
Abstract
Background:
The clinical presentation of cardiac abnormalities in HIV-infected patients may be atypical or masked by concurrent illnesses that lead to misdiagnosis or they remain undiagnosed; therefore, this study was aimed to determine the frequency of cardiac abnormalities in HIV-infected patients.
Material and Methods:
Consecutive HIV-infected patients of age >13 years were studied for 3 months, after obtaining their consent. After clinical assessment, chest x-ray, electrocardiogram, 2-dimensional echocardiography and serum Troponin T levels were done.
Results:
A total of 100 patients were studied, cardiomegaly was observed in the x-ray of 15% of them, abnormal electrocardiogram was seen in 18%, 2-dimensional echocardiography was abnormal in 67%; and diastolic dysfunction (42.8%) was the commonest abnormality followed by dilated cardiomyopathy (17.6%). Serum troponin T was elevated in 8%. The variables, opportunistic infections (OIs), antiretroviral therapy (ART), stage of HIV disease, and CD4 counts, did not affect the frequency of diastolic dysfunction.
Conclusion:
The diastolic dysfunction is the most common cardiac abnormality observed in HIV-infected patients.
Keywords
Introduction
HIV is a pandemic disease which had already affected 34 million people worldwide up until 2010. 1 As of 2009, it was estimated that 2.4 million people were living with HIV in India. 2 HIV infection virtually involves every system, including hematologic, central nervous system, respiratory system, and cardiovascular. The cardiac involvement in HIV-infected patients can occur due to a variety of causes like HIV infection itself, opportunistic infections caused by viruses, fungi, and protozoa, side effects of antiretroviral drugs, and a combination of these factors. Direct infection of target tissue with HIV, inflammation and immunosuppression secondary to HIV infection, and common comorbidities such as alcohol and drug abuse may all contribute to impairment of cardiac function. HIV is known to infect myocytes but is not found to be abundant or highly multiplicative in these cells. 3
The prevalence of cardiac involvement in HIV infection has been reported to range from 28% to 73%. 4 At the beginning of the HIV epidemic, heart muscle disease was the dominant cardiac complication of HIV infection in the developed world, and tuberculous pericarditis (incidence as high as 11% per year) was the most important cardiac manifestation of the disease in Africa. 5 The prevalence of infective endocarditis has been reported to be as high as 34% in HIV-positive cohorts. 4 The cardiac abnormalities reported in HIV-infected patients are dilated cardiomyopathy, pericarditis and pericardial effusion, and pulmonary artery hypertension, vascular diseases, and arrhythmia. Myocarditis and myocardial infection with HIV-1 are the best-studied causes of cardiomyopathy in HIV disease. 6 Elevation in troponin T level may point toward ongoing myocardits in asymptomatic HIV-infected patients. In a study, cardiovascular diseases (CVDs) have attributed up to 20% of mortality in HIV-infected patients. 7 With improved clinical surveillance and treatment, more HIV-infected patients are living longer, and now more attention is being paid toward CVDs. The advent of combined antiretroviral therapy (ART) has changed the pattern of disease in developed countries where premature coronary artery disease and other manifestations of atherosclerosis are now the most common cardiovascular disorders in HIV-infected patients. 8 Although large numbers of studies pertaining to cardiac involvement in HIV-infected patients have been reported from different countries, data from India are scanty. Therefore, this endeavor is done with the objective to determine the pattern of cardiac abnormalities in HIV-infected patients in India and also to find out their relationship with stage of HIV disease.
Materials and Methods
This hospital-based cross-sectional study encompassed subsequent 100 HIV-infected patients who were diagnosed per National AIDS Control Organization (NACO) guidelines between October and December 2010. HIV-infected patients of age >13 years, attending a medical outpatient department (OPD) or HIV clinic, and admitted in medical wards of our institute were studied. Patients who had ischemic, rheumatic, congenital heart disease, and chronic respiratory illness based on history prior to diagnosis of HIV infection were excluded. Posterior–anterior chest X-ray, 12 lead electrocardiography (ECG), 2-dimensional echocardiography (2D echo), and troponin T level (by Immunoanalyzer Cobas E 411, Roche Diagnostics, India Pvt. Ltd.) were carried out in all the study participants. Troponin T level >0.01 ng/mL was considered as abnormal (normal value of troponin T is <0.01 ng/mL). Two-dimensional transthoracic echocardiography, including M mode, color Doppler, pulse wave, and continuous wave Doppler, was done. The 2D echo was performed by an experienced operator using an Agilent Image Point ultrasound instrument with 3.0 and 3.5 MHz transducers. For each study participant, the following views were obtained: left parasternal long axis, left parasternal short axis, apical 2-chamber, and apical 4-chamber. Transmitral flow was assessed in the apical 4-chamber view with the pulsed Doppler sample volume at the leaflet tips. The following variables were measured: parameters measured in left parasternal view by M mode were left ventricular (LV) dimensions in end diastole and end systole, interventricular septum, and LV posterior wall thickness in diastole; and the LV ejection fraction (LVEF) was measured in apical 4-chamber and 2-chamber view by Simpson’s method. Dilated cardiomyopathy (DCMP) was diagnosed at LVEF <45%. Diastolic dysfunction was defined according to pulse wave Doppler parameters. Diastolic dysfunction was categorized into 3 grades, grade 1 defined as E/A ratio <0.75, grade 2 defined as E/A ratio >1, deceleration time (DT) <140 ms, and grade 3 defined as E/A ratio >2, DT <140 ms. In case any cardiac abnormality was detected, expert consultation was taken from cardiology department for further management. Data were analyzed statistically by SPSS 17; and Mann-Whitney U test, the Wilcoxon matched pair signed rank test, paired t test, and the chi-square test were used. A P value <.05 for a 2-sided test was considered statistically significant.
Results
General Characteristics
The mean age of 100 (78% men and 22% women) study patients was 37.31 ± 8.71 years. Past history revealed that 4 had diabetes, 4 had hypertension, and 1 had both, and 2 patients had chronic obstructive pulmonary disease. Regarding the history of addiction, 35 patients were smokers, 13 were alcoholic, and none were intravenous drug abusers. In all, 52 patients had AIDS (World Health Organization [WHO] stage IV) and the remaining had HIV disease. Fifty-one patients were receiving ART for a mean duration of 14.02 months. Opportunistic infections were found in 25% of the patients, and out of which 80% of them had Mycobacterium tuberculosis infection. Table 1 shows general characteristics between AIDS and HIV disease. Only 9 patients were symptomatic (all symptomatic patients had complaints of dyspnea and 2 also had chest pain on exertion). Although diastolic dysfunction was seen in 39 patients, only 7 had dyspnea on exertion.
Comparison of Demographic Variables between HIV Disease versus AIDS.

a
Investigational Parameters
All patients had their chest X-ray, ECG, and serum troponin T levels, but 2D echo was performed only in 91 patients. Nine patients were lost to follow-up. The percentages of cardiac abnormality seen by different investigational tests are shown in Figure 1. On the posterior–anterior view of the chest X-ray, cardiomegaly was observed in 15%, 2 patients had markedly enlarged cardiac silhouette. Of these 2 patients, 1 had dilated cardiomyopathy with severe LV dysfunction while the other patient was diagnosed with moderate aortic regurgitation (AR) with mild LV enlargement on 2D echo. Here, the etiology of AR could be hypertensive heart disease as the patient was a known case of hypertension. Abnormal ECG finding was reported in 18 patients, sinus tachycardia being the commonest (n = 15). Other abnormal ECG findings seen in decreasing order were nonspecific ST-T wave changes (n = 14), intraventricular conduction abnormalities (n = 8), and left atrial enlargement (n = 4). Abnormal 2D echo findings were seen in 67% (61 out of 91), diastolic dysfunction (42.8%) being the commonest abnormality detected (Figure 2). Valvular leak was also seen in 17.6% (16 out of 91), mitral incompetence being the commonest; and other etiologies were aortic and tricuspid incompetence. Pericardial effusion was observed in 10.9%, was moderate in 4, and was minimal in 6 patients, and temponade physiology was not evident in any patients. The LV dysfunction ((LVEF <45%) was seen in 8 patients, out of which 3 were having global hypokinesia suggestive of dilated cardiomyopathy and 5 patients had regional wall motion abnormality with LV dysfunction, and they were referred to cardiovascular department for further evaluation. Two patients had left anterior descending artery territory hypokinesia which might be the harbinger of LV dysfunction. Mild pulmonary artery hypertension (pulmonary artery systolic pressure [PASP] >30 mm Hg) was found in 3 patients and none of them had any past history of chronic respiratory illnesses. Serum troponin T was elevated in 8%; 4 patients had more than 10 times the normal value and all 4 had LV dysfunction on 2D echo. The percentage of abnormal cardiac findings detected by ECG, 2D echo, and troponin T levels did not vary significantly when compared for stage (HIV disease vs AIDS shown in Table 2) and for ART status (ART vs ART-nave HIV-infected patients; Table 3). Logistic regression analysis could not establish any significant relationship between variables, namely older age, sex, history of diabetes and hypertension, smoking, alcohol, opportunistic infections, ART, stage of HIV disease, and CD4 count with diastolic dysfunction. As shown in Table 4, the age group between 30 and 40 years and the age group above 40 years had odds of 7.44 and 5.67, respectively, for diastolic dysfunction to be present in HIV-positive patients. This finding can be explained by the fact that the majority (78%) of the patients in our study were older than 40 years.
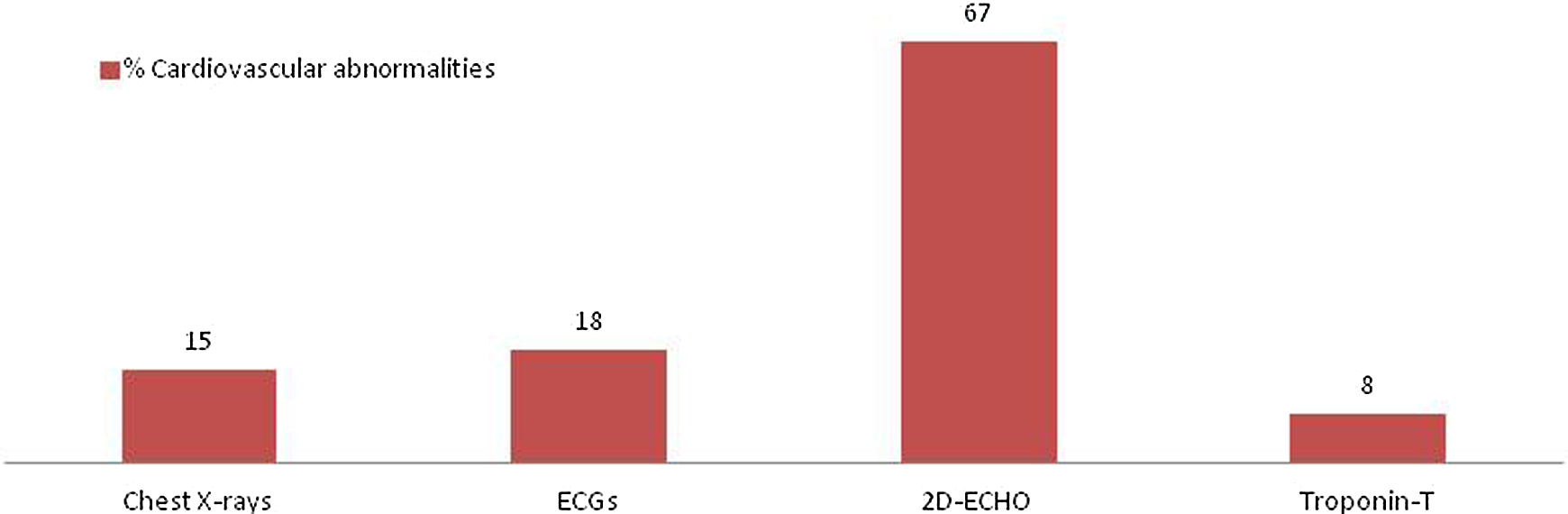
The frequency of cardiovascular abnormalities detected by various investigational tools used in the study.

The frequency of cardiac abnormalities observed in HIV-infected patients by 2D echo examination. Here the diastolic dysfunction was the commonest cardiac abnormality in HIV-infected patients. 2D echo indicates 2 dimensional echocardiography; RWMA, regional wall motion abnormality; PAH, pulmonary arterial hypertension.
Cardiac Investigations in Patients of AIDS and HIV Disease.

Abbreviations: LVEF, left ventricular ejection fraction; 2D, 2-dimentional.
a
b 2D Echocardiography was performed in 91 HIV-infected patients.
Comparison of Variables between Patients on ART versus ART Naive.

Abbreviations: AP, anterior–posterior; 2D, 2-dimentional; ART, antiretroviral therapy.
a Wherever expected frequency in a cross tab was less than 5.
b 2D echocardiography was performed in 91 HIV-infected patients.
Logistic Regression Analysis Done to Correlate Diastolic Dysfunction with Various Variables.a

Abbreviation: ART, antiretroviral therapy.
a Logistic regression analysis could not show high likelihood of diastolic dysfunction in HIV-infected patients in the presence of diabetes, hypertension, smoking, advanced stage, and ART as well as with duration of ART. Unexplained, high prevalence rates of diastolic dysfunction were seen in the younger age group (30-40 years).
Discussion
The exact prevalence of cardiac involvement in HIV/AIDS is uncertain, and it varies from 28% to 73% depending on the screening methods selected, the population studied, and the definition of cardiac abnormality.3,9 In the present study, 2D echo demonstrates cardiac abnormalities in 67% of HIV-infected patients, the commonest being the diastolic dysfunction, and the other less common cardiac dysfunctions in decreasing order were DCMP with valvular leak, pericardial effusion, regional wall motion abnormality, and pulmonary arterial hypertension (PAH).
Diastolic dysfunction is characterized by elevated LV end-diastolic pressure despite normal or subnormal diastolic volume. In a prospective study on 91 HIV-positive cohort, diastolic dysfunction on echocardiography was reported in 37% (95% confidence interval [CI] 27.4-48.1). 10 Since regional LV dysfunction may be the earliest stage of subsequent global LV dysfunction, the identification of this early stage is of critical importance in the management of HIV-associated myocardial disease. 11 The ECG may reveal nonspecific conduction defects or repolarization changes. Up to 57% of asymptomatic HIV-infected patients have baseline ECG abnormalities, including supraventricular and ventricular ectopic beats. 12 Dilated cardiomyopathy has been associated with advanced immunosuppression and lower CD4 counts, and it is an independent risk factor for death. 13 Additionally, current evidence suggests that patients on ART tend to have increased risk of cardiomyopathy 14 and coronary heart disease.15,16 Patients with HIV infections have been shown to have an increased risk of coronary artery disease, and the most likely mechanism is endothelial dysfunction. Other underlying causes may be abnormal lipid metabolism, lipodystrophy syndrome, insulin resistance, and impaired glucose metabolism. In contrast, this study could not establish the association of diastolic dysfunction with advanced stage of HIV disease, CD4 count, and ART status. Diastolic dysfunction was common in the age group between 30 and 40 years and above 40 years, while in the young (less than 30 years), diastolic dysfunction was not significantly present. It could be due to most of the studied patients being older than 30 years of age, and age could also have its own bearing in occurrences of diastolic dysfunction in HIV-positive patients. The prevalence of pericardial effusion was not found to be more than that reported in previous studies. 5 In the present study, PAH was seen in 3.3%, and none of them had any symptoms and previous history of chronic respiratory illness. However, PAH has been reported in around 0.5% of hospitalized AIDS patients and is a cause of severe cardiac impairment with associated cor pulmonalia and death. 7 The pathogenesis of PAH is not clearly known but can be multifactorial. HIV may cause endothelial damage and mediator-related vasoconstriction through stimulation by the envelope glycoprotein 120, including direct release and pulmonary vasoconstrictor effects of endothelin-1 (ET-1), interleukin 6 (IL-6), and tumor necrosis factor-α (TNF-α). HIV is frequently identified in alveolar macrophages on histology. 17 These macrophages release TNF-α, oxide anions, and proteolytic enzymes in response to infection. Effects of ART on pulmonary artery endothelial cells are unknown.
Isolated right ventricular dysfunction with right ventricular hypertrophy is also associated with HIV/AIDS and has been reported at postmortem 18 and echocardiographic studies.19-21 Most cases of isolated right ventricular dysfunction are probably not due to primary myocardial disease from HIV but rather due to secondary changes in the pulmonary circulation from recurrent bronchopneumonia, 21 HIV-induced pulmonary arteritis, 22 and pulmonary tuberculosis, which are common in these patients. Tricuspid regurgitation may also result in volume overload and was a specific cause of right ventricular dysfunction in a man with nonbacterial thrombotic endocarditis and end-stage AIDS. 23 The mechanism for HIV-associated myocardial pathogenesis remains unclear. A variety of potential etiologies have been postulated in HIV-related heart disease, including myocardial infection with HIV itself, opportunistic infections, drug-related cardiotoxicity, nutritional deficiencies, autoimmune responses, and prolonged immunosuppression. It has been reported that HIV virions appear to infect the myocardial tissue in patchy distributions.13,24
The differential diagnosis of diastolic dysfunction in HIV/AIDS includes LV dysfunction secondary to ischemic heart disease, diabetes or hypertension, hypersensitivity reactions to drugs or foreign material, and coronary spasm from cocaine use. 25 In this study, high prevalence of diastolic dysfunction seen can partially be contributed to diabetes and hypertension because 2D echo showed diastolic dysfunction in 4 HIV-infected patients who had diabetes. Diastolic dysfunction was also seen in 2 hypertensive patients, 1 of them had concurrent diabetes. None of our HIV-infected patients with diabetes had dilated cardiomyopathy.
The study is limited because the number of patients studied is small, and there is a lack of sex- and age-matched control groups. This is an observational study that does not help establish a causal relationship of different cardiac abnormalities seen during the study with HIV disease. Because of these constraints newer echocardiographic parameters could not be evaluated.
To conclude, in HIV infection, undermined structural cardiac abnormalities are common, diastolic dysfunction being the commonest one. The diastolic dysfunction is independently associated with HIV infection without being affected by traditional risk factors such as diabetes, hypertension, smoking, and age. HIV-infected patients had a higher prevalence of diastolic dysfunction. The questions, why does it happen; what would be the course of diastolic dysfunction; should HIV-infected patients with mild diastolic dysfunction be treated, are to be answered in the future through further studies with larger numbers of participants, which would also help in understanding the natural history of these abnormalities in HIV-infected individuals.
Footnotes
Authors’ Note
The study was approved by the ethics committee of CSM Medical University, Lucknow, India, where the undertaking was done.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by a research cell of our institute in the form of a short-term intramural project.