
Abstract
Background and Objective. This study compared the efficacy of distributed constraint-induced therapy (dCIT), bilateral arm training (BAT), and control treatment (CT) on motor control and functional performance of the upper limb in stroke patients. Methods. A total of 66 patients with mean stroke onset of 16.20 months and mild to moderate motor impairment were randomized to dCIT, BAT, or CT groups. Each group received treatment for 2 h/d and 5 d/wk for 3 weeks. Pretreatment and posttreatment measures included reaching kinematic variables in unilateral and bilateral tasks, the Wolf Motor Function Test (WMFT), and the Motor Activity Log (MAL). Results. The dCIT and BAT groups had smoother reaching trajectories in the unilateral and bilateral tasks than the CT group. The BAT group, but not the dCIT group, generated greater force at movement initiation than the CT group during the unilateral and bilateral tasks. The dCIT patients had decreased WMFT time and higher functional ability scores than the CT patients. MAL results pointed to better performance in the amount and quality of use of the affected arm than BAT and CT patients. Conclusions. BAT and dCIT exhibited similar beneficial effects on movement smoothness but differential effects on force at movement initiation and functional performance. Therefore, BAT is a better option if improvement of force generation is the treatment goal, and dCIT is more appropriate for improving functional ability and use of the affected arm in daily life. These findings may assist in the planning of individually tailored rehabilitation therapies.
Keywords
Introduction
Approximately 30% to 66% of stroke survivors report persistent movement impairment of their upper extremity (UE) and are unable to use their affected arm in daily activities. 1 Among a wide range of UE interventions, constraint-induced therapy (CIT) 2 and bilateral arm training (BAT) 3 are 2 evidence-based treatments. CIT refers to restraint of the unaffected UE and intense training of the affected UE. The signature form of CIT involves 6 hours of affected UE training daily for 2 weeks and restraint of the unaffected UE for 90% of waking hours. 4,5 Different distributed practice patterns have been developed that use less intensive training and shorter restraint time. 6,7-12 These forms decreased the training hours for each session (0.5 to 3 h/session) and daily restraint hours (5 to 9 h/d) and distributed these sessions to a longer duration (3 to 10 weeks). Studies in stroke patients have shown that standard CIT, distributed CIT (dCIT), and modified CIT are effective in improving movement strategies, including movement efficiency, speed, and smoothness 9,11-13 ; motor skills, such as wrist movements on the Fugl-Myer Assessment and turning cards and picking up a paperclip on the Wolf Motor Function Test (WMFT) 10 ; and the function and frequency of affected hand use. 5,7,8,11,14
Many natural daily activities, however, require bilateral movements. 15 It remains uncertain whether a patient should exclusively use the affected UE for practice, in accord with the concept of CIT, to optimize the treatment outcomes. Rigorous comparisons of CIT with alternative interventions, including BAT, have been proposed to address this concern. 16
BAT has been used as a potential UE rehabilitation intervention for individuals with stroke at all levels of severity. 17-19 BAT programs involve symmetrically bilateral movement with repetitive practice in different forms, 3 such as robot-assisted training, 20 bilateral motor priming (movement practice with rhythmic auditory cueing), 21,22 and repetitive practice of functional tasks (bilateral isokinematic training). 17-19,23-25 The training schedule of most studies was 15 minutes to 2.25 hours daily and 3 to 5 days weekly for 2 to 8 weeks. 3 Some studies demonstrated that BAT had beneficial effects on movement performance (eg, motor impairment, daily use of the affected UE, and muscle power) 20,22,24 and movement strategies (eg, directness/smoothness and speed). 21,26
CIT/dCIT and BAT, implemented in the form of functional task practice, share to a different degree various well-known principles of motor learning, including repetitive practice, task orientation, and goal directedness. 27,28 Conversely, both approaches involve different neural mechanisms:
CIT and dCIT that involve repetitive practice of unilateral functional activities may lead to use-dependent brain reorganization, especially in the damaged hemisphere, resulting in treatment-related motor gains. 29
BAT, in contrast, emphasizes bilateral movements, which may increase recruitment of the ipsilateral (ie, undamaged hemispheric) uncrossed corticospinal tract to facilitate cortical neural plasticity. 30 BAT also capitalizes on the template generated by the undamaged hemisphere to control both arm movements. 3,26
Different neural mechanisms may, arguably, cause different aspects of motor control recovery after the 2 different approaches, which have yet to be studied. Comparative efficacy research on motor control recovery may provide opportunities to address important gaps in knowledge. 31-33 Comparing these 2 approaches can further improve our understanding of the common and unique benefits of both approaches on motor control or daily function. Such a comparison also provides information on possible differential effects that each training approach yields on motor control or functional abilities. 34 Our present study was designed to compare the efficacy of the dCIT and BAT approaches at the motor control and functional levels.
Several studies have contrasted the effects of unilateral versus bilateral training on movement performance, but the results were controversial. 17,18,21,24,25 The bilateral training program in these studies involved asymmetrical bilateral practice, and unlike CID/dCIT, the unilateral training did not involve restraining the unaffected arm, a factor that might decrease the possible efficacy of the treatment program. To date, only 1 study has compared the relative efficacy of dCIT versus BAT on motor impairment, daily function, and quality of life. 14 The outcome measures used in that study relied on participant or therapist ratings of movement and functional performance. Those outcome measures validly demonstrated improvements in motor-related or function-related capacity but were limited in revealing specific changes in movement strategies. Study of movement strategies readily detected through kinematic analysis, 5 is necessary for understanding the mechanisms underlying therapeutic gains and assessing how each intervention approach influences motor control of the affected UE.
The specific purpose of this study was to compare the efficacy of dCIT, BAT, and control treatment (CT) on movement strategies of the affected UE and functional outcome in stroke patients. We hypothesized that dCIT and BAT, compared with CT, would render better performance on movement strategies in the affected UE during unilateral and bilateral testing tasks and also achieve greater motor and functional gains for stroke patients. In addition, dCIT and BAT may produce differential effects on movement strategies and functional outcome given the different treatment principles and neural mechanisms underlying the intervention approaches.
Methods
Participants
We recruited 66 stroke patients (mean age, 53.11 years; mean stroke onset, 16.20 months) from 4 stroke rehabilitation units. Participants had sustained a unilateral stroke, identified by brain imaging, and received independent examinations by a physiatrist and an occupational therapist to determine their eligibility for inclusion according to the following criteria: more than 6 months after onset of an ischemic or hemorrhagic stroke; Brunnstrom stage III or above for proximal and distal parts of the UE 35 ; considerable nonuse of the affected UE, that is, Motor Activity Log (MAL) amount of use (AOU) score < 2.5) 36 ; no serious cognitive deficits (Mini-Mental State Examination score ≥ 23) 37 ; no excessive spasticity of the affected UE (Modified Ashworth Scale score ≤ 2) 38 ; no participation in experimental rehabilitation or drug studies within the past 6 months; and no balance problems sufficient to compromise safety when wearing the constraint mitt. All participants signed informed consent forms approved by the local institutional review board and were blinded to the study hypotheses.
Design
This study used a randomized pretest and posttest control group design. Eligible participants were randomized to dCIT, BAT, or CT treatment groups (Figure 1) using the computerized (block) randomization scheme. A prestratification strategy was applied according to the 4 participating hospitals, so that the 3 therapies were administered at each site. The interventions were administered during regularly scheduled occupational therapy sessions. All other routine interdisciplinary stroke rehabilitation that did not involve UE training, including physical therapy or speech therapy, proceeded as usual.
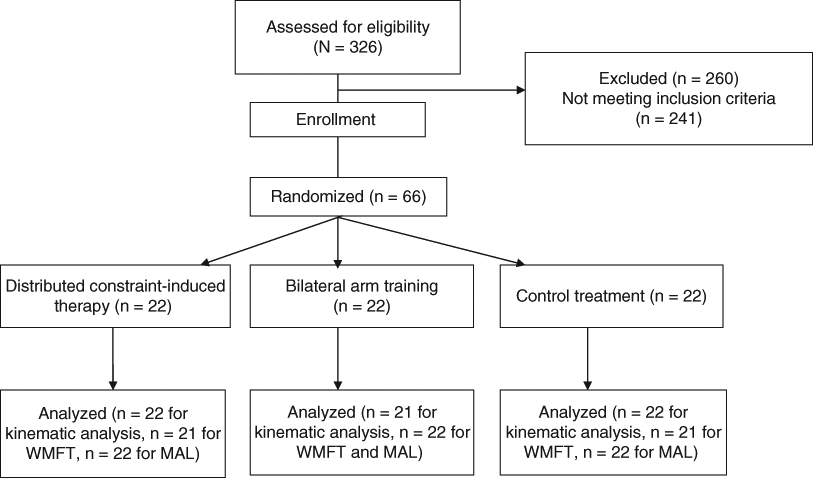
Flow diagram showing the randomization procedure
Five certified occupational therapists were trained in the administration of dCIT, BAT, and CT protocols by the primary investigators to provide consistent intervention protocols. Before and after the 3-week intervention period, kinematic analysis and clinical outcome measures were administered by 2 certified, trained occupational therapists blinded to the participant group.
Interventions
Treatment regimens were designed to ensure that all groups received an equal amount of therapy (ie, 2 hours daily for 5 d/wk for 3 consecutive weeks). This treatment frequency and duration were determined from previous studies of dCIT 8,9,11,14 and BAT 14 that showed beneficial effects on movement strategies and functional outcomes.
The dCIT group focused on using a mitt to restrict the unaffected hand for 6 hours daily and intensively train the affected UE in functional tasks, including reaching to move a cup, picking up coins, picking up a utensil to take food, grasping and releasing various blocks, and other functional movements involved in daily activities. The level of challenge was adapted according to patient ability and improvement during training. Hours of mitten wear each day were recorded by the patients and confirmed by the caregivers.
The BAT group concentrated on the simultaneous movements in symmetric or alternating patterns of both UEs in functional tasks, which involved lifting 2 cups, picking up 2 pegs, grasping and releasing 2 towels, wiping the table with 2 hands, and so on.
Approximately 75% of the therapy in the CT group was based on the principles of neurodevelopmental treatment. This training component included functional task practice for hand function, UE coordination, balance, stretching, and weight bearing of the affected UE. Approximately 25% of the control intervention addressed compensatory practice on functional tasks with the unaffected UE or both UEs.
Outcome Measures
Kinematic analysis acquisition
Experimental tasks used in the kinematic analysis included a unilateral task that involved pressing a desk bell as fast as possible with the index finger of the affected hand and a bilateral task that involved pulling a drawer with the affected hand and retrieving an eyeglass case inside the drawer with the unaffected hand at a comfortable speed. Only reaching movements of the affected hand were recorded. After a practice trial, 3 trials were performed. Both tasks were administered before and after a 3-week intervention.
During the tasks, participants sat on a height-adjustable chair with the seat height set to 100% of the lower leg length, measured from the lateral knee joint to the floor with the participant standing. The table height was adjusted to 2 inches below the elbow. The participant’s hands were rested on the edge of the table. The trunk was harnessed to the chair back to minimize trunk flexion and rotation. 13 The target object (desk bell or drawer) was located along the participant’s midsagittal plane. The reaching distance to the bell and drawer was standardized to the participant’s functional arm length, which was defined as the distance from the medial border of the axilla to the distal wrist crease. 12 If the maximum distance the participant could reach was less than the functional arm length, the distance to the target (the task distance) was adjusted to the maximum reachable distance.
During the 2 tasks, a 7-camera motion analysis system (VICON MX; Oxford Metrics Inc, Oxford, UK), recorded at 120 Hz, was used with a personal computer to capture the movement of a marker attached on the ulnar styloid and in connection with analog signals linked to a bell. Movement onset for both testing tasks was defined as a rise of tangential wrist velocity above 5% of its peak value. Movement offset for the unilateral task was the time when the participant pressed the bell. During the bilateral task, movement offset was defined as a fall of tangential wrist velocity below 5% of its peak value.
Data reduction for kinematic variables
An analysis program coded by LabVIEW language (National Instruments, Inc, Austin, TX) was used to process the kinematic data. Kinematic variables for reaching included normalized movement time (NMT), normalized movement unit (NMU), peak velocity (PV), and the percentage of movement time where peak velocity (PPV) occurred. MT, which refers to the time for execution of the reaching movement and represents temporal efficiency, is the interval between movement onset and offset. 9,11,12 Because the task distance varied across participants, MT and MU were normalized to correct for variations in reaching distance; that is, MT and MU were divided by the distance of reaching. One MU, consisting of 1 acceleration and 1 deceleration phase, can be used to characterize movement smoothness. Fewer MUs indicated smoother movement. 12
PV is the highest instantaneous velocity during the movement and indicates force or impulse at movement initiation. 11,39,40 The time required to reach PV reflects the duration of the initial impulse, and the amplitude of PV reflects the magnitude of the resultant impulse. 41 The greater force of impulse at movement initiation can be reflected by a higher amplitude of PV. 42 PPV was used to characterize the control strategy of reaching and reflects the percentage of movement time used for the acceleration phase. A higher PPV value indicates a longer acceleration phase, suggesting less online error correction and more preplanned control of the reaching movement. 43
Functional assessments
The WMFT is a function-based motor assessment of 17 tasks, including 15 timed and functional ability tasks and 2 strength tasks. 44 Performance time (WMFT-Time), functional ability scores (WMFT-FAS), and strength (WMFT-Strength) were reported. The WMFT has established high reliability and validity in stroke patients. 44-46
The MAL is a functional measure of a participant’s perception of real-world use of the affected UE for 30 daily activities. 47 The AOU and the quality of movement (QOM) of the affected arm were assessed. 47 This scale has good consistency, reliability, and validity in stroke patients. 47,48
Statistical Analysis
Multivariate analyses of covariance (MANCOVAs), which control for the probability of type I errors produced by repeated comparisons, 49 were used to examine change in outcome measures as a function of treatment while controlling for pretreatment performance. We performed 4 separate MANCOVAs for the variables of unilateral reaching, bilateral reaching, WMFT, and MAL, adjusting for pretreatment performance. Follow-up univariate analysis of covariance (ANCOVA) for each dependent variable was used for relative means when the MANCOVA demonstrated a significant effect. 49 To index the magnitude of group differences in performance, η2 = SSb/SStotal was calculated for each outcome variable. The value of η2 is independent of sample size and represents the variability in the dependent variable (posttest performance) that can be explained by group. 50 A large effect is represented by a η2 of at least 0.138, a moderate effect by a η2 of 0.059, and a small effect by a η2 of 0.01. 51
Results
Table 1 summarizes the characteristics of the participants in the 3 groups. Baseline characteristics were comparable across groups. Kinematic data were missing in the BAT group from 1 participant for the unilateral task and from another participant for the bilateral task. Clinical data for the WMFT were missing from 1 participant in the dCIT group and 1 participant in the CT group (Table 2).
Characteristics of Study Participants
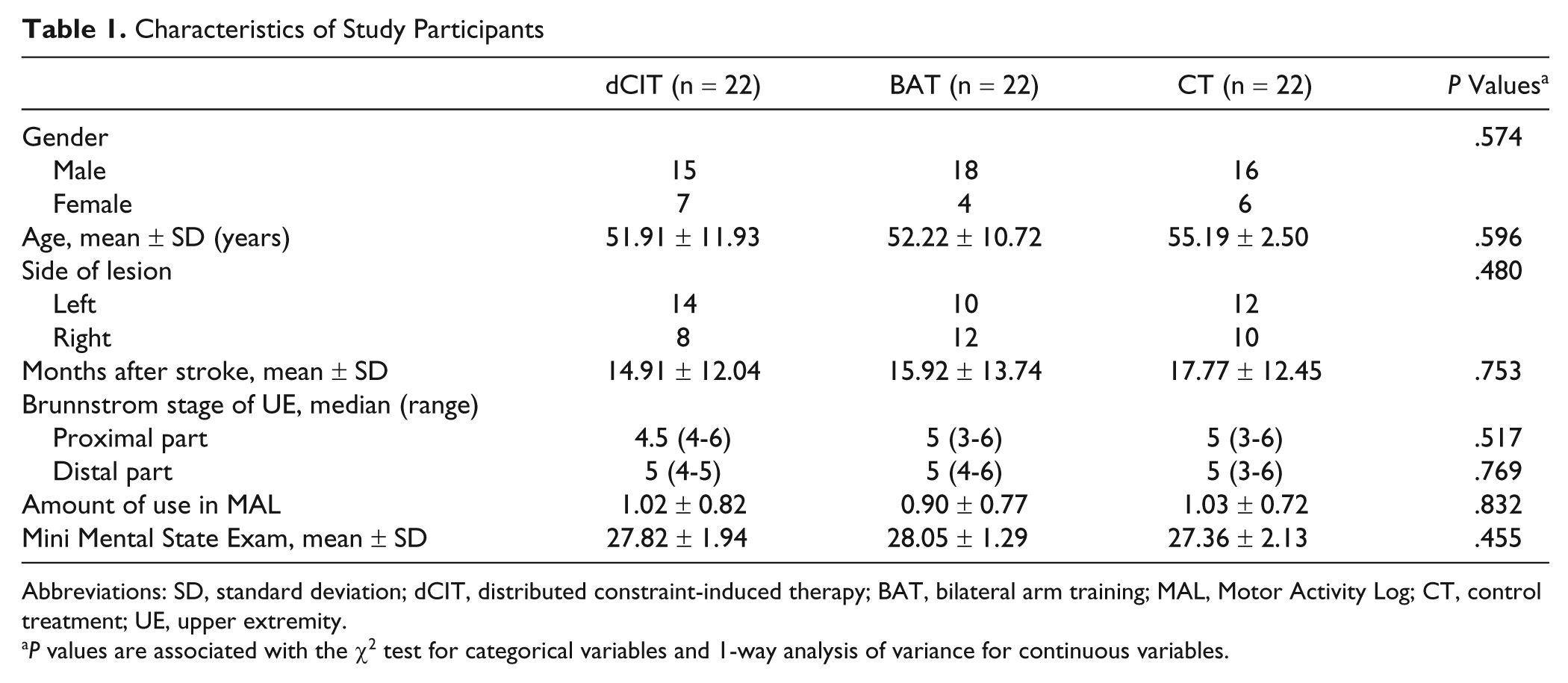
Abbreviations: SD, standard deviation; dCIT, distributed constraint-induced therapy; BAT, bilateral arm training; MAL, Motor Activity Log; CT, control treatment; UE, upper extremity.
P values are associated with the χ2 test for categorical variables and 1-way analysis of variance for continuous variables.
Descriptive and Inferential Statistics for the Kinematic Variables and Clinical Measures
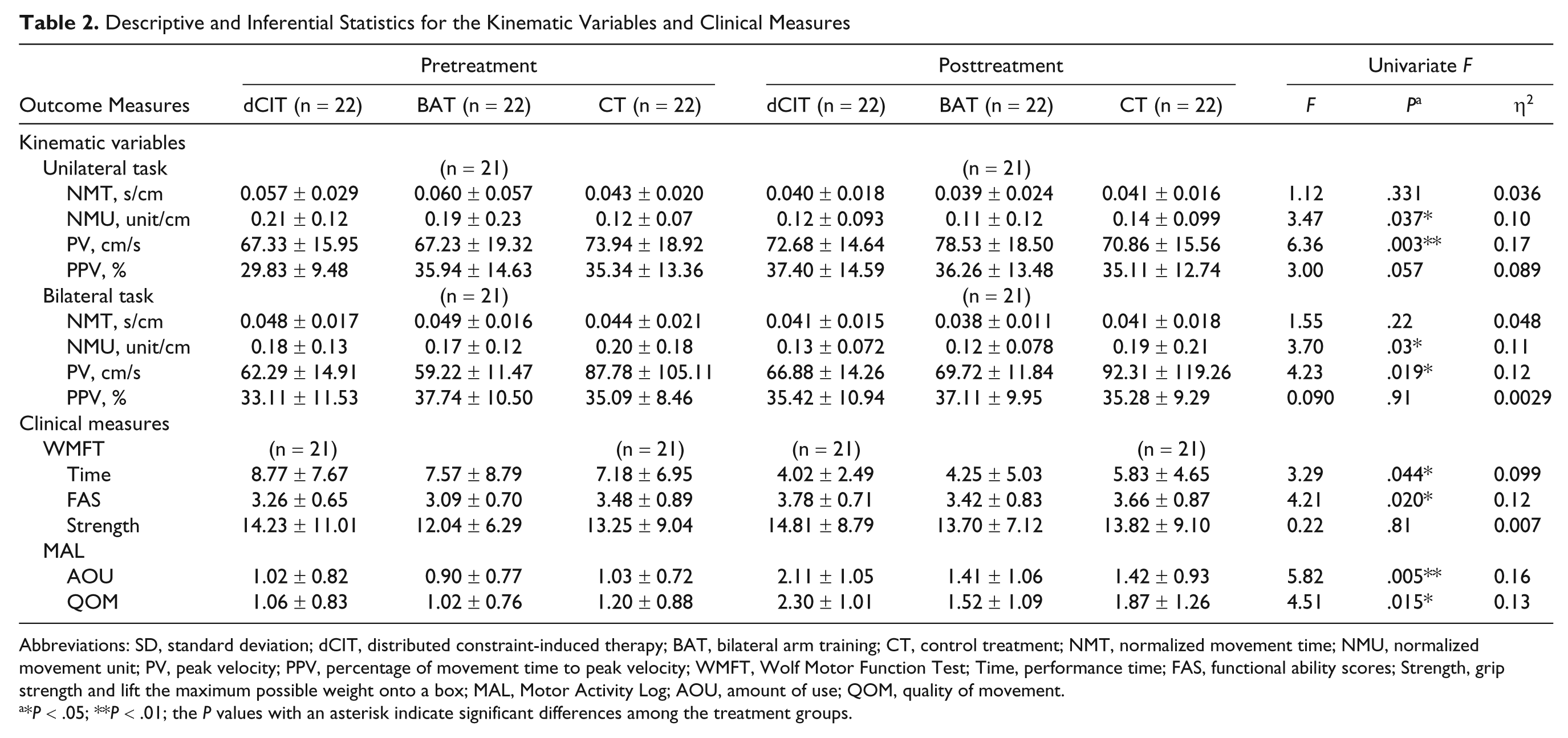
Abbreviations: SD, standard deviation; dCIT, distributed constraint-induced therapy; BAT, bilateral arm training; CT, control treatment; NMT, normalized movement time; NMU, normalized movement unit; PV, peak velocity; PPV, percentage of movement time to peak velocity; WMFT, Wolf Motor Function Test; Time, performance time; FAS, functional ability scores; Strength, grip strength and lift the maximum possible weight onto a box; MAL, Motor Activity Log; AOU, amount of use; QOM, quality of movement.
*P < .05; **P < .01; the P values with an asterisk indicate significant differences among the treatment groups.
Kinematic Measures
MANCOVAs revealed a significant main effect for the group for unilateral and bilateral reaching kinematics (unilateral task: F 8,110 = 3.61, P = .001, power = 0.97; bilateral task: F 6,112 = 5.74, P = .043, power = 0.80). Table 2 reports the results of post hoc ANCOVAs for the kinematic variables. For the unilateral reaching task, a significant and moderate to large effect on NMU and a large effect on PV, but not on NMT and PPV, were found. For the bilateral reaching task, significant and moderate to large effects on NMU and PV, but not on NMT and PPV, were obtained. Participants in the dCIT and BAT groups significantly improved in movement smoothness, whereas the CT group did not (unilateral: P = .021 for dCIT vs CT, P = .032 for BAT vs CT; bilateral: P = .025 for dCIT vs CT, P = .019 for BAT vs CT). No significant difference in NMU was found between the dCIT and BAT groups. Compared with the CT group, the BAT group showed significantly higher PV (unilateral, P < .001; bilateral, P = .006). No significant differences in PV were found between the dCIT and CT groups and between the dCIT and BAT groups.
Clinical Measures
MANCOVAs revealed a significant main effect for group for the WMFT (F 6,112 = 5.74, P = .043, power = 0.77) and the MAL (F 4,120 = 5.74, P ≤ .0001, power = 0.97). Post hoc ANCOVAs showed significant and moderate to large effects on WMFT-Time, WMFT-FAS, and MAL-QOM and a significant and large effect on MAL-AOU but not on WMFT-Strength. The dCIT group demonstrated significantly greater improvements in the WMFT-Time (P = .044) and WMFT-FAS (P = .020) than the CT group. The dCIT group produced higher gains in the MAL-AOU (P = .002 for dCIT vs CT; P = .010 for dCIT vs BAT) and MAL-QOM (P = .036 for dCIT vs CT; P = .005 for dCIT vs BAT) than the CT and BAT groups. No significant difference between the CT and BAT groups was documented in any of the clinical measures.
Discussion
This comparative efficacy study is the first one, to our knowledge, to compare movement strategies and functional abilities of dCIT and BAT. After intervention, the dCIT and BAT groups had smoother reaching trajectories in the unilateral and bilateral tasks than the CT group. The BAT group, but not the dCIT group, also generated greater force at movement initiation during the unilateral and bilateral tasks after the intervention than the CT group. Only the dCIT group showed greater ability to perform functional UE tasks measured by the WMFT than the CT group. The dCIT group also achieved better performance in the amount and quality of use of the affected limb, as measured by the MAL scale, than the BAT and CT groups.
Benefits of dCIT and BAT Relative to CT
As found in previous studies, the dCIT 11 and BAT 21 patients had smoother movement trajectories, reflected by fewer NMUs for performing unilateral and bilateral tasks, than the CT patients. This finding suggests that patients receiving the dCIT or BAT therapy were able to generalize the trained skills of the affected limb to unilateral and bilateral tasks. Compared with the pretreatment NMU, the posttreatment NMU values of the unilateral task were decreased for the dCIT and BAT groups but increased for the CT group, as noted in Table 2. In addition, a normal reaching movement would typically include only 1 MU. 9,42 The reaching distance obtained in this study sample ranged from 14 to 40 cm. The value of NMU for normal reaching might range from 0.025 to 0.07. The pretreatment NMU of the control group is 0.12 and, thus, leaves room for reduction of the NMU. Therefore, the floor effect might not be a plausible explanation for the study result. Studies of motor recovery suggest changes in movement smoothness occur during the process of motor learning. Increased smoothness is a result of a learned coordinative process. 52,53 Both interventions used the learning principles of repetitive and task-oriented practice, which might facilitate the learning course and lead to increases in movement smoothness.
Superior Benefits of BAT or dCIT Over Other Treatments
Participants who received BAT, but not dCIT, significantly improved force generation at movement initiation, as reflected by the variable PV during the unilateral and bilateral tasks, compared with those who received CT, partially consistent with prior research. 11 BAT may facilitate more recruitment of uncrossed corticospinal pathways than dCIT for motor control of the affected limb because BAT involves unaffected limb movement during training periods. 54 This advantage might increase the magnitude of the neural activation signals, thus, recruiting a larger number of motor units for generating high force at the initial stage of the movements 53 and resulting in higher PV. Our findings, however, did not lend direct support to this hypothesis. To validate the hypothesis, future research may integrate surface electromyogram results into kinematic analysis to detect the changes in the recruitment of motor units during the time to reach PV. BAT might also take advantage of interlimb coupling characteristics of the motor control system, so that muscle activity for force generation in the affected arm during BAT could be facilitated by the unaffected side and would tend to be similar to that in the unaffected arm. 55
As found in previous research, improvements in motor functions of the affected UE were greater in the dCIT patients than in the CT group, as reflected by the time and the functional ability aspects of the WMFT. 5,10,13 Similar to previous study findings, the dCIT patients achieved better performance in the amount and quality of use of the affected UE, as measured by the MAL, than the CT 5,12,14 and BAT patients. 14 The dCIT program involved repetitive practice of a variety of unilateral functional tasks and often required dexterity training. Functional motor tasks often may also be performed bilaterally but with different purposes for each hand, such as grasping an apple with one hand and peeling it with the other hand. Therefore, the BAT program might not directly capitalize on the benefits of functional training.
Although all participants received the same frequency and duration of treatment intervention, dCIT is arguably more intensive than BAT and CT because of more “treatment” during restraint wear out of the clinic, which might contribute to the superior performance of dCIT on functional performance. However, the restraint wear out of the clinic in the dCIT group may not necessarily have confounded the study findings. One previous study 8 compared dCIT with a dose-matched control intervention that included restraint of the less affected hand. The dCIT group exhibited significantly better performance in motor function and daily function than the dose-matched CT group. This study 8 lent support for the robust effects on functional improvement of training the affected arm during the dCIT program.
Comparable Benefits of dCIT and BAT Relative to CT
Although the descriptive data showed that NMT decreased from pretest to posttest for the 3 groups, dCIT and BAT did not significantly improve movement efficiency (NMT) more than CT, and the effects of dCIT and BAT on improvement were similar. Although execution time to perform the kinematic tasks (represented by NMT) did not significantly decrease in the dCIT group compared with the CT group, the dCIT group had significantly decreased performance time on the WMFT relative to the CT group. The testing tasks might account for this difference. Tasks for kinematic analysis only involved 2 gross motor tasks, whereas the WMFT involved several gross and fine motor tasks, such as grasp and pinch, and might be sensitive to detect fine motor efficiency in a time domain. Consistent with previous studies, 5,22 this study did not show significant differences in the strength aspects of WMFT among the 3 intervention approaches. This is probably because dCIT and BAT do not emphasize muscle strengthening during training.
The present study did not show significant differences in movement strategies (ie, PPV) among the 3 intervention approaches, although the differences in results in the unilateral task approached significance (P = .057). Higher PPV is thought to have a high proportion of reaching spent in the acceleration phase, indicating favorable use of preplanned strategies in which error corrections do not usually occur. Some motor control and cognitive scientists argue that the initial motor plan is only crudely defined before the onset of movement and is subsequently corrected through internal feedback loops that occur early in the course of the movement during the acceleration phase. The low amplitude of PPV (ie, the short acceleration phase relative to the deceleration phase) might indicate poor preplanning strategy or high efficiency of using internal feedback processes. Accordingly, the combined use of preplanned strategies and internal feedback loops during the acceleration phase may lead to a PPV that is not sensitive enough to detect the differences in the extent to which the preplanning strategy was used and improved among the 3 groups.
Study Limitations
Caution should be exercised about generalizing these results beyond this study. First, this study only used 2 tasks to evaluate the changes in movement strategies after interventions. Future research will need to scrutinize whether the effects after dCIT or BAT can be generalized to daily functional tasks. Second, the study patients had retained some motor function abilities when they entered the study and do not represent patients with minimal movement abilities (eg, Brunnstrom stage 1 or 2). Also, the dCIT group, arguably, received more “treatment” during restraint wear out of the clinic. Future research might use a dose-matched group that receives BAT together with practice on bilateral daily tasks out of the clinic to address the issue of dose equivalence.
Conclusion
This comparative study shed some light on the relative effects of dCIT and BAT on upper-limb movement performance after stroke. BAT and dCIT exhibited similar beneficial effects on movement smoothness but differential effects on force at movement initiation and functional performance. Furthermore, these findings suggest that BAT is a better option if improvement of force generation is the treatment goal. In contrast, dCIT is more appropriate for improving functional ability and use of the affected arm in daily life in patients like those in this trial.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This project was supported in part by the National Science Council (NSC-97-2314-B-002-008-MY3, NSC-97-2314-B-182-004-MY3, and NSC-98-2811-B-002-015) and the National Health Research Institutes (NHRI-EX99-9742PI and NHRI-EX99-9920PI) in Taiwan.