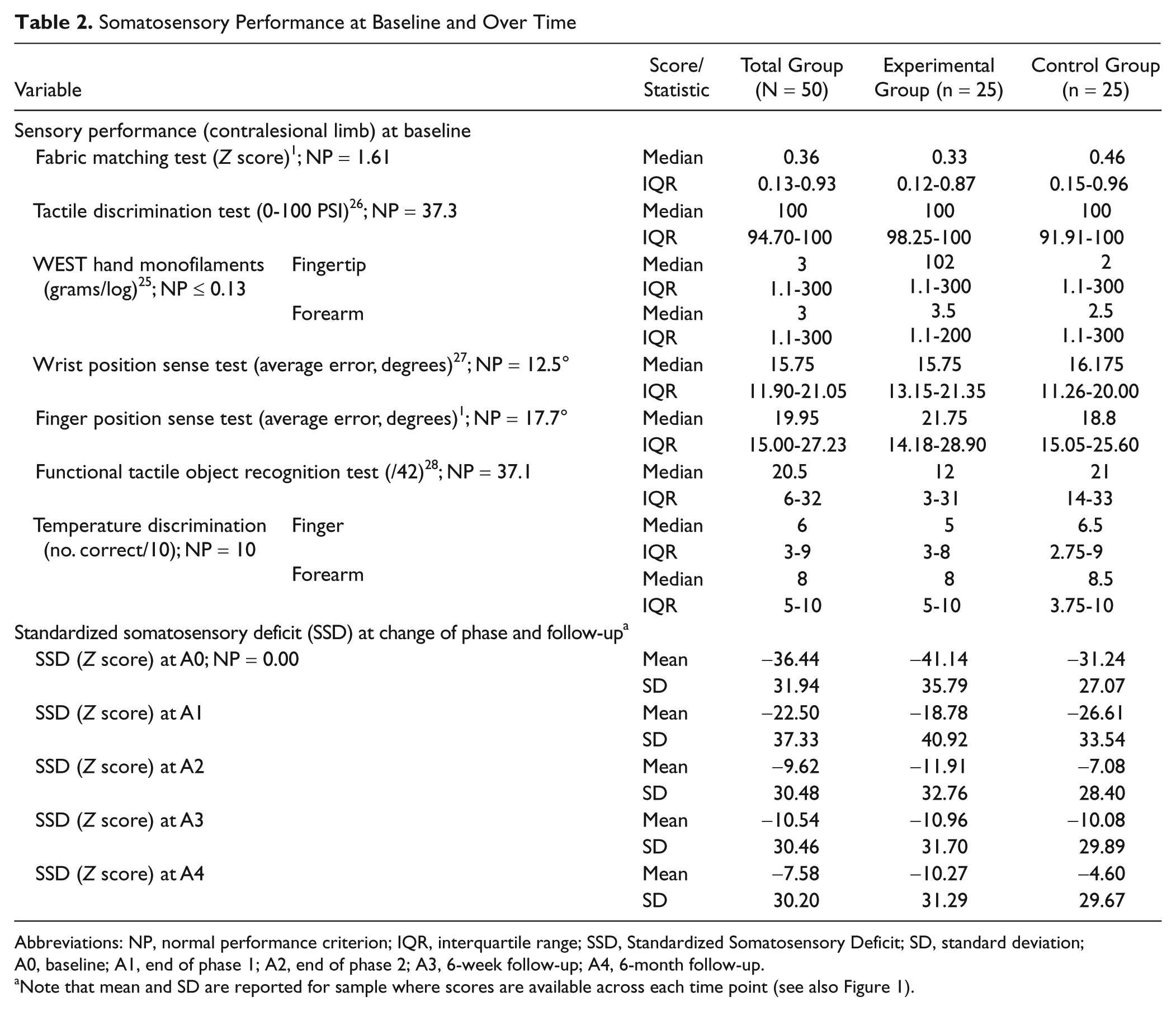
Abbreviations: NP, normal performance criterion; IQR, interquartile range; SSD, Standardized Somatosensory Deficit; SD, standard deviation; A0, baseline; A1, end of phase 1; A2, end of phase 2; A3, 6-week follow-up; A4, 6-month follow-up.
Note that mean and SD are reported for sample where scores are available across each time point (see also Figure 1).
Investigation of Intervention Effect
Results for the primary outcome are presented. There were no adverse events associated with either intervention.
Between-group comparison of an intervention effect
Both immediate and delayed intervention groups showed improvement in the expected direction for the primary outcome across the 5 time points (Figure 2, panel A). Examination of change during phase 1 for those who received the EI revealed a marked improvement of 19.1 SSD (Figure 2). In comparison, the CI group showed a much smaller change on average (8.0 SSD). The planned comparison confirmed that the EI group had a significantly greater improvement in sensory discrimination than the CI group, t(47) = 2.75, P = .004, 1-tailed. The confidence interval for the 11.1 SSD mean between-group change in phase 1 was 3.0 to 19.2 (Figure 2, panel B) and the standard deviation was 4.13 SSD.
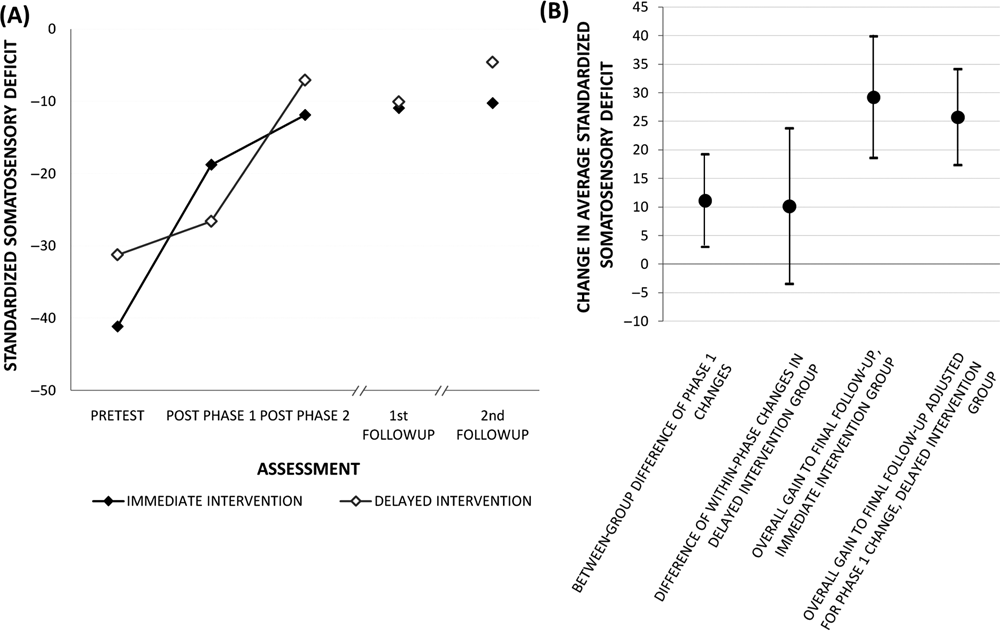
Change in somatosensation over time: Mean standardized deficit at each test occasion and intervention effect for between-group and delayed intervention
Within-group comparison of an intervention effect
During phase 2 (EI), the delayed intervention group showed an average improvement that was 9.4 SSD greater than the improvement obtained in phase 1 (CI; Figure 2). However, this superiority in deficit reduction during EI did not quite reach accepted standards of statistical significance, t(21) = 1.72, P = .05, 1-tailed. Although the reduction of 9.4 SSD (adjusted for change observed during CI) was comparable to the 11.1 SSD change observed for the immediate intervention group, the error margin was larger, yielding a (2-tailed) confidence interval from −3.5 to 23.8 SSD (Figure 2, panel B). Examination of individual change data across phases indicated that the wider standard error was largely because of 5 individuals, all of whom showed marked recovery (>20 SSD) in the CI phase. Four had very mild deficit prior to CI and then plateaued with EI, whereas the fifth showed marked improvement over both phases.
Individual differences and magnitude of intervention effects
Inspection of the magnitude and direction of change over phase 1 suggested a superior improvement for those in the EI group compared with the CI group (Figure 3, panel A). Nearly all in the EI group (22/25) showed a positive change compared to baseline. The scattercloud indicated that the magnitude of change was relatively constant for different levels of impairment severity. In comparison, most individuals in the CI group showed relatively little change (Figure 3A). Those with moderate or severe impairment showed little or no improvement. However, 4 individuals who had only a mild impairment at baseline did show an improvement with repeated exposure alone. Inspection of the magnitude of change for individuals following EI indicates that 36% had a reduction in deficit of at least 50%, 24% were performing in the normal range and only 2 did not show an improvement.
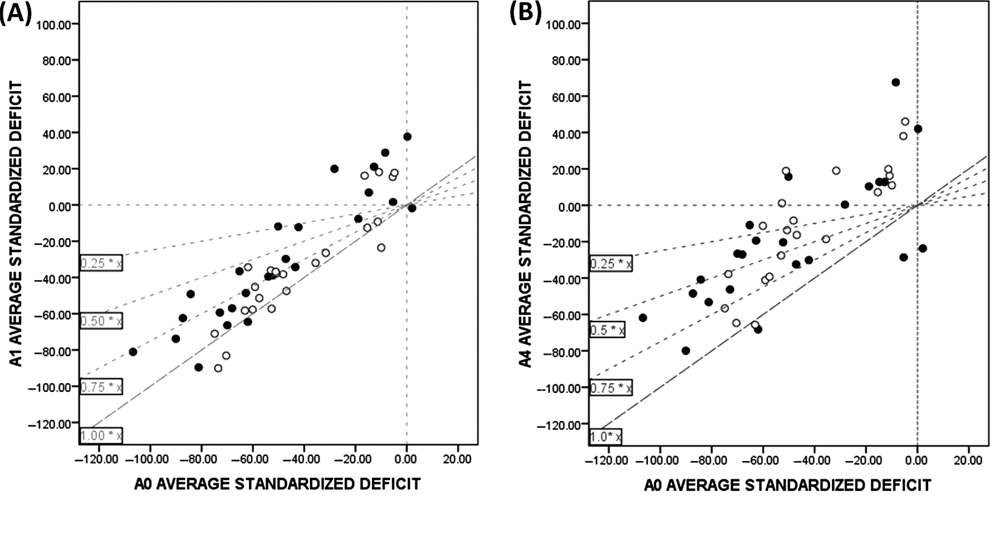
Individual effects of intervention and of gains retained at follow-up
Maintenance and clinical significance of intervention effects
Both groups showed a significant effect of intervention at the 6-week and 6-month follow-ups relative to preintervention status. At 6 weeks, all but 1 individual showed an improvement. A total of 31% (13/42) showed performance within the healthy performance range, 69% reduced their deficit by 50% or more and 83% had a reduction in deficit of ≥25%. A similar pattern was observed at 6 months postintervention (Figure 3, panel B): 36% (16/44) were within the healthy range, 59% showed ≥50% reduction in deficit, 86% showed ≥25% reduction, and 4 individuals had scores less than at preintervention. The overall gain to final follow-up for the immediate intervention group was 29.2 SSD (confidence interval: 18.6 to 39.9; t = 5.56, P < .001) and for the delayed intervention group, when adjusted for phase 1 change, was 25.7 SSD (confidence interval: 17.3 to 34.1; t = 6.37; P < .001).
Discussion
Sensory retraining is effective in improving sensory discrimination capacity in stroke survivors at least 6 weeks after stroke and in the chronic phase of recovery, as indicated by a median time poststroke of 48 weeks at commencement of intervention. A superior between-group intervention effect for the primary outcome of functional sensory discrimination was found (at the end of the first intervention phase) following sensory discrimination training compared with the control intervention of exposure to sensory stimuli. The delayed intervention group also showed improvement following sensory training but did not quite reach accepted standards of statistical significance relative to the control intervention. Magnitude of within-group change was similar to that of the immediate intervention group but showed more variability.
Clinical significance of the intervention effect is evident in the percentage reduction in deficit observed, and maintenance of improvement at 6-week and 6-month follow-ups. Following EI, 36% of stroke survivors showed a halving of their deficit or better. The improvement was maintained and slightly increased at 6 weeks and 6 months postintervention, with 69% and 59% halving their initial deficit or better.
The sensory program was clinically oriented and designed to retrain 3 sensory discrimination functions: texture discrimination, limb position sense, and tactile object recognition. These abilities were selected as they affect function in their own right. 8 As they were addressed simultaneously, the time available to train any one modality was substantially less than for our previous investigations, in which only one modality was trained at a time. 13,14 It is therefore not surprising that the magnitude of change observed seems somewhat lower than when single modalities were trained. In those studies, a larger proportion of participants achieved scores within the normal range for the modality trained. Nevertheless, the positive findings provide strong foundation for dose–response studies to optimize training parameters for individuals.
The program also achieved transfer of training effects to novel stimuli not trained; as stimuli used in assessment were mostly different to the stimuli trained. The degree of similarity–novelty between assessment and training tasks varied in relation to sensory stimuli and discrimination task required for different modalities. For example, texture discrimination was trained across texture stimuli with potentially different distinctive features, that is, from training on rubber, glass, leather, and sandpaper to transfer on fabrics (that were not trained). 14 Training limb position sense in the upper limb involved multiple and single joints and used a defined subset of limb positions. Although some positions used in the WPST assessment were similar to positions used in the training sets, the discrimination task required for the WPST (judging a specific limb position within the full range available) was somewhat different to the training task, where the individual had to judge a position from a predefined set of limb positions (usually 3 to 5) with either large, medium, or small differences between them. Further systematic investigation of transfer across these varying conditions is suggested.
A recent systematic review reported on “passive” and “active” approaches to sensory retraining. 10 It was highlighted that there is currently insufficient evidence about “active” approaches to sensory rehabilitation, and none of these had level II evidence (properly designed randomized control trial) for retraining the upper limb. Similarly, a recent Cochrane review that focused on interventions for sensory impairment in the upper limb, also reported on the relative lack of high-quality randomized controlled trials. 9 The findings from our randomized controlled trial directly address this gap. They are also consistent with meta-analyses of intervention effects obtained in our series of single-case experiments. 8 In the current study, we examined effectiveness of training stroke survivors with varying severity of impairment using trained therapists. Demonstration of significant training effects that are of a relatively large magnitude and maintained over time contributes to the evidence-base supporting introduction into clinical practice. Identification of patient characteristics that may impact on the ability to benefit from training will assist targeting of services to appropriate individuals. Finally, the impact of SENSe training on related functional outcomes, and the relationship between improved sensation on function, is also important in judging the clinical significance of the intervention. Upper limb function (assessed using the Sequential Occupational Dexterity Assessment) and actual use of the upper limb (Motor Activity Log) were measured as secondary outcomes and will be the focus of a subsequent report.
Conclusion and Implications
Our findings provide support for introducing sensory discrimination training to the rehabilitation of stroke survivors with a sensory deficit at least 6 weeks poststroke and in the more chronic phase of recovery. We have shown evidence of the clinical value of sensory retraining through quantification of the magnitude of training effects and maintenance of gains at short and long-term follow-ups. The approach aims to improve lost abilities rather than focus on compensation, and can be used by therapists in rehabilitation and home settings. This is a significant outcome for stroke rehabilitation, given the high prevalence of sensory loss and the negative impact on efficient exploration of the environment and performance of everyday activities.
Footnotes
Acknowledgements
We thank the survivors of stroke for their involvement in the study, the therapists who conducted the assessment and training sessions, and the research assistants who helped with data entry and checking. We also acknowledge Professor Derick Wade, who provided input in the early design phase.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the National Health and Medical Research Council (NHMRC) of Australia [project grant number 191214, and Career Development Award number 307905 to L.M.C]; an Australian Research Council Future Fellowship awarded to L.M.C. [number FT0992299]; the National Stroke Research Institute of Australia and by the Victorian Government’s Operational Infrastructure Support Program. The funding sources had no role in conduct of the study or writing of the report.