
Abstract
Background:
Despite the association between HIV and coronary artery disease (CAD), there are no specific recommendations for the cardiovascular evaluation of the HIV-infected population. Besides being a tool for the evaluation of CAD, the exercise treadmill test (ETT) provides insights into functional capacity and autonomic function, which have been frequently affected in HIV infection, and thus may be useful in this setting.
Methods:
Forty-nine HIV-infected individuals without known CAD underwent ETT. Peak oxygen consumption during exercise (VO2 peak), functional capacity (in metabolic equivalents [METs]), exercise-induced ischemia, chronotropic incompetence (CI) and abnormal heart rate recovery (HRR) after exercise were studied.
Results:
VO2 peak was 31.4±4.8 mL/kg/min and functional capacity was 9.2±1.6 MET. CI was observed in 30.6%, and 10.2% had abnormal HRR. VO2 peak was lower in women and inversely correlated with age and body mass index. None of the patients displayed ischemic changes.
Conclusion:
Although functional capacity was good, risk markers such as CI and abnormal HRR were not infrequent. This study identifies a subgroup of HIV-infected patients–the older, overweight, or obese–who may have higher risk and deserve cardiovascular screening with the ETT.
Introduction
HIV infection is a worldwide epidemic with huge economic and social implications. 1 Since the advent of antiretroviral therapy (ART), survival has increased considerably. Also, muscle wasting and severe loss of functional capacity were very frequent before ART was available but are presently less common. 2 –8 Nonetheless, while improving AIDS-related prognosis, current ART results frequently in metabolic abnormalities, such as dyslipidemia and glucose intolerance, which increase the risk of coronary artery disease (CAD). Nowadays, HIV-infected patients most likely die from common chronic conditions, such as cardiovascular disease, than from opportunistic infections. 9–13
In general populations, the exercise treadmill test (ETT) has been extensively employed for the stratification of cardiovascular risk and as a guide for the institution of therapies and exercise programs. The ETT provides plenty of data that are consistent predictors of outcome; one of them, exercise capacity, is strongly related to cardiovascular prognosis, in individuals infected with HIV or not. 14 –16 Chronotropic incompetence (CI) and abnormal postexercise heart rate recovery (HRR) have also been defined as the markers of cardiovascular risk, either for CAD or all-cause death. 17–20 In a group of HIV-infected patients on ART, Cade et al have also observed impaired postexercise HRR and have suggested a link with autonomic neuropathy, 21 which has been frequently found in this population, especially in the more advanced cases. 22 Nonetheless, currently there are still no specific recommendations for physical evaluation of the HIV-infected patients. Therefore, we aimed to study the ETT as a tool to assess the cardiovascular responses to exercise (exercise capacity, development of CI, or abnormal HRR) and, accordingly, evaluate cardiovascular risk of HIV-infected individuals on ART.
Materials and Methods
HIV-infected individuals aged ≥18 years, attending public, regional HIV clinics were evaluated at the National Institute of Cardiology. Inclusion criteria were the ability to walk on a treadmill, current absence of active opportunistic infections or CD4 count <200 cells/mm3, absence of symptoms suggestive of CAD (typical chest pain or anginal equivalent, evaluated using a questionnaire), 23 a history of cardiovascular disease (considered as history of angina, myocardial infarction, coronary angioplasty, or coronary artery bypass surgery), or chronic pulmonary disease. Exclusion criteria were third-degree left bundle branch block, baseline systolic blood pressure (BP) ≥180 mm Hg or diastolic BP ≥110 mm Hg at the time of the ETT. Written informed consent was obtained from all participants, and the study was approved by the local ethics committee.
Demographic, clinical, and anthropometric data were collected. All patients had fasting venous blood drawn for measures of glycemia and serum lipids. CD4 count and viral load (considered as the most recent in the previous 90 days) were extracted from medical records of the referring HIV clinics. Body mass index (BMI) was considered normal if ≥18.5 and <25 kg/m2. Waist circumference was considered normal when ≤102 cm for men and ≤88 cm for women. Lipodystrophy at the face, the limbs, and the abdomen was defined by patients’ self-report or by an investigator’s observation of morphological changes in body composition (peripheral lipoatrophy or central fat accumulation). Baseline hypertension was defined as systolic BP ≥140 mm Hg, diastolic BP ≥90 mm Hg, or use of antihypertensive medication. Diabetes was defined according to the American Diabetes Association criteria or by the use of hypoglycemic agents. 24 Total cholesterol, low-density lipoprotein (LDL)-cholesterol, high-density lipoprotein (HDL)-cholesterol, and triglycerides were considered abnormal using cutoff limits defined by the National Cholesterol Education Program for individuals with ≥2 risk factors for CAD. 25
Exercise Test Protocol
All patients underwent a Bruce treadmill protocol. 26 ,27 Patients using β-blockers withdrew the drug 48 hours before the ETT. The test might be stopped due to exhaustion, exercise-limiting leg discomfort or chest pain, systolic BP ≥240 mm Hg, or diastolic BP ≥140 (in previously hypertensive patients, or ≥120 mm Hg in individuals without baseline hypertension), or if life-threatening arrhythmias occurred.
The electrocardiographic response to exercise was considered ischemic if patients developed ≥1.5 mm ascending ST segment depression or ≥1 mm horizontal ST segment depression. Blood pressure response to exercise was considered abnormal either when systolic BP decreased ≥10 mm Hg or when systolic BP reached ≥220 mm Hg. Chronotropic incompetence was defined as the inability to reach 85% of the maximal predicted heart rate, according to age and gender.
17
Abnormal HRR after exercise was defined as a decrease in heart rate of <12 bpm in the first minute of recovery, compared to heart rate at peak exercise.
19
Recovery from exercise was performed at 2.5 km/h with 0% incline. Estimated peak oxygen consumption (V
Statistical Analysis
Categorical variables were expressed as number and percentage, and compared with chi-square or Fisher exact test. Continuous variables were expressed as mean ± standard deviation or median and interquartile interval, and compared with Student t test or Mann-Whitney test. Correlations were tested using Pearson or Spearman statistics, for variables with normal or other distributions. Analyses were 2 tailed, with a P value <.05 considered statistically significant. All analyses were performed with R software, version 2.14.
Results
Forty-nine patients, 61.2% male, aged 46.4 ± 8.4 years (30-64 years, with only 2 patients >60 years) were studied. Table 1 depicts demographic and clinical characteristics of the study population. Risk factors for CAD were common, especially dyslipidemia, and 97.9% of the patients had ≥1 risk factor for CAD. Mean BMI was 25.9 ± 4.3; 53% of the patients were overweight, 10.2% were obese, and 4% met criteria for low body weight. Triglycerides, total cholesterol, and LDL-cholesterol levels were above the limits in 10.2%, 8.2%, and 46.9% of the patients, respectively, and HDL-cholesterol was low in 61.2% of the patients. Regarding HIV infection, mean time since diagnosis was around one decade, and most patients had been treated since they were diagnosed with HIV infection. At the time of the study, all took ART (protease inhibitors in >50%). Of note, 83.6% had undetectable viral load.
Demographic and Clinical Variables of the Overall Study Population.a

Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
a n = 49.
b Numbers are mean ± standard deviation, n (%) or median.
Table 2 demonstrates the results obtained from the ETT. Exercise duration was 9.7 ± 2.1 minutes and estimated V
Data from Exercise Treadmill Test.a
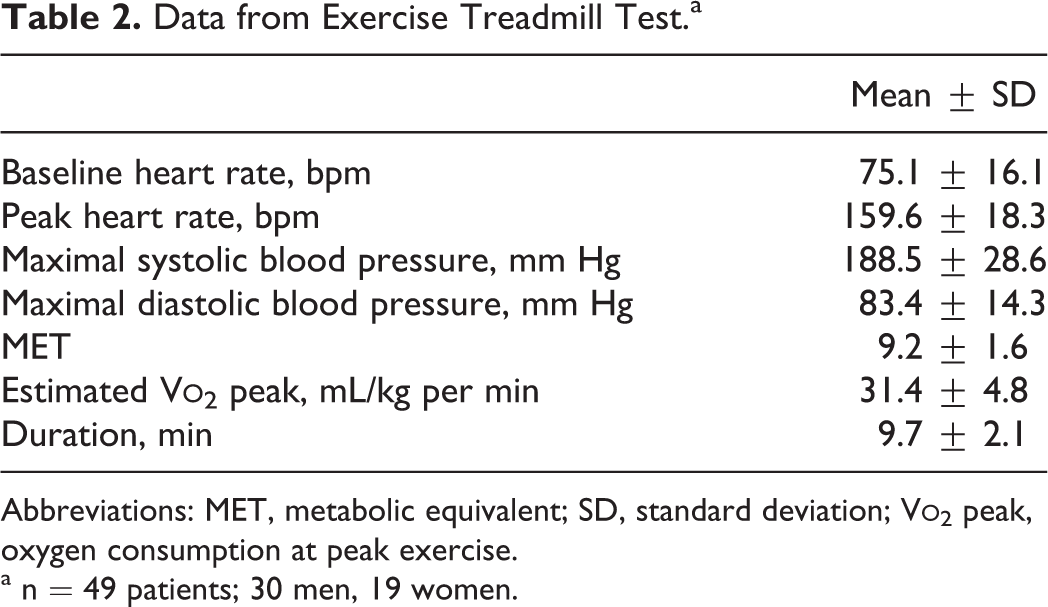
Abbreviations: MET, metabolic equivalent; SD, standard deviation; V
a n = 49 patients; 30 men, 19 women.
There was an inverse correlation between age and estimated V

Correlation between age and oxygen consumption (V
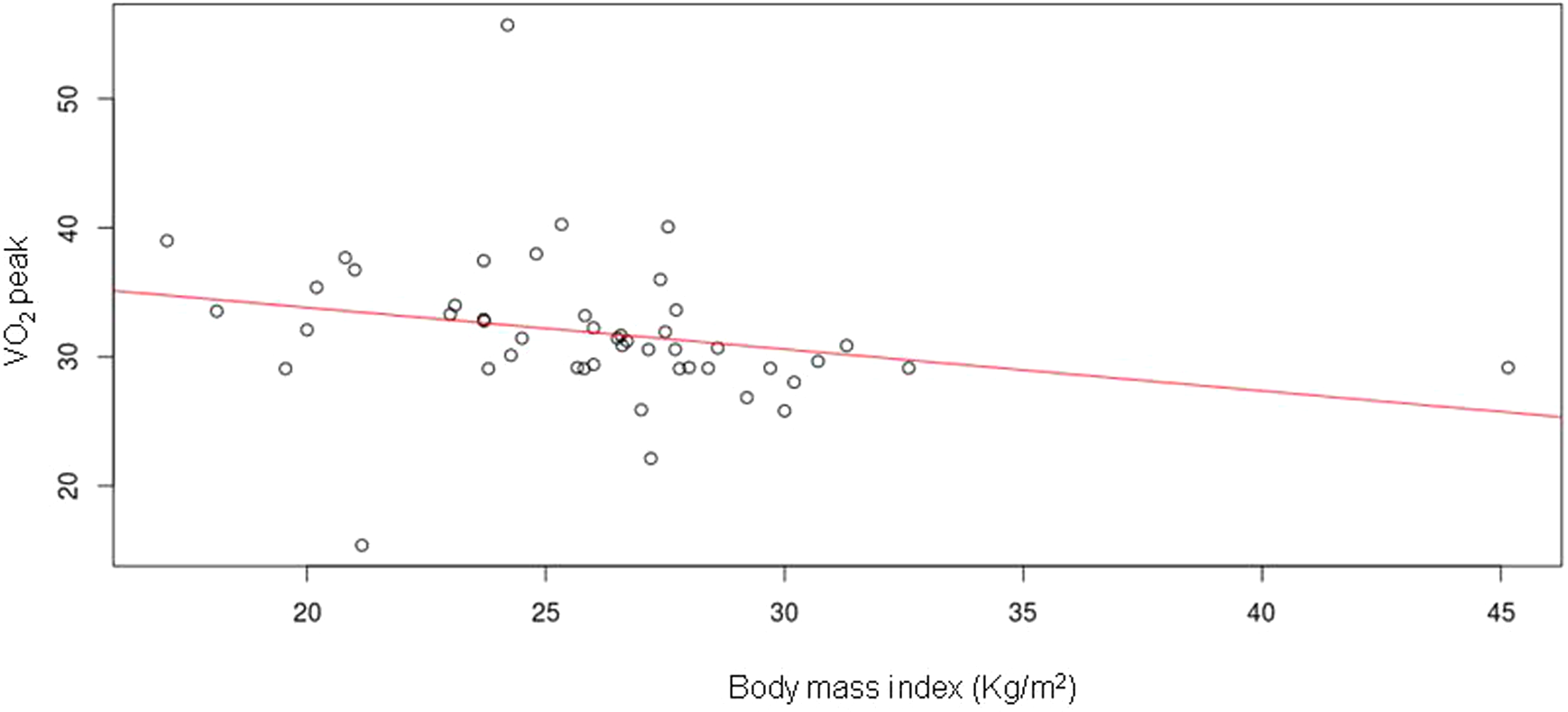
Correlation between body mass index (BMI) and oxygen consumption (V
Tables 3 and 4 display univariate comparisons of variables in patients with or without CI or abnormal HRR. There were no significant associations between clinical variables and abnormal HR responses to exercise or during recovery from it.
Comparisons between Patients With or Without Chronotropic Incompetence (CI).

a Numbers are mean ± standard deviation, n (%) or median.
Comparisons between Patients With Normal or Abnormal Heart Rate Recovery (HRR) after Exercise.

a Numbers are mean ± standard deviation, n (%) or median.
Discussion
With effective ART, HIV-infected patients are surviving longer; in parallel, susceptibility to cardiovascular disease has also increased.
29
–32
In this sense, the evaluation of cardiovascular risk in these patients is relevant to plan interventions aiming at improving cardiovascular prognosis. Whereas there are many studies using the ETT for cardiovascular risk assessment either in healthy populations or in patients with known cardiovascular disease, few have focused on the (increasingly large) population of HIV-infected patients.
33
–36
In this investigation, we studied the associations between patients’ characteristics and abnormal exercise capacity (evaluated using estimated V
This was a relatively young patient group, compared with patients with cardiovascular disease. Therefore, despite the long duration of infection (around 10 years), as well as the high prevalence of risk factors for CAD, the degree of functional impairment in these patients was low. One must have in mind, though, that in the current study, patients had been treated for most of the time since diagnosis of infection, and that at the time data were collected, all took ART, the CD4 count was above AIDS-defining limits, and viral load was undetectable in the majority, what may not reflect the overall HIV-infected population. Indeed, patients with low CD4 were excluded even in the absence of opportunistic infections because of the known association between CD4 count and physical function 2 ,5 which could introduce some confusion when studying cardiorespiratory fitness and its relationship with cardiac disease.
In this study, respiratory gas analysis was not available and, therefore, V
In this study, increasing age and weight were associated with poorer cardiorespiratory fitness, as previously described both in general and in HIV-infected populations.
6,7,43,44
Women had also lower estimated V
Neither clinical nor electrocardiographic ischemic responses were found in any of the study patients. This contrasts with the results of Duong et al who found 11% of ischemic electrocardiographic responses in the ETT of HIV-infected patients. 34 However, their population had a higher proportion of men, and, importantly, some of the patients met AIDS-defining criteria and were therefore in a more advanced stage of infection than our study population, which may account for the difference. Nonetheless, other markers of cardiovascular risk were found; one-fourth of the patients had CI, and 10.2% had abnormal HRR, which may allocate these patients to a higher risk category.
Limitations
This was a small, single-center study of highly select patients, which limits the generalizability of the conclusions. Nonetheless, we believe that the homogeneity of the studied population may be helpful for the understanding of the pathophysiology of disease in that specific subgroup and may also allow more specific conclusions, which might not be possible if “mixed” patients were studied.
Conclusions
The study started under the premise that there might be variables associated with poor functional capacity or with other abnormal responses to exercise which might be potentially modifiable, thus possibly having a favorable effect on prognosis. According to our results, overweight and obesity should be especially targeted, due to the negative correlation between BMI and V
Footnotes
Acknowledgments
The authors thank Mr Marcelo Barros and Mrs Ana Beatriz Lima for their contribution in data collection, and Bernardo Tura, MD, PhD, for statistical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.