
Abstract
Background. Environmental enrichment (EE) is a complex living milieu that has been shown to enhance functional recovery versus standard (STD) housing after experimental traumatic brain injury (TBI) and therefore may be considered a rodent correlate of rehabilitation. However, the typical EE paradigm consists of continuous exposure to enrichment after TBI, which is inconsistent with the limited time frame in clinical rehabilitation. Objective. To determine whether abbreviated EE (ie, rehabilitation-relevant dose response) confers benefits similar to typical EE after TBI. Methods. Adult male rats received either a controlled cortical impact (2.8 mm depth at 4 m/s) or sham injury and were then randomly assigned to TBI + EE, TBI + EE (2 hours), TBI + EE (4 hours), TBI + EE (6 hours), TBI + STD, and respective sham controls. Motor (beam balance/beam walk) and cognitive (Morris water maze) performance was assessed on postoperative days 1 to 5 and 14 to 19, respectively. Results. The TBI + EE (2 hours) and TBI + EE (4 hours) groups were not statistically different from the TBI + STD group in any behavioral assessment. In contrast, the TBI + EE (6 hours) group exhibited significant enhancement of motor and cognitive performance when compared with the TBI + STD group, as well as the TBI + EE (2 hours) and TBI + EE (4 hours) groups (P < .003), and did not differ from the TBI + EE (typical) group. Conclusions. These data demonstrate that abbreviated EE (6 hours) produces motor and cognitive benefits similar to continuous EE after TBI and thus may be considered a dose-relevant rehabilitation paradigm.
Keywords
Introduction
Traumatic brain injury (TBI) affects an estimated 1.7 million Americans each year and results in 52 000 deaths and 120 000 cases of long-term neurological disabilities. 1-5 In addition to the morbidity and mortality caused by TBI, the acute and chronic medical and rehabilitative care along with the loss of productivity due to the inability to return to the workforce in a timely manner, or at all, imposes a significant monetary burden, which is estimated to be more than $50 billion per year. 6 Hence, TBI is a significant public health care concern. To combat this problem, a variety of relatively invasive therapeutic approaches, such as the administration of various pharmacologic strategies, 7-16 hypothermia, 17-20 and neurotrophins 21-24 have been evaluated. Additionally, noninvasive therapeutic approaches that potentially mimic clinical rehabilitation post-TBI, such as exercise 25,26 and environmental enrichment (EE), 27-32 have also been assessed.
EE consists of an enlarged living space, increased social interaction, and novel stimuli that together provide physical and cognitive stimulation 32 that results in a variety of neuroplastic changes after brain injury. 33-37 EE facilitates learning and memory after cortical impact 29,30,32 and fluid percussion brain injury 27,28,31 and also improves motor performance, 29,30,32 thus establishing it as a reasonable rodent correlate of human rehabilitation. The majority of research assessing the potential of EE to mimic clinical rehabilitation after TBI consists of continuous exposure to the complex living milieu. However, clinical rehabilitation after TBI consists of a limited amount of physical and occupational therapy. In many instances, patients must be able to tolerate at least 3 hours of therapy per day to qualify for inpatient rehabilitation, but in practice the length of time (ie, intensity) in therapy after TBI varies from a minimum of 1 hour up to a maximum of 8 hours per day depending on the rehabilitation setting. 38-41 Thus, while the extent of clinical rehabilitation may be longer than the 3-hour minimum, it is certainly shorter than the continuous nature of typically used EE paradigms. The difference between the relatively short duration of daily clinical rehabilitation after TBI and the continuous exposure of EE emphasizes a disparity between the experimental model and the clinical situation.
Thus, the goal of the current study was to evaluate the potential efficacy of an abbreviated enrichment (ie, dose-relevant) paradigm consisting of 2, 4, or 6 hours of EE per day, which may be viewed as more akin to clinical rehabilitation. The hypothesis is that the abbreviated EE groups will exhibit greater motor recovery and acquisition of spatial learning and memory retention when compared with the STD housed group and in a dose-dependent manner would also perform comparably to the continuous EE group.
Materials and Methods
Subjects
Eighty adult male Sprague–Dawley rats (Harlan, Indianapolis, Indiana) weighing 300 to 325 g on the day of surgery were housed in standard steel-wire mesh cages and maintained in a temperature- (21 ± 1°C) and light- (on 7:00
Surgery
A controlled cortical impact injury was produced as previously described. 7,8,43,44 Briefly, surgical anesthesia was induced and maintained with inspired concentrations of 4% and 2% isoflurane, respectively, in 2:1 N2O–O2. After endotracheal intubation, the rats were secured in a stereotaxic frame and ventilated mechanically, and temperature was maintained at 37 ± 0.5°C with a heating blanket. Using aseptic procedures a midline scalp incision was made, the skin and fascia were reflected to expose the skull, and a craniectomy (6 mm in diameter) was made in the right hemisphere (encompassing bregma and lambda and between the sagittal suture and the coronal ridge) with a handheld trephine. The bone flap was removed and the craniectomy was enlarged further with cranial rongeurs. Subsequently, the impacting rod was extended and the impact tip (6 mm, flat) was centered and lowered through the craniectomy until it touched the dura mater, and then the rod was retracted and the impact tip was advanced 2.8 mm farther to produce a brain injury of moderate severity (2.8 mm tissue deformation at 4 m/s). Immediately after the controlled cortical impact, anesthesia was discontinued and the incision was promptly sutured. The rats were subsequently extubated and assessed for acute neurological outcome. Sham rats underwent similar surgical procedures but were not subjected to the impact.
Acute Neurological Evaluation
Hind limb reflexive ability was assessed immediately following the cessation of anesthesia by gently squeezing the rats’ paw every 5 seconds and recording the time to elicit a withdrawal response. Return of the righting reflex was determined by the time required to turn from the supine to prone position.
Housing Conditions (Environmental Manipulation)
Following surgery, and after the effects of anesthesia abated (as evidenced by free movement in the holding cage), the rats were returned to the colony where the TBI and sham groups designated for continuous enrichment were immediately placed in specifically designed 36 × 30 × 20 in. steel-wire cages. The EE cages consisted of 3 levels with ladders to ambulate from one level to another and contained various toys (eg, balls, blocks, and tubes), nesting materials (eg, paper towels), and ad libitum food and water. 30,32 To maintain novelty, the objects were rearranged every day and changed each time the cage was cleaned, which was twice per week. Ten to 12 rats, which included both TBI and sham controls, were housed in the EE. Rats in the STD conditions and those randomly assigned to abbreviated EE were placed in standard steel-wire mesh cages (2 rats per cage) with only food and water. On the following day, and throughout the behavioral assessment period (19 days), the abbreviated EE groups were removed from the STD cages and placed in the EE for their prescribed times (eg, 2, 4, or 6 hours) and then returned to the STD conditions.
Motor Performance
Established beam-balance and beam-walk tasks were used to assess motor function. The beam-balance task consists of placing the rat on an elevated beam (1.5-cm wide) and recording the time it remains on it for a maximum of 60 seconds. The beam-walk task, modified from that originally devised by Feeney et al, 45 consists of training/assessing rats using a negative-reinforcement paradigm to escape ambient light and white noise by traversing an elevated narrow beam (2.5 × 100 cm) and entering a darkened goal box situated at the opposite end. When the rat enters the goal box the adverse stimuli (light and noise) are terminated, thus serving as reinforcement (reward) for completing the task. Performance was assessed by recording both the elapsed time to traverse the beam as well as the distance traveled. The scoring criteria for distance traveled is based on a rating scale from 0 to 5, where 0 indicates an inability to ambulate beyond the start location; 1 to 4 correspond to distal segments of 20, 40, 60, or 80 cm from the start point, respectively; and 5 corresponds with traversing the entire length of the beam (100 cm) and entering the goal box. 7 Rats were tested for beam-balance and beam-walk performance prior to surgery to establish a baseline measure and again on postoperative days 1 to 5. Testing consisted of 3 trials (60 seconds allotted time with an intertrial interval of 30 seconds) per day on each task. The average daily scores for each subject were used in the statistical analyses.
Cognitive Function: Acquisition of Spatial Learning
Spatial learning was assessed in a Morris water maze 46 task that has been shown to be sensitive to cognitive function after TBI. 7-10,47,48 Briefly, the maze consisted of a plastic pool (180 cm diameter, 60 cm high) filled with tap water (26 ± 1°C) to a depth of 28 cm and was situated in a room with salient visual cues that remained constant throughout the study. The platform was a clear Plexiglas stand (10 cm dia meter, 26 cm high) that was positioned 26 cm from the maze wall in the southwest quadrant and held constant for each rat. Spatial learning began on postoperative day 14 and consisted of providing a block of 4 daily trials (4-minute intertrial interval) for 5 consecutive days (14-18) to locate the platform when it was submerged 2 cm below the water surface (ie, invisible to the rat). On day 19 the platform was raised 2 cm above the water surface (ie, visible to the rat) as a control procedure to determine the contributions of nonspatial factors (eg, sensory-motor performance, motivation, and visual acuity) on cognitive performance. For each daily block of trials the rats were placed in the pool facing the wall at each of the 4 possible start locations (north, east, south, and west) in a randomized manner. Each trial lasted until the rat climbed onto the platform or until 120 seconds had elapsed, whichever occurred first. Rats that failed to locate the goal within the allotted time were manually guided to it. All rats remained on the platform for 30 seconds before being placed in a heated incubator between trials. The times of the 4 daily trials for each rat were averaged and used in the statistical analyses.
Cognitive Function: Probe Trial (Memory Retention)
One day after the final acquisition training session (ie, day 19), all rats were given a single probe trial to measure memory retention. Briefly, the platform was removed from the pool, and the rats were placed in the maze from the location point most distal to the quadrant where the platform was previously situated (ie, “target quadrant”) and allowed to freely explore the pool for 30 seconds. Typically, rats that have learned the specific location of the escape platform exhibit a spatial bias and spend significantly more time in the target quadrant. The percent time spent in the target quadrant was used in the statistical analysis.
A spontaneous motor activity recording and tracking (SMART) system (San Diego Instruments, San Diego, California) was used to record the data, which included time to locate the platform, time in the target quadrant, and swim speed.
Data Analyses
Statistical analyses were performed on data collected by observers blinded to treatment conditions using StatView 5.0.1 software (Abacus Concepts, Inc, Berkeley, California). The motor and cognitive data were analyzed by repeated-measures analysis of variance (ANOVA). The acute neurological, probe trial, and swim speed data were analyzed by 1-factor ANOVAs. When the ANOVA showed a significant effect, the Bonferroni/Dunn post hoc test was used to determine specific group differences. The results are expressed as the mean ± standard error of the mean (SEM) and were considered significant when P values were ≤.05 or as determined by the Bonferroni/Dunn statistic after correcting for multiple comparisons.
Results
Two rats were excluded from the analyses (one in the TBI + EE and another in the TBI + EE (2 hours) groups) as they were unable to locate the visible platform, which may be indicative of visual deficits that would preclude accurate assessment of spatial learning. Thus, the data analyses were conducted on 78 rats. Because there were no significant differences in any assessment among the sham control groups, regardless of housing, the data were pooled into one SHAM group.
Acute Neurological Function
No significant differences were observed among the TBI groups in time to recover the hind limb withdrawal reflex in response to a brief paw pinch (right range = 178.5 ± 4.6 to 195.6 ± 5.7 seconds, P > .05; left range = 183.6 ± 4.7 to 200.2 ± 5.8 seconds, P > .05) or for return of righting ability (range = 374.9 ± 14.2 to 412.7 ± 11.9 seconds, P > .05) following the cessation of anesthesia. The lack of significant differences with these acute neurological indices suggests that all groups experienced an equivalent level of injury and anesthesia. 7-12,29,30,32,44
Motor Function: Beam-Balance
No differences were observed among groups prior to surgery as all rats were capable of balancing on the beam for the allotted 60 seconds (Figure 1). Following TBI, all groups, except the TBI + EE, were significantly impaired relative to the SHAM group. The ANOVA revealed significant Group (F 5,72 = 10.647, P < .0001) and Day (F 5,360 = 58.378, P < .0001) differences, as well as a significant Group × Day interaction (F 25,360 = 6.485, P < .0001). The post hoc analysis revealed that the continuous EE group was able to maintain its balance significantly longer, and regain that ability sooner, than the TBI + STD and TBI + EE (4 hours) groups (P = .0005 and P = .0006, respectively). No other comparisons were statistically significant.
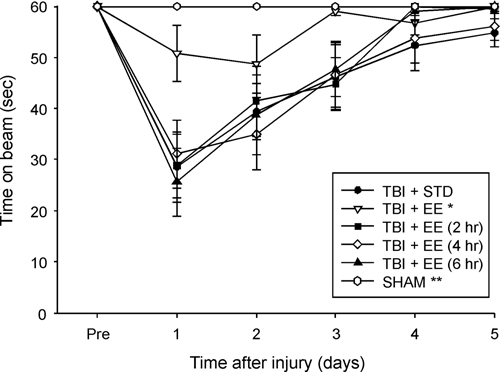
Mean (±SEM) time (seconds) balancing on an elevated narrow beam prior to, and after, TBI or sham injury. Abbreviations: TBI, traumatic brain injury; EE, environmental enrichment. *P < .0005 versus TBI + STD and P < .0006 versus TBI + EE (4 hours). **P < .0001 versus all TBI groups, except the TBI + EE. No other group differences were significant.
Motor Function: Beam-Walk (Traversal Time)
No presurgical differences in time to traverse the beam were revealed among groups as all rats were proficient and reached the goal box in approximately 5 seconds (Figure 2). After TBI, the ANOVA revealed significant Group (F 5,72 = 22.103, P < .0001) and Day (F 5,360 = 163.282, P < .0001) differences, as well as a significant Group × Day interaction (F 25,360 = 14.055, P < .0001). All TBI groups differed from the SHAM controls (P < .0001). Additionally, the TBI + EE and TBI + EE (6 hours) groups traversed the beam significantly quicker than the TBI + STD group (Ps < .0023) and did not differ from one another (P = .29). No other comparisons were significant.
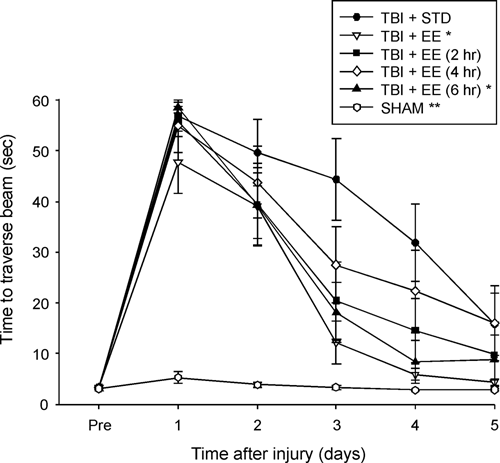
Mean (±SEM) time (seconds) to traverse an elevated narrow beam prior to, and after, TBI or sham injury. Abbreviations: TBI, traumatic brain injury; EE, environmental enrichment. *Ps < .0023 versus TBI + STD. **P < .0001 versus all TBI groups. No other group differences were significant.
Motor Function: Beam-Walk (Distance Traveled)
No presurgical differences were observed among groups as all rats were capable of traversing the entire length of the beam for a score of 5 (Figure 3). However, after TBI, the ANOVA revealed significant Group (F 5,72 = 15.204, P < .0001) and Day (F 5,360 = 113.732, P < .0001) differences, as well as a significant Group × Day interaction (F 25,360 = 11.194, P < .0001). All TBI groups differed from the SHAM controls (P < .0001). Additionally, the TBI + EE and TBI + EE (6 hours) groups returned to baseline performance significantly faster than the TBI + STD group (Ps < .0010) and did not differ from one another (P = .16). No other comparisons were significant.
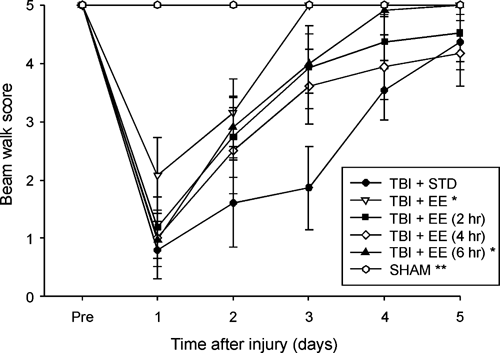
Mean (±SEM) distance traveled along an elevated narrow beam prior to, and after, TBI or sham injury. Abbreviations: TBI, traumatic brain injury; EE, environmental enrichment. *Ps < .0010 versus TBI + STD. **Ps < .0001 versus all TBI groups. No other group differences were significant.
Cognitive Function: Acquisition of Spatial Learning
Analysis of the spatial learning data revealed significant Group (F 5,72 = 26.938, P < .0001) and Day (F 4,288 = 44.118, P < .0001) differences. The post hoc analysis indicated that the TBI + EE and TBI + EE (6 hours) groups were able to locate the escape platform significantly quicker over time versus the TBI + STD, TBI + EE (2 hours), and TBI + EE (4 hours) groups (Ps < .0029) and did not differ from one another (P = .89; Figure 4). The SHAM group was significantly better than all TBI groups (P < .0001). No significant differences in swim speed (range = 31.3 ± 1.1 to 33.9 ± 0.9 cm/s) were observed among the groups. There was no significant difference among the TBI groups, regardless of housing condition, in the time to locate the visible platform, but the SHAM control group was able to reach it in significantly less time (Ps < .0002). The similarity in the TBI groups suggests that neither motor impairments nor visual disparities influenced the assessment of place learning.
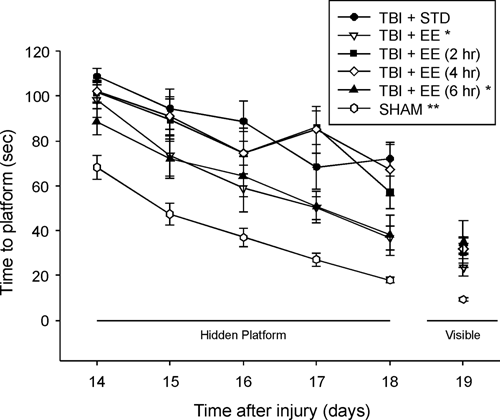
Mean (±SEM) time (seconds) to locate either a hidden (submerged) or visible (raised) platform in a water maze. Abbreviations: TBI, traumatic brain injury; EE, environmental enrichment. *Ps < .0029 versus TBI + STD, TBI + EE (2 hours), and TBI + EE (4 hours). **P < .0001 versus all TBI groups. No significant differences were revealed among the TBI groups for time to locate the visible platform, but the SHAM was able to reach it in significantly less time (Ps < .0002).
Cognitive Function: Probe Trial
Analysis of the probe data revealed significant memory retention in both the TBI + EE and SHAM groups as evidenced by a greater percentage of the 30-second allotted time spent in the target quadrant (40.2 ± 3.8% and 41.8 ± 1.6%, respectively) versus the TBI + STD group (25.6 ± 2.5%; (Ps < .0018). Additionally, the SHAM group was significantly better than the TBI + EE (2 hours) and TBI + EE (4 hours) groups (27.8 ± 3.2% and 29.7 ± 3.3%, respectively) but was not statistically different from the TBI + EE (6 hours) group that spent 34.3 ± 3.4% of its time in the target quadrant (Figure 5). The TBI + EE (6 hours) group was not statistically different from either the continuous EE group (P = .19) or the TBI + STD group (P = .053), although there was a strong trend for enhanced retention versus the latter.
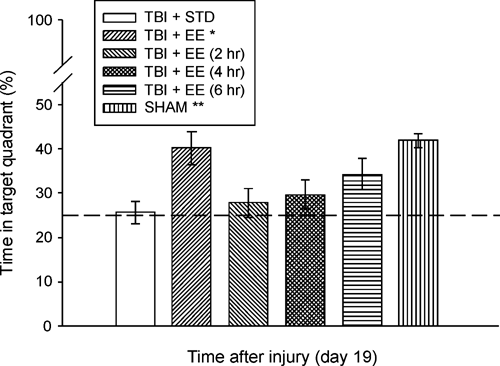
Mean (±SEM) percentage of time spent in the target quadrant (ie, where platform was previously located) following a single probe trial 19 days after cortical impact or sham injury. Abbreviations: TBI, traumatic brain injury; EE, environmental enrichment. *P = .0018 versus TBI + STD. **P < .0011 versus TBI + STD, TBI + EE (2 hours), and TBI + EE (4 hours). No other comparisons were significant. The dotted line represents performance at the chance level (25%).
Discussion
The majority of studies demonstrating the ability of EE to provide significant behavioral improvement after TBI have provided continuous enrichment, which is inconsistent with the limited number of hours per day of rehabilitation seen in the clinical setting. Therefore, if EE is to move forward as a reasonable rehabilitation paradigm it is essential that the dosing parameters be worked out. Hence, the aim of the current study was to determine if abbreviated EE would provide similar motor and/or cognitive benefits as those seen with continuous EE. The data revealed that motor performance and spatial learning was significantly improved in the continuous EE group versus STD housed controls, which replicates previous findings from our laboratory 29,30,32 and others. 27,28,31 Additionally, a novel finding in this study was that the TBI + EE (6 hours) group also conferred significant motor (beam-walk) and cognitive enhancement relative to the STD group. Moreover, in partial support of our hypothesis, the 6-hour EE group performed comparably to the continuous EE group. The 2-hour and 4-hour abbreviated EE groups did not differ from the STD controls in any behavioral measure, which did not support our hypothesis that any dose of EE would confer benefits.
These results indicate that continuous EE may not be necessary for optimal functional recovery after moderate TBI in rats. That the 6-hour EE and continuous EE groups performed similarly may suggest that there is a maximum time of enrichment in which the rats can benefit from the complex stimuli of the enriched setting. A plausible hypothesis is that the novelty, which is critical for optimal benefits, 32 attenuates as time passes. If this is the case, it may be advantageous to change the stimuli (ie, toys) twice per day instead of just once as is our current protocol. Perhaps “reintroducing” the novelty during the dark cycle when rats are more active may lead to greater benefits in the continuous EE groups. Furthermore, that the 2-hour and 4-hour EE groups did not show a benefit suggests that there is a certain threshold of enrichment that is necessary to elicit neurobehavioral recovery. However, a caveat to that statement is required as a study by Gaulke et al 49 reported that 1 hour of EE per day was sufficient to augment cognitive recovery after fluid percussion brain injury. Moreover, in a seminal study, Will et al 50 showed that 2 hours of EE after bilateral occipital cortex lesions was as effective as continuous EE in promoting cognitive benefits. However, the different models of injury along with diverse cognitive training protocols may explain the disparity in the amount of EE necessary to confer cognitive recovery.
The findings of this study may have clinical relevance as severe TBI patients may receive therapy in an acute inpatient setting or as convalescent care at home or in a skilled nursing facility, and the cognitive and physical stimulation provided by the multidisciplinary therapy could be viewed as an enriching environment to patients. It should be noted that the 6 hours of EE shown to benefit outcome in the current study is not inconsistent with clinical rehabilitation. Specifically, whereas the inpatient standard may be a minimum of 3 hours of therapy, this time can certainly be increased, especially in the inpatient setting. There are additional factors of inpatient rehabilitation such as the social interaction with other patients as well as with nurses and other staff that increase stimulation in that environment over what the patient may receive in therapy alone. A prospective study by Shiel et al 39 found that increasing the intensity of rehabilitation in TBI patients resulted in significantly shorter hospital admission and greater functional improvements. Zhu et al 41 showed that a 4-hour per day rehabilitation program resulted in a quicker return to independent functional status than 2 hours per day. Whereas there was no effect on the final level of recovery, the ability to integrate the patient into society faster is certainly beneficial. These clinical reports parallel the data in the current experimental study showing the finding that optimal amount of exposure to rehabilitation in the clinical setting or enrichment in the experimental setting results in improved outcomes.
In conclusion, the findings of this descriptive study show that abbreviated enrichment (6 hours) is capable of producing behavioral benefit comparably with that of continuous EE and may be a promising dose-relevant rehabilitation paradigm. The lack of significant benefits in the 2-hour and 4-hour abbreviated EE groups clearly indicate that there is opportunity for improvement. Given that pharmacotherapies are routinely provided in the clinical setting, it is quite possible to further characterize the EE paradigm such that a subtherapeutic level of EE (2 hours and 4 hours) is provided with subtherapeutic pharmacologic agents that in combination may provide a synergistic effect. This paradigm might be optimal in the clinic because some, if not many, of the deleterious side effects of the drug treatments may be attenuated or avoided all together while still seeing a beneficial effect on functional recovery. Such a study in our animal model is currently ongoing in our laboratory.
Footnotes
Kathryn M. Ehrenberg is currently at Duke University School of Nursing, Durham, North Carolina, USA. Amanda H. Panos is currently at the Department of Behavioral and Social Sciences, Lee University, Cleveland, Tennessee, USA.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported, in part, by National Institutes of Health grants HD046700 and NS060005 awarded to AEK and K12 HD055931 (ERS).