
Abstract
Background. Deterioration of motor function is one of several clinical manifestations following traumatic brain injury (TBI) in children and adolescents. Objective. To investigate the relationship between white matter (WM) integrity using diffusion tensor imaging (DTI) and motor functioning in young TBI patients. Methods. A group with moderate to severe TBI (n = 24) and a control group (n = 17) were scanned using DTI along with standard anatomical scans. Using ExploreDTI software, WM regions/tracts that carry efferent output (motor) from the brain were evaluated, as well as the corpus callosum, brainstem, internal capsule, and subcortical WM structures. Motor function was assessed using the Movement Assessment Battery for Children (M-ABC), consisting of manual dexterity, ball skills, and static and dynamic balance items. Results. TBI patients were less successful on the M-ABC than the controls and showed lower WM fractional anisotropy (FA) in the corpus callosum, anterior corona radiata, corticospinal tract, and cerebellum. Decreased FA was associated with lower motor performance in the TBI group but not in the control group. Conclusion. This study provides evidence for a structural alteration of motor pathways and regions in children and adolescents with TBI that are correlated with motor functioning. Further studies may be able to identify therapeutic targets and monitor the effects of new interventions.
Keywords
Introduction
Accurate elucidation of lesions in patients with traumatic brain injury (TBI) is essential for predicting behavioral outcome and for guiding treatment strategies. Diffuse axonal injury (DAI) is the predominant mechanism of injury in TBI, and its sequelae are the most frequent cause of poor clinical outcome. 1 DAI is characterized by widespread axonal damage due to shearing forces by acceleration, deceleration, or rotation of the brain. DAI most commonly affects white matter (WM) in areas including the corpus callosum, subcortical WM structures, and the brainstem. 2,3 Motor disorders are common and disabling symptoms in children and adolescents with TBI. 4,5 However, the diagnosis of lesion severity is difficult because conventional brain magnetic resonance imaging (MRI) is not sufficiently sensitive in detecting DAI.
Recent advances in diffusion tensor imaging (DTI) demonstrate improved sensitivity to DAI. 6 DTI characterizes the properties of water diffusion in the brain, that is, the magnitude of diffusion (mean diffusivity [MD]), the directionality of diffusion (fractional anisotropy [FA]), and its predominant orientation. 7 Diffusion of water molecules in healthy WM is highly directional or anisotropic, occurring more readily along axons, because of natural barriers (cell membranes, myelin, and adjacent axons). Damaged WM bundles have increased diffusion perpendicular to axons and lower anisotropy relative to healthy WM. 8,9 Multiple groups have demonstrated reductions in FA in the chronic phase of mild, moderate, and severe pediatric TBI. 10-13 Moreover, several studies have provided support for an association between FA and injury severity 13 or neurocognitive functioning 12 after pediatric TBI. Although motor problems, and especially long-term motor problems, may have substantial negative consequences for the quality of life, only a few DTI studies have investigated associations between microstructure and motor impairments in TBI. 14,15 In these studies, injury in both efferent and afferent pathways was found to correlate with reduced postural control and eye–hand coordination using instrumented measures. Although quantitative movement analyses achieve a high degree of validity and reliability, they cannot include the whole movement repertoire. These methods often focus on simple motor tasks (hand movements) or basic movement patterns (postural control), and they often require elaborate technical equipment and time-demanding data evaluation. Moreover, the need to focus on selected motor tasks limits the number of eligible patients who can participate and may also impede the detection of changes in motor proficiency. Therefore, we decided to perform assessments of gross and fine motor skills using a clinical motor test battery in the present study.
Our study was designed to establish the relationship between WM diffusion abnormalities and chronic impairment of motor function after TBI in children and adolescents. The first aim was to assess degree of motor behavior impairment in TBI patients when compared with normally developing controls with respect to manual dexterity, balls skills, and balance. Then, DTI was used to determine the integrity of anatomical structures associated with motor performance in an attempt to quantify structural brain damage. The ultimate aim was to investigate the neural basis of motor deficits in TBI by correlating impairments in behavior to microstructural damage in motor-relevant brain regions.
Materials and Methods
Participants
Forty-one children and adolescents participated, including 24 subjects with TBI (mean age, 14.4 years; SE = 7 months; 15 boys and 9 girls) and 17 controls (mean age, 12.4 years; SE = 6 months; 9 boys and 8 girls). The TBI patients were recruited from different rehabilitation centers in Belgium, and their demographic and clinical characteristics are shown in Table 1. The TBI patients were classified as “moderate to severe” based on several factors: the Glasgow Coma Scale score after resuscitation (a subgroup of 8 children had a GCS of 12 or less), the anatomical features of the injury based on inspection by an expert neuroradiologist (see the following), and the injury mechanism (traffic accidents and falls), or combinations thereof. The interval between injury and scanning (age of injury) was on average 4 years, 11 months (SE = 9 months). Their age at injury was on average 9 years, 8 months (SE = 9 months). Although a significant proportion of the TBI group regained ambulatory and self-care skills, many suffered from long-term motor deficits, including spasticity (altered tonus), ataxia (uncoordinated muscle movements), bradykinesia (slowing of movements), reduced range of motion, altered locomotion, imbalance, and/or tremor. Participants were excluded if they had preexisting developmental or intellectual disabilities, a progressive disease, or were taking medication. All control subjects were screened to ensure that they had no history of neurological damage.
Clinical Characteristics of TBI Patients
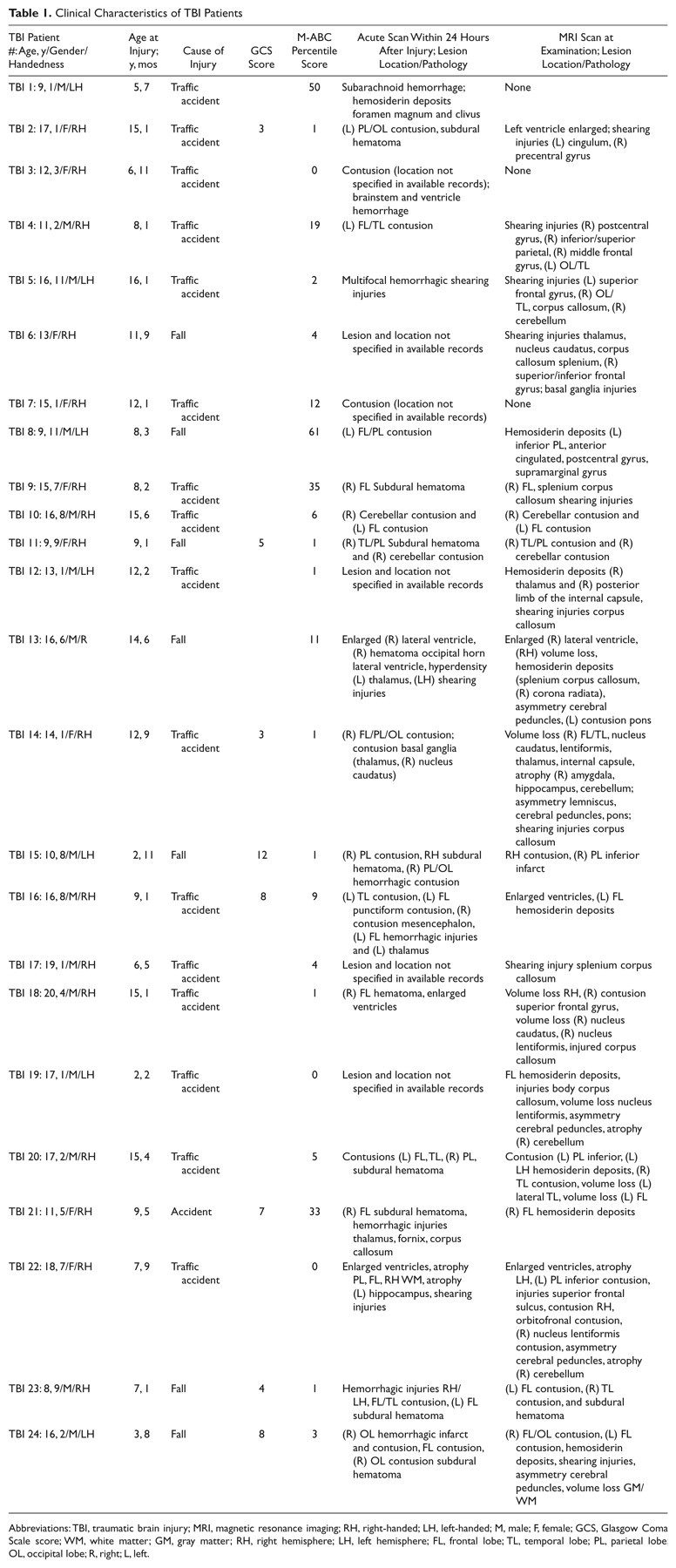
Abbreviations: TBI, traumatic brain injury; MRI, magnetic resonance imaging; RH, right-handed; LH, left-handed; M, male; F, female; GCS, Glasgow Coma Scale score; WM, white matter; GM, gray matter; RH, right hemisphere; LH, left hemisphere; FL, frontal lobe; TL, temporal lobe; PL, parietal lobe;OL, occipital lobe; R, right; L, left.
The parents of all participants gave written informed consent. The consent forms and study protocol were approved by the local ethics committee of biomedical research at Katholieke Universiteit Leuven.
Movement Assessment Battery for Children
Motor function was assessed by using the Movement Assessment Battery for Children (M-ABC). 16,17 The M-ABC is designed for diagnosis of delays or deficits in motor development and shows good reliability and validity. 18-23 It consists of 4 age-related items sets (4-6, 7-8, 9-10, and 11-12 years). Performance of older children was scored according to the norms for 12-year-old children, and they were age-matched for statistical comparison. Each item set was built of 8 tasks, which were assessed via the following 3 subtests: manual dexterity (eg, placing pegs, shifting pegs by rows, threading lace, tracing a trajectory with a pen between 2 curved lines that resembles the shape of a flower), ball skills (eg, throwing a bean bag in a box, throwing a ball at a wall target, catching a ball with 1 hand), and static and dynamic balance (eg, walking backward, hopping in squares, 2-board balance, jumping and clapping). Each item was scored on a scale from 0 to 5. High scores indicated poor motor performance. Summing up the item scores within the 3 subtests produced a performance profile for each subject. The manual dexterity subtest score varied from 0 to 15, the ball skills subtest subscore from 0 to 10, and the static and dynamic balance subtest from 0 to 15. The 3 subtest scores were summed to provide a total test score ranging between 0 (very good) and 40 (extremely impaired). This total score can be expressed as a percentile score that shows a participant’s level of performance in comparison with peers (as shown in Table 1).
MRI Data Acquisition
MR examination took place without sedation on a 3T scanner (Intera, Philips, Best, the Netherlands) with an 8-channel, phased-array head coil. A DTI SE-EPI (diffusion weighted single shot spin-echo echoplanar imaging) was acquired with data acquisition matrix = 112 × 112; field of view (FOV) = 220 × 220 mm2; TR = 7916 ms, TE = 68 ms, parallel imaging factor 2.5, and 68 contiguous sagittal slices (slice thickness = 2.2 mm; voxel size = 2 × 2 × 2.2 mm3) covering the entire brain and the brainstem. A pair of diffusion gradients was applied along 45 noncollinear directions with a b-value of 800 s/mm2. Additionally, one set of images with no diffusion weighting (b = 0 s/mm2) was acquired.
A T1-weighted coronal 3D-TFE (182 contiguous coronal slices covering the whole brain and brainstem; FOV = 250 mm; TE = 4.6 ms; TR = 9.7 ms; slice thickness = 1.2 mm; matrix size = 256 × 256; voxel size = 0.98 × 0.98 × 1.2 mm3) was consequently acquired for anatomical detail (Table 1). These structural MRI scans were investigated by an expert neuroradiologist to indicate location and type of pathology (eg, gliosis, shearing, hemorrhage; see Table 1).
DTI Processing
The DTI data were analyzed and processed in ExploreDTI 24 using the following multistep procedure. The DTI data sets were corrected for subject motion and eddy current–induced geometric distortions. 25 The DW images were realigned to the non-DW image using an affine coregistration method based on mutual information with cubic interpolation to resample the images. 26 During this correction procedure, the b-matrix was adjusted for the rotational component of subject motion to ensure correct diffusion tensor estimates. The diffusion tensor model was fitted to the data using the Levenberg–Marquardt nonlinear regression method. 27 The diffusion measure FA was subsequently calculated as described previously. 28 The first step in the DTI coregistration process consisted of the construction of a population-based MNI template. 29,30 With this template, an affine and, subsequently, a high-dimensional nonaffine DTI-based coregistration technique could be applied to obtain the final DTI data sets in MNI space. 31,32 In the nonaffine coregistration approach, the images are modeled as a viscous fluid, imposing a constraint on the local deformation field. During normalization, the Jacobian is constrained to reduce the chance of forcing the underlying brain structures in an anatomically nonplausible way. This viscous fluid model was optimized for aligning multiple diffusion tensor components and has been applied successfully in a wide range of applications, where adjusting for morphological intersubject (and intergroup) differences, such as, for instance, ventricle size, is considered to be of paramount importance. 33-36 Based on a recently developed simulation framework, the nonaffine DTI-based coregistration method, in particular, has been shown to provide highly accurate registration results. 37 Each scan was visually checked for accuracy after both the motion correction and coregistration steps.
Definition of Regions of Interest (ROIs)
The WM parcellations, developed by Mori et al, 29 were applied to the normalized images and the corresponding FA values averaged across the 3D ROI labels. In doing so, the following 8 WM tracts and regions were defined: the corpus callosum, corticospinal tract, superior cerebellar peduncle, inferior cerebellar peduncle, cerebral peduncle, anterior corona radiata, anterior limb of the internal capsule, and posterior limb of the internal capsule. We also used the add-ons to the analysis software package FSL, 38 which provide other atlases in MNI space, such as the probabilistic cytoarchitectonic atlas, developed by Eickhoff et al, 39 and a digitized version of the original Talairach atlas. 40,41 In particular, we investigated the thalamus, cerebellum, brainstem, and the whole brain WM label. The latter is used here as a global index of WM integrity, that is, a tissue level that is not labeled as gray matter (GM, cortex, and nuclei) or cerebral spinal fluid.
The rationale for proposing the first series of WM regions was based on previous research, labeling those as being vulnerable in patients with TBI, including the corpus callosum, subcortical WM structures (thalamus and cerebellum), internal capsule, and brainstem. 42 Furthermore, we were interested in WM alterations in the motor pathways at different levels of the brain. Therefore, WM regions/tracts that carry efferent output were selected, such as the corticospinal tract, cerebral peduncle, anterior corona radiata, internal capsule (anterior and posterior limb), and cerebellar peduncles (superior, inferior). For visualization purposes, tracts were reconstructed on a 3D T1-image for a single representative subject, and regions were presented on FA maps of the WM atlas of Mori et al 29,43 in Figures 1 and 2, respectively.
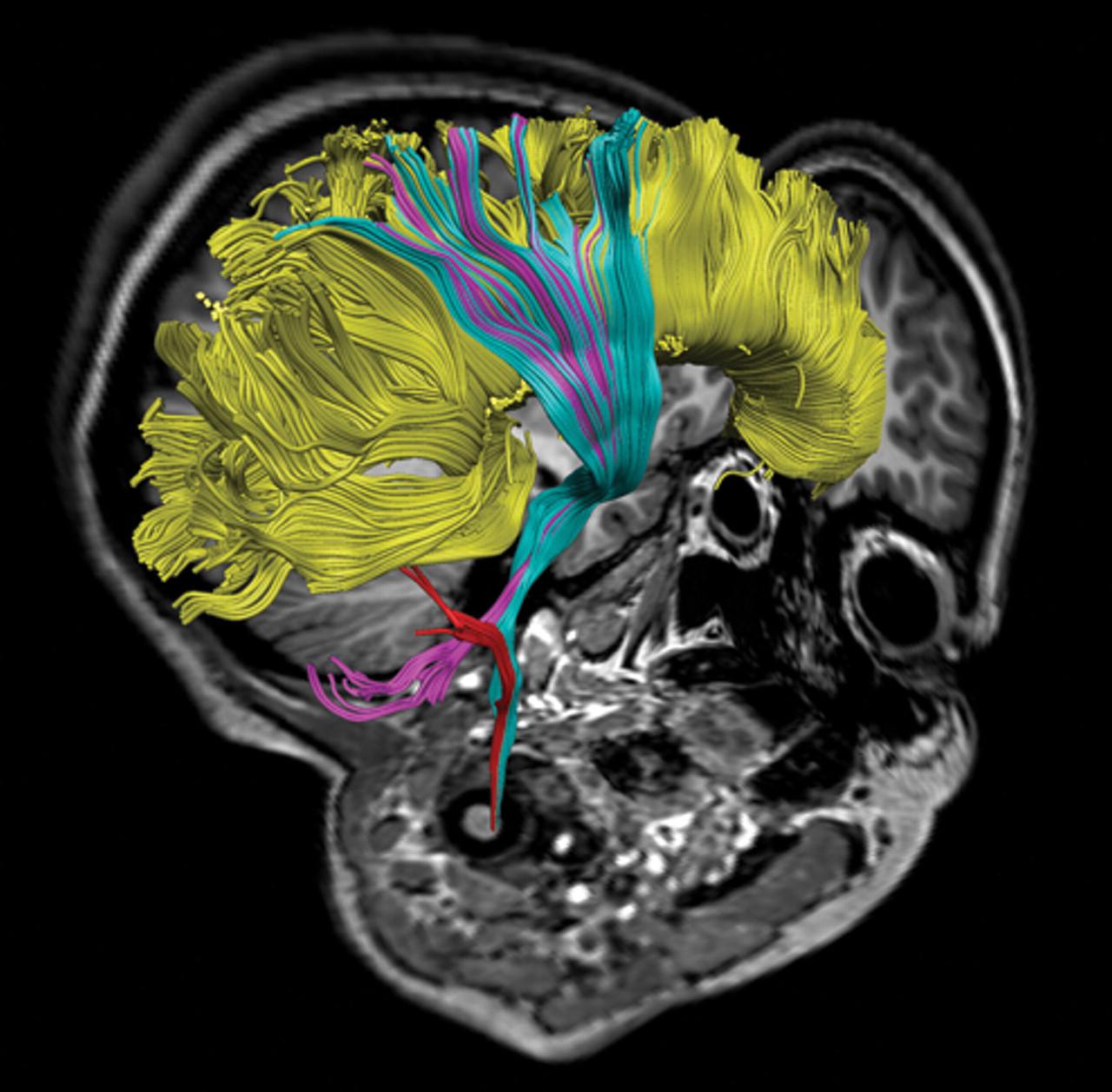
Motor tracts used in the study. Tracts were reconstructed and displayed on a 3D T1-image for a typical control subject: corticospinal tract (cyan), inferior cerebellar peduncle (red), superior cerebellar peduncle (pink), corpus callosum (yellow).
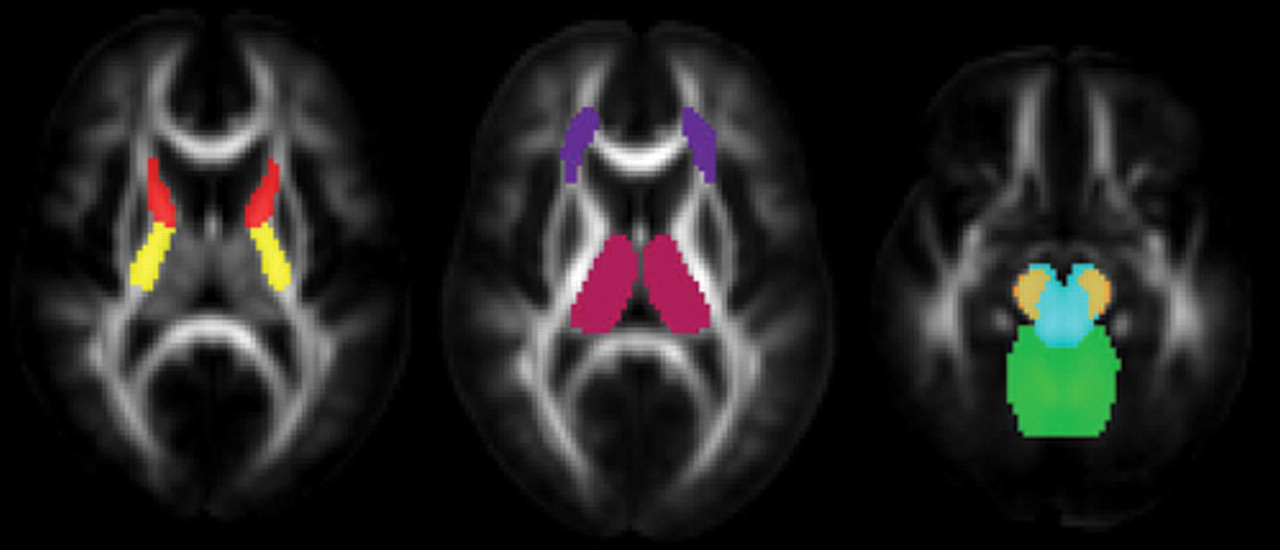
Example sensory and motor regions of interest masks depicted on fractional anisotropy maps of the white matter atlas of Mori et al 43 . Anterior limb of the internal capsule (red), posterior limb of the internal capsule (yellow), cerebellum (green), brainstem (blue), anterior corona radiata (violet), thalamus (pink), cerebral peduncle (orange). The ROIs are shown here on a slice at its middle location.
A close examination of the contributions of each hemisphere showed no significant main effect of cerebral hemisphere (right, left) on FA, and there were no differential symmetry effects across the 2 groups (both P > .05). Since diffuse injuries occur over a more widespread area, the bilateral average of these tracts and regions were used. As such, the remaining analyses were collapsed across hemispheres.
Statistical Analysis
Group comparisons
A 2-sample t test was used to test statistical significance when comparing FA and motor performance between the normal control group and TBI group. Data were confirmed to have a normal distribution using the Shapiro–Wilks normality test.
Relationship of WM integrity with motor functioning
The behavioral parameters of the clinical motor test battery (total and 3 subtest motor scores) were used to assess relationships between measures of WM integrity (12 WM structures) and motor functioning using partial Pearson correlations within the TBI group. We removed the effect of the random variable age, because FA of a few WM regions/tracts increased with age in our sample, for example, FA increased with age in the inferior cerebellar peduncle (r = .44; P < .05). Bonferroni corrections for multiple comparisons were made (hence P < .004 was considered significant following correction for the between-group comparisons regarding FA and P < .016 for the M-ABC variables and the correlation analyses).
Results
Group Differences in Motor Performance
The TBI group scored on average poorer than the control group on most M-ABC measures (as shown in Table 2): manual dexterity, t(39) = −3.48, P < .001; balance, t(39) = −1.81, P < .001; and total score, t(39) = −4.52, P < .001. Effect of group reached marginal significance for ball skills (P < .10).
Group Results (mean and standard error) on M-ABC Variables
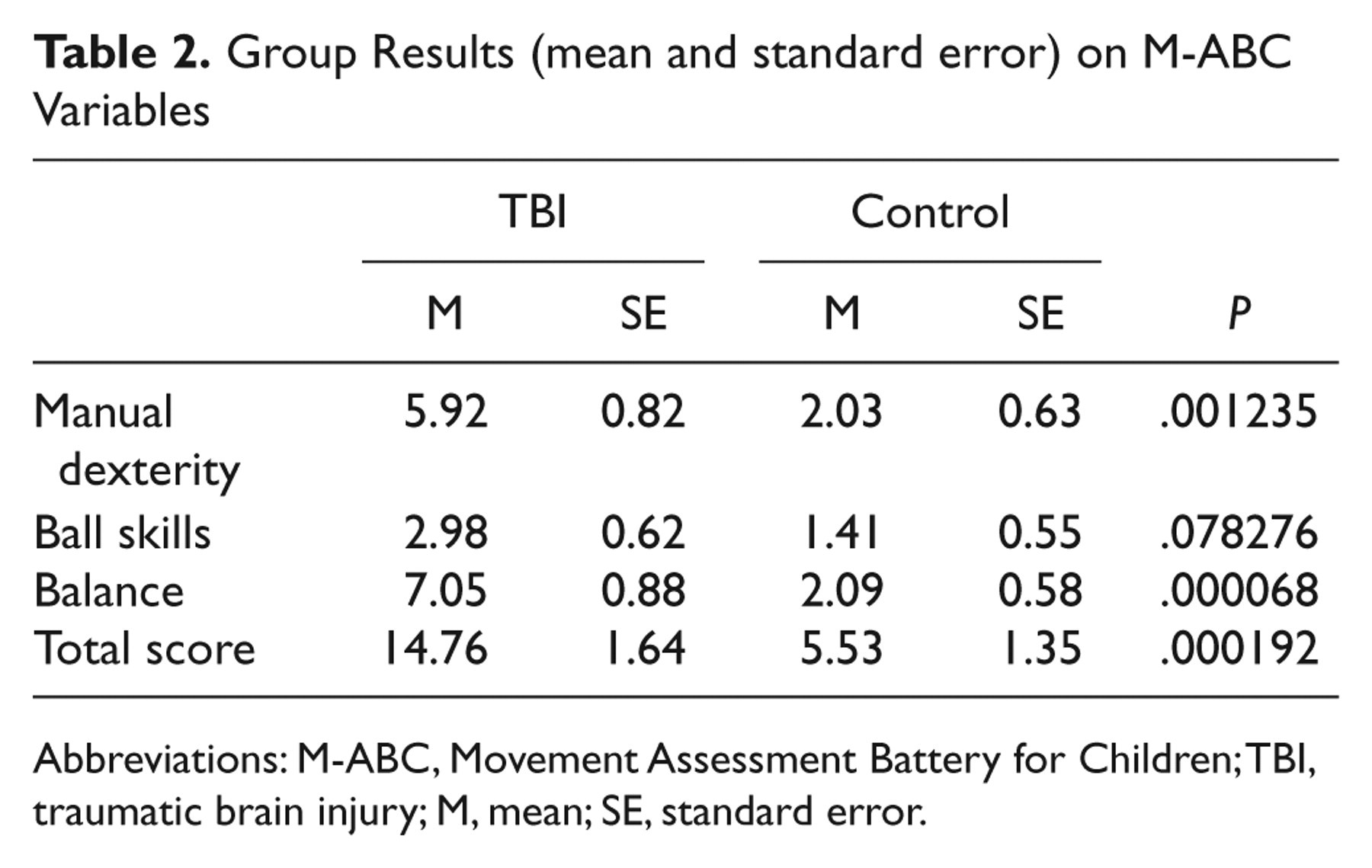
Abbreviations: M-ABC, Movement Assessment Battery for Children; TBI, traumatic brain injury; M, mean; SE, standard error.
Group Differences in FA
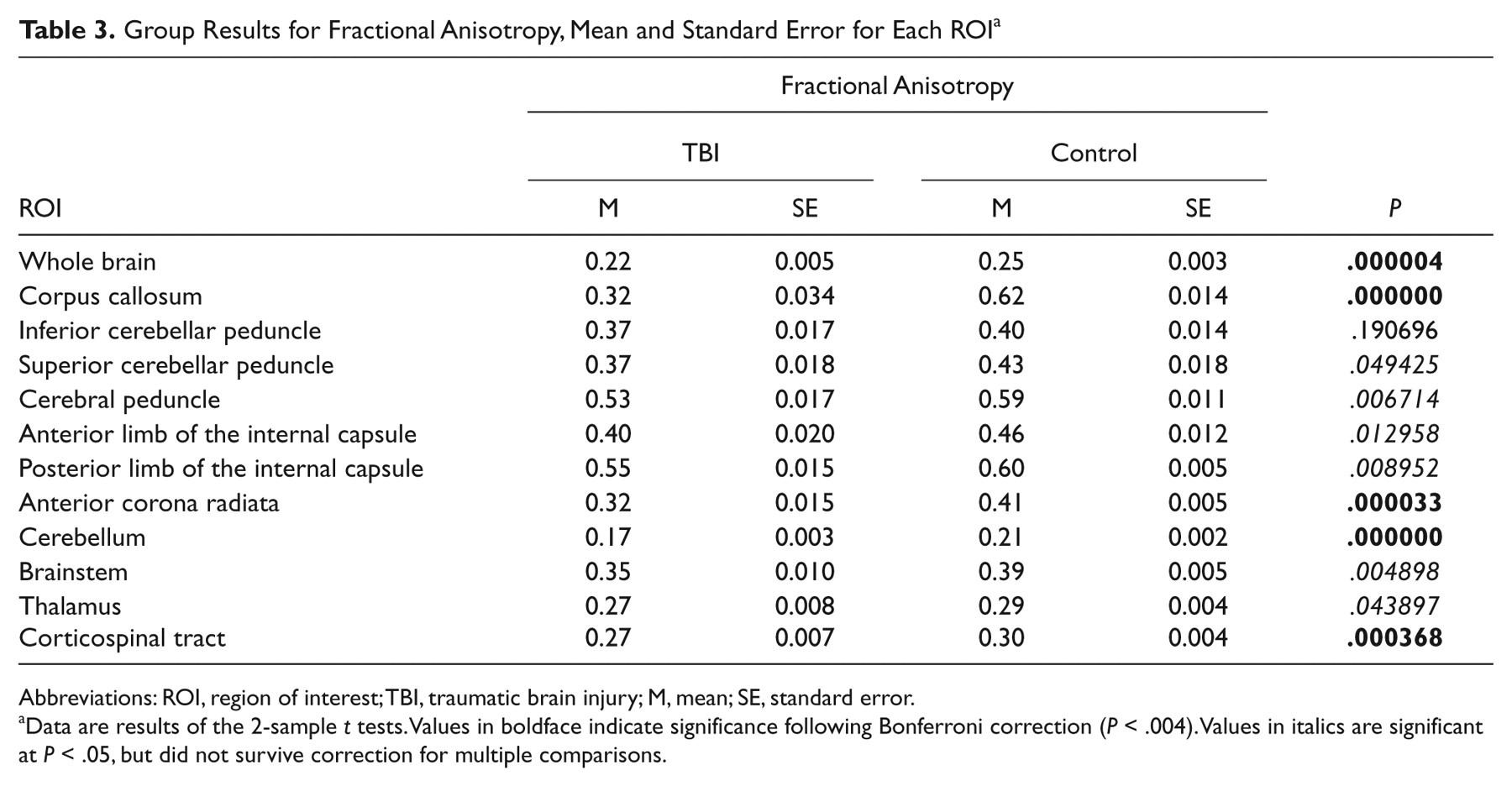
Overall, there was a significant main effect of group on whole brain FA, that is, WM FA was reduced in the TBI group relative to the controls, t(39) = 5.37, P < .001. As can be seen in Table 3, TBI patients showed significantly reduced FA along the corticospinal tract, t(39) = 3.90, P < .001, corpus callosum, t(39) = 7.08, P < .001, anterior corona radiata, t(39) = 4.69, P < .001, and cerebellum, t(39) = 7.04, P < .001.
Group Results for Fractional Anisotropy, Mean and Standard Error for Each ROI a
Abbreviations: ROI, region of interest; TBI, traumatic brain injury; M, mean; SE, standard error.
Data are results of the 2-sample t tests. Values in boldface indicate significance following Bonferroni correction (P < .004). Values in italics are significant at P < .05, but did not survive correction for multiple comparisons.
Relationship Between White Matter Integrity and Motor Functioning
To examine the relationship between WM integrity and motor function, we conducted a series of correlations between performance on the clinical motor test battery and FA within the entire TBI group. Significant negative correlations were found between the manual dexterity subscore and FA of the cerebellum (r = −.72; P < .001), indicating that poor scores on the fine motor M-ABC items coincided with lower FA. Also, the ball skills subscore correlated with mean FA in the fibers passing through the cerebellum (r = −.60; P < .01). Lower balance skill levels were associated with a lower FA in the corticospinal tract (r = −.68; P < .001). None of the M-ABC scores were correlated with FA within the control group.
Discussion
The present study demonstrated that DTI provides valuable quantitative information regarding WM microstructure in TBI patients. It was possible to clearly differentiate the patient and control group according to their FA values. Moreover, motor ability subscores (M-ABC) correlated with the DTI metrics.
Group Differences in Motor Functioning
Negative effects of brain injury on motor performance were clearly shown by the outcomes on the M-ABC. Fifteen TBI patients had a percentile score of 5 or less, indicating deviant motor performance, and 5 scored between the 5th and the 15th percentile, indicating that they were at risk for having motor problems. Specifically, the TBI group scored on average worse than the control group on the total score of the M-ABC, balance subscore, and manual dexterity subscore. There was also a trend toward lower ball skills in the TBI group. The motor deficits and behavioral changes seen following TBI are well described in the literature. Kuhtz-Bushbeck et al 4,5 showed deficits in fine motor skills, speed, and coordination, using hand function tests in children with moderate to severe TBI. Gagnon et al 44 reported that children with mild TBI showed balance deficits at 12 weeks postinjury on the balance subtest of the Bruininks-Oseretsky Test of Motor Proficiency, the Postural Stress Test, and on the eyes-closed conditions in the Pediatric Clinical Test of Sensory Interaction for Balance.
Group Differences in White Matter Integrity
DTI findings provide further evidence of abnormal motor processing in TBI. The pattern of abnormality found in this study is consistent with the preliminary case reports of diffusion imaging in children with TBI. 42 However, the current study reveals a considerably more extensive pattern of abnormality. Moreover, in contrast to previous DTI studies, which used ROI analyses, making them vulnerable to intrasubject and intersubject variability, we applied an automated observer-independent approach for assessing groupwise microstructural differences in several WM pathways/regions of the brain.
The significantly decreased FA in the corpus callosum in the TBI group can be explained by the shearing injuries to the deep parasagittal WM. 45 The corpus callosum is one of the structures to receive the highest strain concentration. Vulnerability of the corpus callosum to DAI has been shown in adults and children by neuropathologic and MRI studies. 46,47 The FA abnormalities are consistent with previous DTI studies that have shown decreased FA in the corpus callosum following acute TBI 3,48,49 and in chronic TBI patients. 10,50 Corpus callosum injury is of concern because of its central role in interhemispheric transfer of information and processing speed. 51,52
The pattern of observed impairment of WM in the cerebellum corresponds well with previous animal models of TBI. 53,54 Overall, these models revealed robust cerebellar damage following direct or indirect injury including regionally specific Purkinje cell injury or loss, activation of glia in a distinct spatial pattern, and traumatic axonal injury. There are also several clinical reports of cerebellar atrophy following TBI in children 55,56 and adults. 57 Together, these findings emphasize the vulnerability of the cerebellum to TBI and suggest the cerebellum as a target for therapeutic intervention.
In addition to the areas reported above, we found decreased FA along the corticospinal tract, including the anterior corona radiata. Significant FA differences in the corticospinal tract have been reported in patients with stroke, 58,59 congenital hemiplegia, 60,61 and mild TBI patients. 62,63 Moreover, recent studies in moderate-to-severe TBI adults also demonstrated an FA reduction in the corticospinal tract and anterior corona radiata. 62,64 The abnormalities found within the corticospinal tract in our TBI group appear critically associated with their observed motor deficits.
Detection of structural damage with DTI is a major advance in diagnostic imaging. However, linking structural damage to relevant functional consequences of TBI remains the essential link in determining the diagnostic utility of DTI and its relevance for patient monitoring during treatment. Our study contributed to bridging the gap between structure and function and is one of the few studies establishing relationships between DTI measures and motor function in TBI, as discussed next.
Structural Integrity of the Brain and Its Relationship to Motor Functioning
We tested whether damage in motor WM tracts/regions in the TBI group was associated with impairments in motor function, as assessed by the clinical motor test battery. In several brain structures, FA values were significantly correlated with the subscores of the M-ABC. Specifically, a significant correlation was obtained between manual dexterity and FA in the cerebellum. Also, the ball skills subscore was significantly correlated to mean FA in the cerebellum, and we found a significant correlation between the static and dynamic balance subscore and FA of the corticospinal tract.
The location of the significant correlations coincided with neural areas known to be important in specific motor functions. The cerebellum plays a distinct role in coordination and balance/postural control. The superior cerebellar peduncle represents the major output pathway of the cerebellum, including the dentatorubrothalamocortical and cerebellothalamocortical pathways, involved in sensorimotor integration. 65 FA of the corticospinal tract, which is associated with control of voluntary body posture adjustments, was significantly correlated with balance. Interestingly, in most of the regions where FA values in TBI patients were significantly lower than controls (ie, cerebellum and corticospinal tract), high correlations with the M-ABC scores were observed. Moreover, the regions with the highest correlations were not those with the greatest variability in values.
Important to note, only a marginally significant negative correlation was found between global WM neuropathology and manual dexterity whereas those between FA in individual ROIs and motor function did reach significance. This observation suggests that injury to specific WM tracts and regions is probably responsible for the motor deficits seen in patients with moderate-to-severe TBI. The absence of a relationship between whole brain anisotropy and behavioral measures is inconsistent with previous studies, 62,66 which have reported significant relationships between cognition and WM load. However, cognitive functions rely on more widespread cortical and subcortical networks than the motor system, which is likely the reason global WM load correlates with cognitive function but not with motor function.
Methodological Considerations and Conclusion
Limitations of the present study include the difference in mean age and male/female ratio between the TBI and control participants. Initial analyses indicated no difference between males and females in DTI metrics; therefore, the data were combined into a single group. Additional studies with larger sample sizes are needed to allow the modeling of relationships between demographics, FA, and motor performance scores reliably. Taking into account these limitations, the present study is the first report demonstrating that WM abnormalities detected by DTI are directly related to a decreased motor function in a young TBI group using a clinical motor test battery. This correlation between brain WM structure and behavior, and more specifically between FA and motor deficits, is of major interest for improving prediction of motor outcome in TBI patients. Such a prognostic tool can be used to design focused intervention protocols for TBI patients during the first months following injury. Moreover, our findings indicate microstructural alterations during the chronic stage of moderate-to-severe TBI, which may represent structural reorganization relevant to clinical recovery. DTI noninvasively provides quantitative pathophysiological information in vivo, and the prospect of tracking WM microstructural changes over time holds the promise of measuring neuroplasticity and repair following TBI, which eventually may offer a way to monitor therapeutic response. Future longitudinal studies are warranted that combine DTI with volumetric measurements, ideally with multiple data acquisitions at short time intervals. The potential of DTI as a prognostic marker requires further investigation in larger studies.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Support for this study was provided through a grant from the Research Programme of the Research Foundation—Flanders (FWO) (Levenslijn # 7.0004.05 and G.0482.010). Karen Caeyenberghs is funded by a postdoctoral fellowship of the Research Foundation—Flanders (FWO).